
Abstract
BK polyomavirus (BKPyV) causes major complications in solid organ transplant recipients but little is known about its role in the development of urothelial carcinoma (UC) during immunosuppression. Immunohistochemistry (IHC) screening for polyomavirus large T antigen (LTag) was performed in 94 micropapillary UC (MPUC), 480 unselected UC, 199 muscle invasive UC (including 83 UC with variant differentiation), 76 cases of plasmocytoid, nested and large nested UC and 15 posttransplant UC. LTag expressing UC were reevaluated regarding their histomorphological features and characterized by IHC for p53 and HER2, chromogenic in situ hybridization for HER2 and SNaPshot analysis of the TERT promoter and HRAS. Real-time PCR and next generation sequencing (NGS) were performed to search for BKPyV-DNA and for variants in the tumor and viral genomes. We detected five LTag expressing UC which were diagnosed between 2 and 18 years after kidney (n = 4) or heart (n = 1) transplantation. 89 MPUC without history of organ transplantation and overall 755 UC (including cases with variant histology) were LTag negative. Of the five LTag expressing UC, three were MPUC, one showed extensive divergent differentiation with Mullerian type clear cell carcinoma, and one displayed focal villoglandular differentiation. All five tumors had aberrant nuclear p53 expression, 2/5 were HER2-amplified, and 3/5 had TERT promoter mutations. Within the 50 most common cancer related genes altered in UC we detected very few alterations and no TP53 mutations. BKPyV-DNA was present in 5/5 UC, chromosomal integration of the BKPyV genome was detectable in 4/5 UC. Two UC with BKPyV integration showed small deletions in the BKPyV noncoding control region (NCCR). The only UC without detectable BKPyV integration had a high viral load of human herpesvirus 6 (HHV-6). Our results suggest that LTag expression of integrated BKPyV genomes and resulting p53 inactivation lead to aggressive high-grade UC with unusual, often micropapillary morphology.
Similar content being viewed by others


Introduction
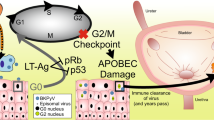
Solid organ transplantation is the only definite treatment of end-stage organ failure but lifelong immunosuppression leads to an increased risk of viral infections and malignancies [1, 2]. One frequent complication after kidney transplantation is polyomavirus associated nephropathy, predominantly caused by the human BK polyomavirus (BKPyV). BKPyV was described in 1971 [3] as the first member of the human polyomavirus family which now comprises 14 viruses [4]. Polyomaviruses are small DNA viruses which encode two early mRNAs that are translated into the large T antigen (LTag) and the small T antigen. LTag is able to bind and block the tumor suppressor functions of p53 and pRB [5]. The oncogenic potential of polyomaviruses has been studied extensively [6, 7] and a causative role has been shown for Merkel cell polyomavirus (MCPyV) in Merkel cell carcinoma of the skin [8].
BKPyV is widely distributed with an overall IgG antibody seroprevalence rate of about 80% [9]. Primary infection usually occurs during childhood and is followed by latency of BKPyV mainly in renal epithelial cells and transitional cells of the urogenital tract, but also in tonsils, lymphocytes, blood monocytes, and brain [5, 10]. Immunosuppression can cause BKPyV reactivation with lytic replication in permissive tissues. Although lytic infection can often be asymptomatic and transient, ongoing high level virus replication leads to urothelial or renal injury. Resulting polyomavirus associated nephropathy occurs in a significant percentage of kidney transplant recipients and often leads to graft failure and transplant loss [11], BKPyV-associated hemorrhagic cystitis is a common complication after allogeneic hematopoietic stem cell transplantation [12]. For BKPyV, an association between BKPyV reactivation and an increased incidence of UC in renal transplant recipients has initially been observed [13, 14]. Up to date, <50 BKPyV-associated posttransplant UC have been reported [15, 16]. These tumors affect tissues of BKPyV latency and usually occur in kidney transplants or in the recipients' bladder. It is assumed that asymptomatic latent or productive lytic infections lead to rare genetic accidents with integration of BKPyV genomes. Tumor cells typically show strong expression of polyomavirus LTag but no productive/lytic infection [10]. BKPyV-associated tumors often display a variant morphology, e.g., micropapillary UC (MPUC), an aggressive UC variant with frequent TP53 mutations, and HER2 alterations [15, 17]. NGS based data are available for <20 BKPyV-associated UC [16, 18,19,20,21,22]. We performed a molecular study for another five cases of this rare and probably underrecognized entity.
Materials and methods
Case selection
Tissue microarrays (TMA) [23] containing 94 MPUC collected from archival material of nine cooperating centers in Germany and France were screened for polyomavirus LTag expression by immunostaining with a SV40 LTag epitope cross reacting antibody.
