
Abstract
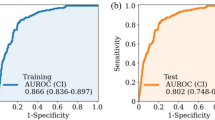
Accurate prediction of tracheostomy after craniotomy for supratentorial intracerebral hemorrhage (sICH) remains challenging. This study aimed to develop, externally validate, and interpret a machine learning model for individualized risk prediction. A retrospective multicenter cohort was constructed, including 738 patients from Weifang People’s Hospital and 186 from Weifang Hospital of Traditional Chinese Medicine who underwent craniotomy between January 2017 and December 2024. Predictor variables were screened using least absolute shrinkage and selection operator (LASSO) and multivariate logistic regression. Logistic regression, random forest, and extreme gradient boosting (XGBoost) models were trained with repeated 10-fold cross-validation and assessed for discrimination, calibration, and clinical utility. Five key predictors were identified: Glasgow Coma Scale, age, hematoma volume, operative time, and serum bicarbonate. In external validation, XGBoost demonstrated the most balanced and robust performance, with an AUROC of 0.86 and a Brier score of 0.15, and showed superior net benefit on decision curve analysis. SHapley Additive exPlanations confirmed clinical plausibility, and a web-based dynamic nomogram was developed for individualized prediction. This explainable XGBoost model provides reliable and interpretable estimation of postoperative tracheostomy risk, facilitating evidence-based perioperative decision-making and resource allocation in neurocritical care.
Similar content being viewed by others

Data availability
The datasets analyzed during the current study are not publicly available due to institutional data-use regulations and patient confidentiality policies. De-identified data and analytic code are available from the corresponding author upon reasonable request and approval by the participating institutions.
References
Bösel, J. Use and Timing of Tracheostomy After Severe Stroke. Stroke 48, 2638–2643 (2017).
Lais, G. & Piquilloud, L. Tracheostomy: Update on why, when and how. Curr. Opin. Crit. Care 31, 101–107 (2025).
Premraj, L. et al. Tracheostomy timing and outcome in critically ill patients with stroke: A meta-analysis and meta-regression. Crit. Care 27, 132 (2023).
Kurtz, P. et al. How does care differ for neurological patients admitted to a neurocritical care unit versus a general ICU?. Neurocrit. Care 15, 477–480 (2011).
Pelosi, P. et al. Management and outcome of mechanically ventilated neurologic patients. Crit. Care Med. 39, 1482–1492 (2011).
Steidl, C. et al. Tracheostomy, extubation, reintubation: Airway management decisions in intubated stroke patients. Cerebrovasc. Dis. 44, 1–9 (2017).
Abulhasan, Y. B., Teitelbaum, J., Al-Ramadhani, K., Morrison, K. T. & Angle, M. R. Functional outcomes and mortality in patients with intracerebral hemorrhage after intensive medical and surgical support. Neurology 100, e1985–e1995 (2023).
Hoffman, H., Jalal, M. S. & Chin, L. S. Prediction of mortality after evacuation of supratentorial intracerebral hemorrhage using NSQIP data. J. Clin. Neurosci. 77, 148–156 (2020).
Ho, U.-C., Hsieh, C.-J., Lu, H.-Y., Huang, A.-H. & Kuo, L.-T. Predictors of extubation failure and prolonged mechanical ventilation among patients with intracerebral hemorrhage after surgery. Respir. Res. 25, 19 (2024).
Hu, X. et al. Surgical outcomes from haematoma evacuation for intracerebral haemorrhage in the INTERACT3 study. Lancet Reg. Health - Western Pac. 62, 101669 (2025).
Yu, Z. et al. Chinese multidisciplinary guideline for management of hypertensive intracerebral hemorrhage. Chin. Med. J. (Engl.) 135, 2269–2271 (2022).
Schönenberger, S., Al-Suwaidan, F., Kieser, M., Uhlmann, L. & Bösel, J. The SETscore to predict tracheostomy need in cerebrovascular neurocritical care patients. Neurocrit. Care 25, 94–104 (2016).
Szeder, V., Ortega-Gutierrez, S., Ziai, W. & Torbey, M. T. The TRACH score: Clinical and radiological predictors of tracheostomy in supratentorial spontaneous intracerebral hemorrhage. Neurocrit. Care 13, 40–46 (2010).
Rass, V. et al. Factors associated with prolonged mechanical ventilation in patients with subarachnoid hemorrhage—the RAISE score*. Crit. Care Med. 50, 103 (2022).
Chen, X.-Y. et al. A nomogram for predicting the need of postoperative tracheostomy in patients with aneurysmal subarachnoid hemorrhage. Front. Neurol. 12, 711468 (2021).
Zhang, Z. et al. Prediction of microvascular obstruction from angio-based microvascular resistance and available clinical data in percutaneous coronary intervention: An explainable machine learning model. Sci. Rep. 15, 3045 (2025).
Ballı, M., Dogan, A. E., Senol, S. H. & Eser, H. Y. Machine learning based identification of suicidal ideation using non-suicidal predictors in a university mental health clinic. Sci. Rep. 15, 13843 (2025).
Lundberg, S. M. & Lee, S. I. A unified approach to interpreting model predictions. in Advances in Neural Information Processing Systems vol. 30Curran Associates, Inc., (2017).
Lundberg, S. M. et al. From local explanations to global understanding with explainable AI for trees. Nat Mach Intell 2, 56–67 (2020).
