
Abstract
Inactivation of the CDKN2A–CDKN2B locus has been reported in the most frequent subtypes of cutaneous T-cell lymphomas (CTCLs), mycosis fungoides, Sézary syndrome (SS) and CD30+ cutaneous anaplastic large cell lymphoma. To investigate whether genetic or epigenetic inactivation of CDKN2A–CDKN2B is more specifically observed in certain CTCL subtypes with clinical impact, we used array-comparative genomic hybridization, quantitative PCR, interphase fluorescent in situ hybridization and methylation analyses of p14ARF p16INK4A and p15INK4B promoters. We studied 67 samples from 58 patients with either transformed mycosis fungoides (n=24), SS (n=16) or CD30+ cutaneous anaplastic large cell lymphoma (n=18). We observed combined CDKN2A–CDKN2B deletion in both transformed mycosis fungoides (n=17, 71%) and SS patients (n=7, 44%), but, surprisingly, in only one CD30+ cutaneous anaplastic large cell lymphoma case. Interphase fluorescent in situ hybridization showed 9p21 loss in 17 out of 19 cases, with 9p21 deletion indicating either hemizygous (n=4) or homozygous (n=2) deletion, with mixed patterns in most patients (n=11). The limited size of 9p21 deletion was found to account for false-negative detection by either BAC arrays (n=9) or fluorescent in situ hybridization (n=2), especially in patients with Sézary syndrome (n=6). Methylation was found to be restricted to the p15INK4B gene promoter in patients with or without 9p21 deletion and did not correlate with prognosis. In contrast, CDKN2A–CDKN2B genetic loss was strongly associated with a shorter survival in CTCL patients (P=0.002) and more specifically at 24 months in transformed mycosis fungoides and SS patients (P=0.02). As immunohistochemistry for p16INK4A protein was not found to be informative, the genetic status of the CDKN2A–CDKN2B locus would be relevant in assessing patients with epidermotropic CTCLs in order to identify those cases where the disease was more aggressive.
Similar content being viewed by others


Main
The cell cycle, and especially G1–S progression, is controlled by the p14ARF-mdm2-p53 and p16INK4A/p15INK4B-Rb1 pathways (reviewed by Sharpless and DePinho1). Both p16INK4A and p15INK4B proteins are able to induce cell-cycle arrest in the G1 phase by inhibiting the cyclin-dependent kinases CDK4- and CDK6-mediated phosphorylation of the retinoblastoma protein that is required for cell-cycle progression (reviewed by Barbacid et al2 and Ortega et al3). The p14ARF protein mainly acts on the MDM2–p53 pathway, inducing either cell cycle arrest or apoptosis (reviewed by Sherr et al4 and Gil and Peters5).
Interestingly, the p14ARF, p16INK4A and p15INK4B proteins are encoded by the same CDKN2A–CDKN2B locus on the chromosomal band 9p21: p15INK4B is encoded by CDKN2B and p14ARF and p16INK4A are encoded by an alternative reading frame of CDKN2A.1 The two proteins p14ARF and p16INK4A are translated after transcription control of separate promoters and their respective transcripts contain a specific first exon (exon-E1β and exon-E1α, respectively) but share exon-2- and 3-encoded sequences.6 The entire CDKN2A–CDKN2B locus is frequently lost and/or mutated in a wide range of human primary solid and hematopoietic neoplasias.7, 8 Restricted genetic losses or epigenetic silencing by promoter hypermethylation has also been described in solid tumors and skin cancers.9, 10, 11, 12, 13
Epidermotropic cutaneous T-cell lymphomas (CTCLs), that is, mycosis fungoides and Sézary syndrome (SS), account for more than 50% of cutaneous lymphomas.14, 15 The early tumor node metastasis (TNM) stages of mycosis fungoides (Ia–IIa) are characterized by limited skin lesions, patches or plaques, and a low proportion (10–20%) of neoplastic T-cells in the upper dermis and epidermis. In advanced stages (IIb–IVb), tumor cells become more abundant and epidermotropism may be lost.14 SS occurs de novo in advanced stages (III or IV) and involves more than 90% of the skin (erythroderma), with generalized lymphadenopathy and neoplastic T-cells, coined Sézary cells, in the skin, lymph nodes and peripheral blood.14 In patients with SS, tumor cells may be scarce in skin biopsies and blood rating is a valuable way to rank patients with low blood involvement (B1 stage) and high blood burden (B2 stage), with more than 1000 atypical cells per microliter.15
In patients with either mycosis fungoides or SS, transformation occurs with the presence of more than 25% of large cells within dense dermal infiltrates, and is more commonly associated with skin tumors than plaques or erythrodermic lesions.15, 16, 17 Transformation of mycosis fungoides offers poor prognosis, with extracutaneous spread and a median survival of less than 2 years.17, 18 In SS, transformation into large cells may also occur at either the blood or skin level.19 In epidermotropic CTCLs, progression to advanced stage, large cell transformation or leukemic B2 phase can take place within 2 years, defining patients with rapid progressive disease and poor survival.16 Conversely, primary CD30+ cutaneous anaplastic large cell lymphoma corresponds to solitary or localized skin nodules or tumors composed of a non-epidermotropic infiltrate of large T-cells expressing the CD30 antigen (>75%).14 Most patients are cured, sometimes by spontaneous regression or more frequently by local therapy (excision or radiotherapy), and the 10-year survival rate is over 90%.20 However, CD30+ cutaneous anaplastic large cell lymphoma may be harmful in about one-third of patients presenting either large tumoral skin lesions or multiple skin relapse.14, 20
It has been suggested by specific genetic analyses that CDKN2A–CDKN2B loss may be a predictive criterion for CTCL and for patients' prognosis and management. Using microsatellite markers surrounding the CDKN2A–CDKN2B locus, loss of heterozygosity (LOH), suggesting either hemizygous or homozygous deletion, was indeed detected equally in the early and late stages of mycosis fungoides (21%) and SS (37%) cases (25% of epidermotropic CTCL).21 Another group suggested that LOH or homozygous deletion was not present in patients with early-stage and stable mycosis fungoides (n=21), but appeared during the tumoral progression of mycosis fungoides (3 out of 11 samples).22 Interestingly, no point mutation of either p16INK4A or p15INK4B genes was found, but aberrant 5′-CpG island methylation of either p16INK4A and/or p15INK4B, but not of p14ARF, was detected.21, 22, 23 In SS, selective hypermethylation of p15INK4B but not p14ARF or p16INK4A was observed in 42% of cases,21, 24 a pattern not seen in aggressive mycosis fungoides.22 Using enrichment in tumor cells by microdissection of 25 skin samples, LOH was similarly observed in two out of 15 plaque-stage mycosis fungoides and in two out of 10 tumor-stage mycosis fungoides.25 A similar approach for 11 CD30+ cutaneous anaplastic large cell lymphomas revealed LOH at 9p21 locus but not at 17p13 in 64% of cases.26 Conventional cytogenetic and comparative genomic hybridization analysis of 28 SS cases, combined with literature survey of 274 SS karyotypes, did not identify 9p21 loss as a cytogenetic feature of SS.27 Nor did comparative genomic hybridization studies of both mycosis fungoides and SS cases find 9p21 loss as a recurrent imbalance of these lymphomas.28, 29 However, recent array-comparative genomic hybridization data obtained by the Leiden University group identified 9p21 loss in 41% of patients, with mycosis fungoides associated with lower survival rate.30, 31 By comparison, the deletion was not found in patients with SS.30, 31 Whether 9p21 deletion could be detected by interphase fluorescent in situ hybridization was not determined.
