
Abstract
Introduction:
Transcranial motor evoked potential (TcMEP) monitoring is the gold standard for intra-operative neurological monitoring (IOM) of motor pathways during complex spine surgery because of its high sensitivity and specificity. However, although it is very low, the rate of false-negatives in TcMEP monitoring is not zero. Therefore, over-reliance on TcMEP monitoring can cause potentially preventable motor deficits.
Case presentation:
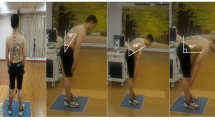
We report a case of motor deficits due to nerve root stretch after surgical correction of a congenital lumbar kyphoscoliosis in a 56-year-old woman. TcMEPs did not show any significant changes during surgery, whereas free-run electromyography (EMG) demonstrated a long-lasting train activity in the left quadriceps femoris muscle (QF) after correction at the osteotomy area. According to the normal findings on TcMEP monitoring, we did not release the correction. Postoperatively, a significant decrease (grade 2-) in the manual muscle test for the left QF and iliopsoas muscle and hypesthesia of the left anterior thigh was revealed. Fortunately, muscle strength was fully recovered without revision surgery at 6 months postoperatively; however, numbness in the left anterior thigh persisted at 2 years after surgery.
Discussion:
Our report suggests that the possibility of false-negative TcMEPs should be kept in mind, especially during surgery with a risk of nerve root injury. When abnormal findings in the free-run EMG, including long-lasting train activity, are observed, surgeons should consider performing appropriate responses, such as the release of the correction, even when no substantial changes are seen in the TcMEPs.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T et al. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus 2012; 33: E10.
Suk SI, Kim JH, Kim WJ, Lee SM, Chung ER, Nah KH . Posterior vertebral column resection for severe spinal deformities. Spine 2002; 27: 2374–2382.
Boachie-Adjei O, Yagi M, Nemani VM, Sacramento-Dominguez C, Akoto H, Cunningham ME et al. Incidence and risk factors for major surgical complications in patients with complex spinal deformity: a report from an SRS GOP site. Spine Deform 2015; 3: 57–64.
Burton DC, Carlson BB, Place HM, Fuller JE, Blanke K, Cho R et al. Results of the scoliosis research society morbidity and mortality database 2009–2012: a report from the Morbidity and Mortality Committee. Spine Deform 2016; 4: 338–343.
Bose B, Sestokas AK, Schwartz DM . Neurophysiological detection of iatrogenic C-5 nerve deficit during anterior cervical spinal surgery. J Neurosurg Spine 2007; 6: 381–385.
Lieberman JA, Lyon R, Feiner J, Hu SS, Berven SH . The efficacy of motor evoked potentials in fixed sagittal imbalance deformity correction surgery. Spine 2008; 33: E414–E424.
Lyon R, Lieberman JA, Feiner J, Burch S . Relative efficacy of transcranial motor evoked potentials, mechanically-elicited electromyography, and evoked EMG to assess nerve root function during sustained retraction in a porcine model. Spine 2009; 34: E558–E564.
Iwasaki H, Tamaki T, Yoshida M, Ando M, Yamada H, Tsutsui S et al. Efficacy and limitations of current methods of intraoperative spinal cord monitoring. J Orthop Sci 2003; 8: 635–642.
Macdonald DB, Al Zayed Z, Al Saddigi A . Four-limb muscle motor evoked potential and optimized somatosensory evoked potential monitoring with decussation assessment: results in 206 thoracolumbar spine surgeries. Eur Spine J 2007; 16: S171–S187.
Tsutsui S, Tamaki T, Yamada H, Iwasaki H, Takami M . Relationships between the changes in compound muscle action potentials and selective injuries to the spinal cord and spinal nerve roots. Clin Neurophysiol 2003; 114: 1431–1436.
Macdonald DB, Stigsby B, Al Homoud I, Abalkhail T, Mokeem A . Utility of motor evoked potentials for intraoperative nerve root monitoring. J Clin Neurophysiol 2012; 29: 118–125.
Gunnarsson T, Krassioukov AV, Sarjeant R, Fehlings MG . Real-time continuous intraoperative electromyographic and somatosensory evoked potential recordings in spinal surgery: correlation of clinical and electrophysiologic findings in a prospective, consecutive series of 213 cases. Spine 2004; 29: 677–684.
Jimenez JC, Sani S, Braverman B, Deutsch H, Ratliff JK . Palsies of the fifth cervical nerve root after cervical decompression: prevention using continuous intraoperative electromyography monitoring. J Neurosurg Spine 2005; 3: 92–97.
Quraishi NA, Lewis SJ, Kelleher MO, Sarjeant R, Rampersaud YR, Fehlings MG . Intraoperative multimodality monitoring in adult spinal deformity: analysis of a prospective series of one hundred two cases with independent evaluation. Spine 2009; 34: 1504–1512.
Devlin VJ, Schwartz DM . Intraoperative neurophysiologic monitoring during spinal surgery. J Am Acad Orthop Surg 2007; 15: 549–560.
Obi T, Mochizuki M, Isobe K, Mizoguchi K, Takatsu M, Nishimura Y . Mechanically elicited nerve root discharge: mechanical irritation and waveform. Acta Neurol Scand 1999; 100: 185–188.
Raynor BL, Padberg AM, Lenke LG, Bridwell KH, Riew KD, Buchowski JM et al. Failure of intraoperative monitoring to detect postoperative neurologic deficits: a 25-year experience in 12375 spinal surgeries. Spine 2016; 41: 1387–1393.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Ohashi, M., Watanabe, K., Furutani, K. et al. False-negative transcranial motor evoked potentials (TcMEPs) during surgery for congenital lumbar kyphoscoliosis: a case report. Spinal Cord Ser Cases 3, 17053 (2017). https://doi.org/10.1038/scsandc.2017.53
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/scsandc.2017.53
