
Abstract
This study aims to examine the effects of three intervention approaches—Latin dance intervention alone, mindfulness intervention alone, and a combined mindfulness–Latin dance intervention—on social anxiety among left-behind adolescents in rural China. A randomized controlled trial was conducted with 84 participants(age = 10.90 ± 3.05) assigned to four groups: a Latin dance-only group, a mindfulness-only group, a combined Latin dance and mindfulness group, and a control group. The intervention lasted 12 weeks. Social anxiety was assessed at baseline, post-intervention, and at a 6-week follow-up. Data were analyzed using repeated measures ANOVA. Significant reductions in social anxiety were observed over time in all three intervention groups (F(3, 80) = 15.42, p < 0.001), with no significant change in the control group (p > 0.05). The combined intervention group showed the greatest improvement, and treatment effects were maintained at follow-up. Combined intervention produced the most substantial and sustained reductions in social anxiety, whereas Latin dance led to rapid but less durable improvements and mindfulness yielded modest but stable effects. These findings suggest that integrating body-based and cognitive-emotional approaches may represent a superior strategy for enhancing both the effectiveness and maintenance of social anxiety interventions in left-behind adolescents.
Similar content being viewed by others
Introduction
China’s rapid industrialization and urbanization over the past decades have led to large-scale rural-to-urban migration, resulting in the formation of a massive population of migrant workers. According to the National Bureau of Statistics, as of 2022, approximately 295.6 million individuals were classified as rural migrant workers, with 172 million working outside their registered domicile—accounting for over one-third of the rural household population1. While labor migration has generated substantial economic benefits, it has also contributed to widespread parental absence and the emergence of a socioeconomically and psychologically vulnerable subgroup: left-behind adolescents. Left-behind adolescents—defined as youth aged 13 to 18 who reside in rural areas without the continuous presence of one or both parents for at least six months due to labor migration—exhibit elevated risks of psychological and behavioral problems2. Empirical studies have documented a higher prevalence of depression3, anxiety4, post-traumatic stress symptoms5, and externalizing behaviors such as aggression and delinquency2n this population. These outcomes are exacerbated by emotional neglect, reduced parental monitoring, and limited access to psychosocial resources6,7,8.
Among the various mental health challenges faced by adolescents, social anxiety is particularly prominent and persistent. Social anxiety refers to an intense fear of negative evaluation in social situations, which can lead to impaired academic performance, disrupted peer relationships, and reduced quality of life9,10. Recent meta-analyses have provided updated estimates of global prevalence, with higher rates typically observed in younger populations11. In the Chinese context, a systematic review by Tang et al.12reported an overall social anxiety prevalence of approximately 12% among children and adolescents, highlighting its public health significance. Notably, left-behind adolescents appear to be at even greater risk. A meta-analysis synthesizing 18 studies (N = 18,544) using the Social Anxiety Scale for adolescents reported a pooled detection rate of 36.1% among rural left-behind adolescents, significantly higher than the 20.2% observed in non–left-behind peers. More recent studies have yielded prevalence estimates ranging from 12% to over 30%, depending on the measurement tools and sampling period, consistently indicating that left-behind adolescents experience disproportionately high levels of social anxiety. Given the enduring nature of social anxiety and its elevated burden in this vulnerable population, identifying effective, targeted interventions for left-behind adolescents is both urgent and essential.
Latin dance, in contrast, offers a socially engaging and movement-based modality grounded in embodiment theory13 and social learning theory14, Through rhythmic coordination, nonverbal expression, and interpersonal synchrony, Latin dance enhances body awareness, social connection, and emotional expression15,16. fostering self-efficacy and confidence17,18. Compared to solitary physical activity, Latin dance naturally embeds peer interaction and feedback, making it a culturally relevant and feasible intervention for Chinese adolescents18,19.
Mindfulness-based interventions (MBIs) have gained strong empirical support as evidence-based approaches for managing anxiety in youth. Rooted in present-moment, nonjudgmental awareness20,21, MBIs improve attentional control, emotional regulation, and cognitive defusion22,23,24. According to the Self-Regulatory Executive Function model25. mindfulness reduces rumination and avoidance—two core mechanisms underlying social anxiety—by increasing meta-awareness and acceptance-based coping. Thus, mindfulness primarily targets internal cognitive–emotional regulation, helping adolescents relate to social-evaluative thoughts with less reactivity.
