
Abstract
Digital health interventions (DHIs), delivered via digital platforms such as internet-based programs, mobile applications or short messages, may improve patient-reported outcomes (PROs), but comparative effectiveness is unclear. We conducted a network meta-analysis of randomized controlled trials in adults undergoing elective surgery under general anesthesia, identified in PubMed, Embase, CENTRAL, and Web of Science to March 1, 2025. Standardized mean differences (SMDs), mean differences (MDs) with minimal important differences (MIDs), and 95% CIs were estimated. Risk of bias was assessed with RoB 2 and certainty of evidence with GRADE. Fifty-six trials (6,154 patients) were included. Extended reality (XR) most effectively reduced perioperative anxiety (SMD 0.60; 95% CI 0.37–0.84; MD 8.05; MID 6.71; moderate-certainty). For postoperative pain, mobile applications (SMD 0.64; 95% CI 0.32–0.95; MD 1.36; MID 1.0; moderate-certainty) and XR (SMD 0.51; 95% CI 0.26–0.76; MD 1.09; MID 1.0; moderate-certainty) were probably effective. For quality of life, 2D video yielded the greatest gain (SMD 0.99; 95% CI 0.11–1.88; MD 0.11; MID 0.05; high-certainty). XR also improved satisfaction (SMD 1.27; 95% CI 0.63–1.91; MD 1.91; MID 0.75; moderate-certainty). These findings suggest that DHIs may improve perioperative PROs.
Similar content being viewed by others


Introduction
Patient-reported outcomes (PROs) are patient-centered assessments that capture key aspects of health status, including physical and psychological well-being, health-related quality of life, treatment satisfaction, and healthcare experience1,2. In the perioperative setting, PROs provide essential insights into the effects of surgical interventions and perioperative care on patients’ anxiety, pain, quality of life, and overall satisfaction3. This direct documentation of symptom burden and treatment impact provides critical perspective to inform the development and implementation of emerging healthcare technologies4,5.
The perioperative period—spanning preoperative, intraoperative, and postoperative phases—represents a highly stressful and uncomfortable interval for patients. Given its profound impact on patient experiences, this period is a critical setting for the application of PROs6. Psychophysiological responses, such as heightened pain and anxiety, are commonly experienced during this period7. These responses can compromise preoperative stability (e.g., elevated blood pressure, poor sleep, or reduced nutritional intake) and increase the risk of intraoperative and postoperative complications, ultimately hindering comprehensive and positive recovery8,9,10. Effective pain and anxiety management is therefore essential to all aspects of recovery, including mental status, nutritional intake, cost of care, rehabilitation, patient satisfaction, and overall PROs11.
Enhancing PROs through nonpharmacological strategies like patient education is a cornerstone of perioperative patient-centered care, with benefits for reducing anxiety, improving pain control, and increasing satisfaction12,13. However, traditional in-person education faces limitations in staffing, scalability, time, and accessibility14, emphasizing the urgent need for scalable and efficient alternatives. Digital health interventions (DHIs) have thus emerged as a promising solution to deliver personalized and accessible support for perioperative education and symptom management15,16.
Defined by the World Health Organization (WHO) as “a discrete functionality of digital technology that is applied to achieve health objectives”, DHIs are delivered directly to patients via digital platforms such as internet-based programs, mobile applications, or short message service systems17,18. Evidence across surgical specialties has demonstrated the effectiveness of these web-based and mobile tools in providing education, symptom monitoring, and patient support19,20,21. Compared to in-person interventions, DHIs offer notable advantages, including enhanced patient experiences, improved understanding of treatment options’ benefits and risks, and better management of anxiety, pain, and quality of life22.
Despite the rapidly growing interest in applying DHIs to manage perioperative conditions such as pain, anxiety, and quality of life impairment, to our knowledge, the implications of DHIs for PROs in the perioperative care have not been quantitatively assessed. This network meta-analysis aims to comprehensively evaluate the effectiveness of DHIs for perioperative conditions as reported in published randomized controlled trials (RCTs) and to assess the extent to which differences in outcomes may be explained by various intervention types.
