
Abstract
Background and objectives
The benefits of enteral feeding in critically ill children have been well described, but the use of non-invasive respiratory support has been shown to delay initiation of feeds, in part due to safety concerns. We aimed to examine the association of enteral feeding by mouth and orogastric tube on clinically significant adverse events in children with bronchiolitis being treated with non-invasive respiratory support via nasal interfaces.
Methods
A retrospective cohort study of patients 0–24 months of age between 2016 and 2022 in a quaternary care hospital pediatric intensive care unit with a diagnosis of bronchiolitis and treatment with non-invasive respiratory support via nasal interface. Standard comparative statistics and multivariable regression were used to determine the association between oral and nasogastric feeding and clinically significant outcomes such as new diagnosis of pneumonia and escalation in respiratory support, as well lengths of stay.
Results
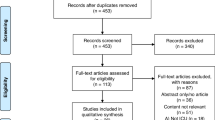
There were 407 patients 24 months or younger who were admitted with bronchiolitis and treated with non-invasive respiratory support. There was a 4.65 increased odds of developing a new pneumonia for patients who were fed nasogastrically versus orally. There were no differences in the development of pneumonia based on type of respiratory support, whether an escalation in respiratory support was needed, or based on the highest level of support received. Both pediatric intensive care unit and overall hospital lengths of stay were decreased in those who were orally fed.
Conclusions
Enteral feeding in children with bronchiolitis receiving non-invasive respiratory support appears to be safe and not associated with escalation in support or new diagnoses of pneumonia. Oral feeds were associated with decreased lengths of stay. Further work is needed to assess long term safety and ability to achieve adequate nutritional requirements.
Impact
-
Enteral feeding of children with bronchiolitis requiring non-invasive respiratory support via nasal interfaces did not have an effect on clinically significant adverse events
-
Feeding by mouth led to decreased risk of pneumonia and shorter inpatient length of stay
-
Future work is needed to study the ability to achieve nutrition goals when feeding by mouth on non-invasive support
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 14 print issues and online access
$259.00 per year
only $18.50 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Mikhailov, T. A. et al. Early enteral nutrition is associated with lower mortality in critically ill children. J. Parenter. Enter. Nutr. 38, 459–66 (2014).
Canarie, M. F. et al. Risk factors for delayed Enteral nutrition in critically Ill children. Pediatr. Crit. Care Med. 16, 283–9 (2015).
Mehta, N. M. et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. J. Parenter. Enter. Nutr. 41, 706–742 (2017).
Mehta, N. M. & Compher, C. A.S.P.E.N. clinical guidelines: nutrition support of the critically ill child. J. Parenter. Enter. Nutr. 33, 260–76 (2009).
Srinivasan, V. Heart and Lung Failure-Pediatric Insulin Titration (HALF-PINT) Study Investigators. et al. Early enteral nutrition is associated with improved clinical outcomes in critically Ill children: a secondary analysis of nutrition support in the heart and lung failure-pediatric insulin titration trial. Pediatr. Crit. Care Med. 21, 213–221 (2020).
Mehta, N. M., Bechard, L. J., Zurakowski, D., Duggan, C. P. & Heyland, D. K. Adequate enteral protein intake is inversely associated with 60-d mortality in critically ill children: A multicenter, prospective, cohort study. Am. J. Clin. Nutr. 102, 199–206 (2015).
Conway, T. P., Halaby, C., Akerman, M. & Asuncion, A. The use of High-Flow Nasal Cannula and the timing of safe feeding in children with bronchiolitis. Cureus 13, e15665 (2021).
Lenihan, A. et al. A retrospective analysis of feeding practices and complications in patients with critical bronchiolitis on non-invasive respiratory support. Children 8, 410 (2021).
Morley, S. L. Non-invasive ventilation in paediatric critical care. Paediatr. Respir. Rev. 20, 24–31 (2016).
Canning, A., Fairhurst, R., Chauhan, M. & Weir, K. A. Oral feeding for infants and children receiving nasal continuous positive airway pressure and high-flow nasal cannula respiratory supports: a survey of practice. Dysphagia 35, 443–454 (2020).
Dumpa, V., Kamity, R., Ferrara, L., Akerman, M. & Hanna, N. The effects of oral feeding while on nasal continuous positive airway pressure (NCPAP) in preterm infants. J. Perinatol. 40, 909–915 (2020).
Ferrara, L. et al. Effect of nasal continuous positive airway pressure on the pharyngeal swallow in neonates. J. Perinatol. 37, 398–403 (2017).
Canning, A., Clarke, S., Thorning, S., Chauhan, M. & Weir, K. A. Oral feeding for infants and children receiving nasal continuous positive airway pressure and high flow nasal cannula: a systematic review. BMC Pediatr. 21, 83 (2021).
Gray, S. et al. Oral feeding on high-flow nasal cannula in children hospitalized with bronchiolitis. Hosp. Pediatr. 13, 159–167 (2023).
