
Abstract
The 11 March 2011 earthquake and tsunami in Japan resulted in ~19,000 lost lives and the displacement of nearly a quarter million people owing to extensive property damage and evacuation from the nuclear meltdown in Fukushima. We sought to prospectively examine whether exposure to disaster-related trauma affected blood pressure levels among young children. We sampled children in three affected prefectures (Miyagi, Fukushima, Iwate) and one unaffected prefecture (Mie). The participants (mean age 6.6 years) and their caregivers answered a baseline survey (N = 320) and a follow-up survey 4 years after the earthquake (N = 227, follow-up rate 71%). Disaster-related trauma was assessed at the baseline, and blood pressure measurements were taken at the follow-up. We converted blood pressure data into age/sex/height-specific z-scores. In linear regression models, we controlled for body mass index, income, age, sex, and housing situation (living in the same house as before the disaster, in a shelter, or in a new house). The number of traumatic experiences was related to diastolic blood pressure in a dose-dependent manner but was not related to systolic blood pressure. Children reporting four or more traumatic experiences had marginally significant elevated diastolic blood pressure (β = 0.43, p = 0.059). Among specific types of disaster trauma, witnessing a fire was significantly related to higher diastolic blood pressure (β = 0.60, p = 0.009). In conclusion, disaster-related trauma was associated with higher diastolic blood pressure among young children 4 years after the traumatic events.
Similar content being viewed by others

Introduction
On 11 March 2011, an immense earthquake and ensuing massive tsunami brought devastating impacts to east Japan. The earthquake was the one of the largest recorded in history, with a Richter-scale magnitude of 9.0. The disaster caused the loss of an estimated 19,630 lives, with an additional 2569 people listed as missing and 6230 injured [1]. More than 6 years after the disaster, nearly 84,000 people still remain displaced [2].
Among survivors, children have been identified as a vulnerable group, particularly with regard to the life-long consequences of exposure to disaster-related trauma. Previous studies of young survivors of the Great East Japan Earthquake disaster found that experiences of disaster-related trauma were related to more behavioral problems (2 years after the disaster), including suicidal ideation up to 3 years after the disaster [3, 4]. On the other hand, young children might be more resilient than other age groups given their plasticity and ability to become resilient [5]. However, one question that has been less well documented is whether trauma experiences have lingering effects on aspects of children’s physical health, such as their blood pressure.
Previous literature has studied the impacts of disasters on blood pressure among adult survivors, including in the aftermath of the Great East Japan Earthquake. For example, affected civil servants showed significantly greater blood pressure increases than nonpublic employees in the disaster-affected area ~8 months after the event [6]. Two years after the disaster, people evacuated from Fukushima showed significantly higher blood pressure [7]. Only one previous report attempted to investigate the effects of disaster-related trauma on children; this study examined cardiometabolic profiles, including peripheral arterial stiffness, in adolescents and young children who were living close to the World Trade Center during the 9.11 terrorist attacks ~14 years after the event [8]. This study did not show any adverse effects of traumatic experiences on cardiometabolic measures.
Higher blood pressure in childhood (even within the “normal” range) is known to track into adulthood and increase the risk of hypertension [9]. In addition, elevated blood pressure among children and adolescents has been reported to be associated with target organ damage, including left ventricular hypertrophy, increased carotid intimal-medial thickness, and renal damage [10,11,12,13].
In the current study, we sampled children from three areas directly affected by the 2011 Great East Japan Earthquake: Miyagi and Iwate prefectures (which were devastated by the earthquake and tsunami), and Fukushima prefecture (which was directly affected by the earthquake, tsunami and nuclear disaster). We also sampled children from Mie prefecture (which was not affected). Our aim was to examine the long-term impact of disaster-related trauma on blood pressure among young children.
