
Abstract
This prospective multicenter study examined the incidence, risk factors, and recovery course of C5 palsy after surgery for cervical ossification of the posterior longitudinal ligament in 482 patients treated at 28 institutions between 2015 and 2017. C5 palsy was defined as a postoperative decline of at least one grade in deltoid MMT strength. Overall, 6.0% of patients developed C5 palsy, with notable variation by surgical procedure: 4.0% after anterior decompression and fusion, 4.6% after laminoplasty, and 11.8% after posterior decompression and fusion. Nearly half of the affected patients developed symptoms on the day of surgery, and deltoid strength dropped from a mean of 4.7 preoperatively to 2.3 at onset. Over the following two years, 81% of patients regained their preoperative motor function. Better outcomes were observed in younger individuals and in those without concurrent biceps brachii weakness, whereas older patients and those with multimuscle involvement showed less favorable recovery. These findings clarify the expected clinical course of C5 palsy after OPLL surgery and highlight patient factors that may help guide prognosis and perioperative counseling.
Similar content being viewed by others


Introduction
Ossification of the posterior longitudinal ligament (OPLL) is a condition where abnormal bone forms within the spinal ligament, leading to compression of the spinal cord and nerve root. The pathophysiology of OPLL is multifactorial and involves genetic, metabolic, and environmental factors that drive ectopic bone formation. Treatment options for OPLL include both conservative and surgical approaches, with the choice depending on symptoms, severity, spinal cord compression and spinal alignment. Surgery is generally recommended for patients with neurological symptoms classified as progressive and/or moderate or above.
Surgical management of cervical OPLL includes anterior, posterior, and combined approaches, each with distinct advantages and risks. The optimal procedure is tailored to each patient’s anatomy and disease severity, balancing the need for effective decompression with the risk of complications. Compared with other cervical spine surgeries, surgery for cervical OPLL is associated with a relatively high rate of complications. The risk and type of complications can vary depending on whether an anterior or posterior surgical approach is used. Common complications, which can occur in any surgical procedure, include neurological deficits, dural tears with cerebrospinal fluid leaks, implant or graft issues, infection, and C5 palsy.
C5 palsy is a complication characterized by weakness of the deltoid and biceps brachii muscles, which sometimes occurs after posterior cervical surgeries but can also occur after anterior cervical surgeries. C5 palsy is known to be transient but can be permanent. There have been several reports of C5 palsy related to cervical spondylotic myelopathy; however, few reports have specifically focused on OPLL, and thus, clear evidence is lacking. This study focused on the prevalence of C5 palsy following OPLL surgery and aimed to prospectively examine the pathological patterns, risk factors, and detailed clinical course of C5 palsy using a nationwide large-scale Japanese OPLL database.
Methods
This study was conducted in accordance with the principles of the Declaration of Helsinki, and was approved by the internal review boards at all participating sites and the internal review board overseeing the Data Management Center (IRB No. M2019-272). Informed consent was obtained from all individual participants included in the study. The clinical information was collected using an electronic data capture (EDC) system created with FileMaker (Claris International, Inc., US) (Supplementary Fig. 1).
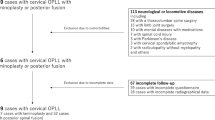
This multi-institutional investigation of surgery for cervical OPLL was performed on the basis of data from the Japanese Multicenter Research Organization for Ossification of the Spinal Ligament. This study was approved by all 28 institutions belonging to the Japanese Multicenter Research Organization for Ossification of the Spinal Ligament. A total of 482 patients with cervical OPLL who underwent surgery were prospectively registered between April 2015 and July 2017. The occurrence of and risk factors for C5 palsy were analyzed in all of these patients.
Of the 482 patients, 403 patients (83.6%) who could be followed for at least 2 years were included in this study. Patients who had a history of cervical surgery and who experienced neurological disturbances owing to disc herniation, infection, trauma, or spondylosis were excluded.