Results
Description of included studies
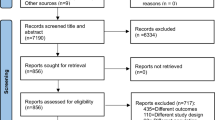
We screened 12,240 records and assessed 205 full-text articles for eligibility, ultimately included 56 RCTs involving 6154 participants (47% male). The pooled mean age was 53.77 years (95% CI 53.50–54.05). Most studies were conducted in China (13 trials, 23%), Turkey (9 trials, 16%), and the United States (8 trials, 14%). Details of the study selection process are presented in Fig. 1, and the characteristics of included RCTs are summarized in Table S4. The risk of bias assessment indicated that 86% of studies had a low or concered risk of bias, while eight studies were rated as high risk—two due to randomization issues and six due to missing outcome data (Fig. S1, Table S5). No significant publication bias was found based on comparison-adjusted funnel plots and Egger’s tests (Figs. S2 and S3). Table S6 summarizes the results of incoherence assessments between direct and indirect estimates, Table S7 display the results of between-study heterogeneity assessments, and Table S8 presents the results of certainty of evidence assessments for direct, indirect, and network comparisons.

Study Flow Diagram.
Data analysis
Figure 2 illustrates network plots of RCTs comparing various DHIs across four outcomes: anxiety, pain, quality of life, and satisfaction. In the network plots, the thickness of the connecting lines represents the number of trials between specific interventions, and the node size reflects the sample size. The number of included studies that reported data on each outcome was as follows: 32 for anxiety, 37 for pain, 17 for quality of life, and 9 for satisfaction.

a Anxiety, b Pain, c Quality of Life, and d Satisfaction. Each circular node represents a type of intervention. The node size is proportional to the total number of patients. Connecting lines indicate direct comparisons of interventions, and their width is proportional to the number of pairwise comparisons. Abbreviations: XR Extended reality, 2D = 2 dimensional, App application.
Figure 3 summarizes the comparative effectiveness and certainty of evidence across interventions. XR was categorized as among the most effective interventions for reducing perioperative anxiety and improving patient satisfaction. Mobile applications were most effective for reducing postoperative pain, while 2D video was most effective for improving quality of life. These classifications were based on point estimates exceeding the MID and confidence intervals entirely or mostly above the MID.

We categorized the interventions into three tiers based on their effects relative to reference group (i.e., standard care). Most effective interventions had a point estimate exceeding the minimal important difference (MID) with the 95% confidence interval (CI) entirely above the MID. Intermediate effective interventions had a point estimate above the MID but a 95% CI that crossed the MID. Least effective interventions had a point estimate not exceeding the MID, indicating no clinically meaningful difference from standard care. Bold text indicates that the 95% CI did not cross the null effect (statistical significance).
Table 1 presents the detailed results of the network meta-analysis. Compared with standard care, XR significantly reduced anxiety (SMD 0.60; 95% CI 0.37–0.84; MD 8.05; I² 82%), exceeding the MID of 6.71; because of this substantial heterogeneity, the certainty of evidence was rated as moderate. 2D video also reduced anxiety (SMD 0.46; 95% CI 0.18–0.75; MD 6.18; I² 43%), but did not reach the MID, indicating uncertain clinical relevance despite high-certainty evidence. For postoperative pain, mobile applications (SMD 0.64; 95% CI 0.32–0.95; MD 1.36; I² 84%) and XR (SMD 0.51; 95% CI 0.26–0.76; MD 1.09; I² 78%) both exceeded the MID of 1.0, yet substantial heterogeneity again led to moderate-certainty evidence. 2D video showed the greatest improvement in quality of life (SMD 0.99; 95% CI 0.11–1.88; MD 0.11), surpassing the MID of 0.05 with high-certainty evidence. XR also improved patient satisfaction (SMD 1.27; 95% CI 0.63–1.91; MD 1.91; I² 88%), exceeding the MID of 0.75; however, because of the substantial heterogeneity, this result was also graded as moderate-certainty evidence. Detailed league tables for these outcomes are provided in Figs. S4– S7.
Subgroup and sensitivity analysis
We conducted two subgroup analyses. The first analysis examined the timing of anxiety assessment, categorized as preoperative and postoperative. For preoperative anxiety, XR showed the greatest effect (SMD 0.83; 95% CI 0.54–1.12; MD 7.48; I² 72%), exceeding the MID of 4.51, with moderate-certainty evidence. For postoperative anxiety, 2D video showed the largest effect size among interventions (SMD 0.39; 95% CI 0.07–0.72; MD 7.39; I² 62%), but the estimated benefit did not exceed the MID threshold of 9.48 and was supported by low-certainty evidence (Table S9).
