
Abstract
Background
Paediatric inflammatory multisystem syndrome (PIMS) is a rare condition temporally associated with SARS-CoV-2 infection. Using national surveillance data, we compare presenting features and outcomes among children hospitalized with PIMS by SARS-CoV-2 linkage, and identify risk factors for intensive care (ICU).
Methods
Cases were reported to the Canadian Paediatric Surveillance Program by a network of >2800 pediatricians between March 2020 and May 2021. Patients with positive versus negative SARS-CoV-2 linkages were compared, with positive linkage defined as any positive molecular or serologic test or close contact with confirmed COVID-19. ICU risk factors were identified with multivariable modified Poisson regression.
Results
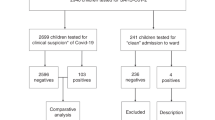
We identified 406 children hospitalized with PIMS, including 49.8% with positive SARS-CoV-2 linkages, 26.1% with negative linkages, and 24.1% with unknown linkages. The median age was 5.4 years (IQR 2.5–9.8), 60% were male, and 83% had no comorbidities. Compared to cases with negative linkages, children with positive linkages experienced more cardiac involvement (58.8% vs. 37.4%; p < 0.001), gastrointestinal symptoms (88.6% vs. 63.2%; p < 0.001), and shock (60.9% vs. 16.0%; p < 0.001). Children aged ≥6 years and those with positive linkages were more likely to require ICU.
Conclusions
Although rare, 30% of PIMS hospitalizations required ICU or respiratory/hemodynamic support, particularly those with positive SARS-CoV-2 linkages.
Impact
-
We describe 406 children hospitalized with paediatric inflammatory multisystem syndrome (PIMS) using nationwide surveillance data, the largest study of PIMS in Canada to date.
-
Our surveillance case definition of PIMS did not require a history of SARS-CoV-2 exposure, and we therefore describe associations of SARS-CoV-2 linkages on clinical features and outcomes of children with PIMS. Children with positive SARS-CoV-2 linkages were older, had more gastrointestinal and cardiac involvement, and hyperinflammatory laboratory picture.
-
Although PIMS is rare, one-third required admission to intensive care, with the greatest risk amongst those aged ≥6 years and those with a SARS-CoV-2 linkage.
Similar content being viewed by others


Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
Data availability
De-identified data that underlie the results reported in this article (text, tables, figures, and appendices) and that abide by the privacy rules of the Canadian Paediatric Surveillance Program and the Public Health Agency of Canada can be made available to investigators whose secondary data analysis study protocol has been approved by an independent research ethics board.
References
Riphagen, S., Gomez, X., Gonzalez-Martinez, C., Wilkinson, N. & Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 395, 1607–1608 (2020).
Feldstein, L. R. et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N. Engl. J. Med. 383, 334–346 (2020).
Whittaker, E. et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA 324, 259–269 (2020).
Tam, H., El Tal, T., Go, E. & Yeung, R. S. M. Pediatric inflammatory multisystem syndrome temporally associated with COVID-19: a spectrum of diseases with many names. CMAJ 192, E1093–E1096 (2020).
Radia, T. et al. Multi-system inflammatory syndrome in children & adolescents (MIS-C): a systematic review of clinical features and presentation. Paediatr. Respir. Rev. 38, 51–57 (2021).
The Royal College of Paediatrics and Child Health. Guidance: Paediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19; https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-multisystem-%20inflammatory%20syndrome-20200501.pdf.
World Health Organization. Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19: Scientific Brief; https://www.who.int/publications/i/item/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (2020).
Centers for Disease Control and Prevention, Emergency Preparedness and Response 8. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19); https://emergency.cdc.gov/han/2020/han00432.asp (2020).
Canadian Paediatric Surveillance Program. About the CPSP; https://cpsp.cps.ca/about-apropos.
Drouin, O. et al. Characteristics of children admitted to hospital with acute SARS-CoV-2 infection in Canada in 2020. CMAJ 193, E1483–E1493 (2021).
Canadian Paediatric Surveillance Program. COVID-19. www.cpsp.cps.ca/surveillance/study-etude/covid-19.
Adeli, K., Higgins, V., Trajcevski, K. & White-Al Habeeb, N. The Canadian laboratory initiative on pediatric reference intervals: a CALIPER white paper. Crit. Rev. Clin. Lab Sci. 54, 358–413 (2017).
McCrindle, B. W. et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation 135, e927–e999 (2017).
Statistics Canada. Preliminary dataset on confirmed cases of COVID-19. Public Health Agency of Canada; https://doi.org/10.25318/132600032020001-ENG (2020)
Statistics Canada. Population Estimates on July 1st, by Age and Sex; https://doi.org/10.25318/1710000501-ENG (2021)
Feldstein, L. R. et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA 325, 1074–1087 (2021).