We also screened large series of consecutive UC, including other histopathological variants. In detail a TMA of 480 consecutive UC diagnosed in our department from 1998 until 2004 including variant UC (n = 21 MPUC, n = 11 sarcomatoid, n = 4 plasmacytoid, n = 1 lymphoepithelioma-like, n = 1 nested, n = 2 neuroendocrine) and a TMA with 199 consecutive muscle invasive UC treated with radical cystectomy and also including variant UC (n = 10 MPUC, n = 10 sarcomatoid, n = 10 neuroendocrine, n = 7 plasmacytoid, n = 2 lymphoepithelioma-like, n = 2 nested, n = 1 clear cell, n = 1 large nested) [24] was investigated by immunohistochemistry (IHC). Furthermore specific TMAs of our studies of UC with variant histology were screened with IHC, including 24 plasmocytoid, 33 nested, and 19 large nested carcinomas.
A retrospective search of the records of the departments of surgical pathology and nephropathology (University Hospital Erlangen) including routine and consult cases was performed to identify UC in solid organ transplant recipients for subsequent LTag immunostaining. Institutional review board approval (University Hospital Erlangen) was obtained for molecular analysis of archival material.
Morphology and IHC
Complete histomorphological reevaluation of hematoxylin and eosin (H&E)-stained tumor slides of the five LTag expressing UC was done according to the current TNM and WHO classification systems [25, 26] by two experienced uropathologists (AH, SB).
IHC was performed on a fully automated IHC slide staining system (BenchMark XT System, Ventana Medical Systems Inc., Tucson, AZ) using the following antibodies: p53 (DAKO, DO-7, 1:50), SV40 (Abcam, PAb416, 1:1000), and Her2 (Dako, Poly, 1:1000). Additional GATA3 (DCS, L50–823, 1:1000) and PAX8 (Cell Marque, Poly, 1:50) staining was performed for cases 3 and 4 to clarify that these tumors are UC. IHC was considered significant for LTag in the case of any nuclear staining and for TP53 in cases with aberrant staining, including nuclear diffuse immunoreactivity, or complete loss of expression. Patchy immunostaining of p53 was considered wild-type pattern [27]. HER2 IHC was evaluated according to the recommendations of the American Society of Clinical Oncology and the College of American Pathologists (ASCO/CAP) [28]. HER2-CISH analysis with the SPEC HER2/CEN17 Probe Kit (Zytovision GmbH, Bremerhaven, Germany) was performed according to the manufacturer’s instructions and evaluated as recommended in the revised ASCO/CAP guidelines for HER2 amplification in breast cancer [28].
Nucleic acid isolation
Formalin-fixed paraffin-embedded (FFPE) tissue was available for cases 1–4 and fresh frozen tissue for case 5. Tumor and nontumor areas were marked separately on H&E stained slides prior to manual dissection. Nucleic acid isolation was performed according to a previously reported protocol [29] using the Maxwell® 16 LEV Blood DNA Kit (Promega, Mannheim, Germany).
SNaPshot analysis of TERT promotor and HRAS
Mutation hot spots of the TERT promoter (at positions −146, −124, and −57 bp) and of HRAS (at codons 12, 13, and 61) were investigated using SNaPshot analysis as previously described [30, 31] with an ABI Prism 3500 Genetic Analyzer and the SNaPshotTM Multiplex Kit (Applied Biosystems, Foster City, CA, USA).
Viral detection and quantification
Real-time PCR was performed to detect BKPyV-DNA [32] and human herpesvirus 6 (HHV-6) DNA [33]. To evaluate the number of cells investigated, a real-time PCR assay for the ALB gene was performed [34]. PCR reactions were performed in a final volume of 50 µl using 10 µl DNA, 25 µl of TaqMan® Universal PCR Master Mix (Thermo Fisher Scientific), 25 pmol of each primer, and 10 pmol of each fluorescence labeled probe (Table S1). After an initial denaturation phase of 10 min at 95 °C, 45 cycles of denaturation at 95 °C for 15 sec, and a combined annealing and extension phase at 60 °C for 1 min were performed using the ABI PRISM® 7500 (TaqMan). The lower detection limit was between five and ten DNA copies per reaction in all real-time PCR assays.