The second subgroup analysis investigated the impact of different interventions on anxiety and pain levels in open and minimally invasive surgeries. In open surgeries, XR showed the greatest benefit (SMD 0.65; 95% CI 0.37–0.92; MD 10.90; I² 46%), exceeding the MID of 8.39 with high-certainty evidence. 2D video (SMD 0.46; 95% CI 0.19–0.72; MD 7.71; I² 45%) and web applications (SMD 0.38; 95% CI 0.04–0.72; MD 6.37; I² 56%) significantly reduced anxiety, but both fell short of the MID threshold, suggesting uncertain clinical relevance despite high-certainty evidence. In minimally invasive surgeries, mobile applications demonstrated the largest effect (SMD 1.11; 95% CI 0.33–1.89; MD 10.18), exceeding the MID of 4.59, with high-certainty evidence. 2D video also showed a clinically meaningful benefit (SMD 0.81; 95% CI 0.32–1.30; MD 7.43), surpassing the MID and supported by high-certainty evidence.
For pain management in open surgeries, XR was the most effective intervention (SMD 0.75; 95% CI 0.44–1.06; MD 1.76; I² 42%), with high-certainty evidence and a clinically meaningful effect exceeding the MID of 1.0. Mobile applications (SMD 0.58; 95% CI 0.25–0.91; MD 1.36; I² 73%) also exceeded the MID, supported by moderate-certainty evidence. Although 2D video showed a statistically significant benefit (SMD 0.37; 95% CI 0.04–0.70; MD 0.87; I² 0%), the effect did not reach the MID threshold, indicating limited clinical relevance. In minimally invasive surgeries, none of the interventions achieved a statistically significant or clinically meaningful reduction in pain compared with standard care. Figs. S8– S13 present detailed network plots, forest plots comparing each intervention with standard care, and league tables summarizing the findings.
The sensitivity analysis excluded studies with a high risk of bis (n = 8) identified using the RoB 2 tool. Results for anxiety, pain, and satisfaction were consistent with the primary analysis. In terms of quality of life, both 2D video (SMD 0.99; 95% CI 0.13–1.86) and XR (SMD 0.93; 95% CI 0.07–1.78) showed significant effectiveness. This indicates that the primary analysis may have underestimated the impact of XR on quality of life by including studies with a high risk of bias. Additional visual representations of the results are provided in Fig. S14, which includes forest plots and league tables.
Discussion
This study conducted a large-scale quantitative analysis involving over 6154 participants from 56 RCTs to evaluate the existing evidence on the outcomes of DHIs for enhancing PROs in perioperative care. Our findings indicate that DHIs were associated with significant improvements in perioperative PROs—anxiety, pain, quality of life, and satisfaction—compared with standard care. Among the interventions, XR, mobile applications (e.g., interactive apps for perioperative education, postoperative care guidance or real-time health monitoring), and video-based tools showed the most consistent and substantial effects.
Regarding timing of outcomes, XR was particularly effective in reducing preoperative anxiety, while 2D video showed greater effectiveness for postoperative anxiety. In open surgeries, XR demonstrated the strongest effects on both pain control and anxiety alleviation. For minimally invasive procedures, mobile applications proved more effective in alleviating anxiety and pain. These findings highlight the potential of DHIs as innovative and effective tools for optimizing perioperative PROs, providing tailored, scalable, and patient-centered solutions across diverse surgical settings. To enhance clinical interpretability, we prespecified MID for anxiety, quality of life, and satisfaction as 0.5 times the pooled standard deviation, and 1.0 point on the 0–10 pain scale for postoperative pain, so that effect estimates could be judged against patient-relevant thresholds of benefit.
