
Abstract
Stroke, as the second leading cause of death globally, is characterized by high disability and mortality rates and urgently needs biomarkers for risk stratification. This study aims to use data from the China Health and Retirement Longitudinal Study (CHARLS) cohort to explore the association of the uric acid to HDL-C ratio (UHR), BMI with incident stroke. A total of 3756 participants aged 45 and above without a history of stroke were included from the CHARLS data from 2011 to 2020. Stroke events were confirmed through follow up data. UHR was calculated as the ratio of serum uric acid (mg/dL) to high density lipoprotein cholesterol (mg/dL). Statistical methods such as the Cox proportional hazards regression model, restricted cubic spline analysis, mediation effect test (Bootstrap method), and and multiplicative and additive interactions analysis were used to systematically evaluate the association of the combined UHR and BMI indicators with stroke risk. The UHR was significantly associated with stroke risk (HR = 1.03, p = 0.005), with the highest UHR group having 1.61 times the risk of the lowest group (p = 0.003). Subgroup analysis indicated that this association was significant in the non-diabetic population (p < 0.001) but not in the diabetic population (interaction p = 0.002). UHR mediated 18% of the association between BMI and stroke risk (95% CI 6.7–38%). No significant multiplicative and additive interactions were found between BMI and UHR on incident stroke.Restricted cubic spline analysis showed an approximately linear dose–response relationship between UHR and stroke risk (p for non linearity = 0.917). The study results indicate that UHR is significantly and positively correlated with stroke risk, and its value in stroke risk stratification is significantly enhanced when used in combination with BMI.
Similar content being viewed by others

Introduction
Stroke, as the second leading cause of death globally, is characterized by high disability and mortality rates1,2. Stroke is defined as acute focal injury to the central nervous system caused by vascular reasons, resulting in neurological deficits3. Most strokes are ischemic, caused by reduced blood flow, usually due to arterial occlusion. A rarer type of ischemic stroke is venous infarction caused by cerebral venous or sinus obstruction. The remaining 10–40% of strokes are hemorrhagic, caused by rupture of cerebral arteries4. The adverse prognosis and long-term family burden caused by stroke make it crucial to fully understand and identify risk factors for effective prevention strategies.
Recently, a novel composite lipid marker, the uric acid to high density lipoprotein cholesterol ratio (UHR), has gained recognition for its remarkable accuracy in predicting a range of diseases, including obesity5, hypertension6, and cardiovascular disease (CVD)7. Uric acid (UA) and HDL-C represent two key pathways: pro oxidative endothelial damage and vascular protection, respectively. UA induces oxidative stress and vascular endothelial damage via the xanthine oxidase pathway, while HDL-C exerts atherosclerosis protective effects through reverse cholesterol transport and anti-inflammatory actions8. Combining UA and HDL-C into the UA/HDL-C ratio (UHR) can simultaneously quantify the redox imbalance constituted by these two antagonistic pathways7, and the predictive ability of UHR for stroke risk needs further exploration.
Obesity is considered one of the most important modifiable risk factors for ischemic stroke, and obesity indicators represented by BMI can reflect chronic systemic inflammation caused by adipose tissue9; when combined with UHR, BMI provides dual “exposure vulnerability” information, which is expected to further improve the precision of stroke risk stratification.
The CHARLS databases, covering 28 provinces nationwide, has longitudinal biospecimens and medically verified stroke endpoints from 2011 to 2020, providing an ideal real world data platform to explore the association between UHR and stroke and to evaluate the joint association of the UHR and BMI combined index with stroke10.In summary, this study aims to investigate the associations between UHR, BMI, UHR and BMI, and stroke risk to perform risk stratification and provide a scientific basis for the early identification of high-risk populations for stroke and the development of personalized intervention strategies.