NGS and sequence analysis
DNA from four FFPE- and one fresh frozen-tumor was converted into Illumina NGS libraries and sequenced on HiSeq 4000 or X-Ten (Macrogen Inc, Seoul, Republic of Korea). Paired reads (between 313 and 880 million/sample) were aligned to the human genome, and BKPyV integration sites were identified from broken paired reads mapped to human (hg19) and BKPyV genomes. For this, patient specific BKPyV consensus genomes were generated by mapping reads to the BKPyV RefSeq genome (NC_001538) and filling of gaps from this reference. Reads not mapping to human and BKPyV genomes were also mapped against the NCBI RefSeq dataset of DNA virus genomes (Fig. S1) [35]. RNA-seq of a strand specific library made from rRNA depleted (Ribo-Zero) total tumor RNA from the fresh frozen-tumor sample (case 5) was performed to test cellular and viral gene expression. All bioinformatic analyses were performed with CLC Genomics Workbench 11 and 12 (Qiagen, Aarhus, DK). Mutants were identified from de-duplicated read mappings (to hg38, coverage 10, frequency >5%) and filtered for clinical relevant variants in the ClinVar 20171029 database, focusing on a set of 50 genes most frequently involved in bladder cancer and variants therein present with at least two reads and 10% frequency and annotations “pathogenic” or “likely pathogenic”.
The BKPyV genotype was assigned by multiple sequence alignment of the BKPyV VP1 gene sequence of the patient strains and 79 VP1 sequences from the database, followed by construction of a phylogenetic tree using the Neighbor Joining method and the Jukes Cantor nucleotide substitution model, and subtypes assigned by nucleotide BLAST of patient specific consensus genomes against the 162 BKPyV genomes used by Luo et al. [36].
Results
Case identification and clinical presentation
IHC staining of 94 MPUC revealed two LTag expressing UC (cases 1 and 2). Retrospective assessment of clinical data showed that both patients were kidney transplant recipients. Subsequent screening of the records of our departments of surgical pathology and nephropathology identified 15 UC which were diagnosed after solid organ transplantation (n = 12 kidney, n = 2 heart, and n = 1 liver recipient). Among them, another 3 LTag expressing UC were found (cases 3–5).
IHC staining of additional TMAs with overall 755 conventional and variant UC (24 plasmacytoid variant UC, 33 nested variant UC, 19 large nested variant UC, 480 consecutive UC of all stages and 199 muscle-invasive UC, both including variant UC) did not show any LTag expressing UC.
Patient and tumor characteristics and clinical follow up data of the five LTag expressing cases are shown in Table 1. For patients 1 and 3, no information was available to assess a possible BKPyV reactivation. In patient 2, graft biopsy showed no polyomavirus associated nephropathy 1 month after the second kidney transplantation. Patient 4 had no clinical symptoms of BKPyV reactivation and tested repeatedly negative for BK viremia during routine checkup. Patient 5 had suffered from hemorrhagic cystitis due to BKPyV reactivation after heart transplantation.
Morphology and IHC
Clinico-pathological and morphological characteristics of the analyzed posttransplant UC are shown in Table 2. Histological examination revealed one pure MPUC (case 1), and two UC with MPUC components >90% (case 2), and 10% (case 5), respectively, the latter with a concurrent exophytic non-invasive papillary urothelial carcinoma (pTa, high-grade) component with micropapillary areas at the surface and extensive urothelial carcinoma in situ (CIS) covering the whole bladder (Fig. 1). The remaining two UC (cases 3 and 4) showed a focal conventional UC component. The unusual glandular pattern in case 3 mainly corresponded to clear cell carcinoma of Mullerian type, and there was concomitant urothelial CIS. IHC revealed GATA3 expression and at least focal coexpression of PAX8 in both the CIS and the invasive tumor component. According to the current WHO classification [26] this tumor represents urothelial carcinoma with extensive divergent differentiation with Mullerian type clear cell carcinoma. In case 4 there was extensive villoglandular pattern with nuclear expression of GATA3, whereas PAX8 was completely negative (Fig. 2).

BKPyV-associated UC showed micropapillary growth pattern (a, d, m) with variable extent, UC with extensive divergent differentiation with Müllerian type clear cell carcinoma (g) and unusual villoglandular pattern (j). All tumors showed nuclear expression of LTag (b, e, h, k, n) and p53 overexpression (c, f, i, l, o).

Both cases showed nuclear staining for GATA3 (a, b). Case 3 showed additional focal PAX8 staining in a subset of invasive carcinoma and carcinoma in situ cells (c). Case 4 was negative for PAX8 (d).
All five tumors showed nuclear staining for LTag in the invasive and CIS component while benign urothelium and surrounding benign structures were negative for LTag (Fig. 3). As a productive lytic replication would also take place in surrounding normal tissue, we assume that LTag expression most likely originated from integrated virus and not from productive infection. Aberrant expression for p53 was found in the invasive and CIS component of all five tumors. Benign urothelium showed a wild-type pattern for p53 with faint basally accentuated patchy nuclear staining. HER2 amplification was found in two tumors: case 2 (immunoscore 1+) and case 5 (immunoscore 3+).