Shadman, K. A. et al. Feeding during high-flow nasal cannula for bronchiolitis: associations with time to discharge. J. Hosp. Med 14, E43–E48 (2019).
Sochet, A. A., McGee, J. A. & October, T. W. Oral nutrition in children with bronchiolitis on high-flow nasal cannula is well tolerated. Hosp. Pediatr. 7, 249–255 (2017).
Conway, T. P., Halaby, C., Akerman, M. & Asuncion, A. The use of high-flow nasal cannula and the timing of safe feeding in children with bronchiolitis. Cureus 13, e15665 (2021).
Slater, A., Shann, F. & Pearson, G. PIM2: A revised version of the Paediatric Index of Mortality. Intensive Care Med 29, 278–85 (2003).
Tume, L. N. et al. Enteral feeding of children on noninvasive respiratory support: a four-center European study. Pediatr. Crit. Care Med. 22, 192 (2021).
Shetty, S. et al. HHFNC and NCPAP and full oral feeding in BPD infants. Eur. J. Pediatr. 175, A238–A239 (2016).
Sbaih, N., Hawthorne, K., Lutes, J. & Cavallazzi, R. Nutrition therapy in non-intubated patients with acute respiratory failure. Curr. Nutr. Rep. 10, 307–316 (2021).
Sochet, A. A. et al. Enteral nutrition improves vital signs in children with bronchiolitis on noninvasive ventilation. Hosp. Pediatr. 11, 135–143 (2021).
Leroue, M. K., Good, R. J., Skillman, H. E. & Czaja, A. S. Enteral nutrition practices in critically Ill Children requiring noninvasive positive pressure ventilation. Pediatr. Crit. Care Med. 18, 1093–1098 (2017).
Slain, K. N., Martinez-Schlurmann, N., Shein, S. L. & Stormorken, A. Nutrition and high-flow nasal cannula respiratory support in children with bronchiolitis. Hosp. Pediatr. 7, 256–262 (2017).
Hanin, M., Nuthakki, S., Malkar, M. B. & Jadcherla, S. R. Safety and efficacy of oral feeding in infants with BPD on nasal CPAP. Dysphagia 30, 121–127 (2015).
Bapat, R., Gulati, I. K. & Jadcherla, S. Impact of simple feeding quality improvement strategies on aerodigestive milestones and feeding outcomes in BPD infants. Hosp. Pediatr. 9, 859–866 (2019).
LaTuga, M. S. et al. Clinical characteristics of premature infants who orally feed on continuous positive airway pressure. Early Hum. Dev. 139, 104833 (2019).
Leibel, S. L. et al. Comparison of Continuous positive airway pressure versus High flow nasal cannula for Oral feeding Preterm infants (CHOmP): randomized pilot study. J. Matern. Fetal Neonatal Med. 35, 951–957 (2022).
Dalgleish, S. R., Kostecky, L. L. & Blachly, N. Eating in “SINC”: safe individualized nipple-feeding competence, a quality improvement project to explore infant-driven oral feeding for very premature infants requiring noninvasive respiratory support. Neonatal Netw. 35, 217–27 (2016).
Glackin, S. J., O’Sullivan, A., George, S., Semberova, J. & Miletin, J. High flow nasal cannula versus NCPAP, duration to full oral feeds in preterm infants: a randomised controlled trial. Arch. Dis. Child Fetal Neonatal Ed. 102, 329 (2017).
Fernandes, N. D. et al. Measured CPAP in a noninvasive pediatric airway and lung model. Respir. Care 66, 87–94 (2021).
Zheng, Y. R. et al. Bi-level positive airway pressure versus nasal CPAP for the prevention of extubation failure in infants after cardiac surgery. Respir. Care 67, 448–454 (2022).
Author information
Authors and Affiliations
Contributions
Kelsey Finnegan: conceptualized and designed the study, coordinated data collection and acquisition of data, interpreted data, drafted the initial manuscript, and approved the final manuscript as submitted. Julia Smalley: conceptualized and designed the study, coordinated data collection and acquisition of data, drafted the initial manuscript, and approved the final manuscript as submitted. Barbara Gallagher: conceptualized and designed the study, coordinated data collection and acquisition of data, drafted the initial manuscript, and approved the final manuscript as submitted. Michael Salt: analyzed and interpreted the data, reviewed and revised the manuscript, and approved the final manuscript as submitted. Kimberly Whalen: coordinated data collection and acquisition of data, drafted the initial manuscript, and approved the final manuscript as submitted. Michael Flaherty: conceptualized and designed the study, analyzed and interpreted data, drafted the initial manuscript, and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Finnegan, K., Smalley, J., Gallagher, B. et al. Enteral feeding in pediatric patients with bronchiolitis requiring non-invasive support via nasal interface. Pediatr Res 98, 1892–1896 (2025). https://doi.org/10.1038/s41390-025-04022-z
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41390-025-04022-z