While prior studies have explored mindfulness and Latin dance separately, few have examined their integration. Importantly, the two modalities may be theoretically complementary: mindfulness strengthens internal awareness and emotional regulation, whereas Latin dance promotes external social engagement and embodied expression. When combined, mindfulness provides a cognitive foundation for managing anxiety, and Latin dance offers real-time opportunities to apply these skills in social contexts. In addition, mindfulness enhances interoceptive awareness, enabling individuals to more accurately perceive and interpret internal bodily signals that support emotional clarity, which in turn contributes to more adaptive responses to social anxiety.This dual-target approach addresses both intrapersonal and interpersonal dimensions of social anxiety, potentially producing synergistic effects that exceed either intervention alone.Therefore, the present study investigates whether the integration of mindfulness and Latin dance yields superior outcomes compared to each intervention implemented independently.
Despite increasing research on psychosocial interventions, left-behind adolescents in rural China remain underrepresented in intervention studies and face unique stressors such as disrupted attachment and limited mental health resources26. Therefore, the present study evaluated the effects of three interventions—mindfulness, Latin dance, and a combined mindfulness + Latin dance program—on social anxiety among rural left-behind adolescents. We hypothesized that while both mindfulness and Latin dance would reduce social anxiety, the combined intervention would yield the greatest and most sustained improvements due to the complementary mechanisms of internal regulation and external social engagement.
Methods
Participants
A priori power analysis for repeated measures ANOVA (4 groups × 3 time points: baseline, post-intervention, and 6-week follow-up) was conducted using G*Power 3.1.9.7. Assuming a medium-to-large effect size (f = 0.30, based on Cohen’s conventions27 and prior studies of mindfulness and Latin dance interventions in adolescents28, α = 0.05, and power (1 − β) = 0.85, a minimum of 20 participants per group was required. To account for an estimated 15% attrition rate, the target enrollment was adjusted to 23 participants per group, yielding a total sample size of 92 participants. In practice, 8 participants dropped out during the study period due to illness or scheduling conflicts (4 from the latin dance group, 4 from the mindfulness group, 4 from the combined group and 4 from the control group,). Participant flow and attrition are summarized in the CONSORT diagram (See Fig. 1).

Flow Diagram.
A total of 84 participants were rural left-behind adolescents from Huaihua Experimental Middle School in Hunan Province, China, who were screened and identified as being at risk for social anxiety, using a combination of school counselor referrals, posters, and classroom announcements. Recruitment was facilitated through cooperation with the school administration and classroom teachers, who distributed study information sheets and consent forms to guardians of eligible left-behind students. Participation was voluntary, and only students who met the inclusion criteria and returned written parental consent and child assent were enrolled. Inclusion criteria were as follows: (I) aged 13–18 years; (II) scoring ≥ 8 on the Adolescent Social Anxiety Scale; (III) no formal mindfulness training in the past year; (IV) Participants did not regularly engage in physical exercise or meditation training, in order to avoid exposure to similar interventions and to ensure the feasibility of completing the 12-week intervention; and (V) absence of serious physical illness.
Participants were excluded if they met any of the following conditions: (I)Use of psychiatric medication, including ongoing treatment with antidepressants or anxiolytics; (II) History of neurological or psychiatric surgery, either scheduled or recently performed; (III) Regular engagement in psychological counseling or psychotherapy; (IV) Participation in any concurrent behavioral or pharmacological clinical trial; (V) Involvement in instructor-led or structured exercise programs; (VI) Diagnosis of neurological disorders (e.g., epilepsy, traumatic brain injury).
Study design
This study employed a parallel-group, evaluator-blinded randomized controlled trial (RCT) design to assess the effects of three interventions—Latin dance (LG), mindfulness (MG) and a combined mindfulness and Latin dance program (LMG)—on social anxiety symptoms. To clarify the overall study duration, the 12-week intervention phase was followed by a 6-week follow-up period to evaluate the short-term sustainability of treatment effects, resulting in a total study timeline of 18 weeks. Control group (CG) served as a no-intervention and did not receive any treatment during the study period. Interventions were delivered by professionals with appropriate credentials: mindfulness instructors were nationally certified psychological counselors with formal MBSR training; Latin dance instructors held physical education degrees and Latin dance coaching certifications. The study adhered to the ethical guidelines of the Declaration of Helsinki and was approved by the University Medical Research Ethics Committee (Approval No. 2022039). Written informed consent was obtained from all participants and their parents or legal guardians before enrollment. No adverse events were reported during the intervention or follow-up periods.