C5 palsy was defined as a case in which the postoperative manual muscle test (MMT) score for the unilateral deltoid muscle was at least one point lower than the preoperative score, regardless of the degree of biceps brachii muscle weakness. Patient information included age, sex, body mass index (BMI), comorbidities, duration of symptoms, and Japanese Orthopedic Association (JOA) cervical myelopathy score1. Imaging findings included the ossification type on X-ray, the C2–7 angle, the ossification occupation ratio, the K-line2 (Fig. 1), and the T2 high-signal intensity in the spinal cord on MRI; for patients with C5 palsy, the MMT scores for the biceps brachii, triceps brachii, wrist extensors, wrist flexors, finger flexors, and finger extensors as well as the deltoid muscle were examined at seven time points (preoperatively, at the time of onset, at discharge, 3 months, 6 months, 1 year, and 2 years postoperatively). The surgical information, surgical procedure, number of vertebrae operated on, and surgical vertebral level was also investigated. Imaging findings were evaluated by expert spine surgeons at each facility.

Radiological parameters. (a) C2-7 angle. (b) Representative images of K-line (−) and K-line (+).
Statistical analysis was performed using SPSS Statistics, version 24 (IBM Corp., Chicago, IL). Mann–Whitney U test, the chi-squared test and Fisher’s exact test were used to perform a statistical univariate analysis of the risk factors for the occurrence of and poor recovery from C5 palsy. Multivariate logistic regression analysis was performed on items that had a P value of less than 0.2 in univariate analysis to determine risk factors for C5 palsy. Given the observational nature of this study and the limited number of C5 palsy events (n = 29), a parsimonious multivariable logistic regression model was used to reduce overfitting. Covariates were selected a priori to account for key domains that may confound procedure selection and C5 palsy risk, including OPLL severity (occupation ratio), anatomical severity distribution (most stenotic level), baseline alignment (preoperative C2–7 angle), and surgical extent (number of operated segments), together with surgical procedure (PDF). As a sensitivity analysis, the longitudinal MMT recovery curve was additionally summarized after categorizing patients by post-palsy management (any intervention vs. no intervention). Because interventions were not protocolized and the number of cases was limited, these analyses were considered exploratory and were not intended to estimate treatment effects. To assess robustness to inter-institutional variability across 28 centers, we additionally fitted an institution-clustered generalized estimating equation (GEE) logistic model with an independent working correlation structure and a robust (sandwich) covariance estimator. All the data are expressed as the means ± standard deviations. A P value < 0.05 was considered to indicate a statistically significant difference.
Results
The patients’ demographic data are shown in Table 1. There were 357 male patients (74.1%) and 125 female patients (25.9%), with an average age of 64.5 years. The average BMI was 25.7 kg/m2, and the average disease duration was 42.1 months. The average preoperative JOA score was 10.5 points. Imaging findings revealed an average C2–7 angle of 9.9 degrees and an average C2–7 range of motion (ROM) of 26.6 degrees. The average occupation ratio at the maximum stenosis site was 46.8%, and the average thickness of the ossified lesions was 5.6 mm. The K-line (-) was present in 156 patients (32.4%), and T2 hyperintensity (HIZ) was observed in 414 patients (85.9%).
The surgical procedures used were anterior decompression and fusion (ADF) in 99 patients (20.5%), laminoplasty (LAM) in 261 patients (54.1%), posterior decompression and fusion (PDF) in 110 patients (22.8%), and anterior-posterior (A-P) in 12 patients (2.5%). The average number of vertebral levels involved in surgery was 3.1.
