
Abstract
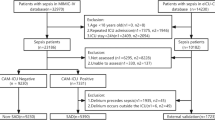
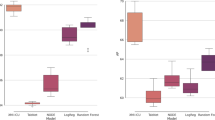
Sepsis has heterogeneous clinical trajectories, but conventional severity scores offer only static risk estimates. Timely, dynamic prediction could enable personalized intervention. In this multicenter retrospective study of 47,936 ICU patients meeting Sepsis-3 criteria from one institutional and two public datasets (MIMIC-III, eICU; sensitivity in MIMIC-IV), group-based trajectory modeling identified latent recovery patterns. An ensemble machine-learning model incorporating dynamic physiological variability was trained, temporally validated, and externally tested; clinical impact was assessed following implementation. Three trajectories emerged: rapid recovery (41.5%), slow recovery (36.4%), and clinical deterioration (22.1%). In the final binary classification task, AUROC was 0.92 (development), 0.89 (internal), 0.84 (MIMIC-III) and 0.77 (eICU); median warning time before deterioration was 17.6 h (Overall pooled across all cohorts). Reduced heart rate variability (SD < 10 bpm) predicted mortality (adjusted HR 2.17). Implementation reduced ICU stay by 1.8 days, machanical ventilation by 2.3 days, and 28-day mortality by 5.7%. This externally validated trajectory-based model offers accurate, early risk stratification for sepsis, supporting proactive, individualized critical care.
Similar content being viewed by others

Data availability
The data used in this study are available from the MIMIC-III and eICU Collaborative Research Database, subject to completion of the required data use agreements and credentialing. Access can be obtained via PhysioNet (https://physionet.org/) for MIMIC-III and via the eICU Collaborative Research Database program for eICU. The authors are not permitted to publicly share the underlying patient-level data. Institutional data are available from corresponding authors upon reasonable request.
Code availability
Analysis code to reproduce the experiments is available at https://github.com/ccmzhangrui/sepsis-trajectory-python-data.
References
Rudd, K. E. et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet. 395, 200–211 (2020).
Prescott, H. C. & Angus, D. C. Enhancing recovery from sepsis: a review. JAMA. 319, 62–75 (2018).
Iwashyna, T. J., Ely, E. W., Smith, D. M. & Langa, K. M. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 304, 1787–1794 (2010).
Kennedy, M., Joyce, N., Howell, M. D., Lawrence Motley, J. & Shapiro, N. I. Identifying infected emergency department patients admitted to the hospital ward at risk of clinical deterioration and intensive care unit transfer. Acad. Emerg. Med. 17, 1080–1085 (2010).
Vincent, J. L. & Moreno, R. Clinical review: scoring systems in the critically ill. Crit Care 14, 207 (2010).
Raith, E. P. et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 317, 290–300 (2017).
Ferreira, F. L., Bota, D. P., Bross, A., Mélot, C. & Vincent, J. L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA. 286, 1754–1758 (2001).
Zimmerman, J. E., Kramer, A. A., McNair, D. S. & Malila, F. M. A. cuteP. hysiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Crit. Care Med. 34, 1297–1310 (2006).
Fleuren, L. M. et al. Machine learning for the prediction of sepsis: a systematic review and meta-analysis of diagnostic test accuracy. Intensive Care Med. 46, 383–400 (2020).
Nemati, S. et al. An interpretable machine learning model for accurate prediction of sepsis in the ICU. Crit. Care Med. 46, 547–553 (2018).
Shashikumar, S. P. et al. Early sepsis detection in critical care patients using multiscale blood pressure and heart rate dynamics. J. Electrocardiol. 50, 739–743 (2017).
Henry, K. E., Hager, D. N., Pronovost, P. J. & Saria, S. A targeted real-time early warning score (TREWScore) for septic shock. Sci. Transl. Med. 7, 299ra122 (2015).
Desautels, T. et al. Prediction of sepsis in the intensive care unit with minimal electronic health record data: a machine learning approach. JMIR Med. Inform. 4, e28 (2016).
Futoma, J. et al. An improved multi-output Gaussian process RNN with real-time validation for early sepsis detection. Proc. Mach. Learn. Healthcare 68, 243–254 (2017).
Wong, A. et al. External validation of a widely implemented proprietary sepsis prediction model in hospitalized patients. JAMA Intern. Med. 181, 1065–1070 (2021).
Seymour, C. W. et al. Derivation, validation, and potential treatment implications of novel clinical phenotypes for sepsis. JAMA 321, 2003–2017 (2019).
Scicluna, B. P. et al. Classification of patients with sepsis according to blood genomic endotype: a prospective cohort study. Lancet Respir. Med. 5, 816–826 (2017).
Moorman, J. R. et al. Mortality reduction by heart rate characteristic monitoring in very low birth weight neonates: a randomized trial. J. Pediatr. 159, 900–906 (2011).