In order to assess the genetic and epigenetic status of the CDKN2A–CDKN2B locus in the main CTCL subtypes, we investigated 69 samples with high tumor-cell content. We used a combination of array-comparative genomic hybridization, locus-specific interphase fluorescent in situ hybridization analysis, real-time quantitative PCR and real-time quantitative methylation-specific PCR. The results were analyzed along with evolutive features in order to determine the clinical relevance of our findings.
Materials and methods
Patients and Materials
We selected 58 patients with primary CTCL: 24 with transformed mycosis fungoides, 13 with primary SS, 3 with secondary SS and 18 with CD30+ cutaneous anaplastic large cell lymphomas, on the basis of available fresh frozen material and informed consent in accordance with French bioethical law. Their main features are summarized in Table 1. In the 24 patients with transformed mycosis fungoides, 29 samples were analyzed either from skin (n=24), blood (n=3), node (n=1) or spleen (n=1). In the 16 patients with SS, only blood samples were studied (n=16). In the 18 patients with CD30+ cutaneous anaplastic large cell lymphomas, 22 samples were obtained from skin (n=18), blood (n=2) or lymph node (n=2). All patients with CD30+ cutaneous anaplastic large cell lymphoma had cutaneous nodules or tumors, with more than 75% of CD30+ ALK-large anaplastic cells. Both epidermotropic and non-epidermotropic CTCL updated criteria were used to assess TNM stages.15, 32
High-molecular-weight DNA was extracted from fresh frozen tissue samples by proteinase-K digestion and phenol/chloroform extraction. For uncultured peripheral blood lymphocytes, a salt-extraction method was used as previously described.33
Array-Comparative Genomic Hybridization
Array-based comparative genomic hybridization was performed on bacterial artificial chromosome (BAC) microarrays consisting of 3113 (3K) BAC clones (Integrachip; IntegraGen, Evry, France) or 5600 (5K) BAC clones (version 7: V7; Integragen), with coverage of the human genome at 0.5–1-Mb resolution. BAC clones were spotted in quadruplicates onto glass slides.
As shown in Supplementary Figure 1, chromosome-9 was covered by 115 BAC clones in the 3K array and the 9p21 region by 17 clones spanning from 9p21.1 to 9p21.3. For the 5K array, chromosome-9 was covered by 197 clones and the 9p21 region by 26 clones, including the BAC clone RP11-149I2 specific for p16INK4A/CDKN2A locus.
The test and reference DNAs (600 ng) were labeled by random priming (Fisher Scientific Bioblock, Illkirch, France) using Cy3-dCTP and Cy5-dCTP, respectively (GE Healthcare, Orsay, France). Reference DNA was derived from whole-blood cell extraction from 20 healthy individuals. Unincorporated nucleotides were removed using Microcon YM-30 (Millipore, Paris, France). Labeled test and reference DNAs were mixed with 150 μg of Cot-1 DNA (Roche, Meylan, France), 100 μg of Salmon sperm DNA (Fisher Scientific Bioblock) and ethanol-precipitated. The pellet was dissolved in 68 μl of hybridization buffer (2xSSC, 10% dextran sulfate, 50% formamide and milliQ water). Probes were denatured for 1 min 30 s at 100°C, cooled down for 5 min at 4°C and incubated at 37°C for 30 min to allow blocking of repetitive sequences.
Hybridization was performed for 17 h at 37°C using a specific device (Corning, Schiphol-Rijk, the Netherlands). Slides were washed at 54°C for 5 min in 2xSCC, 0.1% SDS, twice at room temperature for 5 min in 1xSSC, 5 min in 0.2xSCC, 2 min in milliQ water, rapidly dipped and removed 15 times in isopropanol and finally dried.
Arrays were scanned using a ScanArray 4000XL (Perkin Elmer, Courtaboeuf, France). GenePix Pro V4.0 software (Axon Instruments, Saint Grégoire, France) was used to locate features automatically and to measure fluorescence intensities for Cy3 and Cy5 channels. Data analysis was performed using a Curie Institute VAMP tool through the CAPweb bioinformatics platform (http://bioinfo-out.curie.fr/CAPweb/). An assay was retained if more than 90% of BAC clones presented a good signal-to-noise ratio of at least 3.
In order to refine BAC array-CGH data, 10 samples (Table 2) were also analyzed on a 105 K Agilent's Human Genome oligonucleotide microarray with an average resolution of 21.7 kb (Agilent Technologies, Massy, France). The hybridization and scanning protocols were performed as recommended by the manufacturer (Agilent Technologies). In brief, either male or female reference DNA (Promega, Charbonnieres, France) and tumor DNA was digested using Alu1 and Rsa1 (Promega). The test and reference DNAs were labeled by random priming (Agilent Technologies) with Cy3–dCTP and Cy5–dCTP (GE Healthcare), respectively, purified with Microcon YM-30 (Millipore) and combined. The hybridization mixture contained the labeled DNAs, 2 × hybridization buffer (Agilent), 10 × blocking agent (Agilent) and Human Cot-1 DNA (Invitrogen). Scanning was performed with a G2565BA device using Agilent Feature Extraction software 9.5, then imported into Agilent CGH analytics 3.5 software for analysis.