Method
Our study analyzed data from the CHARLS databases. The CHARLS database, a large scale, prospective national cohort, randomly selects participants via a multi-stage stratified probability sampling design across 450 communities in 150 counties of 28 Chinese provinces to ensure national representation. Trained staff collected baseline data through face to face interviews from June 2011 to March 2012 (Wave 1). Socio demographic and health factors were assessed biennially via standardized questionnaires. Initially, Wave 1 recruited 17,708 participants, with subsequent follow ups in 2013 (Wave 2), 2015 (Wave 3), 2018 (Wave 4), and 2020 (Wave 5)10.
Cohort selection and criteria
This study employed a cohort design, using data from participants initially enrolled in 2011 as baseline. We included individuals aged 45 who had no history of stroke diseases. Further exclusion was carried out based on the following criteria:
-
(1)
missing data on UA,HblA1c,LDL-C,or HDL—C;
-
(2)
lack of information regarding diabetes or hypertension history;
-
(3)
missing details on age, education, smoking, marital and reproductive status, or alcohol consumption history;
-
(4)
exclusion of those who did not complete stroke history.
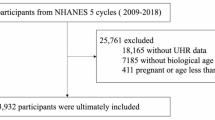
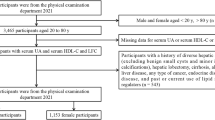
After these inclusion and exclusion steps, 5608 participants were left for subsequent analysis.Furthermore, due to incomplete follow up data in CHARLS, an additional exclusion was performed, leaving 3756 participants in CHARLS for the final analysis. The detailed results are presented in Fig. 1.

Flowchart of subject selection. Note:CHARLS, China Health and Retirement Longitudinal Study; UA, uric acid; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
Data collection and definitions
Interviewers administered questionnaires to collect and record sociodemographic information (gender and age), health related behaviors (smoking and alcohol use), and medical history (stroke, diabetes, and hypertension). Trained professionals conducted anthropometric measurements, including height, weight, and blood pressure. During blood pressure measurement using an electronic sphygmomanometer, three readings of systolic (SBP) and diastolic blood pressure (DBP) were taken, and the average was recorded. Participants provided fasting venous blood samples in the morning, which were analyzed for glucose (glu), HbA1c, and low—density lipoprotein cholesterol (LDL—C).
The UHR was calculated as (UA/HDL-C)*100%, UA and HDL—C levels were measured in mg/dL.
Diabetes was diagnosed based on glu ≥ 126 mg/dL, HbA1c ≥ 6.5%, a physician’s diagnosis, or current use of hypoglycemic medication. Hypertension was defined as SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, a physician’s diagnosis, or current use of antihypertensive medication11.
Statistical analysis
Continuous variables are presented as mean and standard deviation, and categorical variables as numbers and percentages. One way ANOVA or chi square tests were used to compare variable differences across UHR quartiles. For Cox regression, our analysis involved three models: Model 1 was unadjusted; Model 2 adjusted for gender, age, smoking, alcohol consumption, and place of residence; and Model 3 further adjusted for hypertension history, diabetes history and LDL—C based on Model 2.
To explore the potential nonlinear relationship between UHR and stroke risk, we performed a restricted cubic spline (RCS) analysis using the rms package in R. The optimal number of knots was selected by comparing models with 3, 4, and 5 knots based on the Akaike Information Criterion (AIC). The model with 3 knots (placed at the 10th, 50th, and 90th percentiles of the UHR distribution) was chosen as it yielded the smallest AIC. The resulting spline function was incorporated into a Cox proportional hazards model adjusted for gender, age, smoking, alcohol consumption, place of residence, hypertension history, diabetes history, and LDL-C (Model 3).
To explore whether BMI modifies the association between the UHR and incident stroke, we performed stratified analyses within three BMI strata: < 24.0 kg/m2, 24.0–27.9 kg/m2, and ≥ 28.0 kg/m214. Participants were further divided into twelve cross classified groups according to these BMI strata and UHR quartiles, using the group with BMI < 24.0 kg/m2 and UHR in quartile 1 as the common reference; hazard ratios (HRs) and 95% confidence intervals (CIs) for stroke were estimated for each group.