Randomization and allocation
Eligible participants were randomly assigned to one of the four groups (LG, MG, LMG, CG) in a 1:1:1:1 ratio using a computer-generated randomization sequence created in SPSS (v26.0). Stratified randomization was used based on gender to ensure balance across groups. An independent statistician generated the sequence, and group assignments were placed in sequentially numbered, opaque, sealed envelopes to ensure allocation concealment. Randomization was conducted by a coordinator not involved in recruitment or delivery of interventions. Outcome assessors, who were psychology graduate students trained in mental health measurement, remained blinded to participant group allocation throughout the study.
Ethics approval
The study was approved by the Ethics Committee of Hunan Normal University prior to the initiation of the project (Approval Number: 2022039).
Consent to participate
Informed consent was obtained from all participants before the commencement of the study. All procedures complied with the Declaration of Helsinki.
Intervention procedures
Latin dance group
Participants in this group engaged in a supervised Latin dance program four times per week for 12 weeks, consistent with physical activity guidelines recommending moderate-intensity exercise at least 3–5 days per week for mental health benefits in youth29. Each 40-minute session consisted of: Check-in and 10-minute warm-up (joint mobility, dynamic stretching), 25-minute dance-based aerobic training using basic Latin steps (e.g., stationary cha-cha turns, forward and side steps, cha-cha combinations), 5-minute cool-down and relaxation, Latin dance sessions were progressive in intensity, gradually increasing from basic to combined steps to sustain a moderate-intensity range (55%–70% of maximum heart rate). Blood pressure and resting heart rate were measured at baseline for all participants to screen for exercise contraindications and to establish physiological baselines(see Fig. 2 for detailed session structure).
To ensure consistent exercise intensity and participant engagement across all dance sessions, a standardized choreography and fixed pacing were used for each class. Heart rate was monitored at multiple time points during the sessions to maintain physical activity within a safe and moderate-intensity range. Instructors also used an engagement observation checklist to rate students’ effort, coordination, and participation, and provided immediate feedback or encouragement when necessary to maintain involvement. These procedures helped ensure both fidelity and safety in the implementation of the Latin dance intervention.

Flowchart of working Latin dance intervention.
Mindfulness group
This 12-week intervention consisted of four weekly sessions lasting 40 min each. The frequency and duration were based on prior evidence indicating that mindfulness-based programs delivered 4 times per week for 40 min per session are effective in reducing anxiety and enhancing emotional regulation in adolescents26,30. The program followed a three-phase structure. Phase 1 (Preparation) introduced foundational concepts and strategies related to mindfulness to build students’ awareness of its relevance to emotional well-being. Phase 2 (Practice) served as the core of the intervention, with each session incorporating 20-minute guided mindfulness exercises using standardized techniques such as positive affirmations, gratitude journaling, and visualization of successful social interactions. Phase 3 (Integration) emphasized the application of learned strategies in daily life through activities such as guided meditation, mindful eating, and structured emotional regulation tasks, aiming to facilitate the incorporation of mindfulness into everyday routines. A standardized intervention manual adapted from youth-appropriate mindfulness protocols (e.g., Mindfulness-Based Cognitive Therapy for Adolescents) was used to ensure consistency. Each session was delivered in small groups of 8–12 participants to maintain group cohesion and allow for individualized guidance (see Fig. 3 for the intervention flowchart).
To ensure adherence to the mindfulness protocol, multiple fidelity-monitoring strategies were implemented. Attendance was recorded at every session to track participant engagement. In addition, students completed brief practice logs to document any mindfulness activities conducted outside of class. Instructors used a standardized session fidelity checklist to ensure that core components (e.g., breathing awareness, body scanning, guided reflection) were delivered consistently. Furthermore, instructors participated in weekly supervision meetings with the research team to review session quality and address any deviations from the protocol.

Flowchart of working Mindfulness intervention.
Combined group
This group participated in an integrated training schedule four times per week for 12 weeks. Each session consisted of 20 min of mindfulness (following the same curriculum as the mindfulness group), a 5-minute rest, and 20 min of Latin dance (as described above). This structure aimed to leverage the emotional regulation benefits of mindfulness with the social and physical engagement of latin dance(see Fig. 4 for schedule overview).

Flowchart of working combined intervention.
Control group
Participants in the control group were randomly selected and received no active intervention during the 18-week period. They were instructed to maintain their normal daily routines and did not participate in any structured exercise or mindfulness training. However, they underwent the same monitoring procedures and completed the same assessments as the intervention groups to ensure consistency and comparability in outcome evaluation.