Cherqaoui, B., Koné-Paut, I., Yager, H., Bourgeois, F. L. & Piram, M. Delineating phenotypes of Kawasaki disease and SARS-CoV-2-related inflammatory multisystem syndrome: a French study and literature review. Rheumatology (Oxford) 60, 4530–4537 (2021).
Laverty, M. et al. Multisystem inflammatory syndrome in children in Canada. Can. Commun. Dis. Rep. 47, 461–465 (2021).
Henderson, L. A. et al. American College of Rheumatology Clinical Guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 1. Arthritis Rheumatol. 72, 1791–1805 (2020).
Henderson, L. A. et al. American College of Rheumatology Clinical Guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 2. Arthritis Rheumatol. 73, e13–e29 (2021).
Swadling, L. et al. Pre-existing polymerase-specific T cells expand in abortive seronegative SARS-CoV-2. Nature 601, 110–117 (2022).
Abrams, J. Y. et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: a retrospective surveillance study. Lancet Child Adolesc. Health 5, 323–331 (2021).
Yurttutan, S., Güllü, U. U., İpek, S., Gungor, S. & Yurttutan, N. Clinical and laboratory findings of multisystem inflammatory syndrome in children (MIS-C) below age 1. Clin. Rheumatol. 40, 2515–2516 (2021).
Brodin, P. SARS-CoV-2 infections in children: understanding diverse outcomes. Immunity 55, 201–209 (2022).
Public Health Agency of Canada. Asthma in Canada – Data Blog; https://health-infobase.canada.ca/datalab/asthma-blog.html (2018).
Public Health Agency of Canada. Childhood Obesity; https://www.canada.ca/en/public-health/services/childhood-obesity/childhood-obesity.html (2016).
Mahmoud, S. et al. Treatment of MIS-C in children and adolescents. Curr. Pediatr. Rep. 10, 1–10 (2022).
Matsubara, D. et al. Longitudinal assessment of cardiac outcomes of multisystem inflammatory syndrome in children associated with COVID-19 infections. J. Am. Heart Assoc. 11, e023251 (2022).
Zambrano, L. D. et al. Effectiveness of BNT162b2 (Pfizer-BioNTech) mRNA vaccination against multisystem inflammatory syndrome in children among persons aged 12-18 years – United States, July-December 2021. MMWR Morb. Mortal. Wkly Rep. 71, 52–58 (2022).
Holm, M. et al. Risk and phenotype of multisystem inflammatory syndrome in vaccinated and unvaccinated Danish children before and during the Omicron wave. JAMA Pediatr. 176, 821–823. https://doi.org/10.1001/jamapediatrics.2022.2206 (2022)
Levy, N. et al. Severity and incidence of multisystem inflammatory syndrome in children during 3 SARS-CoV-2 pandemic waves in Israel. JAMA 327, 2452–2454. https://doi.org/10.1001/jama.2022.8025 (2022)
Kenney, P. O., Chang, A. J., Krabill, L. & Hicar, M. D. Decreased clinical severity of pediatric acute COVID-19 and MIS-C and increase of incidental cases during the Omicron wave in comparison to the Delta wave. Viruses 15, 180 (2023).
Henderson, L. A. & Yeung, R. S. M. MIS-C: early lessons from immune profiling. Nat. Rev. Rheumatol. 17, 75–76 (2021).
Acknowledgements
The authors wish to thank the pediatricians, pediatric subspecialists, and health professionals who voluntarily responded to CPSP surveys. We also wish to thank the members and leadership of the Paediatric Inpatient Research Network (PIRN) for the cases reported and their dedication to the CPSP. We are enormously grateful to the staff of the CPSP for their dedication, diligence, and commitment to this study. Lastly, the authors also wish to thank members of the CPSP Scientific Steering Committee who serve as stewards of the program.
Funding
Financial support for the Canadian Paediatric Surveillance Program (CPSP) was received from the Public Health Agency of Canada (PHAC). The CPSP is governed by an independent Scientific Steering Committee (SSC) comprised of individuals from both CPS and PHAC (the funder). Members of the SSC reviewed and approved the study design. Individuals from PHAC, CPS, and the SSC participated in the interpretation of the data. The final report was provided to PHAC for review; however, the study team maintained scientific independence and the authors were under no obligation to accept or incorporate changes to the manuscript.