Pagetoid spread of CIS with nuclear expression of LTag adjacent to the invasive carcinoma. Note negativity in the normal urothelial, stromal and endothelial cells.
TERT promoter and HRAS mutation analysis by SNaPshot
Mutations of the TERT promoter were found in 3/5 LTag expressing UC (Table 2). Case 3 could not be evaluated at position −57 and we obtained a PCR-product of reduced size at −146, possibly corresponding to a deletion at this position. Mutations of the HRAS gene were not found in 4/4 evaluable cases. Case 3 was not evaluable as no PCR-products could be generated. This might be explained by a reduced DNA quality and degradation at the regions of interest.
Viral detection and NGS
All five LTag expressing UC contained BKPyV-DNA with a viral load of about two BKPyV-DNA copies per cell (0.3–4.3 copies/cell; Table 3). We also tested six posttransplant UC without LTag expression for BKPyV-DNA and none contained BKPyV-DNA.
NGS analysis of the five LTag expressing UC could be performed only from tumor tissue but not from adjacent normal tissue due to limited quality and quantity of the samples. BKPyV integration was detected in 4/5 tumors with one distinct integration site in each of tumors 1, 3, and 4 and at least two integration sites in tumor 5. The integration sites were in intergenic and intronic regions of the tumor genome and affected different human genes: LGR4, DEK, RNF144B, THADA, SMC5, KLF9, PRKAR2A and SLC6A18 (Fig. S2). Breakpoints in the BKPyV genomes were located in LTag, VP2, and VP3. All four tumors with integrated BKPyV-DNA contained intact BKPyV early coding regions as shown by NGS reads covering these regions (Fig. S2) and shown by expression of the early gene product LTag.
RNA-seq was performed from fresh frozen tissue for tumor 5 and showed strong transcription of the early coding regions for small Tag and LTag but scarcely of late structural BKPyV genes (Fig. S3). RNA-seq could not be performed for cases 1–4 due to the low quantity and quality of the FFPE material.
In cases 1 and 3, the integrated BKPyV genomes had small deletions within the in the P-block [22] of the noncoding control region (NCCR) (Fig. S4). The five BKPyV isolates represented three different genotypes (Fig. S5).
The only tumor without detectable BKPyV integration (case 2) was found to contain HHV-6 DNA with an average viral load of about one HHV-6 DNA copy per cell (Fig. S6).
Analysis of the 50 most common cancer related genes altered in UC [37] showed only few alterations per case and no mutations in the TP53 tumor suppressor gene nor in the HRAS gene. Most of the detected alterations have been described in the ClinVar database and ranked as benign/likely benign or of uncertain significance (e.g., TTN: p.Val10240Phe, p.Val9503Ile, p.Glu5963Gly). Few pathogenic or likely pathogenic mutations were detected in cases 2, 3, and 4 (Table 3).
Discussion
Herein, we characterize five LTag expressing UC which were diagnosed between 2 and 18 years after kidney (n = 4) or heart (n = 1) transplantation. The first two cases were detected among 94 MPUC, and only retrospective analysis showed a posttransplant state. This observation triggered a retrospective screening of our records which yielded 15 posttransplant UC, with LTag expression present in 3/15 (20%). Others reported a somewhat higher LTag prevalence in UC in kidney transplant (31%) [38] or solid organ recipients (44%) [16]. BKPyV-associated UC can arise in graft and non-graft sites due to reactivation of latent BKPyV of donor or recipient origin. Case 3 developed in the renal pelvis of the kidney graft, while the other four UC affected the urinary bladder.
All five LTag expressing tumors were high-grade tumors and had at least partial variant morphology. Three were MPUC or showed a focal MPUC component. MPUC account for 0.7–6% of UC and are associated with a poor prognosis [39]. Two tumors showed extensive and unusual glandular patterns, one of them representing UC with extensive divergent differentiation with Mullerian type clear cell carcinoma, the other with villoglandular morphology. Since variant and unusual morphologic patterns have been reported in BKPyV-associated UC [15, 16, 40], we additionally investigated rare variant UC other than MPUC for LTag expression. Among 76 plasmacytoid, nested and large nested variant UC we did not find any positive cases. Additional search in two TMAs containing tissue cores of altogether 679 urothelial carcinomas including rare variant UCs (MPUC, sarcomatoid, plasmacytoid, neuroendocrine, lymphoepithelioma-like, nested, large nested, and clear cell) no LTag expressing cases were found, which confirms the low incidence of LTag expressing UC.