Multiplicative interaction was evaluated by including a product term (BMI stratum × UHR quartile) in the Cox model; the HR for this term quantifies the magnitude of departure from multiplicativity. Additive interaction was assessed with three complementary metrics: relative excess risk due to interaction (RERI), attributable proportion (AP), and the synergy index (SI). RERI = 0, AP = 0, and SI = 1 indicate no additive interaction. RERI > 0, AP > 0, and SI > 1 denote a synergistic effect, implying that the combined influence of BMI and UHR exceeds the sum of their individual contributions. Conversely, RERI < 0, AP < 0, and SI < 1 suggest an antagonistic interaction. Delta method derived 95% CIs were computed for RERI, AP, and SI12.
Subsequently, mediation analysis based on Cox regression was employed to examine the mediating role of UHR in the relationship between BMI and stroke. The mediation models included the same adjustment covariates as Model 3: gender, age, smoking, alcohol consumption, place of residence,diabetes,hypertension and LDL-C.The total, indirect, and direct effects were assessed using the bootstrap method with 1,000 resamples. The bootstrap method, a nonparametric statistical technique, is utilized in mediation analysis to evaluate the significance of indirect effects13. All statistical analyses were conducted using R (v4.3.1) with the following key packages: survival , rms, and mediation,msm etc.,with a significance level set at p < 0.05.
Result
Baseline characteristics
Table 1 presents the baseline characteristics of the 3,756 participants stratified by UHR quartiles. Participants with higher UHR were more likely to be male, reside in urban areas, and have higher levels of education, BMI, and LDL-C. The prevalence of traditional cardiometabolic risk factors, including hypertension, diabetes, and histories of smoking and alcohol consumption, increased significantly across ascending UHR quartiles (all p for trend < 0.001).
Association of UHR and BMI with Incident Stroke
In Cox proportional hazards models (Table 2), both continuous UHR and BMI showed significant, positive associations with stroke risk after full adjustment for demographic and clinical confounders (Model 3). For each 1% increase in UHR, the risk of stroke increased by 3% (HR = 1.03, 95% CI 1.01–1.05, p = 0.005). Similarly, each 1 kg/m2 increase in BMI was associated with a 4% higher stroke risk (HR = 1.04, 95% CI 1.03–1.07, p < 0.001). When analyzed by quartiles, participants in the highest UHR quartile (Q4) had a 1.61 fold greater risk of stroke compared to those in the lowest quartile (Q1) (95% CI 1.18–2.21, p = 0.003).
Subgroup analyses
Stratified analyses revealed a significant interaction between UHR and diabetes status on stroke risk (p for interaction = 0.002, Fig. 2). The positive association between UHR and stroke was strong and significant in non diabetic individuals (p < 0.001) but was attenuated and non significant in those with diabetes (p = 0.653). UHR remained significantly associated with stroke risk in subjects without kidney disease (HR = 1.031, 95% CI 1.008–1.054, p = 0.008). In subjects with kidney disease, the association was attenuated and not statistically significant (HR = 1.028, 95% CI 0.932–1.133, p = 0.583). A formal test for interaction between UHR and kidney disease status was not statistically significant (p for interaction = 0.580).No significant interactions were observed with other covariates, including BMI strata, suggesting the UHR and stroke association is consistent across different levels of obesity.

Subgroup and interaction analyses of the association between UHR and stroke Note: Forest plot shows hazard ratios (HRs) per 1% increase in UHR. Analyses were adjusted for age, sex, smoking, alcohol, and residence. The dashed vertical line indicates the reference (HR = 1.0). P for interaction is shown for diabetes status. Abbreviations: UHR, uric acid to HDL-C ratio; CI, confidence interval.
