
Abstract
Neoadjuvant immunotherapy can induce pathologic complete response (pCR) in patients with localized deficient mismatch repair (dMMR)/microsatellite instability-high (MSI-H) tumors. The long-term outcomes of these patients are unknown, as is the clinical utility of measuring circulating tumor DNA (ctDNA). Follow-up was evaluated in patients enrolled in a phase II trial (NCT04082572) that evaluated the efficacy and safety of pembrolizumab in patients with localized dMMR/MSI-H tumors. The primary outcomes of this trial have previously been reported. 3-year EFS and OS rates were 80% (95% CI: 66% – 93%) and 94% (95% CI: 86% – 100%). Patients without detectable ctDNA after pembrolizumab had higher 3-year EFS and OS rates than patients with detectable ctDNA after pembrolizumab (3-year EFS 92% vs 20%; p < 0.001, 3-year OS 100% vs 80%; p < 0.001). Patients with colorectal cancer (CRC) who had undetectable ctDNA after pembrolizumab were more likely to have pCR compared to those with detectable ctDNA after pembrolizumab (91% vs 0%; p = 0.03). Patients with CRC who were managed non-operatively and had undetectable ctDNA after pembrolizumab had a higher 2-year EFS rate than patients with detectable ctDNA after pembrolizumab (100% vs 33%; p = 0.03). Pembrolizumab demonstrates long-term efficacy in patients with localized dMMR/MSI-H tumors.
Similar content being viewed by others


Introduction
Neoadjuvant immunotherapy induces high rates of clinical and pathological responses in patients with localized deficient mismatch repair (dMMR)/microsatellite instability-high (MSI-H) solid tumors and could be a non-surgical, curative strategy1,2,3. However, accurate radiographic response assessment to immunotherapy can be limited by underestimation of the depth of response due to tumoral immune cell infiltration (“pseudoprogression”) and difficulty measuring luminal tumors4,5. Endoscopy is invasive and may fail to provide a representative tumor response due to spatial heterogeneity, and radiographic and endoscopic assessments of response in this setting can be discordant6,7. Circulating tumor DNA (ctDNA) has shown promise in guiding treatment approaches to adjuvant therapy for resectable colorectal cancer (CRC) and some metastatic solid tumors8,9,10. However, its potential application to guide treatment decisions for patients with localized disease in the neoadjuvant setting has not been thoroughly explored, particularly among patients with dMMR/MSI-H solid tumors.
We evaluated the 3-year event-free survival (EFS) rate and 3-year overall survival (OS) among patients enrolled in a phase II clinical trial (NCT04082572) that evaluated the efficacy and safety of pembrolizumab in patients with locally advanced dMMR/MSI-H solid tumors3. Further, we investigated ctDNA kinetics over the course of treatment with pembrolizumab to determine whether ctDNA has utility as a biomarker for pathologic complete response (pCR), EFS, and OS.
Results
Clinical features of patients with all locally advanced dMMR/MSI-H solid tumors
As of March 31, 2024, the median follow-up was 2.9 years (range: 0–3.8 years). Table 1 displays the clinical features of all 35 patients. Twenty-seven patients had CRC, one patient had a meningioma, one patient had duodenal adenocarcinoma, one patient had endometrial adenocarcinoma, two patients had pancreatic adenocarcinoma, one patient had gastric adenocarcinoma, and one patient had ampullary adenocarcinoma. The etiology of dMMR status was sporadic in 19 (54%) patients and Lynch Syndrome in 16 (46%) patients. The estimated median TMB for 31 evaluable patients was 49.6 mut/Mb (range: 4.2–134.4 mut/Mb). The median number of cycles of pembrolizumab was 8 among the 17 patients who underwent surgery. The median number of cycles of pembrolizumab was 16 among the 18 patients who did not undergo surgery.