Perioperative discomfort is a major clinical concern, with studies reporting high prevalence of severe anxiety and frequent pain23. Most patients express strong demand for more comprehensive information throughout the perioperative process to reduce uncomfortable experience24. Multiple studies have demonstrated that DHIs effectively reduce anxiety, pain, and stress, while enhancing quality of life and patient satisfaction across various surgical procedures, including cardiac, orthopedic, and musculoskeletal surgeries11,25,26. In a randomized crossover study, a telehealth-based virtual reality program reduced pain intensity, pain interference and behavior, and mood and sleep disturbances in individuals with chronic orofacial pain27. Additionally, DHIs have been associated with decreased rates of 30-day readmissions and emergency department visit rates following abdominal surgeries28. These DHIs may provide personalized support, education, and self-management tools in the future29. While most studies report DHI outcomes equivalent to or better than standard care, evidence quality varies, necessitating further research to establish long-term efficacy and cost-effectiveness20,30,31.
Our results were consistent with previous systematic reviews and meta-analysis studies on DHIs, which have also identified improvements in chronic pain, functioning, and quality of life, although these studies did not specifically focus on the perioperative population32,33,34,35. A large-scale review of over 1200 controlled trials have supported the effectiveness of DHIs and also confirmed their therapeutic potential in managing pain and mood disorders31. For musculoskeletal pain, DHIs demonstrate small to moderate effects in reducing pain, improving functioning, and enhancing quality of life34,35. For cardiac patients, DHIs, particularly telemonitoring systems, have beneficial effects on depression and anxiety36,37,38. For cancer patients, DHIs effectively improve quality of life and reduce anxiety and depression symptoms39. Moreover, DHIs have been shown to significantly reduce systolic blood pressure in patients with hypertension and were also considered helpful in inequities elimination, as they can be widely disseminated without reducing intervention fidelity40,41. Overall, DHIs offer a scalable, accessible and high-potential solution for improving PROs across various health conditions.
The strength of this study is that, to our knowledge, it was the first to provide an overview of the implications of DHIs for PROs in perioperative period. However, our findings should be interpreted considering several limitations. First, substantial statistical and clinical heterogeneity was observed across several pooled analyses, particularly for pain, anxiety and quality-of-life outcomes. This heterogeneity is likely related to differences in intervention modalities and protocols (e.g., types and intensity of digital health interventions), surgical procedures (open vs minimally invasive surgery and different specialties), patient populations (such as age and baseline psychological status), and methodological approaches (including outcome measures and follow-up time points). Although we used random-effects models and conducted prespecified subgroup and sensitivity analyses to explore these sources of heterogeneity, residual heterogeneity remained; therefore, these pooled estimates should be interpreted with caution. Second, our MID-based categorization of intervention effectiveness was a pragmatic aid to interpretation rather than a strict hypothesis-testing framework. Although we defined “most effective” interventions as those whose point estimates and 95% CIs exceeded the MID, a few borderline comparisons with 95% CIs marginally crossing the MID were still grouped in this category when most of the interval lay above the threshold, so the certainty of benefit for these comparisons may be slightly overstated. Third, the variability in DHI parameters across different clinical conditions prevented a thorough assessment of the effects and quality of each intervention. Additionally, it was difficult to extract and classify interventions in a standardized way, such as videos in mobile applications, which complicates the isolation of individual intervention effects. Future research should further evaluate the effectiveness and practicality of combined interventions or investigate more advanced technologies, such as AI-driven models, in perioperative care settings42,43,44. From a practical perspective, our findings suggest that XR-based and mobile application-based interventions may be prioritized for patients with high preoperative anxiety or at risk of moderate-to-severe postoperative pain, while their implementation should take into account local resources, staff training, digital literacy, and patient preferences.
In this network meta-analysis of 56 RCTs, DHIs—particularly XR, mobile applications, and video-based interventions—significantly reduced anxiety and pain and improved quality of life and patient satisfaction compared with standard care during the perioperative period. Despite challenges in clinical implementation, these findings highlight the potential of DHIs to enhance perioperative PROs. Further high-quality RCTs are warranted to confirm and expand upon these benefits.
Methods
Study design
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Network Meta-Analysis Checklist (Supplement 1)45. We registered this network meta-analysis with the International Prospective Register of Systematic Reviews (PROSPERO, CRD42025632341).
Literature search and study selection
We used a combination of Medical Subject Headings and free-text terms to conduct a systematic search in PubMed, Embase, the Cochrane Central Register of Controlled Trials, and Web of Science from inception to March 1st, 2025. Details of the search strategies for each database are provided in Table S1. Additionally, we manually screened the reference lists of included studies to identify potentially relevant articles that might be missed during the initial database search.