Fluorescent In Situ Hybridization Signal for 9p21 Locus
To determine the percentage of cells with 9p21 deletion, dual-color fluorescent in situ hybridization was performed either on conventional cytogenetic preparations after short-term cultures, interphase nuclei isolated from fresh tumors or from formalin-fixed, paraffin-embedded tissues, or on frozen tumor imprints as described by Marty et al.34 The probe set contains both chromosome-9 centromere-specific (CEP-9, Spectrum Green) and locus-specific 9p21 (Spectrum Orange) probes (Abbott Molecular, Rungis, France). For each sample, 100 tumor cells or nuclei were individually scored using a fluorescence microscope (Zeiss, Jena, Germany) equipped with appropriate band-pass filters. Images were captured through a high-resolution camera (JAI M300) with the ISIS software (MetaSystems, Altlussheim, Germany). The ratio between locus-specific and centromere signals in individual cells allowed us to classify samples either as normal or as deleted above a 5% threshold of cells showing either a monoallelic (1/2, 3/4) or billalelic (0/2, 0/4,..) pattern.35
Real-Time Quantitative PCR
The genetic dosage of three different exons and the reference gene Albumin was determined by real-time quantitative PCR using specific primers and their corresponding hydrolysis probes using an Mx4000 real-time PCR detection system (Stratagene, Massy, France). The probes and primers were synthesized by Eurogentec (Angers, France) according to the published sequences given in Supplementary Table 1.36, 37, 38 Specificity was checked by melting-curve analysis using Mesagreen Q-PCR master mix plus (Eurogentec). Amplification reactions (25 μl) were performed in duplicate with 10 ng of genomic DNA, 200 nM of each primer, 300 nM hydrolysis probes and 12.5 μl of Q-PCR Master mix Kit (Eurogentec). Each PCR included 95°C for 10 min, followed by 40 cycles at 95°C for 15 s, 60°C for 1 min and 72°C for 30 s. A five-point standard curve established by serial dilution of healthy donor DNA ranging from 25 to 1.6 ng of DNA was included in each PCR experiment. The normalization of DNA input at 10 ng was shown by the same Ct value for albumin for all samples (less than 1 Ct variation). An arbitrary amount of each exon input was calculated against the calibration curve. Next, the ratio of target exon to the Albumin reference exon was established and expected to be around 1 in the absence of imbalance.38 The DNA of the LN401 glioblastoma cell line (gift of Dr A Merlo, University Hospital, Basel, Switzerland) with homozygous deletion at the INK4A locus provided a 0 ratio value.36 Five healthy control DNAs were used to determine threshold values (mean±2 s.d.) as follows: 1.30–0.84 for exon-1α of p16INK4A/CDKN2A, 1.25–0.86 for exon-2 of p16INK4A/CDKN2A and p14ARF 1.20–0.83 for exon-1 of p15INK4B/CDKN2B.
Bisulfite-Modification and Methylation-Specific PCR
The methylation status of the p14ARF, p15INK4B and p16INK4A promoter region was determined by methylation-specific PCR after bisulfite treatment of DNA, which converts all unmethylated cytosines to uracils, as described.35, 39 After bisulfite treatment of 1 μg of DNA, a methylation-specific, real-time PCR was conducted using 1 μl (40 ng) of bisulfite-modified DNA and the primer designed for methylated and unmethylated p14ARF, p15INK4B and p16INK4A promoter genes.40, 41 The sequence of primer pairs for both methylated and unmethylated promoter genes and their corresponding probes are provided in Supplementary Table 2. Real-time amplification was performed and analyzed with an MX 4000 real-time PCR device (Stratagene). DNA derived from HDLM2 cell line (gift from Dr JF Garcia, CNIO, Madrid, Spain) was used as positive control for methylated p14ARF, p15INK4B and p16INK4A sequences. DNA from peripheral blood lymphocytes of a healthy donor, presenting no amplification for p14ARF, p15INK4B and p16INK4A promoter methylated sequences, served as control for unmethylated sequences.
Statistical Analysis
Correlation with clinicopathological features was performed for patients with available follow-up data, corresponding to 24 transformed mycosis fungoides, 13 primary SS, 3 secondary SS and 16 CD30+ cutaneous anaplastic large cell lymphoma. Survival analysis was performed using SAS software V 9.1 (SAS Institute, Cary, NC, USA). Overall survival was measured from the time of sampling to the date of death or last follow-up. Observations on patients lost to follow-up or alive at the last follow-up were considered to be censored. Non-parametric Kaplan–Meier survival curves and log-rank tests were calculated for all patients as well as for patients with epidermotropic CTCLs only (transformed mycosis fungoides and Sézary syndrome) after exclusion of CD30+ cutaneous anaplastic large cell lymphoma cases, as these usually display a long survival and no CDKN2A–CDKN2B loss. This latter analysis was performed at either 24 months or at the time of last data collection.
Results
To determine the genetic and epigenetic status of CDKN2A–CDKN2B genes, 67 samples from 58 patients with either transformed mycosis fungoides (n=24), primary SS (n=13), secondary SS (n=3) or CD30+ cutaneous anaplastic large cell lymphoma (n=18) were investigated by a combination of array-based comparative genomic hybridization, fluorescent in situ hybridization, quantitative PCR for genetic dosage of the p14ARF, p15INK4B and p16INK4A genes, and methylation-specific PCR for epigenetic analysis.
Patients' main clinical features, sample origin and the overall incidence of CDKN2A–CDKN2B genetic or epigenetic inactivation are summarized in Table 1.
Patients with mycosis fungoides were at transformed tumoral T3 stage and skin tumor samples were studied in all of them. A high proportion (71%) of transformed mycosis fungoides cases exhibited CDKN2A–CDKN2B genetic loss as compared with patients with other CTCL subtypes (44% in patients with SS, 6% in patients with CD30+ cutaneous anaplastic large cell lymphoma).
The results provided by the different assays are thereafter documented in Table 2 only for patients and samples showing CDKN2A–CDKN2B deletion.