C5 palsy was observed in 29 patients (6.0%). In the univariate analysis, the C3/4 level, which was the most stenotic on the preoperative MRI, had a significantly higher rate in the C5 palsy group (125/453 vs. 13/29, p = 0.047) (Table 2). Age (64.5 ± 11.6 vs. 64.1 ± 12.1 years, p = 0.87), male sex (74.4% vs. 69.0%, p = 0.52), BMI (25.6 ± 4.3 vs. 26.5 ± 4.2 kg/m2, p = 0.30), disease duration (42.6 ± 63.4 vs. 32.4 ± 37.8 months, 0.40), the presence of comorbidities (78.1% vs. 79.3, p = 1), the preoperative JOA score (10.5 ± 3.0 vs. 10.6 ± 2.8, p = 0.98), and number of surgical vertebrae (3.8 ± 1.3 vs. 4.1 ± 1.0, p = 0.19) did not significantly differ between the groups. When the imaging findings were compared, the occupation ratio (43.4 ± 15.7 vs. 49.3 ± 15.8, p = 0.053), C2-7 ROM (26.7 ± 13.8 vs. 23.7 ± 13.3, p = 0.26), C2-7 angle (10.1 ± 11.6 vs. 5.9 ± 12.1, p = 0.059), K-line (-) (32.7% vs. 27.6%, p = 0.57), and MRI T2 HIZ (85.9% vs. 86.2%, p = 1) did not significantly differ between the groups. When categorized by surgical procedure, the incidence of C5 palsy was 4 cases (4.0%) in the ADF group, 12 cases (4.6%) in the LAM group, 13 cases (11.8%) in the PDF group, and 0 cases (0%) in the A-P group. The incidence rate of C5 palsy was significantly higher in the PDF group (p = 0.019). Multivariate analysis of the PDF procedure, ossification occupation ratio, preoperative C2-7 angle, C3/4 as the most stenotic level, and number of operated segments revealed that only the PDF procedure was a significant risk factor for C5 palsy (p = 0.032) (Table 3). Sensitivity analyses using stricter definitions (MMT ≤ 3 and a ≥ 2-grade drop in deltoid MMT) yielded incidences of 5.0% and 4.4%, respectively, and showed directionally consistent associations, with posterior decompression and fusion remaining significant under the MMT ≤ 3 definition (Supplementary Table S1).
The date of C5 palsy onset was on the day of surgery in 14 patients (48%), followed by postoperative day (POD) 1 (2 patients), POD 2 (4 patients), POD 3 (4 patients), POD 4 (2 patients), POD 5 (1 patient), POD 7 (1 patient), and POD 17 (1 patient) (Fig. 2). The incidence of C5 palsy on the day of surgery was 75% in the ADF group, 33% in the LAM group, and 64% in the PDF group (Table 4).

Onset timing of C5 palsy.
Intraoperative monitoring was performed in 19 out of 29 cases of C5 palsy. Of these, four showed signal alternation during surgery. Of these, two showed signs of C5 palsy immediately after surgery, one showed two days after surgery, and one showed three days after surgery.
Conservative treatment involving rest was chosen for C5 palsy patients, except in one case where additional surgery was performed. Among these cases, six received steroid administration and four underwent hyperbaric oxygen therapy.
The mean preoperative MMT score for the deltoid muscle was 4.7 ± 0.84 points, whereas the score at the time of onset was 2.3 ± 0.88 points. The decrease in MMT score for the biceps muscle was observed in 18 out of 26 patients with C5 palsy (69%). The subsequent temporal course of MMT scores (deltoid and biceps muscles) was as follows: at the time of worsening (2.3 ± 0.88, 2.8 ± 1.0), 3 months postoperatively (3.4 ± 1.2, 4.0 ± 0.94), 6 months postoperatively (3.8 ± 1.3, 4.2 ± 1.0), 1 year postoperatively (4.2 ± 1.1, 4.4 ± 1.0), and 2 years postoperatively (4.5 ± 0.99, 4.6 ± 0.76) (Fig. 3). Twenty-one patients (81%) recovered to their preoperative level. One patient (3.8%) remained below an MMT score of 3 for either the deltoid or biceps muscle at the final follow up.

Longitudinal recovery of patients with C5 palsy.
Among the 26 patients with C5 palsy who completed 2-year follow-up, post-palsy management was heterogeneous. Sixteen patients received no additional intervention, whereas 10 patients received at least one intervention, including steroid administration (n = 6) and hyperbaric oxygen therapy (HBO; n = 4), with one overlapping case, and one patient underwent reoperation. To explore whether these co-interventions materially affected the observed recovery pattern, we descriptively compared longitudinal MMT trajectories between patients with any intervention and those without (Supplementary Figure S2). At 2 years, complete recovery was observed in 12/16 (75%) patients without intervention and 9/10 (90%) patients with intervention, without a statistically significant difference (Fisher’s exact test, p = 0.6169).