This review targeted adults (≥18 years) undergoing elective surgery under general anesthesia. Eligible trials compared perioperative DHIs and two conditions that were face-to-face visits and standard care. DHIs were technologies including extended reality (XR), mobile applications, web-based platforms, video interventions, and telemedicine (see details in Table S2). Outcomes of interest were anxiety, pain, quality of life, and patient satisfaction (Table S3). Only RCTs were included.
Two investigators first independently screened studies by the titles and abstracts, followed by an assessment of the full texts of the potentially eligible articles. Any discrepancies were resolved by thorough examination and discussion to reach a consensus. Persistent disagreements were referred to a third senior author for a final decision.
Data extraction
Two investigators independently extracted data from eligible articles using a standardized form. The extracted data included: the first author’s name, year of publication, country of study, participant characteristics (sample size, mean or median age, and sex distribution [n (%)]), type of surgery, details of the intervention and control groups, timing of the DHIs, measured outcomes, assessment instruments, and the time points for outcome evaluation. Discrepancies between the reviewers were resolved by re-checking and discussion to ensure accuracy.
Risk of Bias assessment
We evaluated risk of bias for the included RCTs using Cochrane’s risk-of-bias tool (RoB 2)46, assessing five domains: (1) randomization process bias, (2) intervention deviations bias, (3) missing outcome data bias, (4) outcome measurement bias, and (5) reported results selection bias. Each domain was rated as “low risk”, “some concerns”, or “high risk”. Overall bias was rated as “low” if all domains were low risk, as “some concerns” if no domain was high risk but some were concerns, or as “high” if any domain was high risk.
Statistical analysis
We calculated standardized mean differences (SMDs) with corresponding 95% confidence intervals (CIs) for all outcomes due to variability in measurement instruments across studies. A result was considered statistical significance when the 95% CI excluded zero. To enhance clinical interpretability, SMDs were converted into mean differences (MDs) on commonly used scales by multiplying each SMD by the pooled standard deviation of control groups47. These scales included the State Anxiety Inventory for anxiety, the Visual Analog Scale for pain, the EuroQol Five-Dimensional Utility Score for quality of life, and the Numeric Rating Scale for patient satisfaction. To judge whether the study’s effect was important for the patients, we used the minimal important difference (MID) as decision threshold. The MID was defined as 0.5 times the pooled standard deviation for anxiety, quality of life, and satisfaction48, and as 1.0 for pain49.
We conducted a frequentist random-effects network meta-analysis with the graph-theoretical method using the netmeta package in the R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria)50. We presented network estimates in forest plots and league tables and ranked interventions based on P-scores. Transitivity was evaluated by comparing covariate distributions, including participants’ mean age, sex distribution, and the timing (e.g., preoperative or postoperative) and type of DHI. Heterogeneity (inconsistency) across studies was assessed using Cochran’s Q test and quantified with the I² statistic; a Q-test P < 0.05 was considered to indicate statistically significant heterogeneity51. Incoherence between direct and indirect estimates was assessed using the netsplit function in the netmeta package in R software, with a P < 0.05 suggesting significant incoherence52. We assessed publication bias using comparison-adjusted funnel plots and Egger’s test for asymmetry in direct comparisons with at least 10 studies53. A P < 0.1 in Egger’s test suggested potential publication bias.
Two predefined subgroup analyses were stratified by the timing of outcome assessment (preoperative anxiety vs postoperative anxiety) and the type of surgery (open vs minimally invasive). Sensitivity analyses were performed by excluding studies identified as having a high risk of bias.
Certainty of evidence
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework for network meta-analyses was utilized to evaluate the certainty of evidence for direct, indirect, and network estimates54. Certainty levels were classified as high, moderate, low, or very low, with downgrading considerations including risk of bias, heterogeneity, indirectness, publication bias, intransitivity, incoherence, and imprecision55,56. We categorized the interventions using the minimally contextualized framework57. Compared to reference group (i.e., standard care), interventions were categorized as most effective if the point estimates exceeded the MID and the 95%CI did not cross the MID, while those with a point estimate above the MID but a 95%CI that crossed the MID threshold were categorized as intermediate effective. Interventions with a point estimate not exceeding the MID were categorized as the least effective as they were not convincingly superior to standard care.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary materials. Further datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Weinfurt, K. P. & Reeve, B. B. Patient-reported outcome measures in clinical research. JAMA 328, 472–473 (2022).