Author information
Authors and Affiliations
Contributions
The study was conceived by T.E.T., M.-P.M., S.K.M., D.S.F., E.H., R.S., and R.S.M.Y.; T.E.T. wrote the first draft of the manuscript, and D.S.F. conducted the statistical analysis. All authors had access to the data, and D.S.F., C.M.H., M.L., M.K., and S.K.M. accessed and verified the data underlying the study. All authors contributed to data collection, reviewed the study results and manuscript, and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
M.-P.M. has received consulting fees from Sobin and AbbVie and payment for expert testimony from the Canadian Medical Protective Association. S.K.M. has received honoraria for lectures from GlaxoSmithKline, was a member of ad hoc advisory boards for Pfizer Canada and Sanofi Pasteur, and is an investigator on an investigator-led grant from Pfizer. R.A.B. has received honoraria and participated in advisory boards with SOBI, Roche, Amgen, and AbbVie. K.B. served as Past President of the Community Paediatrics Section of the Canadian Paediatric Society and has received royalties from Brush Education. K.C. is Chair of the Acute Care Committee of the Canadian Paediatric Society and is past president of the Emergency Medicine Section of the Canadian Paediatric Society. E.J.D. is Chair of the Scientific Research Committee and a director of Epilepsy Canada. She is also a member of Partners Against Mortality in Epilepsy and the advisory boards of Cardiol, Pendopharm and Stoke Therapeutics. C.F. is Chair of the Scientific Steering Committee for the Canadian Paediatric Surveillance Program, former Chair of the Specialty Committee in Pediatrics of the Royal College of Physicians and Surgeons of Canada, former President of the Canadian Paediatric Society, and member of the Executive as Secretary of the Canadian Critical Care Society. She has received reimbursement for travel expenses from Canadian Paediatric Society and the Royal College of Physicians and Surgeons of Canada. She has also received an honorarium for a presentation at a continuing education conference from the Université de Sherbrooke. S.F. is the President of the Association of Medical Microbiology and Infectious Disease Canada and has received consulting fees from Toronto Metropolitan University. F.K. has received honoraria for presentations given to the Association des Pédiatres du Québec and receives CMV testing kits from Altona Diagnostics. R.M.L. has received honoraria for serving as a consultant to Sobi, Novartis, Sanofi, and Eli Lilly, as chair for data monitoring committees for Eli Lilly and Novartis, and from the Canadian Rheumatology Association. C.M.H. is the Director of Children’s Mental Health of Ontario, and the Director of medical affairs for the Canadian Paediatric Society and the Canadian Paediatric Surveillance Program. J.P. reports grants from MedImmune, grants and personal fees from Merck and AbbVie, and personal fees from AstraZeneca, all outside the submitted work. R.P. is a consultant for Verity Pharmaceuticals. M.S. is supported via salary awards from the BC Children’s Hospital Foundation and the Michael Smith Foundation for Health Researc and has been an investigator on projects funded by GlaxoSmithKline, Merck, Moderna, Pfizer, Sanofi Pasteur, Seqirus, Symvivo and VBI Vaccines. All funds have been paid to his institute, and he has not received any personal payments. M.L.S. is an employee of the Public Health Agency of Canada. R.S. has received honoraria and served on an advisory board and as a consultant with Novartis, honoraria from Canadian Rheumatology Association, is a board member for Rheumatology for All, and her institution receives funding from Bristol Myers Squibb for a patient registry for which she is PO. E.H. has participated in advisory board meetings of CSL-Behring and Takeda, data safety monitoring boards of Rocket Pharmaceutical and Jasper Therapeutics, and has a patent application with the biotech Immugenia and the biotech Immune Biosolutions. All other authors report no declaration of interests.
Ethics approval and consent to participate
Research ethics approval was obtained at Health Canada-PHAC (REB #2020-002P), The Hospital for Sick Children (REB #1000070001), the Centre Hospitalier Universitaire Sainte-Justine (IRB #MP-21-2021-2901), and at individual sites as required by local policies. In Quebec, the study was conducted as a multicenter study with clinical data collected by study co-investigators, and serologies from CHUSJ done for research purposes (REB #3195) prior to the introduction of clinical testing were also included. The CPSP operates under legal authority derived from Section 4 of the Department of Health Act and Section 3 of the Public Health Agency of Canada Act. As a national surveillance program operating under these authorities (with the exception of the Province of Quebec), the CPSP does not collect any individual data elements deemed to be unique identifiers, and physicians who report cases to the CPSP are not required to obtain informed consent from patients. Participating physicians from Quebec obtain Research Ethics Board approvals from their institution in order to report clinical data to the Program. This is consistent with the Canadian Medical Association and Tri-Council Policy Statements, which allow for the collection of non-nominal and non-identifiable information for conditions under surveillance. All CPSP participants are pediatricians and pediatric subspecialists who voluntarily report cases, based on information already included in the medical chart. If any data elements requested on the questionnaire are not readily available in the chart, the physician indicates that they are unknown and do not contact the families to seek these specific details. In some cases, individual reporting physicians may provide consent to the CPSP to contact them (i.e., the reporting physician) directly to clarify cases of discrepant, missing, or unclear data. A willingness to be contacted by the CPSP is not a condition of participation in the program. Only the CPSP staff who have security clearance are aware of the name of the reporting physician; the study team does not receive this information in order to further protect patient confidentiality.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
El Tal, T., Morin, MP., Morris, S.K. et al. Paediatric inflammatory multisystem syndrome in Canada: population-based surveillance and role of SARS-CoV-2 linkage. Pediatr Res 94, 1744–1753 (2023). https://doi.org/10.1038/s41390-023-02668-1
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41390-023-02668-1