When comparing the fully recovered group and the non-fully recovered group, the decreases in the MMT score for the deltoid muscle at the worst stage were 2.8 ± 0.84 and 2.3 ± 1.0, respectively, with no significant difference. On the other hand, in terms of biceps brachii muscle strength, biceps brachii muscle weakness was observed concurrently in 13 of 21 patients (62%) in the recovery group, whereas it was observed in all 5 patients in the nonrecovery group. In other words, all 8 patients who did not exhibit biceps brachii muscle weakness recovered to preoperative levels. There was a significant difference in age at onset between the fully recovered and nonfully recovered groups (60.5 ± 11.7 vs. 74.0 ± 9.0, p = 0.023) (Table 5). At 2 years postsurgery, complete recovery from palsy was achieved in 100% of the patients in the ADF group, 72% of the patinets in the LAM group, and 82% of the patients in the PDF group (Table 4). Prognostic modeling for non-full recovery was underpowered due to the small number of poor-recovery cases, and prediction thresholds require validation in larger independent cohorts.
For the 21 patients who achieved complete recovery, the final recovery time was at discharge (23 ± 15.2 days postoperatively) in seven patients, six months postoperatively in eight patients, one year postoperatively in three patients, and two years postoperatively in three patients. The visual analogue scale (VAS) pain scores on upper limbs for the C5 palsy (-) and C5 palsy (+) groups were 60.6 ± 29.15 and 67.9 ± 26.7 before surgery, 37.7 ± 29.6 and 47.8 ± 35.9 at 6 months after surgery, and 41.12 ± 32.81 and 46.6 ± 32.2 at 1 year after surgery. No significant differences were observed between these groups. 46.6 ± 32.2), and 2 years postoperatively (41.4 ± 30.1, 44.4 ± 33.3), with no significant difference observed in any group.
Sensitivity analyses using stricter definitions of C5 palsy (deltoid MMT ≤ 3 and a ≥ 2-grade decrease) yielded incidences of 5.0% (24/482) and 4.4% (21/482), respectively (vs. 6.0% [29/482] for the primary definition). In an institution-clustered GEE model with robust standard errors, point estimates were directionally consistent with the primary model; stenosis at C3/4 remained significant (OR 2.13, 95% CI 1.38–3.29), and the association for posterior decompression and fusion was attenuated to borderline significance (OR 2.71, 95% CI 0.99–7.44) (Supplementary Table S2).
Discussions
The present study prospectively investigated postoperative C5 palsy in 482 cases of cervical OPLL surgery. The incidence of C5 palsy was 6.0% (29 cases), with a significantly higher incidence observed in PDF (11.8%). 81% of C5 palsy patients showed improvement to preoperative levels; however, elderly patients exhibited a tendency towards poorer recovery. All C5 palsy patients who did not exhibit biceps brachii muscle weakness recovered to preoperative levels.
C5 palsy is a known complication following cervical spine surgery, with the reported incidence rate varying from 0.58% to 7.8% depending on the study population, surgical technique, and definition used3,4,5. A meta-analysis of 79 studies and 13,621 patients reported that the overall pooled prevalence of C5 palsy was 5.3% (95% CI 4.6–6.0%)6. Male patients and patients who undergo procedures involving posterior approaches (especially laminectomy and fusion) are reported to be at increased risk3,6,7. Other risk factors include OPLL, preexisting foraminal stenosis, and excessive spinal cord drift during surgery7,8. Most patients achieve full or partial recovery within 6 months, although severe cases may take longer9. Hofler et al. reported a median time to recovery of 2.0 months (IQR: 0.18–8.24 months)10, and Bydon et al. noted improvement within 3–6 months11. At present, clinical guidelines are lacking regarding the management of postoperative C5 palsy, and treatment strategies vary across surgeons and institutions12. In this multicenter cohort, postoperative management was not protocolized and was left to the treating surgeon; accordingly, most cases were managed conservatively, while adjunctive therapies or reoperation were used in selected patients.