Outcomes of patients with all locally advanced dMMR/MSI-H solid tumors
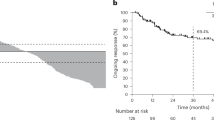
The 3-year EFS and OS rates for all 35 patients were 80% (95% CI: 66–93%) and 94% (95% CI: 86–100%), respectively (Fig. 1A, B). The 3-year EFS rate was 83% (95% CI: 65% – NA) in 17 patients who underwent surgery compared to 76% (95% CI: 56% –97%) in 18 patients who did not undergo surgery (p = 0.667) (Supplementary Fig. 1A). The 3-year OS rate was 100% in 17 patients who underwent surgery compared to 89% (95% CI: 74% – NA) in 18 patients who did not undergo surgery (p = 0.067) (Supplementary Fig. 1B). ORR in the updated analysis was 82%, with three of 14 patients who were categorized as partial responses in the original trial report developing complete responses. Thirteen (39%) patients had complete responses, and 14 (42%) patients had partial responses. Eleven of 17 patients who underwent surgical resection had a pCR (65% pCR rate in all patients). Fourteen of these 17 patients had CRC, 11 of whom had a pCR (79% pCR rate in patients with CRC). None of the patients who had a pCR recurred clinically after a median follow-up of 35 months. Of the three patients who did not experience a pCR, one had local disease recurrence seven months after resection. The other two patients had not experienced disease recurrence at their last follow-up (41 and 28 months after surgery, respectively).

A – 3-year event-free survival (EFS) rate among all patients. Kaplan–Meier for EFS for the full study cohort (n = 35). The 3‑year EFS rate was 80 % (95 % CI, 66–93). Tick marks denote censored observations, and the shaded band represents the 95% CI. B 3-year overall survival (OS) rate among all patients. Kaplan–Meier curve for OS for the full study cohort (n = 35). The 3-year OS rate was 94% (95% CI, 86–100). Tick marks denote censored observations, and the shaded band represents the 95% CI.
No additional patients with available follow-up data experienced progressive events beyond the six patients identified in the original trial report. All six of these patients were deemed to have initially resectable disease prior to neoadjuvant pembrolizumab. Two had pancreatic adenocarcinoma, and four had CRC. The two patients with pancreatic adenocarcinoma underwent surgical resection, one after chemotherapy, with neither achieving pCR. Both are currently without disease recurrence at 34 and 39 months after surgery. Two of the four patients with CRC did not undergo surgery after experiencing disease progression. Surgery was recommended to one of these two patients, but the patient elected to forego further cancer-directed treatment and died 41 months after their first dose of pembrolizumab, while the second patient was treated with encorafenib, binimetinib, and cetuximab and, due to progression and extensive comorbidities, was not able to undergo surgical resection. This patient died eight months after their first dose of pembrolizumab. The other two patients with CRC proceeded to surgery upon disease progression, and neither had a pCR. One of these patients experienced disease recurrence seven months after surgery and received four cycles of ipilimumab plus nivolumab, followed by maintenance nivolumab, and is alive without disease 35 months after surgery, while the other patient did not receive adjuvant therapy and is disease-free 28 months after surgery.
Two patients who did not undergo surgery were lost to follow-up - one international patient returned to their home country and was lost to follow-up 40 days after their first dose of pembrolizumab. The other patient had a change in their health insurance plan and was lost to follow-up 15 months after their first dose of pembrolizumab. No other treatment-related adverse events occurred beyond the 13 patients who experienced Grade 1 or 2 events and two who experienced Grade 3 events identified in the original trial report.
ctDNA characteristics and outcomes
Sixteen (48.6%) of 35 patients had detectable ctDNA at baseline. Fourteen of the 16 patients with detectable ctDNA at baseline had CRC, one had gastric adenocarcinoma, and one had endometrial adenocarcinoma. Thirty-two of 35 patients were evaluable for analysis pertaining to outcomes by ctDNA status, as three patients were excluded because they either did not have sufficient blood collected after their last dose of pembrolizumab for ctDNA analysis or had inadequate tissue for NGS. Fourteen (44%) of the 32 evaluable patients had detectable baseline ctDNA, with a mean and median VAF of 5.0% and 0.8% (range 0.3–29.5%). Nine of these 14 patients cleared ctDNA with a mean and median number of cycles to ctDNA clearance of 3.7 and 2 (range: 1–16 cycles). The 3-year EFS rate was 92% in 27 patients who were ctDNA(-) after pembrolizumab compared to 20% (95% CI: 10–70%) in five patients who were ctDNA(+) after pembrolizumab (p < 0.001) (Fig. 2A). The 3-year OS rate was 100% in 27 patients who were ctDNA(-) after pembrolizumab compared to 80% (95% CI: 52% – NA) in five patients who did not clear ctDNA (e.g., were ctDNA(+) after pembrolizumab) (p < 0.001) (Fig. 2B).