Methods
Data from the Great East Japan Earthquake Follow-up for Children (GEJE-FC) were used. We have previously described our study sample [4]. As summarized in Fig. 1, after the disaster, we focused on three affected Japanese prefectures—Iwate, Miyagi, and Fukushima—which were severely impacted by the earthquake and tsunami (Iwate, Miyagi) or by radiation from the Fukushima nuclear power plant explosion. Focusing on municipalities with severe damage, three municipalities from Iwate, one from Miyagi, and four from Fukushima were selected. We reached out to all of the local preschools, inviting them to join our study. Four out of 32 preschools in Iwate, two out of 16 in Miyagi, and four out of 120 Fukushima agreed to participate. Refusals were mainly owing to the turnover of residents as people had to leave their city. Finally, we approached the parents of 787 children from September 2012 to June 2013. We obtained informed verbal assent from the children and written consent from the parents (n = 220, initial response rate; 28.0%).

Participant flow for the analytic sample
Approximately one and half years after the earthquake (from September 2012 to June 2013), we conducted the baseline study in 182 children, and 55 siblings were also added by informed consent (for a total of 237 children). The participants were invited again to join the follow-up study (n = 156, follow-up rate in the disaster-affected area: 66%), which was implemented ~ 4 years after the disaster, from July 2014 to January 2015.
For our control sample, we also recruited children from Mie Prefecture, which is located in the central region of Japan and was not directly affected by the disaster despite being located in a coastal area. Informed consent was obtained from the parents of 85 children (initial response rate: 12%), 80 of whom participated in the baseline study. After adding three siblings of these participants, the baseline measures were completed in a total of 83 children, and 71 children participated in the follow-up (follow-up rate: 86%).
A total of 320 children (237 in the disaster-affected areas and 83 in the control area) enrolled in the baseline study, and 227 (156 in the disaster-affected areas and 71 in the control area) completed the follow-up study (overall follow-up ratio: 71%). This research and the informed consent procedure were approved by the Research Ethics Committee at the National Center for Child Health and Development and Tokyo Medical and Dental University.
Measurements
At baseline, a child psychiatrist or clinical psychologist interviewed each child about his or her subjective traumatic experiences. Privacy was maintained by interviewing each child in a separate room within a local community center. The list of potential traumatic experiences included losing a family member or close relative in the disaster, losing a close friend or distant relative, witnessing the tsunami waves, witnessing someone being swept away by the tsunami, witnessing a fire, being subject to lifestyle restrictions owing to radiation (e.g., being unable to play outside or drink tap water) and witnessing at least one dead body. Caregivers also completed questionnaires and reported the children’s trauma experiences, such as being separated from their family and losing or experiencing damage to their homes.
At the follow-up study, the participants underwent a series of physiological measurements, including height, weight and blood pressure. After a rest period, both systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured three times by trained testers using automatic oscillometric sphygmomanometers (Omron HEM-7080IT, Omron Healthcare Co. Ltd, Kyoto, Japan), and the average of the 2nd and 3rd SBP and DBP measurements were used as the outcome. Regarding height and weight, participants were asked to take shoes off but leave other clothes on. The error ranges were ± 0.1 mm for height and ± 0.1 kg for weight.
Because height, weight, and sex have a strong influence on children’s blood pressure, SBP and DBP were both converted into z-scores based on these factors following a validated procedure and US reference values established by the U.S. Centers for Disease Control [14]. All other information, e.g., family size and household income in the follow-up year, was obtained from the caregivers via interviews and questionnaires.
Statistical analysis
The association between the number of traumatic events and blood pressure z-score was investigated using ordinary least squares regression analysis. We also examined the association between each specific type of traumatic experience and blood pressure z-scores. In multivariable adjusted models, we controlled for potential mediators, including body mass index, family size, adjusted household income, age, sex, and housing status at the time of the follow-up study. We also included indicator variables (fixed effects) for each prefecture.
Results
Table 1 shows the characteristics of the follow-up sample. The mean age of the baseline sample was 6.5 years (standard deviation: 1.4), and that of the follow-up sample was 8.5 years (mean age 6.7 as of the baseline survey) (standard deviation: 1.2). Among the sample, 7.0% experienced 4 or more traumatic experiences, 42.7% had experienced 1–3, and 50.2% had no exposure to any disaster-related trauma. In addition, 63.9% of the children lived in their previous house, 8.8% were still living in a shelter, and 25.1% were living in a new house.