Mechanical factors such as traction, compression, or tethering of the C5 nerve root during or after surgery are strongly implicated in the development of C5 palsy, which can result from foraminal stenosis, excessive posterior shift of the spinal cord after decompression, or intraoperative maneuvers such as shoulder depression, which increases tension on the C5 rootlets8,11,13,14. In anterior surgery, characteristic causes of C5 palsy include traction stress on the C5 nerve root due to enlargement of the intervertebral space, as well as relative traction on the C5 nerve root caused by anterior spinal cord displacement. In posterior surgery, causes include traction on the nerve root due to posterior spinal cord displacement, and foraminal stenosis caused by corrective fixation. Several studies have reported that a reduced foraminal diameter correlates with C5 palsy15,16, with Nakashima et al. reporting relative risks of 1.73 and 0.33 for cord shift and foramen width, respectively17. Additionally, chemical or ischemic injury to the anterior horn cells of the spinal cord at the C5 level, possibly due to preoperative ischemia and postoperative reperfusion, is another proposed mechanism9,13. In this study, the date of C5 palsy onset al.so ranged from the date of surgery to 17 days after surgery, suggesting that the cause of C5 palsy is multifactorial. Intraoperative neuromonitoring signal changes were recorded; however, interventional responses and management algorithms were not standardized across institutions, precluding analysis of the relationship between neuromonitoring-driven interventions and subsequent outcomes.
In this study, the degree of deltoid muscle weakness did not affect improvement in C5 palsy patients. This may be because this study focused specifically on OPLL. Multisegment involvement, less cervical lordosis, and smoking history are also reported as predictors of poor recovery from C5 palsy18,19. In this study, the mean age of the fully recovered group (60.5 years) was significantly younger than that of the nonfully recovered group (74.0 years). Although we did not evaluate sarcopenia or frailty, these unmeasured geriatric factors may have contributed to poorer recovery in older patients. It is understandable that elderly individuals have lower neural reserve capacity. The median time to recovery is often reported as 2 to 8 months, and the median time in this study was 6 months postoperatively. However, since 3 patients (12%) showed improvement even at 2 years postoperatively, longer-term observation is also important.
Recovery from C5 palsy may be associated with the occurrence of biceps brachii muscle weakness at onset. 28% of the patients with C5 palsy who also had biceps brachii muscle weakness at onset still had residual palsy at two years postoperatively. Biceps impairment suggests C6 nerve damage, and concomitant C5 palsy with bicipital impairment impairs both the C5 and C6 nerves, which could explain why compensatory recovery from deltoid impairment is inhibited. ADF resulted in complete recovery of C5 palsy in all patients, whereas LAM and ADF resulted in recovery rates of 72% and 82%, respectively. This may be due to residual anterior horn or nerve root damage because of insufficient resolution of anterior compression in posterior procedures. Additionally, spared spinal mobility after laminoplasty may hinder nerve recovery. C5 palsy is occasionally accompanied by pain; however, this study found no significant difference in upper limb VAS scores at 6 months post-surgery, suggesting that improvement may have occurred within 6 months. While some reports say that the prognosis of C5 palsy is worse when the initial motor weakness is more severe, this was not found to be the case in this study. Although the reason for this difference is unclear, the present study’s specific focus on OPLL, the inclusion of different surgical procedures, and its prospective nature may have contributed to the observed difference.
The incidence of C5 palsy after cervical surgery is greater in patients with OPLL (ranging from approximately 5.8% to 12.4%) than in patients without OPLL7,20,21. Increased postoperative cervical lordosis and marked anterior spinal cord compression at C3 are also associated with increased risk in patients with OPLL21,22. Kaneyama et al. reported that OPLL is a significant risk factor for postoperative C5 palsy (odds ratio: 43.8, P = 0.048)23. In the present study, C3/4 being the most stenotic level was identified as a risk factor for C5 palsy in univariate analysis. This result may suggest the involvement of a C5 medullary segment disorder present at the C3/4 level as one of the factors contributing to C5 palsy, but it may be attributable to PDF-related confounding factors.