Chang, S. S. & Movsas, B. How vital are patient-reported outcomes?J. Natl. Cancer Inst. 114, 347–348 (2022).
Black, N. Patient reported outcome measures could help transform healthcare. BMJ 346, f167–f167 (2013).
Dai, W. et al. Patient-reported outcome-based symptom management versus usual care after lung cancer surgery: a multicenter randomized controlled trial. JCO. 40, 988–996 (2022).
Pearce, F. J. et al. The role of patient-reported outcome measures in trials of artificial intelligence health technologies: a systematic evaluation of ClinicalTrials.gov records (1997–2022). Lancet Digit. Health 5, e160–e167 (2023).
Wang, X. S. & Gottumukkala, V. Patient-reported outcomes: Is this the missing link in patient-centered perioperative care? Best. Pract. Res. Clin. Anaesthesiol. 35, 565–573 (2021).
Tadesse, M. et al. Effect of preoperative anxiety on postoperative pain on patients undergoing elective surgery: prospective cohort study. Ann. Med. Surg. 73, 103190 (2022).
Ni, K., Zhu, J. & Ma, Z. Preoperative anxiety and postoperative adverse events: a narrative overview. Anesthesiol. Perioper. Sci. 1, 23 (2023).
Gu, X., Zhang, Y., Wei, W. & Zhu, J. Effects of preoperative anxiety on postoperative outcomes and sleep quality in patients undergoing laparoscopic gynecological surgery. J. Clin. Med. 12, 1835 (2023).
Holzer, K. J. et al. The impact of compassion-based interventions on perioperative anxiety and depression: a systematic review and meta-analysis. J. Affect. Disord. 365, 476–491 (2024).
Valentijn, P. P. et al. Digital health interventions for musculoskeletal pain conditions: systematic review and meta-analysis of randomized controlled trials. J. Med. Internet Res. 24, e37869 (2022).
McDonald, S., Page, M. J., Beringer, K., Wasiak, J. & Sprowson, A. Preoperative education for hip or knee replacement. Cochrane Database Syst. Rev. 2014, CD003526 (2014).
Guo, P., East, L. & Arthur, A. A preoperative education intervention to reduce anxiety and improve recovery among Chinese cardiac patients: a randomized controlled trial. Int. J. Nurs. Stud. 49, 129–137 (2012).
Amoah, V. M. K. et al. A qualitative assessment of perceived barriers to effective therapeutic communication among nurses and patients. BMC Nurs. 18, 4 (2019).
Lewkowitz, A. K. et al. The effect of digital health interventions on postpartum depression or anxiety: a systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 230, 12–43 (2024).
Bodenheimer, T. & Sinsky, C. From triple to quadruple aim: care of the patient requires care of the provider. Ann. Fam. Med. 12, 573–576 (2014).
Shaffer, K. M. et al. Digital health and telehealth in cancer care: a scoping review of reviews. Lancet Digit. Health 5, e316–e327 (2023).
Zakiyah, N. et al. Economic evaluations of digital health interventions for patients with heart failure: systematic review. J. Med. Internet Res. 26, e53500 (2024).
Wu, K. A. et al. Digital health for patients undergoing cardiac surgery: a systematic review. Healthcare 11, 2411 (2023).
van der Meij, E. et al. Personalised perioperative care by e-health after intermediate-grade abdominal surgery: a multicentre, single-blind, randomised, placebo-controlled trial. Lancet 392, 51–59 (2018).
Hao, X. et al. Control Tower in the hospital: a structure–process–outcome systemic review of telemedicine systems for interprofessional collaboration. npj Digit. Med. 8, 669 (2025).
Kondylakis, H. et al. A digital health intervention for stress and anxiety relief in perioperative care: protocol for a feasibility randomized controlled trial. JMIR Res. Protoc. 11, e38536 (2022).
Walker, E. M. K., Bell, M., Cook, T. M., Grocott, M. P. W. & Moonesinghe, S. R. Patient reported outcome of adult perioperative anaesthesia in the United Kingdom: a cross-sectional observational study. Br. J. Anaesth. 117, 758–766 (2016).
