
Abstract
Background
The pathogenesis of late-onset sepsis (LOS) in preterm infants is poorly understood and knowledge about risk factors, especially prenatal risk factors, is limited. This study aimed to assess the association between the cause of preterm birth and LOS in very preterm infants.
Methods
2052 very preterm singletons from a national population-based cohort study alive at 72 h of life were included. Survival without LOS was compared by cause of preterm birth using survival analysis and Cox regression models.
Results
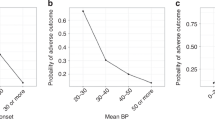
437 (20.1%) had at least one episode of LOS. The frequency of LOS varied by cause of preterm birth: 17.1% for infants born after preterm labor, 17.9% after preterm premature rupture of membranes, 20.3% after a placental abruption, 20.3% after isolated hypertensive disorders, 27.5% after hypertensive disorders with fetal growth restriction (FGR), and 29.4% after isolated FGR. In multivariate analysis, when compared to infants born after preterm labor, the risk remained higher for infants born after hypertensive disorders (hazard ratio HR = 1.7, 95% CI = 1.2–2.5), hypertensive disorders with FGR (HR = 2.6, 95% CI = 1.9–3.6) and isolated FGR (HR = 2.9, 95% CI = 1.9–4.4).
Conclusion
Very preterm infants born after hypertensive disorders or born after FGR had an increased risk of LOS compared to those born after preterm labor.
Impact
-
Late-onset sepsis risk differs according to the cause of preterm birth.
-
Compared with those born after preterm labor, infants born very preterm because of hypertensive disorders of pregnancy and/or fetal growth restriction display an increased risk for late-onset sepsis.
-
Antenatal factors, in particular the full spectrum of causes leading to preterm birth, should be taken into consideration to better prevent and manage neonatal infectious morbidity and inform the parents.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
McElrath, T. F. et al. Pregnancy disorders that lead to delivery before the 28th week of gestation: an epidemiologic approach to classification. Am. J. Epidemiol. 168, 980–989 (2008).
Basso, O. & Wilcox, A. Mortality risk among preterm babies: immaturity versus underlying pathology. Epidemiology 21, 521–527 (2010).
Delorme, P. et al. Cause of preterm birth as a prognostic factor for mortality. Obstet. Gynecol. 127, 40–48 (2016).
Kamath-Rayne, B. D., DeFranco, E. A., Chung, E. & Chen, A. Subtypes of preterm birth and the risk of postneonatal death. J. Pediatr. 162, 28–34.e2 (2013).
Stout, M. J. et al. Neonatal outcomes differ after spontaneous and indicated preterm birth. Am. J. Perinatol. 35, 494–502 (2018).
Gagliardi, L. et al. Pregnancy disorders leading to very preterm birth influence neonatal outcomes: results of the population-based ACTION cohort study. Pediatr. Res 73, 794–801 (2013).
Garite, T. J. et al. A multicenter prospective study of neonatal outcomes at less than 32 weeks associated with indications for maternal admission and delivery. Am. J. Obstet. Gynecol. 217, 72.e1 (2017).
Chevallier, M. et al. Leading causes of preterm delivery as risk factors for intraventricular hemorrhage in very preterm infants: results of the EPIPAGE 2 cohort study. Am. J. Obstet. Gynecol. 216, 518.e1 (2017).
Torchin, H. et al. Placental complications and bronchopulmonary dysplasia: EPIPAGE-2 Cohort Study. Pediatrics 137, e20152163 (2016).
Hanke, K. et al. Preterm prelabor rupture of membranes and outcome of very-low-birth-weight infants in the German Neonatal Network. PLoS ONE 10, e0122564 (2015).
Stoll, B. J. et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics 110, 285–291 (2002).
Olivier, F., Bertelle, V., Shah, P. S., Drolet, C. & Piedboeuf, B. Association between birth route and late-onset sepsis in very preterm neonates. J. Perinatol. 36, 1083–1087 (2016).