Maki et al. reported that the incidence of C5 palsy is greater with laminectomy and fusion than with laminoplasty or anterior approaches24, which is compatible to the present study. The incidence of C5 palsy in the PDF (11.8%) group in this study also tended to be higher than that in the ADF (4.0%) or LAM (4.6%) groups. However, there may be confounding factors that were not included in this multivariate analysis, since the choice of surgical procedure was based on surgeons’ preferences. A comparison of posterior surgery with and without fixation revealed that C5 palsy tended to occur earlier in the PDF group (0.92 ± 1.2 days) than in the LAM group (3.6 ± 4.7 days) (p = 0.085). Although tethering of nerve roots can occur due to a posterior shift of the spinal cord after posterior decompression in both procedures25, foraminal stenosis associated with fixation may also occur in patients who undergo PDF26, which may explain the earlier occurrence. In this study, there was no difference in the angle of correction between the C5 palsy (-) and (+) group in PDF (-1.7 ± 9.9 vs. 3.0 ± 13.6, p = 0.284).
Prior OPLL-focused studies have predominantly evaluated postoperative C5 palsy in posterior decompression cohorts. In a prospective laminoplasty series, Kaneyama et al. reported that the presence of OPLL was associated with an increased likelihood of postoperative C5 palsy, suggesting that OPLL-related pathology may confer additional vulnerability of the C5 segment/root complex23. In an OPLL cohort undergoing posterior process-splitting laminoplasty, Li et al. further highlighted foraminal factors (e.g., C4/5 foraminal stenosis) and perioperative radiographic changes as potential contributors to C5 palsy27. Together, these OPLL-oriented datasets provide important mechanistic hypotheses; however, their procedure mix is largely limited to posterior approaches, which may constrain direct comparisons across contemporary surgical strategies. In contrast, the present nationwide prospective multicenter registry captured a broader spectrum of real-world surgical management for cervical OPLL, including a substantial proportion of anterior procedures in addition to posterior approaches. This wider procedure representation is a key strength of our study, allowing us to benchmark the incidence, onset timing, and longitudinal recovery of C5 palsy across different surgical strategies within a single prospective framework. While we could not directly test certain imaging-based hypotheses (e.g., standardized foraminal measurements), our findings complement posterior-dominant OPLL series by providing multicenter, approach-inclusive clinical trajectories and prognosis estimates.
Several limitations should be noted. Standardized imaging variables relevant to C5 palsy pathogenesis, such as quantitative C4/5 foraminal diameter/stenosis grading and pre-/postoperative foraminal changes were not prespecified or collected; therefore, we could not evaluate foraminal factors (including preoperative C4/5 foraminal stenosis) or directly test imaging-based mechanisms. Because procedure selection (ADF, LAM, and PDF) and post-palsy management were not randomized or protocolized across institutions, residual confounding (including confounding by indication) cannot be excluded; thus, the observed associations, including that between PDF and C5 palsy, should be interpreted as observational rather than causal. In addition, given the relatively low frequency of C5 palsy and the small number of non-fully recovered cases, prognostic analyses of recovery were underpowered. Furthermore, C5 palsy was defined as unilateral upper-limb palsy to reduce diagnostic confounding by major spinal cord injury; bilateral palsy and concomitant C6 involvement could not be fully assessed, and the prevalence of prophylactic foraminotomy was not systematically captured. Postoperative outcomes were assessed mainly using muscle strength (MMT) and pain scores without PROMs. Because the number of non-fully recovered cases was limited, the prognostic findings should be interpreted as exploratory, and validation in larger cohorts is warranted. Finally, excluding patients with prior cervical surgery or concurrent neuropathies may limit generalizability, and the small numbers of circumferential/combined procedures and ADF with supplemental posterior fixation precluded evaluating their potential preventive effects on C5 palsy. Future prospective OPLL cohorts incorporating PROMs will be important to quantify patient-perceived disability and quality of life in relation to C5 palsy.