Gobbo, M. et al. Experience and needs during perioperative care: a focus group study. Patient Prefer. Adherence 14, 891–902 (2020).
Lin, S.-J. et al. Perioperative application of chatbots: a systematic review and meta-analysis. BMJ Health Care Inf. 31, e100985 (2024).
Luo, Z. et al. Digital health interventions in pediatric perioperative care: a network meta-analysis. JAMA Pediatr. 179, 1153 (2025).
Colloca, L. et al. Telehealth virtual reality intervention reduces chronic pain in a randomized crossover study. npj Digit. Med. 8, 192 (2025).
Grygorian, A., Montano, D., Shojaa, M., Ferencak, M. & Schmitz, N. Digital health interventions and patient safety in abdominal surgery. JAMA Netw. Open 7, e248555 (2024).
Javadi, N., Gwilt, I. & Davis, A. Potential benefits of designing immersive technologies to reduce anxiety in the perioperative patient journey. Proc. DRS https://doi.org/10.21606/drs.2022.491 (2022).
Gentili, A. et al. The cost-effectiveness of digital health interventions: a systematic review of the literature. Front. Public Health 10, 787135 (2022).
Khalili-Mahani, N. & Tran, S. The bigger picture of digital interventions for pain, anxiety and stress: a systematic review of 1200+ controlled trials. in Lecture Notes in Computer Science (ed. Duffy, V. G.) 67–78, https://doi.org/10.1007/978-3-031-06018-2_5 (Springer International Publishing, 2022).
Chang, H., Zhou, J., Chen, Y., Wang, X. & Wang, Z. Comparative effectiveness of eHealth interventions on the exercise endurance and quality of life of patients with COPD: a systematic review and network meta-analysis. J. Clin. Nurs. 33, 3711–3720 (2024).
Slattery, B. W. et al. An evaluation of the effectiveness of the modalities used to deliver electronic health interventions for chronic pain: systematic review with network meta-analysis. J. Med. Internet Res. 21, e11086 (2019).
Zangger, G. et al. Benefits and harms of digital health interventions promoting physical activity in people with chronic conditions: systematic review and meta-analysis. J. Med. Internet Res. 25, e46439 (2023).
Knight, S. R. et al. Mobile devices and wearable technology for measuring patient outcomes after surgery: a systematic review. npj Digit. Med. 4, 157 (2021).
Jang, S. et al. A systematic review and meta-analysis of the effects of rehabilitation using digital healthcare on musculoskeletal pain and quality of life. J. Pain Res. ume 16, 1877–1894 (2023).
Hewitt, S., Sephton, R. & Yeowell, G. The effectiveness of digital health interventions in the management of musculoskeletal conditions: systematic literature review. J. Med. Internet Res. 22, e15617 (2020).
Kaihara, T. et al. Efficacy of digital health interventions on depression and anxiety in patients with cardiac disease: a systematic review and meta-analysis. Eur. Heart J. Digit. Health 3, 445–454 (2022).
Zhang, Y. et al. Digital health psychosocial intervention in adult patients with cancer and their families: systematic review and meta-analysis. JMIR Cancer 10, e46116 (2024).
Moghimian, M. et al. The effect of digital health interventions on postpartum depression or anxiety: a systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 230, 12–43 (2024).
Katz, M. E. et al. Digital health interventions for hypertension management in US populations experiencing health disparities. JAMA Netw. Open 7, e2356070 (2024).
Shimada, K. et al. Artificial intelligence-assisted interventions for perioperative anesthetic management: a systematic review and meta-analysis. BMC Anesthesiol. 24, 306 (2024).
Wang, B. et al. A systematic literature review on integrating AI-powered smart glasses into digital health management for proactive healthcare solutions. npj Digit. Med. 8, 410 (2025).
Lee, H., Chen, Q. & Ma, D. AI aiding perioperative anaesthetic management: on the way but not ready yet. Anesthesiol. Perioper. Sci. 2, 43 (2024).
Hutton, B. et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162, 777–784 (2015).
Sterne, J. A. C. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
Andrade, C. Mean difference, standardized mean difference (SMD), and their use in meta-analysis: as simple as it gets. J. Clin. Psychiatry 81, 11349 (2020).