Array-Comparative Genomic Hybridization Analyses
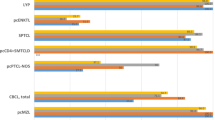
On the whole, array-based comparative genomic hybridization (either BAC or oligonucleotide array) detected CDKN2A–CDKN2B loss in 19 out of 28 tested samples from 25 patients (Figure 1). The 3K and/or 5K BAC arrays allowed the detection of 9p21 genetic loss in 13 samples and six additional samples were only found to be deleted using the 105K Oligonucleotide arrays (1, 2, 9, 19, 20, 21). As summarized in Table 2, deletion was confirmed by another technique in all cases. Interestingly, the nine array-negative samples (4, 5, 8, 10, 12, 14, 15, 22, 24) were only analyzed with a BAC array, except case-5. They were further found to carry deletion at 9p21 as detected by either fluorescent in situ hybridization assay (8, 10, 12, 14, 15, 22, 24) and/or quantitative PCR for genetic dosage (4, 5, 8, 10, 12, 14, 22, 24). The compilation of array-based comparative genomic hybridization data also allowed the evaluation of the extent of deletion, as illustrated in Figure 1 and Table 2. For some patients (3, 6b, 13, 17, 23), a large chromosome-9 or 9p deletion was observed. For most patients, deletion ranged from 2.5 to 6 Mb. Six patient samples (11, 18, 19, 20, 21 and 25) exhibited very limited deletion (less than 1 Mb) detected by either one BAC clone and/or a few oligonucleotide probes.

Array-based comparative genomic hybridization profiles of CTCL patients presenting 9p21 deletion. Array-based comparative genomic hybridization profiles obtained through the VAMP graphical tool (http://bioinfo-out.curie.fr/CAPweb/) after co-hybridization of tumoral and control DNAs. Hybridization was performed on the 3K array, except for case-19, 22, 23 and 25, which used the 5K array. These graphs represent the log2 ratio of the fluorescence intensities along chromosome-9. Gains appear in red, losses in green and balanced signals in yellow. The blue bar and the black landmark indicate the CDKN2B–CDKN2A locus and the centromere position, respectively.
Fluorescent In Situ Hybridization Testing For 9p21 Locus
To investigate 9p21 hemizygous deletion or homozygous deletion and to evaluate the proportion of cells with deletion, 30 available samples with epidermotropic CTCL were analyzed by fluorescent in situ hybridization using a 190-kb 9p21 locus-specific probe covering D9S1749, D9S1747 p16INK4A/CDKN2A, p14ARF/ARF, D9S1748, p15INK4B/CDKN2B and D9S1752. Results are summarized in Figure 2 and Table 2. Like array-based comparative genomic hybridization, fluorescent in situ hybridization also detected 9p21 deletion in a high proportion of epidermotropic CTCL samples (17 out of 30, 57%) and interestingly in seven cases not found to harbor deletion by BAC array-based comparative genomic hybridization (cases 8, 10, 12, 14, 15, 22, 24). Only six cases were found to contain a homogeneous population of cells with either hemizygous deletion (cases 13, 14, 23 and 24) or homozygous deletion (cases 7 and 21) (Figure 2b). Most cases (6, 8, 9, 10, 11, 12, 15, 20, 22) presented with a mixture of cells with hemizygous deletion and homozygous deletion and a predominance of cells showing homozygous deletion (Figure 2a). Five CD30+ cutaneous anaplastic large cell lymphoma cases were found to exhibit a normal pattern.

Interphase fluorescent in situ hybridization with Spectrum Green (CEP-9) and Spectrum Orange (9p21 locus) probes. (a) Blood sample from case-22 showing hemizygous deletion at the 9p21 locus in 40% of cells. (b) Homozygous deletion observed in 70% of blood cells from case-21. (c, d) Two green (G) and two red (R) patterns observed in 85% of blood cells from case-18, suggesting no deletion, although red signals were lower (arrowheads) than that in normal cells.
Real-Time Quantitative PCR for p15INK4b and p16INK4a Genetic Dosage
Thirty-nine samples (30 with transformed mycosis fungoides, 7 with SS and 2 with CD30+ cutaneous anaplastic large cell lymphoma) were independently analyzed. Deletion was observed for 20 out of 30 samples of patients with transformed mycosis fungoides (67%), but also in 5 out of 7 samples of patients with SS (71%). There was a very good overall concordance with the deleted or undeleted status observed by other techniques as shown in Table 2. Two cases (4 and 5), negative for 9p21 deletion by either array-based comparative genomic hybridization or fluorescent in situ hybridization techniques, were found to harbor deletion for both p16INK4A exon-1α and 2, but not for p15INK4B exon-1, suggesting an interstitial deletion. Two other cases (8 and 16) also showed partial loss but the overall majority of cases showed a common genetic loss of all three exons in accordance with array-based comparative genomic hybridization data (Table 2). Interestingly, case 18 showed a very small deletion detected by oligonucleotide array-based comparative genomic hybridization, also detected by real-time quantitative PCR, while fluorescent in situ hybridization only showed reduction in the signals provided by the commercial locus-specific probe that could not be ascertained as genetic loss (Figure 2d, arrows).
Comparison of the Different Techniques Used to Determine CDKN2A–CDKN2B Genetic Status
There was a good overall concordance between all techniques (array-comparative genomic hybridization, fluorescent in situ hybridization, genetic dosage) investigating CDKN2A–CDKN2B loss, since in 22 out of 25 cases deletion status was confirmed by at least two techniques. Conversely, 33 cases did not exhibit 9p21 deletion using all techniques (data not shown). The sensitivity of each technique for CDKN2A–CDKN2B loss detection was 36% for BAC array, 90% for oligonucleotide array-based comparative genomic hybridization, 94% for fluorescent in situ hybridization analysis and 91% for genetic dosage by quantitative PCR (96% for p16INK4A exon-1α, 88% for p16INK4A exon-2, 88% for p15INK4B exon-1 dosage, respectively). As shown in Table 2, the small size of deletion at 9p21, especially in SS cases, accounted for such results and targeted analyses such as fluorescent in situ hybridization or genetic dosage were found the most sensitive.
p14ARF, p15INK4B and p16INK4A Methylation Status
The p14ARF, p15INK4B and p16INK4A methylation status was analyzed for 41 samples (23 transformed mycosis fungoides and 18 CD30+ cutaneous anaplastic large cell lymphoma samples) by quantitative methylation-specific PCR (Table 1): among cases with CDKN2A–CDKN2B gene deletion, a restricted methylation status of p15INK4B gene was found for 12 transformed mycosis fungoides and one CD30+ cutaneous anaplastic large cell lymphoma case, whereas five cases exhibited an unmethylated profile. The methylation status of p16INK4A promoter was detected in only two cases (4 and 6) and was associated with p15INK4B gene methylation status in one case.4 Interestingly, methylation of p15INK4B gene promoter was also found in six cases without CDKN2A–CDKN2B gene deletion (1 transformed mycosis fungoides and 5 CD30+ cutaneous anaplastic large cell lymphomas). It was associated with p16INK4A-promoter methylation in another CD30+ cutaneous anaplastic large cell lymphoma case without 9p21 deletion. No methylation was detected for the p14ARF-promoter sequence in either deleted or undeleted samples.