This is the largest prospective study of OPLL surgery cases to date, with a C5 palsy incidence rate of 6.0%, which is comparable to previous reports. C5 palsy tends to occur more frequently in patients with OPLL who undergo PDF and should be considered in the preoperative evaluation. The recovery rate to preoperative levels was 81%, which is comparable to reports of C5 palsy in cervical spondylotic myelopathy, but there was no correlation between muscle weakness and the recovery rate. Importantly, the prognosis of C5 palsy in elderly individuals may also be poor. C5 palsy improved over time after onset, and some patients continued to improve even after six months, highlighting the need for long-term follow-up.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.
References
Hirabayashi, K. et al. Expansive open-door laminoplasty for cervical spinal stenotic myelopathy. Spine 8, 693–699. https://doi.org/10.1097/00007632-198310000-00003 (1983).
Fujiyoshi, T. et al. A New Concept for Making Decisions Regarding the Surgical Approach for Cervical Ossification of the Posterior Longitudinal Ligament: The K-Line. Spine 33 (2008).
Oh, J. K. et al. Epidemiology of C5 palsy after cervical spine surgery: a 21-center study. Neurospine 16, 558 (2019).
Onuma, H. et al. Identifying Factors for Predicting Postoperative Segmental Motor Paralysis in Patients Undergoing Anterior Cervical Spine Surgery: A Multicenter Study. Spine 50 (2025).
Nagoshi, N. et al. Comparison of Surgical Outcomes After Open- and Double-Door Laminoplasties for Patients with Cervical Ossification of the Posterior Longitudinal Ligament: A Prospective Multicenter Study. Spine 46, E1238–E1245. https://doi.org/10.1097/brs.0000000000004094 (2021).
Shou, F. et al. Prevalence of C5 nerve root palsy after cervical decompressive surgery: a meta-analysis. Eur. Spine J. 24, 2724–2734. https://doi.org/10.1007/s00586-015-4186-5 (2015).
Gu, Y. F. et al. Incidence and Risk Factors of C5 Palsy following Posterior Cervical Decompression: A Systematic Review. PloS one. 9 https://doi.org/10.1371/journal.pone.0101933 (2014).
Jack, A. et al. Factors Associated With C5 Palsy Following Cervical Spine Surgery: A Systematic Review. Global Spine J. 9, 881–894. https://doi.org/10.1177/2192568219874771 (2019).
Sakaura, H., Hosono, N., Mukai, Y., Ishii, T. & Yoshikawa, H. C5 Palsy after Decompression Surgery for Cervical Myelopathy: Review of the Literature. Spine 28, 2447–2451. https://doi.org/10.1097/01.BRS.0000090833.96168.3F (2003).
Hofler, R. C. et al. C5 Palsy after Cervical Laminectomy: Natural History in a 10 year Series. The spine journal: official J. North. Am. Spine Society (2021).
Bydon, M. et al. Incidence and prognostic factors of c5 palsy: a clinical study of 1001 cases and review of the literature. Neurosurgery 74 (6), 595–604 (2014). discussion 604 – 595.
Lubelski, D. et al. Treatment of C5 Palsy: An International Survey of Peripheral Nerve Surgeons. Global Spine J. 14, 2225–2231. https://doi.org/10.1177/21925682231171853 (2024).
Hirabayashi, S., Kitagawa, T., Yamamoto, I., Yamada, K. & Kawano, H. Postoperative C5 Palsy: Conjectured Causes and Effective Countermeasures. Spine Surg. Relat. Res. 3, 12–16. https://doi.org/10.22603/ssrr.2018-0016 (2018).
Alonso, F. et al. Potential Mechanism for Some Postoperative C5 Palsies: An Anatomical Study. Spine 43, 161. https://doi.org/10.1097/BRS.0000000000002281 (2018).
Blizzard, D. J. et al. The role of iatrogenic foraminal stenosis from lordotic correction in the development of C5 palsy after posterior laminectomy and fusion. J. Orthop. Surg, Res. 10, 1–8 (2015).