The relationship between the number of traumatic experiences and blood pressure was examined using regression analysis, as shown in Table 2. In model 1, when crude regression analysis was employed, both SBP and DBP z-scores were significantly elevated only among the group with 1–3 traumatic experiences (SBP z-score: β = 0.32 p = 0.008, DBP z-score: β = 0.21 p = 0.049). In the group with four or more traumatic experiences, both SBP and DBP tended to be elevated (SBP z-score: β = 0.31 p = 0.19, DBP z-score: β = 0.37 p = 0.067), although the associations were not statistically significant. In model 2, which adjusted for sex, age, BMI, housing status, household adjusted income and prefecture fixed effects, no association was found between SBP z-scores and the number of traumatic experiences. However, a marginally significant relationship remained between the number of traumatic experiences and the DBP z-score. Compared with children without traumatic experiences, the group with 1–3 experiences had a 0.08-point higher DBP z-score (p = 0.56), and the group with four or more experiences had a 0.43-point elevated DBP z-score (p = 0.059), suggesting a dose–response association.
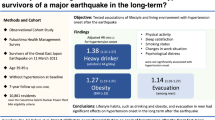
We reran the regression models to examine the association between each specific type of traumatic experience and blood pressure, and the results are presented in Table 3. In model 1, none of the individual traumatic experiences was related to SBP or DBP z-scores. In model 2, only “witnessing a fire” was related to elevated DBP z-scores (β = 0.60 p = 0.009), whereas other experiences were not related to SBP or DBP z-scores.
Discussion
To our knowledge, this is the first study to focus on the association between disaster-related trauma and blood pressure among young children in the aftermath of the Great East Japan Earthquake. We found that more exposure to traumatic experiences was marginally related in a dose–response manner to increased levels of DBP in a pediatric sample up to 4 years after the earthquake. Interestingly, there was no correlation between disaster-related trauma and SBP after controlling for potential confounding factors. Among the specific types of trauma experiences, only witnessing a fire was correlated with elevated DBP.
Previous studies also found short-term blood pressure changes following disaster exposure, but almost all focused on adult samples. A study among hypertensive outpatients affected by the Hanshin-Awaji Earthquake in 1995 (mean age 68 years) found significant increases in blood pressure up to 4 weeks after the disaster but a return to the baseline within 6 months [15]. Similarly, diabetic patients (mean age 68) had significantly higher SBP up to 3 months after the Niigata Earthquake in 2004; however, it returned to the baseline by 6 months [16]. A 4-year follow-up study of survivors (mean age 41 years) of an Italian earthquake in 1982 showed no difference in blood pressure from the baseline [17]. Although hypertensive patients who survived Hurricane Katrina in 2005 (mean age 62 years) presented significantly elevated SBP 6–16 months after the disaster, longer term follow-up has not been reported [18].
As a previous review reported that mental stress was a factor that elevated blood pressure [19], stress and allostatic load are the hypothesized mechanisms underlying an association between trauma experiences and blood pressure [20]. It has been reported that higher levels of plasma endothelin-1, a potent vasoconstrictor that elevates blood pressure [21], are found in healthy adolescents and young adults with a history of adverse childhood experiences [22]. In addition, adults with a history of childhood adversity were shown to have significantly higher basal inflammatory cytokine secretion levels [23, 24], which also leads to arterial stiffness and elevated blood pressure [25]. Additional mechanisms may involve changes in lifestyle behaviors, such as changes in physical activity owing to mental stress. For example, children in the Fukushima restriction zone were discouraged from exercising outdoors owing to the fear of radiation contamination.