Dose response relationship
Restricted cubic spline analysis confirmed an approximately linear relationship between UHR and the log hazard of stroke (p for non-linearity = 0.917, Fig. 3). The risk of stroke increased steadily across the range of UHR values without evidence of a threshold or plateau effect.

RCS regression analysis on the relationship between UHR and stroke Note: Solid line and shaded area represent the adjusted HR and 95% CI from restricted cubic spline (RCS) analysis with 3 knots. The dashed horizontal line indicates the reference (HR = 1.0). P for nonlinearity = 0.917.
Joint effects and interaction between BMI and UHR
We found no evidence of significant multiplicative or additive interaction between BMI categories and UHR quartiles on stroke risk (Table 3, all interaction p values > 0.05). However, their joint effects were evident (Fig. 4). Compared to the reference group (BMI < 24 kg/m2 and UHR Q1), individuals in the highest risk group (BMI ≥ 28 kg/m2 and UHR Q4) had a substantially elevated stroke risk (HR = 1.88, 95% CI 1.23–2.87).

Interacting and joint effects of UHR and BMI on stroke risk. Note: HRs are shown for cross-classified groups. The reference group (Ref.) is BMI < 24 kg/m2 and UHR Q1. Analyses were adjusted for age, sex, smoking, alcohol, residence, hypertension, diabetes, and LDL-C. Abbreviations: BMI, body mass index; Q, quartile.
Mediating role of UHR
Mediation analysis using a bootstrap approach indicated that UHR explained a significant proportion of the association between BMI and stroke. Specifically, UHR mediated 18.0% (95% CI 6.7%—38.0%) of the total effect of BMI on stroke risk (Fig. 5).

Mediating Effect of UHR in the Relationship Between BMI and Strok Note: Path diagram showing the total, direct, and indirect effects. Proportion mediated (18.0%) was calculated via the bootstrap method. All paths were adjusted for age, sex, smoking, alcohol, and residence.
Discussion
This study, based on a nationally representative cohort of middle-aged and older Chinese individuals, is the first to demonstrate an independent positive correlation between the UHR and stroke, and to identify that UHR mediates 18% of the effect of BMI on stroke risk. Compared with previous studies that examined UA or HDL-C individually, UHR, a simple and easily obtainable indicator, integrates pro oxidative and pro inflammatory loads, offering a more integrated measure of risk than single components.
The study found significant associations between UHR, BMI, and stroke risk, with a gradient increase in stroke incidence across UHR quartiles (Table 2), consistent with the findings of several previous studies14,15,16. UHR exhibits an approximately linear dose response relationship with stroke. As UHR increases, UA mediated endothelial dysfunction, oxidative stress, and activation of inflammatory pathways13 rise, while the anti-inflammatory, endothelial-protective, and antioxidant properties of HDL-C weaken17,18. This dynamic interplay between oxidative stress and lipid protection increases the likelihood of stroke occurrence.