Measures
Social anxiety symptoms
Social anxiety was assessed using the Social Anxiety Scale for adolescents (SASA), originally developed by La Greca et al. and later translated and validated in Chinese by Wang Xiangdong31,32. The scale contains two subscales—Fear of Negative Evaluation and Social Avoidance—using a 3-point Likert format. A total score of ≥ 8 was used as the clinical cut-off. In the current sample, the SASA demonstrated high reliability (Cronbach’s α = 0.892), with subscale alphas exceeding 0.70. The Kaiser-Meyer-Olkin (KMO) value was 0.729, indicating good sampling adequacy.
Statistical analysis
All analyses were conducted using IBM SPSS Statistics (v26.0). Descriptive statistics summarized baseline demographics and symptom variables. Factor analysis of variance and chi-square tests assessed between-group differences at baseline. A repeated measures ANOVA was performed to analyze primary outcomes. Assumptions of normality (Shapiro–Wilk), homogeneity of variance (Levene’s test), and sphericity (Mauchly’s test) were checked. Greenhouse-Geisser correction was applied when necessary. Statistical significance was set at p < 0.05.
Results
Baseline characteristics of participants
A total of 84 (age = 10.90 ± 3.05) left-behind adolescents were randomly allocated to four groups: Control (CG), Latin Dance (LG), Mindfulness (MG), and Combined Intervention (LMG), each comprising 21 participants. Baseline demographic and psychosocial variables—including age, gender distribution, parental marital status, and frequency of parental return—did not significantly differ across groups (all p > 0.05), indicating group comparability prior to intervention(see Table 1).
Intervention effects on social anxiety
At baseline (T0), the four groups did not differ significantly in social anxiety (SA) scores (p > 0.05), indicating comparable starting levels {CG: 10.52 ± 1.99, 95% CI [9.74, 11.30]; DG: 11.14 ± 3.29, 95% CI [9.82, 12.46]; MG: 10.95 ± 3.29, 95% CI [9.63, 12.27]; LMG: 11.00 ± 3.19, 95% CI [9.72, 12.28]}. A significant Group × Time interaction was found (F(6,192) = 7.85, η² = 0.14, p < 0.01), therefore simple effect analyses were conducted to further examine the nature of this interaction. There was also a significant main effect of Time (F(2,192) = 41.89, η² = 0.39, p < 0.001), with overall SA scores decreasing from T0 to T1 and T2. From T0 to T1, the control group showed no meaningful change (p > 0.05), whereas DG {7.57 ± 1.60, 95% CI [6.93, 8.21]}, MG {8.90 ± 1.95, 95% CI [8.12, 9.68]}, and LMG {5.63 ± 1.41, 95% CI [5.07, 6.19]} demonstrated significant reductions (all p < 0.05). This pattern persisted at T2: CG remained stable {10.67 ± 2.13, 95% CI [9.80, 11.54], p > 0.05}, while LG {7.43 ± 1.54, 95% CI [6.82, 8.04]}, and MG {8.67 ± 1.39, 95% CI [8.11, 9.23]} maintained their improvements. Notably, the LMG group exhibited the largest and most sustained decrease, reaching the lowest SA level at T2 {5.41 ± 1.40, 95% CI [4.86, 5.96]}. In contrast, a significant main effect of Group (F(3,96) = 23.60, η² = 0.37, p < 0.001) suggested different overall levels of SA across groups. Post-hoc comparisons confirmed that at both T1 and T2, all intervention groups scored significantly lower than the control group (p < 0.05). Furthermore, the LMG group had significantly lower SA scores than both DG and MG at T1 and T2 (p < 0.05), the difference between DG and MG did not reach statistical significance and the LMG showed the greatest magnitude of reduction and demonstrated a more continuous and sustained improvement over time, indicating a superior effect of the combined intervention.