Trauma experiences were related to DBP but not SBP in our study. A previous study also showed that a history of child abuse was more robustly associated with increases in DBP than SBP among adolescents aged 13–17 years old [26]. In fact, the Framingham heart study revealed that isolated diastolic hypertension is more prevalent in younger people than in older population [27]. These studies suggest that in childhood, stressors such as exposure to traumatic experiences might increase peripheral vascular resistance, which induces elevated DBP. It also increases SBP, but only slightly, as a result of the elasticity of the arterial wall among children. Therefore, we observed an association between disaster-related trauma and isolated DBP elevation, but not SBP elevation. Further studies to elucidate the association between trauma experience in childhood and the elasticity of arterial wall function are warranted.
Some limitations of our study should be noted. First, our sample size was relatively small, partly owing to the low response rate to the baseline survey; consequently, our analysis was underpowered to study some associations, e.g., specific types of disaster experiences and blood pressure. It is possible that there was selection into the study—e.g., by parents who were concerned about their child’s blood pressure (e.g., because of a family history of hypertension). However, this type of selection presumably also applied to the control sample (from Mie); therefore, the direction of bias was not necessarily away from the null. Second, we did not ask our sample to refrain from food intake before the blood pressure measurement, and we implemented the study throughout the day, which could have altered the blood pressure outcomes. Presumably, these alterations were random and introduced bias toward the null. Third, we attempted to control for confounding factors—i.e., prior common causes of disaster experiences and blood pressure, such as household socioeconomic status. However, it is possible that there was residual confounding by other unobserved factors. Fourth, we did not assess blood pressure before the earthquake; hence, we cannot infer whether the disaster experiences directly caused the elevation in blood pressure.
Disaster-related trauma appeared to be associated with higher diastolic blood pressure among young children up to 4 years after the disaster. Long-term follow-up of disaster survivors, including physiologic features such as renal function, is needed given that pediatric blood pressure elevation tracks into adulthood and increases the risk of cardiovascular diseases in adulthood.
References
Reconstruction Agency. Great East Japan Earthquake. 2011.
Reconstruction Agency. The number of displaced people. 2017.
Fujiwara T, Yagi J, Homma H, Mashiko H, Nagao K, Okuyama M. Suicide risk among young children after the Great East Japan Earthquake: a follow-up study. Psychiatry Res. 2017;253:318–24.
Fujiwara T, Yagi J, Homma H, Mashiko H, Nagao K, Okuyama M. Great East Japan Earthquake Follow-up for Children Study Team. Clinically significant behavior problems among young children 2 years after the Great East Japan Earthquake. PLoS ONE. 2014;9:e109342.
Cicchetti D. Resilience under conditions of extreme stress: a multilevel perspective. World Psychiatry. 2010;9:145–54.
Konno S, Munakata M. Blood pressure elevation lasting longer than 1 year among public employees after the Great East Japan Earthquake: the Watari study. Am J Hypertens. 2017;30:120–3.
Ohira T, Nakano H, Nagai M, Yumiya Y, Zhang W, Uemura M, Sakai A, Hashimoto S. Changes in cardiovascular risk factors after the Great East Japan Earthquake. Asia Pac J Public Health. 2017;29:47s–55s.
Trasande L, Koshy TT, Gilbert J, Burdine LK, Marmor M, Han X, Shao Y, Chemtob C, Attina TM, Urbina EM. Cardiometabolic profiles of adolescents and young adults exposed to the World Trade Center Disaster. Environ Res. 2018;160:107–14.
Bao W, Threefoot SA, Srinivasan SR, Berenson GS. Essential hypertension predicted by tracking of elevated blood pressure from childhood to adulthood: the Bogalusa Heart Study. Am J Hypertens. 1995;8:657–65.
Zahka KG, Neill CA, Kidd L, Cutilletta MA, Cutilletta AF. Cardiac involvement in adolescent hypertension. Echocardiographic determination of myocardial hypertrophy. Hypertension. 1981;3:664–8.
Lande MB, Carson NL, Roy J, Meagher CC. Effects of childhood primary hypertension on carotid intima media thickness: a matched controlled study. Hypertension. 2006;48:40–44.