The point estimates suggest potential heterogeneity in the strength of the UHR-stroke association across kidney disease status, which may parallel findings in diabetes. In patients with kidney disease, stroke risk is likely driven more prominently by direct factors such as uremic toxins, severe hypertension, mineral-bone disorders, and systemic inflammation, which may diminish the relative contribution of the metabolic imbalance reflected by UHR. However, given the markedly wider 95% confidence interval and the non-significant interaction test in the kidney disease subgroup, we believe this lack of significant effect modification is at least partly attributable to the limited sample size and lower statistical power within this subgroup, making it difficult to detect a statistically significant effect even if a biological difference exists. Additionally, there was an interaction effect between UHR and diabetes status in the Cox regression for stroke. The p-value was not significant in the group with diabetes, possibly due to “dysfunctional HDL.” HDL undergoes non-enzymatic glycation and oxidative modifications, forming “dysfunctional HDL” that loses its antioxidant/anti-inflammatory capabilities. In this case, HDL-C no longer represents vascular protection levels, which may diminish the relevance of the UHR ratio. The increased ratio no longer reflects the imbalance between “damage” and “protection”19. Moreover, empagliflozin, a first line treatment for diabetes, has been shown to lower UA levels20. Additionally, because individuals with diabetes already have high levels of oxidative stress, the UA/HDL-C ratio may be overshadowed by other more dangerous signals21. Beyond dysfunctional HDL and medication effects, several other factors warrant consideration when interpreting the attenuated association between UHR and stroke in individuals with diabetes. First, the treatment status and specific pharmacotherapy in this population are potential major confounders. Commonly prescribed medications for diabetes and its comorbidities, such as urate lowering agents, statins, and antihypertensive drugs , could directly alter serum levels of UA or HDL-C, thereby distorting the UHR value and its link to underlying vascular pathology22,23,24,25.Second,the pathophysiology of stroke in diabetes may involve more pronounced non atherosclerotic mechanisms (e.g., cerebral small vessel disease) where the UA/HDL-C imbalance, primarily reflecting atherosclerotic propensity, plays a less dominant role26,27,28.These factors may contribute to the non significant p value, suggesting that the UHR and stroke association is stronger in non diabetic populations (stages 0–2), whereas in diabetes, risk stratification may require functional HDL testing or direct oxidative stress markers for accurate risk stratification.
Mediation analysis revealed that UHR mediated 18.0% (95% CI 6.7–38.0%) of the BMI–stroke risk, confirming the pathway “obesity → UA/HDL imbalance → vascular damage → stroke.” Some studies have indicated that a higher BMI is associated with increased hepatic lipase activity, which promotes the breakdown of HDL-C into apolipoprotein A1 and smaller HDL-C particles, thereby leading to a decrease in HDL-C levels29. Another report suggests that the accelerated degradation of HDL-C may be caused by the chronic inflammatory state in patients with high BMI30. On the other hand, higher levels of BMI also alter the function of HDL-C, including reducing its anti-inflammatory effects, weakening its antioxidant and protective effects on endothelial cells, and diminishing cholesterol reverse transport31,32,33.This may explain that higher levels of BMI may be associated with an increased risk of stroke through reducing HDL-C, while obesity may elevate UA by increasing purine metabolism and insulin-mediated renal UA reabsorption34. Therefore, obesity may lead to an increase in UHR by affecting both UA and HDL-C.
Importantly, our study found that UHR still has independent association after adjusting for BMI. One analysis study found that elevated BMI has a causal relationship with decreased HDL-C but no significant effect on stroke risk, which may explain why UHR remains significant after adjusting for BMI35.
Thus, UHR can serve as both a mediator and an independent risk indicator. The combined model simultaneously covers the direct effects of obesity and indirect metabolic effects, and this dual role supports the utility of combining UHR and BMI for risk assessment.
At the same time, we also conducted an indepth study of the potential interaction between BMI and UHR. The experimental results showed that there was no significant synergy or interaction between the two in terms of stroke risk. That is to say, although both BMI and UHR can independently affect stroke risk36,37, and there is even a mediating effect, the combined effect of the two does not exceed the sum of their individual effects. This may be related to the multifactorial nature of stroke. Stroke may be associated with a variety of etiological factors, such as metabolism, genetics, hypertension, diet, etc38, and involves multiple pathways such as neuroinflammation and immune suppression39,40. The complex mechanistic effects of BMI and UHR on stroke may be caused by different factors and pathways, and further research is needed to clarify this.
Conclusion
In this large, prospective cohort of middle-aged and older Chinese adults, we found that a higher UHR was independently associated with an increased long term risk of stroke. A significant interaction was observed with diabetes status, wherein this positive association was evident in non diabetic individuals but not in those with diabetes. The association between UHR and stroke was consistent in direction across different categories of BMI, with no statistically significant effect modification observed. Furthermore, UHR explained approximately 18% of the association between BMI and stroke risk, suggesting a partial mediating role. When used in combination, UHR and BMI provided complementary information for stroke risk stratification. These findings highlight UHR as a readily available biomarker that may be useful for stroke risk assessment, particularly in non-diabetic populations, and its combination with BMI could enhance risk stratification in clinical practice. Further research is needed to validate these associations and explore their utility in diverse populations.