A – 3-year event-free survival (EFS) rate by circulating tumor DNA (ctDNA) status after pembrolizumab. Kaplan–Meier curves for EFS according to ctDNA status after completion of pembrolizumab. Patients who were ctDNA-negative after pembrolizumab (n = 27) experienced a significantly higher 3-year EFS rate than those who were ctDNA-positive after pembrolizumab (n = 5) (92% vs 20%; log-rank P < 0.001). Tick marks indicate censored observations, and shaded areas represent 95 % CI. Red curve = patients who were ctDNA-negative after pembrolizumab. Blue curve = patients who were ctDNA-positive after pembrolizumab. B 3-year overall survival (OS) rate by circulating tumor DNA (ctDNA) status after pembrolizumab. Kaplan–Meier curves for OS according to ctDNA status after completion of pembrolizumab. Patients who were ctDNA-negative after pembrolizumab (n = 27) experienced a significantly higher 3-year OS rate than those who were ctDNA-positive after pembrolizumab (n = 5) (100% vs 80%; log-rank P < 0.001). Tick marks indicate censored observations, and shaded areas represent 95 % CIs. Red curve = patients who were ctDNA-negative after pembrolizumab. Blue curve = patients who were ctDNA-positive after pembrolizumab.
Among evaluable patients with CRC, no clinical features (tumor sidedness, T4 disease, node-positive disease, or BRAF p.V600E mutation) were associated with the presence of detectable baseline ctDNA (Supplementary Table 2). For patients with CRC who had detectable baseline ctDNA, the change in VAF (either increase or decrease) over the treatment period was concordant with imaging (either progression or response) in all patients (Supplementary Table 3).
ctDNA as a marker of pathologic response in patients with CRC
Of the seven patients with CRC who underwent surgery and had detectable ctDNA at baseline, five cleared their ctDNA in the neoadjuvant period, among whom four had a pCR (80% likelihood of pCR with ctDNA clearance). Notably, the one patient who did not have a pCR despite clearing ctDNA had a near-pCR (adenocarcinoma identified in only 1 of 91 lymph nodes). Neither of the two patients who did not clear ctDNA experienced a pCR (0% likelihood of pCR without ctDNA clearance) (Supplementary Figs. 2 and 3). All seven patients with CRC who were ctDNA(-) at baseline had a pCR, while only four of the seven patients who were ctDNA(+) at baseline had a pCR (100% vs 57%; p = 0.19) (Supplementary Table 4). Eleven of 12 patients who were cDNA(-) after pembrolizumab had a pCR, compared to neither of the two patients who were ctDNA(+) after pembrolizumab (92% vs 0%; p = 0.03) (Supplementary Table 5). Patients who were either ctDNA(+) at baseline and cleared ctDNA or were ctDNA(-) at baseline and remained so were more likely to have pCR compared to patients who were ctDNA(+) at baseline and remained ctDNA(+) (p = 0.01) (Supplementary Table 6).
ctDNA as a marker of response in patients with CRC who did not undergo surgery
Of 12 evaluable patients who did not undergo surgery, those who were ctDNA(+) at baseline and remained so had a 2-year EFS rate of 33% (95% CI: NA – 87%), whereas patients who were ctDNA(+) at baseline but cleared ctDNA had a 2-year EFS rate of 100%. Patients who were ctDNA(-) and remained so also had a 2-year EFS rate of 100% (Supplementary Fig. 4).
Discussion
At a median follow-up of approximately 3 years, no late progression events have occurred in patients with locally advanced dMMR/MSI-H solid tumors who underwent surgery or watchful waiting following pembrolizumab. The absence of ctDNA after pembrolizumab was associated with longer 3-year EFS and OS in all patients, pCR in patients with CRC who underwent surgery, and 2-year EFS in patients with CRC who did not undergo surgery. Clearance of ctDNA among patients who had detectable ctDNA at baseline happened early in the treatment course, after a median of two cycles of pembrolizumab. There was no difference between the 3-year EFS and OS rates among patients who underwent surgery and those who did not. This suggests surgery may not have significantly influenced survival, supporting the notion that organ preservation is a viable option in certain scenarios. However, the relatively small number of patients and heterogeneous clinical characteristics in this cohort may limit the generalizability of this finding. The rationale for the concept of neoadjuvant immunotherapy’s continued effectiveness after its discontinuation stems from the notion that an intact primary tumor results in a more robust antitumor immune response, which may partly explain the long-term efficacy seen in this cohort, particularly among the patients who did not undergo surgery. Clearance of ctDNA seems to be a favorable marker for treatment efficacy, which may be related to underlying mechanisms of intrinsic or acquired resistance to immunotherapy that remain poorly understood.