Collins, G. S., Reitsma, J. B., Altman, D. G. & Moons, K. G. M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 162, 55–63 (2015).
Collins, G. S. et al. Protocol for development of a reporting guideline (TRIPOD-AI) and risk of bias tool (PROBAST-AI) for diagnostic and prognostic prediction model studies based on artificial intelligence. BMJ Open 11, e048008 (2021).
Jr, D. W. H., Lemeshow, S. & Sturdivant, R. X. Applied Logistic Regression (Wiley, 2013).
Breiman, L. Random forests. Mach. Learn. 45, 5–32 (2001).
Chen, T., Guestrin, C. & XGBoost: A scalable tree boosting system. in Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining 785–794Association for Computing Machinery, New York, NY, USA, (2016). https://doi.org/10.1145/2939672.2939785
Riley, R. D. et al. Calculating the sample size required for developing a clinical prediction model. BMJ 368, m441 (2020).
Collins, G. S., Ogundimu, E. O. & Altman, D. G. Sample size considerations for the external validation of a multivariable prognostic model: A resampling study. Stat. Med. 35, 214–226 (2016).
Torrini, F. et al. Prediction of extubation outcome in critically ill patients: A systematic review and meta-analysis. Crit. Care 25, 391 (2021).
Asehnoune, K. et al. Extubation success prediction in a multicentric cohort of patients with severe brain injury. Anesthesiology 127, 338–346 (2017).
Namen, A. M. et al. Predictors of successful extubation in neurosurgical patients. Am. J. Respir. Crit. Care Med. 163, 658–664 (2001).
Thille, A. W. et al. Risk factors for and prediction by caregivers of extubation failure in ICU patients: A prospective study. Crit. Care Med. 43, 613–620 (2015).
El Solh, A. A., Bhat, A., Gunen, H. & Berbary, E. Extubation failure in the elderly. Respir. Med. 98, 661–668 (2004).
Lai, C.-C. et al. Establishing predictors for successfully planned endotracheal extubation. Medicine 95, e4852 (2016).
Lehmann, F. et al. Prolonged mechanical ventilation in patients with deep-seated intracerebral hemorrhage: Risk factors and clinical implications. J. Clin. Med. 10, 1015 (2021).
Cai, Y.-H., Wang, H.-T. & Zhou, J.-X. Perioperative predictors of extubation failure and the effect on clinical outcome after infratentorial craniotomy. Med. Sci. Monit. 22, 2431–2438 (2016).
Cheng, H. et al. Prolonged operative duration is associated with complications: A systematic review and meta-analysis. J. Surg. Res. 229, 134–144 (2018).
Boniatti, V. M. C. et al. The modified integrative weaning index as a predictor of extubation failure. Respir. Care 59, 1042–1047 (2014).
Clark, P. A., Inocencio, R. C. & Lettieri, C. J. I-TRACH: Validating a tool for predicting prolonged mechanical ventilation. J. Intensive Care Med. 33, 567–573 (2018).
Al-Ali, A. H. et al. Independent risk factors of failed extubation among adult critically ill patients: A prospective observational study from Saudi Arabia. Saudi J. Med. Med. Sci. 12, 216–222 (2024).
Chang, Y.-C. et al. Ventilator dependence risk score for the prediction of prolonged mechanical ventilation in patients who survive sepsis/septic shock with respiratory failure. Sci. Rep. 8, 5650 (2018).
Maier, I. L. et al. Predictive factors for the need of tracheostomy in patients with large vessel occlusion stroke being treated with mechanical thrombectomy. Front. Neurol. 12, 728624 (2021).
Young, D., Harrison, D. A., Cuthbertson, B. H., Rowan, K. & TracMan Collaborators, F. T. Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: The TracMan randomized trial. JAMA 309, 2121 (2013).
Catalino, M. P. et al. Early versus late tracheostomy after decompressive craniectomy for stroke. J. Intensive Care 6, 1 (2018).
Chen, W. et al. Timing and outcomes of tracheostomy in patients with hemorrhagic stroke. World Neurosurg. 131, e606–e613 (2019).
Bösel, J. et al. Stroke-related early tracheostomy versus prolonged orotracheal intubation in neurocritical care trial (SETPOINT). Stroke 44, 21–28 (2013).
Bösel, J. et al. Effect of early vs standard approach to tracheostomy on functional outcome at 6 months among patients with severe stroke receiving mechanical ventilation: The SETPOINT2 randomized clinical trial. JAMA 327, 1899–1909 (2022).
Acknowledgements
The authors sincerely thank the Department of Neurosurgery teams at Weifang People’s Hospital and Weifang Hospital of Traditional Chinese Medicine for their valuable assistance in data management and case verification.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
F.Q. and Q.Li conceived and designed the study. F.Q. and X.X. collected and curated the clinical data. F.Q. performed data preprocessing, feature selection, model development, visualization, and web deployment. F.Q. drafted the manuscript. H.Y., Y.C., D.T., Y.W., and Q.Liu contributed to manuscript revision. Q.Li supervised the project, interpreted the findings, and critically revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Qiao, F., Xue, X., Yu, H. et al. Explainable machine learning prediction of tracheostomy after craniotomy for supratentorial intracerebral hemorrhage. Sci Rep (2026). https://doi.org/10.1038/s41598-026-41953-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-026-41953-x