Prognosis Implication
Fifty-six patients with CTCL had complete follow-up; 28 of them died, while two CD30+ cutaneous anaplastic large cell lymphoma cases were lost to follow-up. Twenty-three patients were found with 9p21 deletion by the above techniques and of these, 17 died (74%). Among the 33 patients without 9p21 deletion, 11 died (33%). Median overall survival was 12 months for patients with 9p21 deletion and 24 months for patients without 9p21 deletion. As shown by the survival curve in Figure 3a, overall survival was significantly shorter for patients with 9p21 deletion (P=0.002) than for patients without deletion (relative risk 2.2 (1.29–3.81)).

The prognostic value of 9p21 deletion in CTCLs. Actuarial survival curves of CTCL patients calculated from the date of biopsy using the Kaplan–Meier method. The lines correspond to patients without 9p21 deletion and dotted lines indicate patients with 9p21 deletion. The horizontal scale bar corresponds to months. (a) Survival curves of 56 CTCL patients. (b) Survival curves of 40 epidermotropic CTCL patients (that is, transformed mycosis fungoides (TMF) and SS).
Among the 16 CD30+ cutaneous anaplastic large cell lymphoma patients with follow-up, only one exhibited 9p21 deletion. The disease recurred very quickly, but remained at the skin level and the patient is still alive after 108 months and three skin relapses. Other CD30+ cutaneous anaplastic large cell lymphoma cases without 9p21 deletion exhibited either skin relapse (n=8), skin relapse and lymph node involvement (n=3), and five of them died.
Because of their usual good prognosis, we further excluded CD30+ cutaneous anaplastic large cell lymphoma patients from statistical analysis and analyzed 40 patients with epidermotropic CTCL (24 transformed mycosis fungoides and 16 SS cases). Of these patients, 25 died during follow-up (62.5%). Among the 22 patients with 9p21 deletion, 17 died (77%). Of the 18 patients without 9p21 deletion, eight (44%) died. Median overall survival was 15 months for patients with 9p21 deletion and 36 months for patients without 9p21 deletion. When performing analysis at a 24-month follow-up time, a statistical difference for a worse overall survival of patients with 9p21 deletion was found (P=0.02, relative risk 2.9 (1.14–7.19)). However, as shown in the survival curve in Figure 3b, both patients with and without 9p21 deletion had a bad prognosis after 40 months of follow-up and statistical end-point analysis showed that patients with 9p21 deletion were at the statistical significance threshold level for a shorter overall survival than patients without deletion (P=0.055, relative risk 1.7 (0.99–3.06)).
Discussion
In this paper, we have reported the study of a large sample set of patients with CTCL using a combination of genome-wide analyses, namely array-based comparative genomic hybridization, and specific genetic testing such as locus-specific fluorescent in situ hybridization and quantitative PCR to determine the presence of 9p21 deletion involving the CDKN2A–CDKN2B genes, namely p14ARF, p16INK4A and p15INK4B Our data show that CDKN2A–CDKN2B deletion is a frequent feature of late-stage epidermotropic CTCL, including transformed mycosis fungoides (71%) and SS (44%), while it is a very rare event in CD30+ cutaneous anaplastic large cell lymphoma (6%), which is in contradiction to a previous report.26 Such alteration was found to correlate with the overall survival of all patients and especially of patients with epidermotropic CTCL at 24 months of follow-up. Patients at an advanced TNM stage of mycosis fungoides or SS, and especially those with transformed mycosis fungoides, usually have a bad prognosis,16, 17 and it is even more relevant to individualize patients with a more aggressive disease at such stages in view of the choices of treatment available. Furthermore, our data point to the need for appropriate locus-specific methods to investigate the CDKN2A–CDKN2B gene, as most studies have so far relied on the use of a single method. Conventional comparative genomic hybridization studies, together with a literature compilation of 166 mycosis fungoides and SS cases, have not detected 9p21 deletion as a recurrent feature of either mycosis fungoides or SS.27, 29 Several array-based comparative genomic hybridization studies also failed to detect CDKN2A–CDKN2B deletion in patients with either mycosis fungoides or SS.42, 43 For patients with transformed mycosis fungoides, our results agree extensively with those obtained by van Doorn et al30 using a BAC array-based comparative genomic hybridization approach with 1-Mb resolution. In their study, 41% of 22 patients with transformed mycosis fungoides, had 9p21 loss involving the CDKN2A–CDKN2B locus, which is a much lower rate than that in our patients (71%). Using the same methodology, the same group did not detect 9p21 loss in 20 SS patients, which may rely on the design of probes complementary to the 9p21 locus (Supplementary Figure 1).31 In our study, a BAC array with a similar 1-Mb resolution was indeed responsible for many false-negative results, as shown by the detection of 9p21 loss by other techniques. As the CDKN2A–CDKN2B locus corresponded to the minimal common region of deletion between our cases, the locus-specific techniques were found appropriate. Generally, fluorescent in situ hybridization was found to be a valuable tool for CDKN2A–CDKN2B loss detection, showing either hemizygous (n=4) or homozygous (n=2) deletion patterns and a mixture of both patterns in most samples (n=11). This would indicate that CDKN2A–CDKN2B inactivation is an ongoing process during disease development, as other authors have suggested.22 We therefore decided, for statistical analysis purposes, to group cases with either hemizygous deletion, homozygous deletion or both against cases without deletion. The study of sequential samples or experimental models would then allow us to demonstrate such a hypothesis as previously shown for case-6 of this study.33 However, the use of a commercial 9p21 fluorescent in situ hybridization probe of 190 kb length provided two false-negative results in comparison with our real-time quantitative PCR data. Similarly, in a B-cell lymphoma case, a small 9p21 deletion of about 100 kb was recently reported to escape detection by a commercial fluorescent in situ hybridization assay as compared with its detection with a shorter probe by fluorescent in situ hybridization or by high-density oligonucleotide arrays.44 Quantitative genetic testing by multiplex PCR was also found to be reliable for systemic diffuse large B-cell lymphoma.45
Our study also resolves previous discordance between global genome analysis and specific genetic investigation of 9p21 using microsatellite markers for LOH or homozygous deletion determination.21, 22, 23 The use of polymorphic dinucleotide markers has led some groups to claim microsatellite instability in both mycosis fungoides and SS, targeting the CDKN2A–CDKN2B and IFN genes at 9p21 and also PTEN or TP53 genes at 10q23 and 17p13 loci, respectively.21, 46, 47 Recently, a careful study of frozen material with monoallelic microsatellite markers used for hereditary non-polyposis colon cancer analysis did not reveal any microsatellite instability in 12 mycosis fungoides patients with sequential samples.48 A similar observation was also made in our cases (our unpublished results) and CDKN2A–CDKN2B allelic loss is unlikely to be the result of microsatellite instability. The analysis of LOH using polymorphic microsatellite markers may also be difficult when studying formalin-fixed material and/or microdissected specimens, especially in epidermotropic CTCL with chromosomal changes involving 9p, 10q and 17p.25, 30, 31, 49 Using LOH analysis of microdissected specimens, Böni et al26 observed LOH at 9p21, suggesting 9p21 deletion in 64% of 11 CD30+ cutaneous anaplastic large cell lymphoma, a finding not confirmed by this study. Whether mitotic recombination with copy-neutral LOH could account for such divergence should be assessed further by single-nucleotide polymorphism evaluation.
