
Abstract
Background
Intraventricular hemorrhage (IVH) is a serious complication in extremely preterm infants, in whom the first 72 hours of life are critical. We evaluated the impact of an ultrasound-guided circulatory management protocol on IVH incidence.
Methods
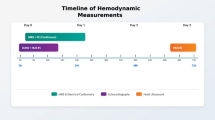
This retrospective study included infants who were born before 28 weeks of gestation and admitted to a tertiary neonatal intensive care unit between January 2018 and September 2024. In June 2022, a new protocol was introduced that incorporated three daily ultrasound assessments, adequate and tailored sedation, and targeted nitroglycerin use guided by ultrasound hemodynamic findings. Clinical outcomes and blood pressure trends were compared between the pre- and post-implementation groups.
Results
Ninety-two infants (49 pre-implementation and 43 post-implementation) were analyzed. The incidence of overall IVH decreased from 37% to 9% (p = 0.002), and severe IVH declined from 16% to 2% (p = 0.03). After implementation, increases in blood pressure were slower, and variability was reduced. No increase in hypotension duration or adverse outcomes was observed.
Conclusion
After the implementation of the ultrasound-guided circulatory management protocol, the IVH incidence significantly decreased. These findings also support the potential of ultrasound by neonatologists in the circulatory management of extremely preterm infants.
Impact statement
-
An ultrasound-guided circulatory management protocol reduced the incidence of intraventricular hemorrhage in extremely preterm infants.
-
The protocol included frequent cardiac and cranial ultrasound assessments, adequate and tailored sedation, and selective nitroglycerin use guided by real-time ultrasound hemodynamic findings.
-
After implementation, blood pressure rose more gradually and fluctuated less, indicating improved hemodynamic stability.
-
These findings support a feasible, individualized approach to protect the immature brain during the most vulnerable period.
-
The study also highlights the potential role of ultrasound by neonatologists in optimizing the care for extremely preterm infants.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 14 print issues and online access
$259.00 per year
only $18.50 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
16 March 2026
The original online version of this article was revised: In the section ‘Circulatory management protocol’, the term ‘μg/kg/h’ should have read ‘μg/kg/min’.
19 March 2026
A Correction to this paper has been published: https://doi.org/10.1038/s41390-026-04922-8
References
Zhou, M., Wang, S., Zhang, T., Duan, S. & Wang, H. Neurodevelopmental outcomes in preterm or low birth weight infants with germinal matrix-intraventricular hemorrhage: a meta-analysis. Pediatr. Res. 95, 625–633 (2024).
Nagy, Z. et al. Occurrence and Time of Onset of Intraventricular Hemorrhage in Preterm Neonates: A Systematic Review and Meta-Analysis of Individual Patient Data. JAMA Pediatr. 179, 145–154 (2025).
McGoldrick, E., Stewart, F., Parker, R. & Dalziel, S. R. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst. Rev. 12, CD004454 (2020).
Kenyon, S., Boulvain, M. & Neilson, J. P. Antibiotics for preterm rupture of membranes. Cochrane Database Syst. Rev. 2013, CD001058 (2013).
Chiriboga, N. et al. Successful implementation of an intracranial hemorrhage (ICH) bundle in reducing severe ICH: a quality improvement project. J. Perinatol. 39, 143–151 (2019).
de Bijl-Marcus, K., Brouwer, A. J., De Vries, L. S., Groenendaal, F. & Wezel-Meijler, G. V. Neonatal care bundles are associated with a reduction in the incidence of intraventricular haemorrhage in preterm infants: a multicentre cohort study. Arch. Dis. Child Fetal Neonatal Ed. 105, 419–424 (2020).
Edwards, E. M. et al. Quality Improvement Interventions to Prevent Intraventricular Hemorrhage: A Systematic Review. Pediatrics 154, e2023064431 (2024).
Isayama, T. The clinical management and outcomes of extremely preterm infants in Japan: past, present, and future. Transl. Pediatr. 8, 199–211 (2019).