Seeman T, Pohl M, Palyzova D, John U. Microalbuminuria in children with primary and white-coat hypertension. Pediatr Nephrol (Berl, Ger). 2012;27:461–7.
Flynn JT. High blood pressure in the young: why should we care? Acta Paediatr. 2018;107:14–19.
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114:555–76.
Saito K, Kim JI, Maekawa K, Ikeda Y, Yokoyama M. The great Hanshin-Awaji earthquake aggravates blood pressure control in treated hypertensive patients. Am J Hypertens. 1997;10:217–21.
Gerin W, Chaplin W, Schwartz JE, Holland J, Alter R, Wheeler R, Duong D, Pickering TG. Sustained blood pressure increase after an acute stressor: the effects of the 11 September 2001 attack on the New York City World Trade Center. J Hypertens. 2005;23:279–84.
Bland SH, Farinaro E, Krogh V, Jossa F, Scottoni A, Trevisan M. Long term relations between earthquake experiences and coronary heart disease risk factors. Am J Epidemiol. 2000;151:1086–90.
Fonseca VA, Smith H, Kuhadiya N, Leger SM, Yau CL, Reynolds K, Shi L, McDuffie RH, Thethi T, John-Kalarickal J. Impact of a natural disaster on diabetes: exacerbation of disparities and long-term consequences. Diabetes care. 2009;32:1632–8.
Munakata M. Clinical significance of stress-related increase in blood pressure: current evidence in office and out-of-office settings. Hypertens Res. 2018;41:553–69.
McEwen BS. Protective and damaging effects of stress mediators. N Engl J Med. 1998;338:171–9.
Khimji AK, Rockey DC. Endothelin--biology and disease. Cell Signal. 2010;22:1615–25.
Su S, Wang X, Kapuku GK, Treiber FA, Pollock DM, Harshfield GA, McCall WV, Pollock JS. Adverse childhood experiences are associated with detrimental hemodynamics and elevated circulating endothelin-1 in adolescents and young adults. Hypertension. 2014;64:201–7.
Hartwell KJ, Moran-Santa Maria MM, Twal WO, Shaftman S, DeSantis SM, McRae-Clark AL, Brady KT. Association of elevated cytokines with childhood adversity in a sample of healthy adults. J Psychiatr Res. 2013;47:604–10.
Danese A, Pariante CM, Caspi A, Taylor A, Poulton R. Childhood maltreatment predicts adult inflammation in a life-course study. Proc Natl Acad Sci USA. 2007;104:1319–24.
Virdis A, Ghiadoni L, Plantinga Y, Taddei S, Salvetti A. C-reactive protein and hypertension: is there a causal relationship? Curr Pharm Des. 2007;13:1693–8.
Gooding HC, Milliren CE, Austin SB, Sheridan MA, McLaughlin KA. Child abuse, resting blood pressure, and blood pressure reactivity to psychosocial stress. J Pediatr Psychol. 2016;41:5–14.
Sagie A, Larson MG, Levy D. The natural history of borderline isolated systolic hypertension. N Engl J Med. 1993;329:1912–7.
Acknowledgements
We thank all the participants in this study. In addition, we appreciate the GEJE-FC team, including psychiatrists and psychologists, for providing necessary mental health support during interviews upon requests. Finally, we thank our research coordinators, especially Ms. Maiko Osawa and Ms. Hisayo Saeki, for organizing the logistics of this study.
Funding
This study was supported by a grant from the Ministry of Health, Labour and Welfare (H24-jisedai-shitei-007).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Watanabe, M., Hikichi, H., Fujiwara, T. et al. Disaster-related trauma and blood pressure among young children: a follow-up study after Great East Japan earthquake. Hypertens Res 42, 1215–1222 (2019). https://doi.org/10.1038/s41440-019-0250-6
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-019-0250-6
Keywords
This article is cited by
-
Five-year blood pressure trajectories of survivors of the tsunami following the Great East Japan Earthquake in Iwate
Hypertension Research (2021)
-
Time course of disaster-related cardiovascular disease and blood pressure elevation
Hypertension Research (2021)