More interestingly, in the majority of our cases, CDKN2A–CDKN2B deletion targeted all three p14ARF p16INK4A and p15INK4B genes, as determined by real-time quantitative PCR. Mice deficient for all three open reading frames (CDKN2AB−/−) are more tumor prone and develop a wider spectrum of tumors, especially of the skin, than CDKN2A mutants.50 Experimental models primarily showed that both p14ARF and p16INK4A are both strong tumor suppressors and that CDNK2A gene loss confers resistance to chemotherapy in experimental lymphoma.1, 5 Moreover, the p15INK4B gene, considered a functional surrogate for p16INK4A, is a critical tumor suppressor in the absence of p16INK4A.50 Interestingly, a specific pattern of p15INK4B-promoter methylation was observed in CTCL cases (transformed mycosis fungoides and CD30+ cutaneous anaplastic large cell lymphoma), whereas p14ARF and p16INK4A promoters were found either unmethylated or very rarely methylated, respectively. A specific methylation of the p15INK4B promoter has been reported in several tumors, especially in adult acute myelogenous leukemia.51 However, selective methylation of the p15INK4B promoter has been observed in systemic CD30+ anaplastic lymphoma independently from CDKN2A–CDKN2B genetic loss, as in our CTCL cases.52 Epigenetic profiling already showed p15INK4B promoter methylation in about 10% of CTCL cases.53 Methylation of CDKN2A–CDKN2B gene promoters was not specifically observed in our epidermotropic CTCL cases with deletion, and cases with homozygous deletion (cases 6 and 7) also exhibited p15INK4B promoter methylation that could be carried by non-tumor cells. The absence of CDKN2A–CDKN2B locus epigenetic global silencing does not support the use of demethylating agents in clinical trials of CTCL.
More importantly, in 40 epidermotropic CTCL cases we found a statistical correlation with overall survival at 24 months, as recently reported in another study of 20 transformed mycosis fungoides at a similar follow-up duration.30 Our data also extend such finding to patients with SS and provide a rationale for genetic testing in clinical trials, as transformed mycosis fungoides patients have a mean survival of about 22 months.16, 17
We were unable to ascertain such genetic loss by immunohistochemistry, as most cases without deletion were also found to be negative for p16INK4A immunoreactivity (our unpublished data), as reported by others.54 Only positive immunostaining of tumor cells for p16INK4A could predict the absence of 9p21 loss in mycosis fungoides.22 Similarly, in cutaneous B-cell large cell lymphoma leg-type, CDKN2a homozygous or hemizygous deletion and promoter silencing by 5′-CpG island methylation has been repeatedly shown to be a strong adverse prognosis factor.55, 56 Such losses could also not be assessed by immunohistochemical analysis of fixed specimens.35, 56 Recently, multiplex ligation-dependent probe amplification has been found to be a reliable tool to assess CDKN2A–CDKN2B deletion in 64 formalin-fixed cutaneous B-cell large cell lymphoma leg-type cases.57
Finally, we observed CDKN2A–CDKN2B deletion in a high proportion of patients with advanced-stage epidermotropic CTCL. In such patients, the genetic status of the CDKN2A–CDKN2B locus had a significant prognostic impact and should be evaluated for its independent prognostic value in prospective therapeutic trials. Targeted analyses such as interphase fluorescent in situ hybridization or quantitative PCR for genetic dosage were found to be the most efficient techniques for such a purpose.
References
Sharpless NE, DePinho RA . The INK4A/ARF locus and its two gene products. Curr Opin Genet Dev 1999;9:22–30.
Barbacid M, Ortega S, Sotillo R, et al. Cell cycle and cancer: genetic analysis of the role of cyclin-dependent kinases. Cold Spring Harb Symp Quant Biol 2005;70:233–240.
Ortega S, Malumbres M, Barbacid M . Cyclin D-dependent kinases, INK4 inhibitors and cancer. Biochim Biophys Acta 2002;1602:73–87.
Sherr CJ, Bertwistle D, W DENB, et al. p53-dependent and -independent functions of the Arf tumor suppressor. Cold Spring Harb Symp Quant Biol 2005;70:129–137.
Gil J, Peters G . Regulation of the INK4b-ARF-INK4a tumour suppressor locus: all for one or one for all. Nat Rev Mol Cell Biol 2006;7:667–677.
Quelle DE, Zindy F, Ashmun RA, et al. Alternative reading frames of the INK4a tumor suppressor gene encode two unrelated proteins capable of inducing cell cycle arrest. Cell 1995;83:993–1000.