Limitation
However, several limitations exist in this study. First, although longitudinal follow up data are available, baseline UA and HDL-C were measured only once, which cannot rule out regression dilution bias caused by long term fluctuations. Future studies should use multiple measurements to elucidate the dynamic changes of UHR and the causal direction with stroke risk. Second, stroke events were self reported by participants or proxies, lacking CT/MRI imaging and neurologist review, which may introduce recall and diagnostic biases. Future research should incorporate objective imaging and standardized classification. Third, potential confounders such as diet, physical activity, renal function, and medication use (e.g., specific UA lowering, lipid modifying and Antidiabetic drugs) were not fully quantified, and residual confounding may still exist. Future studies should collect more detailed lifestyle and medication information. Fourth, the subgroup sample sizes were limited, especially in the interaction analyses involving diabetes and obesity, where the number of events was small, leading to less stable effect estimates. Consequently, although we observed a consistent direction of association between UHR and stroke across BMI strata, the non-significant interaction test should be interpreted with caution, and these findings require validation in larger cohorts. Fifth, the risk associations reported, while adjusted for key confounders, were derived from a single cohort without internal or external validation, which may affect the stability and generalizability of the exact effect estimates. Sixth,in this study, we confirmed that the vast majority of subjects had a UHR below 30, with only 10 cases exceeding 30. However, the UA and HDL-C values in these cases were within measurable physiological ranges and were not laboratory errors or implausible ratios. To preserve valid observational data and avoid selection bias, we did not artificially remove these data points. Nonetheless, the association between UHR > 30 and stroke should be interpreted with caution. Finally, as our analysis is observational, causal inferences between UHR, BMI, and stroke cannot be definitively established.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request. All data generated or analysed during this study are included in this published article.
References
Krishnamurthi, R. V., Ikeda, T. & Feigin, V. L. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: A systematic analysis of the global burden of disease study 2017. Neuroepidemiology 54, 171–179 (2020).
GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 18, 439–458 (2019).
Sacco, R. L. et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American heart association/American stroke association. Stroke 44, 2064–2089 (2013).
Campbell, B. C. V. & Khatri, P. Stroke. Lancet 396, 129–142 (2020).
Wang, Y. et al. Associations of serum uric acid to high-density lipoprotein cholesterol ratio with trunk fat mass and visceral fat accumulation. Diabetes Metab. Syndr. Obes. Targets Ther. 17, 121–129 (2024).
Ahari, R. K. et al. Association of atherosclerosis indices, serum uric acid to high‐density lipoprotein cholesterol ratio and triglycerides‐glucose index with hypertension: A gender‐disaggregated analysis. J. Clin. Hypertens. 26, 645–655 (2024).
Cui, Y. & Zhang, W. Long-term cardiovascular risk and mortality associated with uric acid to HDL-C ratio: A 20-year cohort study in adults over 40. Sci. Rep. 15, 14242 (2025).
Kittelson, K. S., Junior, A. G., Fillmore, N. & da Silva Gomes, R. Cardiovascular-kidney-metabolic syndrome—An integrative review. Prog. Cardiovasc. Dis. 87, 26–36 (2024).
Yumuk, V. et al. European guidelines for obesity management in adults. Obes. Facts. 8, 402–424 (2015).
Zhao, Y., Hu, Y., Smith, J. P., Strauss, J. & Yang, G. Cohort profile: The China health and retirement longitudinal study (CHARLS). Int. J. Epidemiol. 43, 61–68 (2014).
Jiang, L. et al. Non-linear associations of atherogenic index of plasma with prediabetes and type 2 diabetes mellitus among Chinese adults aged 45 years and above: A cross-sectional study from CHARLS. Front. Endocrinol. 15, 1360874 (2024).