At baseline (T0), the four groups did not differ significantly in fear of negative evaluation (FNE) scores (p > 0.05), indicating comparable initial levels {CG: 6.14 ± 1.59, 95% CI [15.63, 19.17]; LG: 6.76 ± 2.05, 95% CI [15.24, 18.68]; MG: 6.71 ± 1.90, 95% CI [15.42, 19.14]; LMG: 6.05 ± 2.36, 95% CI [15.36, 18.96]}. A significant Group × Time interaction was observed (F(6,192) = 3.72, η² = 0.94, p < 0.01), indicating that changes in FNE scores over time differed among groups, and therefore simple effect analyses were conducted. The main effect of Time was also significant (F(2,192) = 34.49, η² = 0.37 p < 0.001), with overall FNE scores decreasing from T0 to T1 and T2. From T0 to T1, the control group showed no meaningful change (p > 0.05), whereas LG {4.43 ± 1.72, 95% CI [11.93, 14.55]}, MG {4.52 ± 1.12, 95% CI [13.20, 16.00]}, and LMG {6.05 ± 2.36, 95% CI [10.45, 12.43]} demonstrated significant reductions (all p < 0.05). This improvement pattern persisted at T2: the control group remained stable(p > 0.05), while LG {4.43 ± 1.72, 95% CI [11.73, 14.19]} and MG {4.52 ± 1.12, 95% CI [12.91, 15.57]} continued to maintain lower scores. Notably, the LMG group exhibited the largest and most sustained reduction, reaching the lowest FNE level at T2 {3.67 ± 1.24, 95% CI [9.46, 11.34]}. In addition, a significant main effect of Group was found (F(3,96) = 11.90, η² = 0.24, p < 0.001), suggesting overall group differences in FNE levels. Post-hoc comparisons showed that at both T1 and T2, all intervention groups scored significantly lower than the control group (p < 0.05). Moreover, the LMG group had significantly lower FNE scores than both DG and MG at T1 and T2 (p < 0.05), indicating that the combined intervention produced the greatest and most enduring improvements over time.
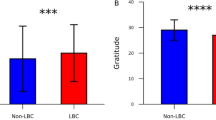
At baseline (T0), the four groups did not differ significantly in social avoidance (SAD) scores (p > 0.05), indicating comparable starting points {CG: 4.76 ± 1.30, 95% CI [11.78, 15.26]; LG: 4.81 ± 2.02, 95% CI [11.16, 14.12]; MG: 4.86 ± 1.42, 95% CI [12.35, 15.17]; LMG: 5.05 ± 1.50, 95% CI [11.98, 14.82]}. A significant Group × Time interaction was detected (F(6,192) = 3.19, η² = 0.15, p < 0.01), indicating that the trajectories of SAD scores differed among groups, and thus simple effect analyses were conducted. The main effect of Time was also significant (F(2,192) = 19.82, η² = 0.26, p < 0.01), with overall SAD scores decreasing from T0 to T1 and T2. From T0 to T1, the control group showed no meaningful improvement (p > 0.05), whereas LG {3.76 ± 1.14, 95% CI [9.20, 11.20]}, MG {3.86 ± 1.35, 95% CI [10.72, 12.80]}, and LMG {3.19 ± 1.12, 95% CI [8.00, 9.28]} demonstrated significant reductions (all p < 0.05). This pattern remained consistent at T2: the control group stayed relatively stable (p > 0.05), while LG {3.48 ± 1.21, 95% CI [8.94, 10.90]} and MG {3.76 ± 1.30, 95% CI [10.43, 12.53]} maintained decreased levels. Most notably, the LMG group achieved the lowest SAD score at T2 {2.76 ± 0.94, 95% CI [7.39, 8.77]}, showing the most pronounced and sustained reduction. Furthermore, the main effect of group was significant (F(3,96) = 8.08, η² = 0.15, p < 0.001), indicating overall differences among groups. Post-hoc analyses confirmed that at T1 and T2, all intervention groups scored significantly lower than the control group (p < 0.05). In addition, the LMG group had significantly lower SAD scores than both DG and MG at T1 and T2 (p < 0.05), demonstrating that the combined intervention yielded the strongest and most persistent improvements in social avoidance.(See Table 2; Fig. 5).

Effects of different interventions on Social Anxiety.
Discussion
Interpretation of findings
This study aimed to evaluate the effects of Latin dance and mindfulness interventions on social anxiety among left-behind adolescents in rural China. The results demonstrated that three interventions significantly reduced social anxiety symptoms compared to the control condition. These improvements were sustained at follow-up. Importantly, the combined intervention group showed the most pronounced reductions in anxiety, outperforming both the Latin dance-only and mindfulness-only groups.
Comparison with previous literature
Latin dance has been recognized as an effective approach to promoting psychological well-being, as its integration of rhythmic movement, music, and self-expression can alleviate stress and enhance mood and engagement19,33,34. Consistent with these findings, our study also observed immediate reductions in social anxiety following the Latin dance intervention. Nevertheless, similar to previous school-based studies reporting improvements in self-efficacy and peer connectedness18,19. our results also indicated enhanced social interaction and engagement among participants in the Latin dancegroup, which may serve as short-term protective factors against social anxiety. However, unlike prior studies that reported relatively sustained benefits, we found that the effects of Latin dancediminished at follow-up. This discrepancy may be due to differences in intervention duration, the absence of ongoing practice, or the heightened academic pressure faced by rural adolescents, suggesting that Latin dancealone may not produce lasting changes without continued support.