Stoll, B. J. et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics 126, 443–456 (2010).
Mitha, A. et al. Neonatal infection and 5-year neurodevelopmental outcome of very preterm infants. Pediatrics 132, e372–e380 (2013).
Bright, H. R. et al. Neurocognitive outcomes at 10 years of age in extremely preterm newborns with late-onset bacteremia. J. Pediatr. 187, 43–49 (2017).
Shane, A. L., Sánchez, P. J. & Stoll, B. J. Neonatal sepsis. Lancet 390, 1770–1780 (2017).
Carr, R., Brocklehurst, P., Doré, C. J. & Modi, N. Granulocyte-macrophage colony stimulating factor administered as prophylaxis for reduction of sepsis in extremely preterm, small for gestational age neonates (the PROGRAMS trial): a single-blind, multicentre, randomised controlled trial. Lancet 373, 226–233 (2009).
ELFIN Trial Investigators Group. Enteral lactoferrin supplementation for very preterm infants: a randomised placebo-controlled trial. Lancet 393, 423–433 (2019).
Ohlsson, A. & Lacy, J. B. Intravenous immunoglobulin for preventing infection in preterm and/or low birth weight infants. Cochrane Database Syst. Rev. 7, CD000361 (2013).
Ancel, P.-Y. & Goffinet, F. EPIPAGE 2: a preterm birth cohort in France in 2011. BMC Pediatr. 14, 97 (2014).
Shrier, I. & Platt, R. W. Reducing bias through directed acyclic graphs. BMC Med. Res. Methodol. 8, 70 (2008).
Howell, E. A. et al. Differences in morbidity and mortality rates in black, white, and hispanic very preterm infants among New York City hospitals. JAMA Pediatr. 172, 269–277 (2018).
Dietz, P. M. et al. Infant morbidity and mortality attributable to prenatal smoking in the U.S. Am. J. Prev. Med. 39, 45–52 (2010).
Klemetti, R., Gissler, M., Sainio, S. & Hemminki, E. At what age does the risk for adverse maternal and infant outcomes increase? Nationwide register-based study on first births in Finland in 2005-2014. Acta Obstet. Gynecol. Scand. 95, 1368–1375 (2016).
Declercq, E., MacDorman, M., Cabral, H. & Stotland, N. Prepregnancy body mass index and infant mortality in 38 U.S. States, 2012-2013. Obstet. Gynecol. 127, 279–287 (2016).
McGovern, M. et al. Challenges in developing a consensus definition of neonatal sepsis. Pediatr. Res. 88, 14–26 (2020).
Monier, I. et al. Fetal and neonatal outcomes of preterm infants born before 32 weeks of gestation according to antenatal vs postnatal assessments of restricted growth. Am. J. Obstet. Gynecol. 216, 516.e1 (2017).
Ballow, M., Cates, K. L., Rowe, J. C., Goetz, C. & Desbonnet, C. Development of the immune system in very low birth weight (less than 1500 g) premature infants: concentrations of plasma immunoglobulins and patterns of infections. Pediatr. Res. 20, 899–904 (1986).
Wirbelauer, J., Thomas, W., Rieger, L. & Speer, C. P. Intrauterine growth retardation in preterm infants ≤32 weeks of gestation is associated with low white blood cell counts. Am. J. Perinatol. 27, 819–824 (2010).
Strunk, T. et al. Histologic chorioamnionitis is associated with reduced risk of late-onset sepsis in preterm infants. Pediatrics 129, e134–e141 (2012).
Downey, L. C., Smith, P. B. & Benjamin, D. K. Risk factors and prevention of late-onset sepsis in premature infants. Early Hum. Dev. 86(Suppl 1), 7–12 (2010).
Smith, P. B. et al. Is an increased dwell time of a peripherally inserted catheter associated with an increased risk of bloodstream infection in infants? Infect. Control Hosp. Epidemiol. 29, 749–753 (2008).