In the five LTag positive UC, IHC staining for LTag was restricted to tumor tissue. As a productive lytic replication would also take place in surrounding normal tissue, LTag expression most likely originated from integrated virus and not from productive infection.
Mutations in the TERT promoter were present in 3/5 cases, they are the most frequent alterations in UC and frequently found in MPUC [41, 42]. As TERT promoter mutations are detectable irrespective of stage and grade they might reflect early events in UC development. TERT promotor mutations could result in increased telomerase expression stabilizing tumor cell genomes and might facilitate transformation of cells with BKPyV-DNA integration. We found two MPUC with HER2 amplification which has been reported in 5–10% of advanced UC and in up to 42% of MPUC [43,44,45,46,47]. Assessment of the HER2 status can detect a subset of tumors that may benefit from anti-HER2 targeted therapies which are currently tested in clinical trials.
BKPyV-DNA was detectable in all five LTag expressing UC but was not present in six posttransplant UC without LTag expression. NGS showed chromosomal integration of BKPyV-DNA in 4/5 UC affecting four human genes, two of which (THADA, LGR4) have been implicated in cancer development [48, 49]. This study significantly enlarges the limited number of UC with proven BKPyV integration. Others have reported intronic, exonic and intergenic integration of BKPyV in the tumor genome with variant breakpoints in the viral genome [15, 16, 18, 19, 21, 22, 50]. In a similar manner, unique and random chromosomal integration sites of polyomavirus MCPyV are present in Merkel cell carcinoma [51]. Polyomavirus associated tumorigenesis is associated with unregulated LTag expression and subsequent p53 binding and inactivation [52, 53], while in UC without viral integration p53 inactivation is usually caused by mutations of the TP53 gene. According to this proposed mechanism, all five UC in our study revealed aberrant p53 expression by IHC but no TP53 gene mutations by NGS. In addition, NGS detected only one to five alterations per tumor within the 50 most common cancer related genes altered in UC [37]. There were very few pathogenic or likely pathogenic mutations and most of the affected genes (PCLO, PANK2, RYR1, FLG, TTN, and ATM) were also reported as mutated in a pan cancer analysis based on TCGA data [54], which might reflect common biological processes in many cancers. As human embryonic kidney cells transfected with BKPyV-DNA were reported to grow only in the presence of a mutated and activated HRAS oncogene [55], we specifically searched for HRAS mutations in the LTag expressing UC, but detected none.
The paucity of pathogenic genomic mutations suggests that carcinogenesis occurs via unregulated LTag expression in BKPyV-associated UC. Sirohi et al. [16] reported a lower number of deleterious genomic mutations in LTag expressing UC compared with UC without LTag expression.
We detected a break point in the viral LTag in one case, but NGS data suggested that BKPyV integrated as a concatemer. Therefore, a full functional set of BKPyV genes was present in the tumor facilitating the expression of LTag. Insertional breakpoints within the BKPyV large or small T antigen genes have also been reported by others in UC which nevertheless expressed LTag, indicating that BKPyV integration was also in a concatemeric form [16, 21]. We could perform transcriptional analysis only for case 5 where RNA-seq showed strong transcription of the early region genes for small and LTag. There was nearly no transcription of the late structural genes suggesting very limited or absent lytic replication of BKPyV.
In two UC, the integrated BKPyV genomes had small deletions within the viral NCCR, which have been attributed a role in deregulation of LTag expression [10]. However, two other UC with BKPyV integration and one UC without detectable BKPyV integration did not have such mutations.
In case 2, we failed to detect BKPyV integration. FFPE material from this tumor was limited and 10 years old, consequently DNA was of relatively low quality. We obtained low genome coverage and the lowest BKPyV read numbers from this tumor, therefore we might have missed BKPyV integration. Interestingly, we detected about one copy HHV-6 DNA per tumor cell, suggesting inherited chromosomally integrated HHV-6 (ciHHV-6). We had no additional tissue available from this patient to test this hypothesis. HHV-6 can integrate near the subtelomeric/telomeric junction of chromosomes and can be genetically transmitted, which occurs in 0.6–2% of the general population [56]. HHV-6 integration is a proposed mechanism to establish viral latency but no association with human cancer has been observed. Our search in the TCGA supplemental data revealed no UC with HHV-6 integration among 412 muscle invasive UC [37].
In summary, we describe five posttransplant UC with distinct morphology and LTag expression. Unique and random BKPyV integration was detectable in four tumor genomes. The proposed mechanism of tumorigenesis is BKPyV lytic reactivation under immunosuppression leading to erroneous chromosomal BKPyV integration with unregulated LTag expression and subsequent p53 inactivation. IHC screening for LTag should be performed in posttransplant UC to identify patients with BKPyV-associated UC. Some of these patients might benefit from cessation of immunosuppression as reported in individual cases [21, 22] or from therapy with checkpoint inhibitors as recently shown for Merkel cell carcinoma [57, 58].