Mindfulness-based interventions (MBIs) have shown efficacy in reducing cognitive reactivity and improving emotional regulation by promoting non-judgmental awareness of internal experiences35.Prior research has demonstrated reductions in rumination and negative self-referential thinking, as well as improvements in self-esteem and anxiety regulation36,37. Our findings partially align with this literature: the mindfulness group exhibited moderate reductions insocial anxiety, supporting the role of attentional regulation and emotional awareness. However, the effects in our study were smaller than those reported in many adult samples, which may reflect developmental differences in cognitive maturity and the need for age-appropriate adaptations. This reinforces concerns about the direct transferability of adult-based mindfulness protocols to adolescents and highlights the importance of tailoring MBIs for younger populations.
Importantly, our combined intervention (mindfulness + dance) produced the most significant and sustained improvements, exceeding the effects of either modality alone. The superior outcomes observed in the combined intervention group may be attributed to a synergistic effect of mindfulness and Latin dance, which operate through distinct yet complementary pathways. At the psychological level, Latin dance offers a socially engaging and emotionally evocative context in which adolescents can actively apply mindfulness skills. By maintaining present-moment awareness during dance activities, participants are better able to stay grounded, reduce self-critical thoughts, and manage anxiety in real-time social interactions. Conversely, mindfulness enhances awareness of bodily sensations and emotional states, which may increase confidence, expressiveness, and interpersonal attunement during dance. This reciprocal facilitation promotes emotion regulation, improves social functioning, and strengthens self-efficacy. From a neurobiological perspective, the integration of physical movement and cognitive focus may activate complementary mechanisms. Aerobic exercise such as Latin dance increases endorphin levels, enhances cerebral blood flow, and promotes the release of neurotrophins like brain-derived neurotrophic factor (BDNF), thereby supporting neural plasticity and brain health38,39,40. Mindfulness, in turn, regulates the stress response system and modulates neural circuits involved in emotion regulation and attentional control35,41,42. Evidence from animal studies further suggests that both physical exercise and mental training independently promote hippocampal neurogenesis, while their combination yields additive effects on neuronal proliferation and integration39,40,41. Taken together, these psychological and neurobiological mechanisms may explain why combining mindfulness with Latin dance produces greater improvements in social anxiety than either intervention alone. The synergistic effects observed in this study extend previous literature and provide novel evidence that a multimodal intervention may be particularly effective for addressingsocial anxiety in left-behind adolescents in rural contexts.
Practical implications
These findings have important practical implications. First, they support the use of low-cost, school-based interventions in rural areas where mental health services are scarce. Integrating physical activity with psychological training appears culturally acceptable and feasible in these settings. Second, the success of the combined intervention offers a model for linking physical education with social–emotional learning in school curricula, promoting more holistic development. Third, this approach may help address mental health disparities among left-behind adolescents, who face unique emotional challenges due to parental absence.
Practically, schools can incorporate brief mindfulness exercises to improve emotional regulation and structured Latin dance sessions to enhance engagement, motivation, and peer connection. The combined model provides an adaptable and scalable framework for educators and policymakers, enabling rural schools to support resilience, reduce psychological distress, and sustain academic motivation within existing resources.
Limitations
This study has several limitations. (I) the sample consisted solely of left-behind adolescents with elevated social anxiety from a single rural region in China. The geographic, cultural, and demographic homogeneity of the sample limits the external validity of the findings. Because left-behind adolescents experience unique socio-emotional stressors due to prolonged parental absence, the observed intervention effects may not fully generalize to urban youth, adolescents from non–left-behind families, or individuals in other cultural contexts. (II) All psychosocial variables were assessed using self-report questionnaires. Although researchers provided instructions and supervision, social anxiety is associated with self-criticism, avoidance, and social desirability bias, which may have influenced participants’ responses and affected data accuracy and internal validity. In addition, relying solely on self-report measures limits the ability to capture behavioral or physiological manifestations of anxiety. Future studies should therefore consider incorporating multi-method assessment approaches—such as parent or teacher reports, behavioral observations, or physiological indicators—to obtain a more comprehensive understanding of adolescents’ anxiety profiles. (III) The age range of the sample was relatively narrow and primarily limited to early adolescence, which restricts developmental representativeness. Future studies should include a broader age range to examine whether different developmental stages exhibit differential responsiveness to mindfulness- and dance-based interventions. (V) all participants exhibited elevated levels of social anxiety, which enhances internal validity but limits understanding of the interventions’ applicability to general or subclinical populations. Including typically developing adolescents or individuals with varying levels of social anxiety in future research would help determine the broader.
although the sample demonstrates adequate statistical power and provides valuable insights into a specific regional context, its restriction to a single county in Hunan Province limits the generalizability of the results. Future research incorporating samples from diverse socioeconomic regions across China would help verify the broader applicability of the findings.