Norman, G. R., Sloan, J. A. & Wyrwich, K. W. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med. Care 41, 582–592 (2003).
Myles, P. S. et al. Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br. J. Anaesth. 118, 424–429 (2017).
Neupane, B., Richer, D., Bonner, A. J., Kibret, T. & Beyene, J. Network meta-analysis using R: a review of currently available automated packages. PLoS ONE 9, e115065 (2014).
Higgins, J. P. T. & Thompson, S. G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 21, 1539–1558 (2002).
Dias, S., Welton, N. J., Caldwell, D. M. & Ades, A. E. Checking consistency in mixed treatment comparison meta-analysis. Stat. Med. 29, 932–944 (2010).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 315, 629–634 (1997).
Izcovich, A., Chu, D. K., Mustafa, R. A., Guyatt, G. & Brignardello-Petersen, R. A guide and pragmatic considerations for applying GRADE to network meta-analysis. BMJ. 381, e074495 (2023).
Schünemann, H. J. et al. GRADE guidelines: 21 part 1. Study design, risk of bias, and indirectness in rating the certainty across a body of evidence for test accuracy. J. Clin. Epidemiol. 122, 129–141 (2020).
Schünemann, H. J. et al. GRADE guidelines: 21 part 2. Test accuracy: inconsistency, imprecision, publication bias, and other domains for rating the certainty of evidence and presenting it in evidence profiles and summary of findings tables. J. Clin. Epidemiol. 122, 142–152 (2020).
Brignardello-Petersen, R. et al. GRADE approach to drawing conclusions from a network meta-analysis using a minimally contextualised framework. BMJ m3900. https://doi.org/10.1136/bmj.m3900 (2020).
Acknowledgements
The Noncommunicable Chronic Diseases-National Science and Technology Major Project (Grant No. 2023ZD0501801 to R.Z. and G.C., 2025ZD0550604 to S.L.), the Sichuan Province Health Research Project (Grant No. ZH2025-103 to T.Z.), the National Natural Science Foundation of China (Grant No. 82371280 to M.O., 72342014 to S.L.), the Science and Technology Department of Sichuan Province (Grant No. 2024ZDZX0017 to X.P., 2023NSFSC1565 to M.O., 2024YFFK0100 to Y.W.), 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (Grant No. ZYYC24001 to S.L.), and the Science and Technology Department of Sichuan Province (Grant No. 2024NSFSC0624 to L.Y.).
Author information
Authors and Affiliations
Contributions
Z.L., R.Z., J.W., and K.N. had full access to all study data and take responsibility for the integrity and accuracy of the analysis. Z.L., R.Z., J.W., and K.N. contributed equally as co-first authors. Z.L., R.Z., J.W., K.N., X.P., L.C., P.L., S.D., M.O., X.H., L.Y., Y.W., G.C., S.L., and T.Z. conceived and designed the study. Z.L., R.Z., J.W., K.N., X.P., L.C., P.L., S.D., M.O., X.H., L.Y., Y.W., G.C., S.L., and T.Z. contributed to data acquisition, analysis, and interpretation. Z.L., R.Z., J.W., K.N., X.P., L.C., P.L., S.D., X.H., and T.Z. drafted the manuscript. Z.L., R.Z., J.W., K.N., X.P., L.C., P.L., S.D., M.O., X.H., L.Y., Y.W., G.C., S.L., and T.Z. critically revised the manuscript for important intellectual content. Z.L., R.Z., J.W., K.N., X.H., and L.C. performed the statistical analysis. R.Z., G.C., S.L., T.Z., M.O., X.P., Y.W., and L.Y. obtained funding. Z.L., R.Z., J.W., K.N., X.P., L.C., P.L., S.D., X.H., L.Y., Y.W., G.C., and T.Z. provided administrative, technical, or material support. X.H., S.L., and T.Z. supervised the study. Z.L., R.Z., J.W., and K.N. conducted article screening, data extraction, and risk of bias assessment. X.H., S.L., and T.Z. guided the analysis plan and background research. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Luo, Z., Zhou, R., Wei, J. et al. Digital health interventions for perioperative patient-reported outcomes: a network meta-analysis. npj Digit. Med. 9, 206 (2026). https://doi.org/10.1038/s41746-026-02398-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41746-026-02398-8