Miyata, M. et al. Extensive use of vasodilator agents and functional echocardiography to monitor extremely-low-birth-weight infants in Japan. J. Neonatal Perinat. Med. 9, 261–269 (2016).
Toyoshima, K. et al. Tailor-made circulatory management based on the stress-velocity relationship in preterm infants. J. Formos. Med Assoc. 112, 510–517 (2013).
Ikeda, T. et al. Changes in the perfusion waveform of the internal cerebral vein and intraventricular hemorrhage in the acute management of extremely low-birth-weight infants. Eur. J. Pediatr. 174, 331–338 (2015).
Tanaka, K. et al. Changes in Internal Cerebral Vein Pulsation and Intraventricular Hemorrhage in Extremely Preterm Infants. Am. J. Perinatol. 41, e37–e45 (2024).
Elsayed, Y. & Ahmed, F. Blood pressure normative values in preterm infants during postnatal transition. Pediatr. Res. 95, 698–704 (2024).
Vesoulis, Z. A. et al. Blood pressure extremes and severe IVH in preterm infants. Pediatr. Res. 87, 69–73 (2020).
Jiang, L. et al. The role of blood pressure variability indicators combined with cerebral blood flow parameters in predicting intraventricular hemorrhage in very low birth weight preterm infants. Front Pediatr. 11, 1241809 (2023).
Noori, S., McCoy, M., Anderson, M. P., Ramji, F. & Seri, I. Changes in cardiac function and cerebral blood flow in relation to peri/intraventricular hemorrhage in extremely preterm infants. J. Pediatr. 164, 264–270.e703 (2014).
Stróżyk, A. et al. Pharmacological pain and sedation interventions for the prevention of intraventricular hemorrhage in preterm infants on assisted ventilation - an overview of systematic reviews. Cochrane Database Syst. Rev. 8, CD012706 (2023).
Simons, S. H. et al. Routine morphine infusion in preterm newborns who received ventilatory support: a randomized controlled trial. JAMA 290, 2419–2427 (2003).
Rozé, J. C. et al. Prolonged sedation and/or analgesia and 5-year neurodevelopment outcome in very preterm infants: results from the EPIPAGE cohort. Arch. Pediatr. Adolesc. Med. 162, 728–733 (2008).
Walter-Nicolet, E. et al. Neurodevelopmental outcomes at five years in children born very preterm (24-31 weeks) exposed to opioids with or without midazolam: results from the French nationwide EPIPAGE-2 cohort study. Lancet Reg. Health Eur. 52, 101242 (2025).
Durrmeyer, X. et al. Abstention or intervention for isolated hypotension in the first 3 days of life in extremely preterm infants: association with short-term outcomes in the EPIPAGE 2 cohort study. Arch. Dis. Child Fetal Neonatal Ed. 102, 490–496 (2017).
Acknowledgements
We would like to express our sincere gratitude to Dr. Jiro Takeuchi, and Dr. Kyoko Sakai, Institute for Clinical and Translational Science, Nara Medical University Hospital, for the valuable clinical-epidemiological advice. We thank Anahid Pinchis, B.Sc., MBA, from Edanz (https://jp.edanz.com/ac), for editing a draft of this manuscript.
Funding
No financial assistance was received in support of the study.
Author information
Authors and Affiliations
Contributions
H.A., N.O. concepted the design, analysis, and interpretation of the data. H.A., T.K., A.O., K.S., M.O., T.K., A.M., Y.T., E. N., H.T., T.N., and Y.U. contributed to data acquisition. H.A. drafted the initial manuscript. All authors critically revised the manuscript critically and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Informed consent
Consent was obtained via opt-out because this study is a retrospective observational study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: In the section ‘Circulatory management protocol’, the term ‘μg/kg/h’ should have read ‘μg/kg/min’.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Aoki, H., Kamamoto, T., Ozu, N. et al. Impact of ultrasound-guided circulatory management protocol on intraventricular hemorrhage in extremely preterm infants. Pediatr Res (2026). https://doi.org/10.1038/s41390-026-04863-2
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41390-026-04863-2