Conclusion
Overall, the findings demonstrate that both Latin dance and mindfulness interventions produced reductions in social anxiety among left-behind adolescents; however, the magnitude and sustainability of their effects differed. Latin dance led to relatively rapid improvements in social anxiety symptoms, likely due to its socially engaging and emotionally stimulating nature, but these effects tended to diminish over time. Mindfulness training also reduced social anxiety, particularly by enhancing emotional awareness and regulation, yet the immediate impact was modest. In contrast, the combined intervention yielded the most substantial and enduring improvements, suggesting a synergistic effect in which the experiential social context of Latin dance and the internal regulatory skills of mindfulness mutually reinforce one another. These results indicate that integrating body-based and cognitive-emotional approaches may offer a more comprehensive and sustainable strategy for alleviating social anxiety in left-behind adolescents.
Data availability
Research data will be available from the corresponding author with a reasonable request.
References
National Bureau of Statistics of China. Report on the Monitoring Survey of Migrant Workers 2022 [J/OL] http://www.stats.gov.cn/
World Health Organization. Adolescent mental health: Fact sheet [J/OL] https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health
Jessar, A. J. et al. Emotional clarity as a mechanism linking emotional neglect and depressive symptoms during early adolescence. J. Early Adolescence. 37 (3), 414–432 (2017).
Hamilton, J. L. et al. Emotional maltreatment, peer victimization, and depressive versus anxiety symptoms during adolescence: hopelessness as a mediator. J. Clin. Child. Adolesc. Psychol. 42 (3), 332–347 (2013).
Gibb, B. E., Abramson, L. Y. & Alloy, L. B. Emotional maltreatment from parents, verbal peer victimization, and cognitive vulnerability to depression. Cogn. Therapy Res. 28, 1–21 (2004).
Gibb, B. E. & Abela, J. R. Emotional abuse, verbal victimization, and the development of children’s negative Inferential styles and depressive symptoms. Cogn. Therapy Res. 32, 161–176 (2008).
Stirling, J. Jr. & Amaya-Jackson, L. Understanding the behavioral and emotional consequences of child abuse. Pediatrics 122(1), 667 (2008).
Schwerdtfeger, K. L. et al. Intergenerational transmission of trauma: the mediating role of parenting styles on toddlers’ DSM-related symptoms. J. Aggress. Maltreatment Trauma. 22 (2), 211–229 (2013).
Rapee, R. M. & Heimberg, R. G. A cognitive-behavioral model of anxiety in social phobia. Behav. Res. Ther. 35 (8), 741–756 (1997).
Holas, P. et al. The relationship between self-esteem and self-compassion in socially anxious. Curr. Psychol. 42 (12), 10271–10276 (2023).
Salari, N. et al. Global prevalence of social anxiety disorder in children, adolescents and youth: A systematic review and meta-analysis. J. Prev. 45 (5), 795–813 (2024).
Tang, X. et al. Prevalence of social anxiety disorder and symptoms among Chinese children, adolescents and young adults: A systematic review and meta-analysis. Front. Psychol. 13, 792356 (2022).
Koch, S. C. et al. Fixing the mirrors: A feasibility study of the effects of dance movement therapy on young adults with autism spectrum disorder. Autism 19 (3), 338–350 (2015).
Quiroga Murcia, C. et al. Shall we dance? An exploration of the perceived benefits of dancing on well-being. Arts Health. 2 (2), 149–163 (2010).
Esmail, A. et al. Effects of dance/movement training vs. aerobic exercise training on cognition, physical fitness and quality of life in older adults: A randomized controlled trial. J. Bodyw. Mov. Ther. 24 (1), 212–220 (2020).
Liu, X., Soh, K. G. & Omar Dev, R. D. Effect of Latin dance on physical and mental health: a systematic review. BMC public. Health. 23 (1), 1332 (2023).
Aguiñaga, S. & Marquez, D. X. Impact of Latin dance on physical activity, cardiorespiratory fitness, and sedentary behavior among Latinos attending an adult day center. J. Aging Health. 31 (3), 397–414 (2019).
Marquez, D. X. et al. BAILA: A randomized controlled trial of Latin dancing to increase physical activity in Spanish-speaking older Latinos. Ann. Behav. Med. 56 (12), 1231–1243 (2022).