Huo, R.-R., Liao, Q., Zhai, L., You, X.-M. & Zuo, Y.-L. Interacting and joint effects of triglyceride-glucose index (TyG) and body mass index on stroke risk and the mediating role of TyG in middle-aged and older Chinese adults: A nationwide prospective cohort study. Cardiovasc. Diabetol. 23, 30 (2024).
Kanbay, M. et al. The role of uric acid in the pathogenesis of human cardiovascular disease. Heart 99, 759–766 (2013).
Zhong, C., Zhong, X., Xu, T., Xu, T. & Zhang, Y. Sex-specific relationship between serum uric acid and risk of stroke: A dose-response meta-analysis of prospective studies. J. Am. Heart. Assoc. 6, e005042 (2017).
Jiang, Q. et al. Serum uric acid to high-density lipoprotein cholesterol ratio is associated with stroke in the elderly: A population-based study. Front. Neurol. 16, 1594080 (2025).
Zhu, T., He, Y. & Bei, E. Increased uric acid to high-density lipoprotein ratio positively correlated with stroke risk. Front. Neurol. 16, 1577077 (2025).
Nofer, J.-R. et al. HDL and arteriosclerosis: Beyond reverse cholesterol transport. Atherosclerosis 161, 1–16 (2002).
Pammer, A. et al. Impaired HDL antioxidant and anti-inflammatory functions are linked to increased mortality in acute heart failure patients. Redox. Biol. 76, 103341 (2024).
Rye, K.-A. Biomarkers associated with high-density lipoproteins in atherosclerotic kidney disease. Clin. Exp. Nephrol. 18, 247–250 (2014).
You, Y., Zhao, Y., Chen, M., Pan, Y. & Luo, Z. Effects of empagliflozin on serum uric acid level of patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 15, 202 (2023).
Matsunaga, T. et al. Glycated high-density lipoprotein regulates reactive oxygen species and reactive nitrogen species in endothelial cells. Metabolism 52, 42–49 (2003).
Aktas, G. et al. Poorly controlled hypertension is associated with elevated serum uric acid to HDL-cholesterol ratio: A cross-sectional cohort study. Postgrad. Med. 134, 297–302 (2022).
Kim, S. C. et al. Clinical and health care use characteristics of patients newly starting allopurinol, febuxostat, and colchicine for the treatment of gout. Arthritis Care Res. (Hoboken) 65, 2008–2014 (2013).
Cao, J. Y. et al. Uric acid predicts long-term cardiovascular risk in type 2 diabetes but does not mediate the benefits of fenofibrate: The FIELD study. Diabetes Obes. Metab. 22, 1388–1396 (2020).
Theofilis, P., Tsimihodimos, V., Vordoni, A. & Kalaitzidis, R. G. Serum uric acid levels and cardiometabolic profile in middle-aged, treatment-naïve hypertensive patients. High Blood Press. Cardiovasc. Prev. 29, 367–374 (2022).
Chen, R., Ovbiagele, B. & Feng, W. Diabetes and stroke: Epidemiology, pathophysiology, pharmaceuticals and outcomes. Am. J. Med. Sci. 351, 380–386 (2016).
Ruan, Z. & Zhao, J. Differential ischemic stroke risk linked to novel subtypes of type 2 diabetes: Insights from a Mendelian randomization analysis. Endocrine 84, 980–988 (2024).
Kong, X. et al. Relationship of admission uric acid to high density lipoprotein cholesterol ratio with unfavorable prognosis among acute ischemic stroke patients. Lipids Health. Dis. 24, 381 (2025).
Wang, P. et al. Perivascular adipose tissue-derived visfatin is a vascular smooth muscle cell growth factor: Role of nicotinamide mononucleotide. Cardiovasc. Res. 81, 370–380 (2009).