References
Engels EA, Pfeiffer RM, Fraumeni JF Jr., Kasiske BL, Israni AK, Snyder JJ, et al. Spectrum of cancer risk among US solid organ transplant recipients. J Am Med Assoc. 2011;306:1891–901.
Collett D, Mumford L, Banner NR, Neuberger J, Watson C. Comparison of the incidence of malignancy in recipients of different types of organ: a UK Registry audit. Am J Transplant. 2010;10:1889–96.
Gardner SD, Field AM, Coleman DV, Hulme B. New human papovavirus (B.K.) isolated from urine after renal transplantation. Lancet. 1971;1:1253–7.
Wang Y, Keinonen A, Koskenmies S, Pitkanen S, Fyhrquist N, Sadeghi M, et al. Occurrence of newly discovered human polyomaviruses in skin of liver transplant recipients and their relation with squamous cell carcinoma in situ and actinic keratosis—a single-center cohort study. Transpl Int. 2019;32:516–22.
Helle F, Brochot E, Handala L, Martin E, Castelain S, Francois C, et al. Biology of the BKPyV: an update. Viruses. 2017;9:1–18.
Papadimitriou JC, Randhawa P, Rinaldo CH, Drachenberg CB, Alexiev B, Hirsch HH. BK polyomavirus infection and renourinary tumorigenesis. Am J Transplant. 2016;16:398–406.
Tognon M, Corallini A, Martini F, Negrini M, Barbanti-Brodano G. Oncogenic transformation by BK virus and association with human tumors. Oncogene. 2003;22:5192–200.
Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science. 2008;319:1096–100.
Knowles WA, Pipkin P, Andrews N, Vyse A, Minor P, Brown DW, et al. Population-based study of antibody to the human polyomaviruses BKV and JCV and the simian polyomavirus SV40. J Med Virol. 2003;71:115–23.
Nickeleit V, Singh HK, Kenan DJ, Mieczkowski PA. The two-faced nature of BK polyomavirus: lytic infection or non-lytic large-T-positive carcinoma. J Pathol. 2018;246:7–11.
Dalianis T, Hirsch HH. Human polyomaviruses in disease and cancer. Virology. 2013;437:63–72.
Arthur RR, Shah KV, Baust SJ, Santos GW, Saral R. Association of BK viruria with hemorrhagic cystitis in recipients of bone marrow transplants. N Engl J Med. 1986;315:230–4.
Chen CH, Wen MC, Wang M, Lian JD, Cheng CH, Wu MJ, et al. High incidence of malignancy in polyomavirus-associated nephropathy in renal transplant recipients. Transplant Proc. 2010;42:817–8.
Wang HH, Liu KL, Chu SH, Tian YC, Lai PC, Chiang YJ. BK virus infection in association with posttransplant urothelial carcinoma. Transplant Proc. 2009;41:165–6.
Odetola OE, Isaila B, Pambuccian SE, Barkan GA. Unusual BK polyomavirus-associated urologic malignancies in renal transplant recipients: report of two cases and review of the literature. Diagn Cytopathol. 2018;46:1050–9.
Sirohi D, Vaske C, Sanborn Z, Smith SC, Don MD, Lindsey KG, et al. Polyoma virus-associated carcinomas of the urologic tract: a clinicopathologic and molecular study. Mod Pathol. 2018;31:1429–41.
Ross JS, Wang K, Gay LM, Al-Rohil RN, Nazeer T, Sheehan CE, et al. A high frequency of activating extracellular domain ERBB2 (HER2) mutation in micropapillary urothelial carcinoma. Clin Cancer Res. 2014;20:68–75.
Bialasiewicz S, Cho Y, Rockett R, Preston J, Wood S, Fleming S, et al. Association of micropapillary urothelial carcinoma of the bladder and BK viruria in kidney transplant recipients. Transpl Infect Dis. 2013;15:283–9.
Kenan DJ, Mieczkowski PA, Burger-Calderon R, Singh HK, Nickeleit V. The oncogenic potential of BK-polyomavirus is linked to viral integration into the human genome. J Pathol. 2015;237:379–89.
Kenan DJ, Mieczkowski PA, Latulippe E, Cote I, Singh HK, Nickeleit V. BK polyomavirus genomic integration and large T antigen expression: evolving paradigms in human oncogenesis. Am J Transplant. 2017;17:1674–80.