Roussel MF . The INK4 family of cell cycle inhibitors in cancer. Oncogene 1999;18:5311–5317.
Pinyol M, Cobo F, Bea S, et al. p16(INK4a) gene inactivation by deletions, mutations, and hypermethylation is associated with transformed and aggressive variants of non-Hodgkin's lymphomas. Blood 1998;91:2977–2984.
Licchesi JD, Westra WH, Hooker CM, et al. Promoter hypermethylation of hallmark cancer genes in atypical adenomatous hyperplasia of the lung. Clin Cancer Res 2008;14:2570–2578.
Herman JG, Merlo A, Mao L, et al. Inactivation of the CDKN2/p16/MTS1 gene is frequently associated with aberrant DNA methylation in all common human cancers. Cancer Res 1995;55:4525–4530.
van Doorn R, Gruis NA, Willemze R, et al. Aberrant DNA methylation in cutaneous malignancies. Semin Oncol 2005;32:479–487.
Pacifico A, Goldberg LH, Peris K, et al. Loss of CDKN2A and p14ARF expression occurs frequently in human nonmelanoma skin cancers. Br J Dermatol 2008;158:291–297.
Badal V, Menendez S, Coomber D, et al. Regulation of the p14ARF promoter by DNA methylation. Cell Cycle 2008;7:112–119.
Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005;105:3768–3785.
Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sézary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood 2007;110:1713–1722.
Diamandidou E, Colome-Grimmer M, Fayad L, et al. Transformation of mycosis fungoides/Sézary syndrome: clinical characteristics and prognosis. Blood 1998;92:1150–1159.
Vergier B, de Muret A, Beylot-Barry M, et al. Transformation of mycosis fungoides: clinicopathological and prognostic features of 45 cases. French Study Group of Cutaneous Lymphomas. Blood 2000;95:2212–2218.
Siegel RS, Pandolfino T, Guitart J, et al. Primary cutaneous T-cell lymphoma: review and current concepts. J Clin Oncol 2000;18:2908–2925.
D'Alessandro E, De Pasquale A, Ligas C, et al. Cytogenetic findings in terminal large cell transformation in a case of Sézary syndrome. Cancer Genet Cytogenet 1992;58:100–104.
Bekkenk MW, Geelen FA, van Voorst Vader PC, et al. Primary and secondary cutaneous CD30(+) lymphoproliferative disorders: a report from the Dutch Cutaneous Lymphoma Group on the long-term follow-up data of 219 patients and guidelines for diagnosis and treatment. Blood 2000;95:3653–3661.
Scarisbrick JJ, Woolford AJ, Calonje E, et al. Frequent abnormalities of the p15 and p16 genes in mycosis fungoides and Sézary syndrome. J Invest Dermatol 2002;118:493–499.
Navas IC, Algara P, Mateo M, et al. p16(INK4a) is selectively silenced in the tumoral progression of mycosis fungoides. Lab Invest 2002;82:123–132.
Navas IC, Ortiz-Romero PL, Villuendas R, et al. p16(INK4a) gene alterations are frequent in lesions of mycosis fungoides. Am J Pathol 2000;156:1565–1572.
Gallardo F, Esteller M, Pujol RM, et al. Methylation status of the p15, p16 and MGMT promoter genes in primary cutaneous T-cell lymphomas. Haematologica 2004;89:1401–1403.
Katona TM, O'Malley DP, Cheng L, et al. Loss of heterozygosity analysis identifies genetic abnormalities in mycosis fungoides and specific loci associated with disease progression. Am J Surg Pathol 2007;31:1552–1556.
Boni R, Xin H, Kamarashev J, et al. Allelic deletion at 9p21–22 in primary cutaneous CD30+ large cell lymphoma. J Invest Dermatol 2000;115:1104–1107.
Mao X, Lillington DM, Czepulkowski B, et al. Molecular cytogenetic characterization of Sézary syndrome. Genes Chromosomes Cancer 2003;36:250–260.
Mao X, Lillington D, Scarisbrick JJ, et al. Molecular cytogenetic analysis of cutaneous T-cell lymphomas: identification of common genetic alterations in Sézary syndrome and mycosis fungoides. Br J Dermatol 2002;147:464–475.
Fischer TC, Gellrich S, Muche JM, et al. Genomic aberrations and survival in cutaneous T cell lymphomas. J Invest Dermatol 2004;122:579–586.
van Doorn R, van Kester MS, Dijkman R, et al. Oncogenomic analysis of mycosis fungoides reveals major differences with Sézary syndrome. Blood 2009;113:127–136.
Vermeer MH, van Doorn R, Dijkman R, et al. Novel and highly recurrent chromosomal alterations in Sézary syndrome. Cancer Res 2008;68:2689–2698.
Kim YH, Willemze R, Pimpinelli N, et al. TNM classification system for primary cutaneous lymphomas other than mycosis fungoides and Sézary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the Cutaneous Lymphoma Task Force of the European Organization of Research and Treatment of Cancer (EORTC). Blood 2007;110:479–484.
Prochazkova M, Chevret E, Beylot-Barry M, et al. Large cell transformation of mycosis fungoides: tetraploidization within skin tumor large cells. Cancer Genet Cytogenet 2005;163:1–6.
Marty M, Prochazkova M, Laharanne E, et al. Primary cutaneous T-cell lymphomas do not show specific NAV3 gene deletion or translocation. J Invest Dermatol 2008;128:2458–2466.
Belaud-Rotureau MA, Marietta V, Vergier B, et al. Inactivation of p16INK4a/CDKN2A gene may be a diagnostic feature of large B cell lymphoma leg type among cutaneous B cell lymphomas. Virchows Arch 2008;452:607–620.
Labuhn M, Jones G, Speel EJ, et al. Quantitative real-time PCR does not show selective targeting of p14(ARF) but concomitant inactivation of both p16(INK4A) and p14(ARF) in 105 human primary gliomas. Oncogene 2001;20:1103–1109.
Bertin R, Acquaviva C, Mirebeau D, et al. CDKN2A, CDKN2B, and MTAP gene dosage permits precise characterization of mono- and bi-allelic 9p21 deletions in childhood acute lymphoblastic leukemia. Genes Chromosomes Cancer 2003;37:44–57.