Badellino, K. O., Wolfe, M. L., Reilly, M. P. & Rader, D. J. Endothelial lipase concentrations are increased in metabolic syndrome and associated with coronary atherosclerosis. PLoS. Med. 3, e22 (2006).
Hahn, B. H. et al. Pro-inflammatory high-density lipoproteins and atherosclerosis are induced in Lupus-prone mice by a high-fat diet and leptin. Lupus 19, 913–917 (2010).
Sorrentino, S. A. et al. Endothelial-vasoprotective effects of high-density lipoprotein are impaired in patients with type 2 diabetes mellitus but are improved after extended-release niacin therapy. Circulation 121, 110–122 (2010).
Sasahara, T., Yamashita, T., Sviridov, D., Fidge, N. & Nestel, P. Altered properties of high density lipoprotein subfractions in obese subjects. J. Lipid Res. 38, 600–611 (1997).
Ford, E. S., Li, C., Cook, S. & Choi, H. K. Serum concentrations of uric acid and the metabolic syndrome among US children and adolescents. Circulation 115, 2526–2532 (2007).
Holmes, M. V. et al. Causal effects of body mass index on cardiometabolic traits and events: A mendelian randomization analysis. Am. J. Hum. Genet. 94, 198–208 (2014).
Liu, X. et al. A J-shaped relation of BMI and stroke: Systematic review and dose-response meta-analysis of 4.43 million participants. Nutr. Metab. Cardiovasc. Dis. 28, 1092–1099 (2018).
Wang, X. et al. The relationship between body mass index and stroke: A systemic review and meta-analysis. J. Neurol. 269, 6279–6289 (2022).
Moskowitz, M. A., Lo, E. H. & Iadecola, C. The science of stroke: Mechanisms in search of treatments. Neuron 67, 181–198 (2010).
Anrather, J. & Iadecola, C. Inflammation and stroke: An overview. Neurotherapeutics 13, 661–670 (2016).
Brea, D. Post-stroke immunosuppression: Exploring potential implications beyond infections. Eur. J. Neurosci. 58, 4269–4281 (2023).
Acknowledgements
We thank the China Health and Retirement Longitudinal Study, CHARLS for providing the data and the selfless contributions of all participants.
Funding
This research was supported by Science and Technology Planning Project of Yunnan Provincial Department of Science and Technology.[grant numbers:202401AY070001-108],Open Project of the Clinical Medical Research Center, The First People’s Hospital of Yunnan Province[grant numbers: 2023YJZX-LN09].
Author information
Authors and Affiliations
Contributions
Shan Li—Conceptualization; Funding acquisition; Data curation; Formal analysis; Investigation; Project administration; Resources; Supervision; Validation; Visualization; Writing—original draft. Jie Liu—Methodology; Software; Formal analysis; Validation; Visualization; Writing—original draft. Kui Zhang—Data curation; Investigation; Formal analysis; Validation; Visualization; Writing—original draft. Kai Zhao—Data curation; Investigation; Software; Validation; Writing—review & editing. Yan Li—Investigation; Resources; Validation; Writing—review & editing. Hangyu Ma—Investigation; Resources; Validation; Writing—review & editing. Yutao Fu—Investigation; Resources; Validation; Writing—review & editing. Jianzhun Chen—Conceptualization; Methodology; Project administration; Supervision; Resources; Validation; Writing—review & editing. Qianhao Zhao—Conceptualization; Methodology; Project administration; Supervision; Resources; Validation; Writing—review & editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Each participant in CHARLS cohort which was conducted under Peking University’s ethics review committee gave their informed permission before taking part (IRB00001052-11015). In addition, the Declaration of Helsinki was followed during our research. The necessary standards and legislation were followed in the execution of all procedures, including the declarations in “Declarations” section.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, S., Liu, J., Zhang, K. et al. Association of serum uric acid to high density lipoprotein cholesterol ratio with stroke. Sci Rep 16, 11565 (2026). https://doi.org/10.1038/s41598-026-41894-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-41894-5