Fu F, Deng W, Yu S, Liu Y, Yu L, Liu R, et al. Occurrence and regression of BK polyomavirus associated carcinoma: a clinical and next-generation sequencing study. Clin Sci (Lond). 2018;132:1753–63.
Müller DC, Ramo M, Naegele K, Ribi S, Wetterauer C, Perrina V, et al. Donor-derived, metastatic urothelial cancer after kidney transplantation associated with a potentially oncogenic BK polyomavirus. J Pathol. 2018;244:265–70.
Bubendorf L, Nocito A, Moch H, Sauter G. Tissue microarray (TMA) technology: miniaturized pathology archives for high-throughput in situ studies. J Pathol. 2001;195:72–9.
Pfannstiel C, Strissel PL, Chiappinelli KB, Sikic D, Wach S, Wirtz RM, et al. The tumor immune microenvironment drives a prognostic relevance that correlates with bladder cancer subtypes. Cancer Immunol Res. 2019;7:923–38.
Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours 8th ed. New York: John Wiley & Sons; 2016. p. 272.
Moch H, Humphrey PA, Ulbright TM, Reuter V. WHO classification of tumours of the urinary system and male genital organs. Lyon: International Agency for Research on Cancer; 2016.
Wang CC, Tsai YC, Jeng YM. Biological significance of GATA3, cytokeratin 20, cytokeratin 5/6 and p53 expression in muscle-invasive bladder cancer. PLoS ONE. 2019;14:e0221785.
Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31:3997–4013.
Stoehr R, Zietz S, Burger M, Filbeck T, Denzinger S, Obermann EC, et al. Deletions of chromosomes 9 and 8p in histologically normal urothelium of patients with bladder cancer. Eur Urol. 2005;47:58–63.
Stoehr R, Taubert H, Zinnall U, Giedl J, Gaisa NT, Burger M, et al. Frequency of TERT promoter mutations in prostate cancer. Pathobiology. 2015;82:53–7.
Kompier LC, Lurkin I, van der Aa MN, van Rhijn BW, van der Kwast TH, Zwarthoff EC. FGFR3, HRAS, KRAS, NRAS and PIK3CA mutations in bladder cancer and their potential as biomarkers for surveillance and therapy. PLoS ONE. 2010;5:e13821.
Knöll A, Stoehr R, Jilg W, Hartmann A. Low frequency of human polyomavirus BKV and JCV DNA in urothelial carcinomas of the renal pelvis and renal cell carcinomas. Oncol Rep. 2003;10:487–91.
Aberle SW, Puchhammer-Stockl E. Diagnosis of herpesvirus infections of the central nervous system. J Clin Virol. 2002;25 (Suppl 1):S79–85.
Korn K, Reil H, Ensser A, Knöll A. No evidence of XMRV infection in immunocompromised patients and HIV-positive individuals from Germany. Infection. 2012;40:181–4.
Brister JR, Ako-Adjei D, Bao Y, Blinkova O. NCBI viral genomes resource. Nucleic Acids Res. 2015;43:D571–7.
Luo C, Bueno M, Kant J, Martinson J, Randhawa P. Genotyping schemes for polyomavirus BK, using gene-specific phylogenetic trees and single nucleotide polymorphism analysis. J Virol. 2009;83:2285–97.
Robertson AG, Kim J, Al-Ahmadie H, Bellmunt J, Guo G, Cherniack AD, et al. Comprehensive molecular characterization of muscle-invasive bladder. Cancer Cell. 2017;171:540–56. e25.
Yan L, Salama ME, Lanciault C, Matsumura L, Troxell ML. Polyomavirus large T antigen is prevalent in urothelial carcinoma post-kidney transplant. Hum Pathol. 2016;48:122–31.
Amin MB, Ro JY, el-Sharkawy T, Lee KM, Troncoso P, Silva EG, et al. Micropapillary variant of transitional cell carcinoma of the urinary bladder. Histologic pattern resembling ovarian papillary serous carcinoma. Am J Surg Pathol. 1994;18:1224–32.
Lin CY, Saleem A, Stehr H, Zehnder JL, Pinsky BA, Kunder CA. Molecular profiling of clear cell adenocarcinoma of the urinary tract. Virchows Arch. 2019;475:727–34.
Allory Y, Beukers W, Sagrera A, Flandez M, Marques M, Marquez M, et al. Telomerase reverse transcriptase promoter mutations in bladder cancer: high frequency across stages, detection in urine, and lack of association with outcome. Eur Urol. 2014;65:360–6.
Nanovic L, Becker YT, Hedican S, Hofmann RM. Sudden late onset of gross hematuria in a previous renal transplant recipient 3 months after transplant nephrectomy. Am J Kidney Dis. 2005;46:e91–4.