Hostein I, Pelmus M, Aurias A, et al. Evaluation of MDM2 and CDK4 amplification by real-time PCR on paraffin wax-embedded material: a potential tool for the diagnosis of atypical lipomatous tumours/well-differentiated liposarcomas. J Pathol 2004;202:95–102.
Lehmann U, Hasemeier B, Lilischkis R, et al. Quantitative analysis of promoter hypermethylation in laser-microdissected archival specimens. Lab Invest 2001;81:635–638.
Esteller M, Tortola S, Toyota M, et al. Hypermethylation-associated inactivation of p14(ARF) is independent of p16(INK4a) methylation and p53 mutational status. Cancer Res 2000;60:129–133.
Lehmann U, Kreipe H . Real-time PCR-based assay for quantitative determination of methylation status. Methods Mol Biol 2004;287:207–218.
Carbone A, Bernardini L, Valenzano F, et al. Array-based comparative genomic hybridization in early-stage mycosis fungoides: recurrent deletion of tumor suppressor genes BCL7A, SMAC/DIABLO, and RHOF. Genes Chromosomes Cancer 2008;47:1067–1075.
Mao X, Orchard G, Lillington DM, et al. Amplification and overexpression of JUNB is associated with primary cutaneous T-cell lymphomas. Blood 2003;101:1513–1519.
Wiesner T, Obenauf AC, Geigl JB, et al. 9p21 deletion in primary cutaneous large B-cell lymphoma, leg type, may escape detection by standard FISH assays. J Invest Dermatol 2009;129:238–240.
Jardin F, Ruminy P, Kerckaert JP, et al. Detection of somatic quantitative genetic alterations by multiplex polymerase chain reaction for the prediction of outcome in diffuse large B-cell lymphomas. Haematologica 2008;93:543–550.
Scarisbrick JJ, Woolford AJ, Russell-Jones R, et al. Loss of heterozygosity on 10q and microsatellite instability in advanced stages of primary cutaneous T-cell lymphoma and possible association with homozygous deletion of PTEN. Blood 2000;95:2937–2942.
Scarisbrick JJ, Woolford AJ, Russell-Jones R, et al. Allelotyping in mycosis fungoides and Sézary syndrome: common regions of allelic loss identified on 9p, 10q, and 17p. J Invest Dermatol 2001;117:663–670.
Assaf C, Sanchez JA, Lukowsky A, et al. Absence of microsatellite instability and lack of evidence for subclone diversification in the pathogenesis and progression of mycosis fungoides. J Invest Dermatol 2007;127:1752–1761.
Prochazkova M, Chevret E, Mainhaguiet G, et al. Common chromosomal abnormalities in mycosis fungoides transformation. Genes Chromosomes Cancer 2007;46:828–838.
Krimpenfort P, Ijpenberg A, Song JY, et al. p15Ink4b is a critical tumour suppressor in the absence of p16Ink4a. Nature 2007;448:943–946.
Herman JG, Civin CI, Issa JP, et al. Distinct patterns of inactivation of p15INK4B and p16INK4A characterize the major types of hematological malignancies. Cancer Res 1997;57:837–841.
Garcia MJ, Martinez-Delgado B, Cebrian A, et al. Different incidence and pattern of p15INK4b and p16INK4a promoter region hypermethylation in Hodgkin's and CD30-positive non-Hodgkin's lymphomas. Am J Pathol 2002;161:1007–1013.
van Doorn R, Zoutman WH, Dijkman R, et al. Epigenetic profiling of cutaneous T-cell lymphoma: promoter hypermethylation of multiple tumor suppressor genes including BCL7a, PTPRG, and p73. J Clin Oncol 2005;23:3886–3896.
Zhang C, Toulev A, Kamarashev J, et al. Consequences of p16 tumor suppressor gene inactivation in mycosis fungoides and Sézary syndrome and role of the bmi-1 and ras oncogenes in disease progression. Hum Pathol 2007;38:995–1002.
Dijkman R, Tensen CP, Jordanova ES, et al. Array-based comparative genomic hybridization analysis reveals recurrent chromosomal alterations and prognostic parameters in primary cutaneous large B-cell lymphoma. J Clin Oncol 2006;24:296–305.
Senff NJ, Hoefnagel JJ, Jansen PM, et al. Reclassification of 300 primary cutaneous B-cell lymphomas according to the new WHO-EORTC classification for cutaneous lymphomas: comparison with previous classifications and identification of prognostic markers. J Clin Oncol 2007;25:1581–1587.
Senff NJ, Zoutman WH, Vermeer MH, et al. Fine-mapping chromosomal loss at 9p21: correlation with prognosis in primary cutaneous diffuse large B-cell lymphoma, leg type. J Invest Dermatol 2009;129:1149–1155.
Acknowledgements
This work was supported by grants from the Ligue Nationale contre le Cancer, Comité de Gironde, the INSERM (grant no. 4CR03G) and Institut National contre le Cancer (INCa) through the Cancéropôle Grand Sud-Ouest (grant ACI 2004-2007 and IGEPAP). EL was supported by a PhD fellowship (2006–2008) from the French Research and Education Ministry. We also thank Professor M D'Incan (CHU Clermont-Ferrand) and Professor L Vaillant and Dr A de Muret (CHU Tours) for providing one CD30+ cutaneous anaplastic large cell lymphoma case each.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure/conflict of interest
The authors declare no conflict of interest.
Supplementary Information accompanies the paper on Modern Pathology website
Rights and permissions
About this article
Cite this article
Laharanne, E., Chevret, E., Idrissi, Y. et al. CDKN2A–CDKN2B deletion defines an aggressive subset of cutaneous T-cell lymphoma. Mod Pathol 23, 547–558 (2010). https://doi.org/10.1038/modpathol.2009.196
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/modpathol.2009.196
Keywords
This article is cited by
-
T cell receptor β-chain-targeting chimeric antigen receptor T cells against T cell malignancies
Nature Communications (2022)
-
Cutaneous T cell lymphoma
Nature Reviews Disease Primers (2021)
-
Cellular origins and genetic landscape of cutaneous gamma delta T cell lymphomas
Nature Communications (2020)
-
MicroRNA-16 mediates the regulation of a senescence–apoptosis switch in cutaneous T-cell and other non-Hodgkin lymphomas
Oncogene (2016)
-
Sézary Syndrome: Clinical and Biological Aspects
Current Hematologic Malignancy Reports (2016)

{kind=link}