Zheng, C. & Ji, H. Analysis of the intervention effect and self-satisfaction of sports dance exercise on the psychological stress of college students. Work 69 (2), 637–649 (2021).
Bishop, S. R. et al. Mindfulness: A proposed operational definition. Clin. Psychol. Sci. Pract. 11 (3), 230 (2004).
Kabat-Zinn, J. Mindfulness-based interventions in context: past, present, and future (2003).
Baer, R. A. Mindfulness training as a clinical intervention: a conceptual and empirical review. Clin. Psychol. Sci. Pract. 10 (2), 125 (2003).
Shapiro, S. L. et al. Mechanisms of mindfulness. J. Clin. Psychol. 62 (3), 373–386 (2006).
Semple, R. J. & Lee, J. Mindfulness-based Cognitive Therapy for Anxious Children: A Manual for Treating Childhood Anxiety (New Harbinger, 2007).
Wells, A. & Matthews, G. Modelling cognition in emotional disorder: the S-REF model. Behav. Res. Ther. 34 (11–12), 881–888 (1996).
Kuyken, W. et al. Effectiveness of the mindfulness in schools programme: non-randomised controlled feasibility study. Br. J. Psychiatry. 203 (2), 126–131 (2013).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences (Routledge, 2013).
Zoogman, S. et al. Mindfulness interventions with youth: A meta-analysis. Mindfulness 6 (2), 290–302 (2015).
Biddle, S. J. & Asare, M. Physical activity and mental health in children and adolescents: a review of reviews. Br. J. Sports Med. 45 (11), 886–895 (2011).
Zenner, C., Herrnleben-Kurz, S. & Walach, H. Mindfulness-based interventions in schools—a systematic review and meta-analysis. Front. Psychol. 5, 603 (2014).
La Greca, A. M. et al. Development of the social anxiety scale for children: reliability and concurrent validity. J. Clin. Child Psychol. 17 (1), 84–91 (1988).
Wang, X., Wang, X. & Ma, H. Hamilton depression rating Scale. In Handbook of mental health rating scales, Expanded Edition, 220–223 (Chinese Journal of Mental Health Press, 1999).
Qi, J. Investigation and analysis of the influence of sports dance based on wireless network mode on college students’mental health. Revista Brasileira De Med. Do Esporte. 27, 70–72 (2021).
Banio, A. The influence of Latin dance classes on the improvement of life quality of elderly people in Europe. Sustainability 12 (6), 2155 (2020).
Goldin, P. R. & Gross, J. J. Effects of mindfulness-based stress reduction (MBSR) on emotion regulation in social anxiety disorder. Emotion 10 (1), 83 (2010).
Nilsson, J. et al. Acute increases in brain-derived neurotrophic factor in plasma following physical exercise relates to subsequent learning in older adults. Sci. Rep. 10 (1), 4395 (2020).
Fabel, K. et al. Additive effects of physical exercise and environmental enrichment on adult hippocampal neurogenesis in mice. Front. NeuroSci. 3, 994 (2009).
Tait, J. L. et al. Influence of sequential vs. simultaneous dual-task exercise training on cognitive function in older adults. Front. Aging Neurosci. 9, 368 (2017).
Hötting, K. & Röder, B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehavioral Reviews. 37 (9), 2243–2257 (2013).
Shors, T. J. et al. Use it or lose it: how neurogenesis keeps the brain fit for learning. Behav. Brain. Res. 227 (2), 450–458 (2012).
Koszycki, D. et al. Randomized trial of a meditation-based stress reduction program and cognitive behavior therapy in generalized social anxiety disorder. Behav. Res. Ther. 45 (10), 2518–2526 (2007).
Goldin, P., Ramel, W. & Gross, J. Mindfulness meditation training and self-referential processing in social anxiety disorder: behavioral and neural effects. J. Cogn. Psychother. 23 (3), 242–257 (2009).
Funding
This research was funded by The National Educational Science Planning Project of China (Grant Number BLA230102).
Author information
Authors and Affiliations
Contributions
X.D. and Q.Y. contributed equally to the conceptualization, methodology, data collection, and original draft preparation. C.L. and Y.S. provided supervision, contributed to data interpretation, and were responsible for reviewing and editing the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ding, X., Yang, Q., Sun, Y. et al. Effects of dance mindfulness and combined interventions on social anxiety in left behind rural adolescents: a randomized controlled trial. Sci Rep 16, 5468 (2026). https://doi.org/10.1038/s41598-026-35039-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-35039-x