Moktefi A, Pouessel D, Liu J, Sirab N, Maille P, Soyeux P, et al. Reappraisal of HER2 status in the spectrum of advanced urothelial carcinoma: a need of guidelines for treatment eligibility. Mod Pathol. 2018;31:1270–81.
Zinnall U, Weyerer V, Comperat E, Camparo P, Gaisa NT, Knuechel-Clarke R, et al. Micropapillary urothelial carcinoma: evaluation of HER2 status and immunohistochemical characterization of the molecular subtype. Hum Pathol. 2018;80:55–64.
Schneider SA, Sukov WR, Frank I, Boorjian SA, Costello BA, Tarrell RF, et al. Outcome of patients with micropapillary urothelial carcinoma following radical cystectomy: ERBB2 (HER2) amplification identifies patients with poor outcome. Mod Pathol. 2014;27:758–64.
Isharwal S, Huang H, Nanjangud G, Audenet F, Chen YB, Gopalan A, et al. Intratumoral heterogeneity of ERBB2 amplification and HER2 expression in micropapillary urothelial carcinoma. Hum Pathol. 2018;77:63–9.
Ching CB, Amin MB, Tubbs RR, Elson P, Platt E, Dreicer R, et al. HER2 gene amplification occurs frequently in the micropapillary variant of urothelial carcinoma: analysis by dual-color in situ hybridization. Mod Pathol. 2011;24:1111–9.
Panebianco F, Kelly LM, Liu P, Zhong S, Dacic S, Wang X, et al. THADA fusion is a mechanism of IGF2BP3 activation and IGF1R signaling in thyroid cancer. Proc Natl Acad Sci USA. 2017;114:2307–12.
Yue Z, Yuan Z, Zeng L, Wang Y, Lai L, Li J, et al. LGR4 modulates breast cancer initiation, metastasis, and cancer stem cells. FASEB J. 2018;32:2422–37.
Kenan DJ, Mieczkowski PA, Latulippe E, Cote I, Singh HK, Nickeleit VBK. Polyomavirus genomic integration and large T antigen expression: evolving paradigms in human oncogenesis. Am J Transplant. 2017;17:1674–80.
Martel-Jantin C, Filippone C, Cassar O, Peter M, Tomasic G, Vielh P, et al. Genetic variability and integration of Merkel cell polyomavirus in Merkel cell carcinoma. Virology. 2012;426:134–42.
Cheng J, DeCaprio JA, Fluck MM, Schaffhausen BS. Cellular transformation by Simian Virus 40 and Murine Polyoma Virus T antigens. Semin Cancer Biol. 2009;19:218–28.
Weinreb DB, Desman GT, Burstein DE, Kim DU, Dikman SH, Johnson EM. Expression of p53 in virally infected tubular cells in renal transplant patients with polyomavirus nephropathy. Hum Pathol. 2006;37:684–8.
Kim H, Kim YM. Pan-cancer analysis of somatic mutations and transcriptomes reveals common functional gene clusters shared by multiple cancer types. Sci Rep. 2018;8:6041.
Pater A, Pater MM. Transformation of primary human embryonic kidney cells to anchorage independence by a combination of BK virus DNA and the Harvey-ras oncogene. J Virol. 1986;58:680–3.
Flamand L. Chromosomal integration by human herpesviruses 6A and 6B. Adv Exp Med Biol. 2018;1045:209–26.
Kaufman HL, Russell J, Hamid O, Bhatia S, Terheyden P, D’Angelo SP, et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016;17:1374–85.
D’Angelo SP, Russell J, Lebbe C, Chmielowski B, Gambichler T, Grob JJ, et al. Efficacy and safety of first-line avelumab treatment in patients with stage IV metastatic Merkel Cell carcinoma: a preplanned interim analysis of a clinical trial. JAMA Oncol. 2018;4:e180077.
Acknowledgements
The authors wish to acknowledge M. Sommerer, S. Blank and V. Popp for excellent technical assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Bertz, S., Ensser, A., Stoehr, R. et al. Variant morphology and random chromosomal integration of BK polyomavirus in posttransplant urothelial carcinomas. Mod Pathol 33, 1433–1442 (2020). https://doi.org/10.1038/s41379-020-0489-0
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41379-020-0489-0
This article is cited by
-
Prevalence of 13 polyomaviruses in actinic keratosis and matched healthy skin samples of immunocompetent individuals
Infectious Agents and Cancer (2022)
-
New developments in existing WHO entities and evolving molecular concepts: The Genitourinary Pathology Society (GUPS) update on renal neoplasia
Modern Pathology (2021)
-
BK polyomavirus infection promotes growth and aggressiveness in bladder cancer
Virology Journal (2020)