Ananth, C. V. & Schisterman, E. F. Confounding, causality, and confusion: the role of intermediate variables in interpreting observational studies in obstetrics. Am. J. Obstet. Gynecol. 217, 167–175 (2017).
Dorling, J. et al. Controlled trial of two incremental milk-feeding rates in preterm infants. N. Engl. J. Med. 381, 1434–1443 (2019).
Underwood, M. A. & Sohn, K. The microbiota of the extremely preterm infant. Clin. Perinatol. 44, 407–427 (2017).
Tarr, P. I. & Warner, B. B. Gut bacteria and late-onset neonatal bloodstream infections in preterm infants. Semin. Fetal Neonatal Med. 21, 388–393 (2016).
Carl, M. A. et al. Sepsis from the gut: the enteric habitat of bacteria that cause late-onset neonatal bloodstream infections. Clin. Infect. Dis. 58, 1211–1218 (2014).
Shaw, A. G. et al. Late-onset bloodstream infection and perturbed maturation of the gastrointestinal microbiota in premature infants. PLoS ONE 10, e0132923 (2015).
Rutayisire, E., Huang, K., Liu, Y. & Tao, F. The mode of delivery affects the diversity and colonization pattern of the gut microbiota during the first year of infants’ life: a systematic review. BMC Gastroenterol. 16, 86 (2016).
Azad, M. B. et al. Impact of maternal intrapartum antibiotics, method of birth and breastfeeding on gut microbiota during the first year of life: a prospective cohort study. BJOG 123, 983–993 (2016).
Cantey, J. B., Pylen, A. K., Wozniak, P. S., Hynan, L. S. & Sánchez, P. J. Early antibiotic exposure and adverse outcomes in preterm, very low birth weight infants. J. Pediatr. 203, 62–67 (2018).
Acknowledgements
We are grateful for the participation of all families of preterm infants in the EPIPAGE-2 cohort study and for the cooperation of all maternity and neonatal units in France. The EPIPAGE-2 study has been funded with support from the French Institute of Public Health Research/Institute of Public Health and its partners the French Health Ministry, the National Institute of Health and Medical Research, the National Institute of Cancer, and the National Solidarity Fund for Autonomy; The French EQUIPEX Program of Investments in the Future (reference ANR-11-EQPX-0038). The PremUp Foundation. The Fondation de France (reference 00050329). M.L. has been supported by grants from the French Society of Pediatrics. The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Consortia
Contributions
Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data: all authors. Drafting the article or revising it critically for important intellectual content: M.L., L.F., P.B., and E.L. Final approval of the version to be published: all authors
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
Consent for participation was provided by mothers at delivery. EPIPAGE-2 was approved by the Committee for the Protection of People participating in biomedical research (reference CPP SC-2873).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Letouzey, M., Foix-L’Hélias, L., Torchin, H. et al. Cause of preterm birth and late-onset sepsis in very preterm infants: the EPIPAGE-2 cohort study. Pediatr Res 90, 584–592 (2021). https://doi.org/10.1038/s41390-021-01411-y
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41390-021-01411-y
This article is cited by
-
Characterising commensal and pathogenic staphylococcal interactions with neonatal and adult blood
Scientific Reports (2025)
-
Preterm sepsis is associated with acute lung injury as measured by pulmonary severity score
Pediatric Research (2023)
-
Early skin-to-skin contact and risk of late-onset-sepsis in very and extremely preterm infants
Pediatric Research (2023)
-
Developments in pediatrics in 2020: choices in allergy, autoinflammatory disorders, critical care, endocrinology, genetics, infectious diseases, microbiota, neonatology, neurology, nutrition, ortopedics, respiratory tract illnesses and rheumatology
Italian Journal of Pediatrics (2021)
-
In neonatal sepsis every catheter matters
Pediatric Research (2021)