Nakajima, H., Kuroda, H., Watanabe, S., Honjoh, K. & Matsumine, A. Risk factors and preventive measures for C5 palsy after cervical open-door laminoplasty. J. Neurosurgery: Spine. 32, 592–599 (2019).
Nakashima, H. et al. Multivariate analysis of C-5 palsy incidence after cervical posterior fusion with instrumentation. J. Neurosurg. Spine. 17 2, 103–110 (2012).
Shikata, J. et al. Insufficient Recovery From C5 Palsy Following Anterior Cervical Decompression and Fusion. Spine 47, 423–429. https://doi.org/10.1097/BRS.0000000000004225 (2021).
Er, M. R. H. et al. Increased Change in Cervical Lordosis Is Associated With Decreased Rate of Recovery in Patients With C5 Palsy. Clin. Spine Surg. 38 https://doi.org/10.1097/BSD.0000000000001680 (2024).
Aiba, A. et al. Characteristics of Postoperative C5 Palsy Following Anterior Decompression and Fusion Surgery for Cervical Degenerative Disorders: Trends Associated with Advancements in Surgical Technique. World Neurosurg. 176, e232–e239. https://doi.org/10.1016/j.wneu.2023.05.037 (2023).
Minoda, Y. et al. Palsy of the C5 Nerve Root After Midsagittal-Splitting Laminoplasty of the Cervical Spine. Spine 28, 1123–1127. https://doi.org/10.1097/01.Brs.0000067261.83984.73 (2003).
Khuyagbaatar, B., Kim, K., Park, W. & Kim, Y. H. Biomechanical investigation of post-operative C5 palsy due to ossification of the posterior longitudinal ligament in different types of cervical spinal alignment. J. Biomech. 57, 54–61. https://doi.org/10.1016/j.jbiomech.2017.03.019 (2017).
Kaneyama, S. et al. Prospective Study and Multivariate Analysis of the Incidence of C5 Palsy After Cervical Laminoplasty. Spine 35, E1553-E1558 (2010).
Maki, S. et al. Characteristics of postoperative C5 palsy following anterior decompression and fusion surgery for cervical degenerative disorders: trends associated with advancements in surgical technique. World Neurosurg. https://doi.org/10.1016/j.wneu.2023.05.037 (2023).
Imagama, S. et al. C5 palsy after cervical laminoplasty: a multicentre study. J. Bone Joint Surg. Br. Volume. 92, 393–400 (2010).
Lee, S. H. et al. Outcomes and Related Factors of C5 Palsy Following Cervical Laminectomy With Instrumented Fusion Compared With Laminoplasty. Spine 41, E574–E579. https://doi.org/10.1097/brs.0000000000001343 (2016).
Li, N. et al. Risk factors for C(5) palsy following the posterior spinal process-splitting laminoplasty for cervical ossification of the posterior longitudinal ligament: a case control study. Ann. Transl Med. 10, 634. https://doi.org/10.21037/atm-22-1730 (2022).
Acknowledgements
The authors express their profound gratitude to all the institutions that have cooperated with them, proof-readers and editors.
Funding
This study was supported by Japan Agency for Medical Research and Development and Japanese Health Labour Sciences Research Grant (grant no. 23ek0109541h0003).
Author information
Authors and Affiliations
Contributions
S.E. managed the data and contributed to data analysis and manuscript writing. T.Y. supervised the study. T.H., K.S., K.K., S.T., Y.M., K.Y., H.O., K.W., K.K., M.K., A.K., T.F., S.M., N.N., Y.N., Y.O., K.A., H.N., T.E., K.M., H.N., K.M., M.M., T.K., K.Y., T.B., S.K., T.O., M.T., H.M., S.F., H.K., H.K., N.N., H.T., S.I., Y.K., K.T., M.N., M.M., and M.Y. contributed to data collection and guidance on the manuscript content. All authors read and commented on previous versions of the manuscript, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Egawa, S., Hirai, T., Sakai, K. et al. Incidence and prognostic factors of postoperative C5 palsy after cervical OPLL surgery: a nationwide prospective multicenter study. Sci Rep 16, 15578 (2026). https://doi.org/10.1038/s41598-026-45807-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-45807-4
