
Abstract
The residual, reversible potentials of neurological-functional recovery in patients paralysed due to a cervical cord injury were periodically checked according to the various assessment methods from the initial period of 72 hours after injury to the final follow-up of 7 years.
In our series, the data on the neurological changes were a little different from those reported in the literature.
In the complete paralysis group, only 2 of the 30 patients showed slight functional recovery of less than 1 grade in the Frankel classification with descent of the cord lesion level. Twenty three patients showed descent of a half to one segment from the initial cord lesion level. The remaining 5 patients deteriorated because of ascent of a half to two segments from the initial cord lesion level. All patients with complete paralysis remained essentially unchanged.
In the incomplete group, 58 of the 70 patients had significant recovery of more than 1 grade in the Frankel classification. The grade of neurological recovery was different in each patient. Patients with a central cord lesion showed remarkably better recovery of the cord function than those with other types of cord lesions. Nineteen of the 49 patients with a central cord lesion regained independent walking ability with or without aid.
Neurological recovery in the incomplete paralysis group might be expected until approximately 6 months after injury. The early appearance of signs of recovery was an indication of better results. There was no difference in the neurological recovery between patients who had been realigned surgically and those who have been realigned non-surgically. Our neurological-functional assessment method reflecting the sectional and logitudinal cord level function and expressing more detailed information was demonstrated.
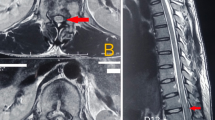
Magnetic resonance imaging (MRI) was used to assess residual cord function. The area of abnormal signal intensity almost corresponded to the cord level diagnosed neurologically.
Similar content being viewed by others
Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Bedbrook G, Hono S T J 1980 Recovery of spinal cord function. Paraplegia 18: 315–323.
Bosch A, Stauffer S, Nickel V L 1971 Incomplete traumatic quadriplegia, a ten year review. JAMA 19: 473–478.
Frankel H L, Hancock D O, Hyslop G, et al 1969 The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia, part I. Paraplegia 7: 179–192.
Kulkarni M V, McArdle C B, Kopanicky D, et al 1987 Acute spinal cord injury: MRImaging a 1.5 T. Radiology 164: 837–843.
Kadoga S, Nakamur T, Kobayashi S, et al 1987 Magnetic resonance imaging of acute spinal cord injury, report of three cases. Neuroradiology 29: 252–255.
Maynard F M, Reynolds G G, Fountain S, et al 1979 Neurological prognosis after traumatic quadriplegia, three-year experience of California regional spinal cord injury care system. Journal of Neurosurgery 50: 611–616.
Merriam W F, Faylor T K F, Roff S J, et al 1986 A reappraisal of acute traumatic central cord syndrome. Journal of Bone and Joint Surgery 68-B: 708–713.
Mirvis S E, Geisler F H, Jelineck J J, et al 1988 Acute cervical spinal trauma; evaluation with 1.5-T MRImaging. Radiology 166: 807–816.
Mirvis S E, Young J W R, Lim C, et al 1987 Hangman's fracture; radiological assessment in 27 cases. Radiology 163: 713–717.
Schneider R E, Cherry G, Pantek H 1954 The syndrome of acute central cervical spinal cord injury. Journal of Neurosurgery 11: 546–577.
Schneider R E 1955 The syndrome of acute anterior spinal cord injury, Journal of Neurosurgery 12: 95–122.
Stauffer E S, Bell G D 1978 Traumatic respiratory quadriplegia and pentaplegia, Orthop Clin North Am, 9: 1081–1088.
Tominaga S 1981 Pentaplegia and respiratory quadriplegia, Med J. Shimane Cent Hosp 8: 19–31.
Young J S, Dexter W R 1978–1979 Neurological recovery distal to the zone of injury in 172 cases of closed, traumatic spinal cord injury. Paraplegia 16: 39–49.
Wilmot C B, Hall K M 1986 Evaluation of acute management of tetraplegia; conservative versus surgical treatment. Paraplegia 24: 148–156.
Zancolli E 1975 Surgery for the quadriplegic hand with active, strong wrist extension preserved, a study of 97 cases. Clin Orthop & Related Research 112: 101–113.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Tominaga, S. Periodical, neurological-functional assessment for cervical cord injury. Spinal Cord 27, 227–236 (1989). https://doi.org/10.1038/sc.1989.34
Issue date:
DOI: https://doi.org/10.1038/sc.1989.34
Keywords
This article is cited by
-
Ulnar nerve integrity predicts 1-year outcome in cervical spinal cord injury
Neurological Research and Practice (2019)