Scheffer, M. et al. Early-warning signals for critical transitions. Nature. 461, 53–59 (2009).
Ahmad, S., Tejuja, A., Newman, K. D., Zarychanski, R. & Seely, A. J. Clinical review: a review and analysis of heart rate variability and the diagnosis and prognosis of infection. Crit. Care. 13, 232 (2009).
Buchman, T. G. The community of the self. Nature. 420, 246–251 (2002).
Seymour, C. W. et al. Time to treatment and mortality during mandated emergency care for sepsis. N Engl. J. Med. 376, 2235–2244 (2017).
Yealy, D. M. et al. A randomized trial of protocol-based care for early septic shock. N Engl. J. Med. 370, 1683–1693 (2014).
Giannini, H. M. et al. A machine learning algorithm to predict severe sepsis and septic shock: development, implementation, and impact on clinical practice. Crit. Care Med. 47, 1485–1492 (2019).
Shimabukuro, D. W., Barton, C. W., Feldman, M. D., Mataraso, S. J. & Das, R. Effect of a machine learning-based severe sepsis prediction algorithm on patient survival and hospital length of stay: a randomised clinical trial. BMJ Open Respir. Res. 4, e000234 (2017).
Futoma, J., Hariharan, S. & Heller, K. Learning to detect sepsis with a multitask Gaussian process RNN classifier. Proc. 34th Int. Conf. Mach. Learn. 70, 1174–1182 (2017).
Mao, Q. et al. Multicentre validation of a sepsis prediction algorithm using only vital sign data in the emergency department, general ward and ICU. BMJ Open 8, e017833 (2018).
Reyna, M. A. et al. Early prediction of sepsis from clinical data: the PhysioNet/Computing in Cardiology Challenge 2019. Crit. Care Med. 48, 210–217 (2020).
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 315, 801–810 (2016).
Seymour, C. W. et al. Assessment of clinical criteria for sepsis: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 315, 762–774 (2016).
Rhee, C. et al. Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009-2014. JAMA 318, 1241–1249 (2017).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med 147, 573–577 (2007).
Collins, G. S., Reitsma, J. B., Altman, D. G. & Moons, K. G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 350, g7594 (2015).
Tibshirani, R. Regression shrinkage and selection via the lasso. J R Stat. Soc. Ser, B Stat Methodol. 58, 267–288 (1996).
Breiman, L. Random forests. Mach. Learn. 45, 5–32 (2001).
Charlson, M. E., Pompei, P., Ales, K. L. & MacKenzie, C. R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40, 373–383 (1987).
Vincent, J. L. et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intens. Care Med. 22, 707–710 (1996).
Delahanty, R. J., Alvarez, J., Flynn, L. M., Sherwin, R. L. & Jones, S. S. Development and evaluation of a machine learning model for the early identification of patients at risk for sepsis. Ann. Emerg. Med. 73, 334–344 (2019).
Futoma, J. et al. An improved multi-output Gaussian process RNN with real-time validation for early sepsis detection. Proc. Mach. Learn. Healthcare. 68, 243–254 (2017).
Pincus, S. M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 88, 2297–2301 (1991).
Van Buuren, S. & Groothuis-Oudshoorn, K. mice: multivariate imputation by chained equations in R. J. Stat. Softw. 45, 1–67 (2011).
Umscheid, C. A. et al. Development, implementation, and impact of an automated early warning and response system for sepsis. J. Hosp. Med. 10, 26–31 (2015).
Austin, P. C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46, 399–424 (2011).
Harrell, F. E. Jr, Lee, K. L. & Mark, D. B. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med 15, 361–387 (1996).
Altman, D. G. & Royston, P. The cost of dichotomising continuous variables. BMJ. 332, 1080 (2006).
Acknowledgements
We thank all the healthcare workers involved in the diagnosis and treatment of patients in the study. Special acknowledgment goes to the critical care teams at Ruijin Hospital for their dedication to patient care and data collection. We also express our gratitude to the teams responsible for the creation and maintenance of the MIMIC-III and eICU databases, whose work made this research possible. We thank Longxiang Su and Fang Wang for their valuable support and assistance during the study.The research funded by Shanghai Science and Technology Commission (23Y11900100), Science and Technology Commission of Shanghai Municipality (24ZR1447000), National Natural Science Foundation of China(82470088) and National High-Level Hospital Clinical Research Funding (2022-PUMCH-D-005, 2022-PUMCH-B-115).
Author information
Authors and Affiliations
Contributions
R.Z., Z.Z, and F.L. conceived the study. R.Z., F.L., Z.Z., and R.T. performed data curation. R.Z. and F.L. developed methodology. W.X., L.L., J.W., Y.L., and H.Q. supervised the project. All authors reviewed the manuscript and approved the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, R., Long, F., Zhao, Z. et al. Machine learning predicts sepsis deterioration trajectories. npj Digit. Med. (2026). https://doi.org/10.1038/s41746-026-02565-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41746-026-02565-x