Evidence of neoadjuvant immunotherapy’s efficacy in dMMR/MSI-H solid tumors is growing. In NICHE-2, 95% of 112 patients with non-metastatic dMMR colon cancer treated with one dose of ipilimumab and two doses of nivolumab, followed by surgery, experienced a major pathologic response (≤10% residual viable tumor), while 67% of patients had a pCR11. Further, in a separate report of 12 patients with stage II or III dMMR rectal adenocarcinoma, all 12 had a clinical complete response and none experienced disease progression or recurrence during follow-up (range: 6–25 months)2. In the NEONIPIGA phase II trial, 17 of 29 patients with dMMR/MSI-H gastric and gastroesophageal adenocarcinoma who received six cycles of nivolumab with two cycles of ipilimumab followed by resection and nine cycles of adjuvant nivolumab had a pCR, and most patients were disease-free at a median follow-up of 14.9 months12.
No consensus exists regarding the optimal number of cycles of neoadjuvant immunotherapy for patients with dMMR/MSI-H solid tumors, and the regimens utilized in trials evaluating the efficacy of immunotherapy in patients with localized disease vary widely. While neoadjuvant immunotherapy has shown efficacy and continues to be incorporated into perioperative treatment paradigms, risks such as treatment-related adverse events are not negligible and may preclude curative-intent surgery. In one meta-analysis of 16,976 patients enrolled in 28 randomized controlled trials that involved either neoadjuvant or adjuvant immunotherapy, the addition of immunotherapy increased the incidence of adverse events leading to treatment discontinuation (odds ratio 3.67, 2.45–5.5; p < 0.0001)13. Therefore, serially monitoring ctDNA, in addition to utilizing imaging and endoscopy, could be a way to identify patients that have higher probabilities of achieving a pCR and prolong EFS and OS while reducing the risk of imparting toxicity from “unnecessary” cycles of neoadjuvant immunotherapy (i.e., in a patient with a clinical complete response and ctDNA clearance but scheduled to receive more cycles of neoadjuvant immunotherapy).
Clearance of ctDNA after neoadjuvant therapy has been shown to be associated with pathologic response in patients with some types of solid tumors. In a phase II trial of neoadjuvant atezolizumab plus docetaxel and oxaliplatin in 14 patients with resectable gastric and gastroesophageal junction adenocarcinomas, clearance of ctDNA prior to surgery correlated with pathological response (p = 0.03)12. Similarly, in an analysis of 84 patients with early-stage breast cancer who received neoadjuvant therapy, patients who remained ctDNA(+) were more likely to have incomplete pathologic response (OR 4.33, p = 0.01)14. However, in patients with proficient MMR (pMMR)/microsatellite stable (MSS) CRC treated with chemotherapy-based neoadjuvant approaches, the association between ctDNA clearance and pathologic complete response is less clear15,16,17,18,19,20. There are likely differences, which remain poorly understood, in how dMMR/MSI-H CRC tumors respond to immunotherapy compared to how pMMR/MSS CRC tumors respond to chemotherapy that influence ctDNA clearance.
Lack of ctDNA clearance after neoadjuvant therapy and shorter survival has been demonstrated in some types of solid tumors. In a cohort of 22 patients with early-stage NSCLC treated with neoadjuvant therapy, detectable ctDNA prior to surgery was associated with inferior RFS compared to patients without detectable ctDNA prior to surgery (HR 7.41, 95% CI: 0.91 – 60.22, p = 0.03)21. In two analyses of patients with early-stage breast cancer who received neoadjuvant chemotherapy, ctDNA detection before surgery was associated with shorter event-free survival (HR 53, 95% CI: 4.5 to 624; P < 0.01) and inferior DFS (HR 2.67, 95% CI: 1.28 – 5.57, p = 0.09)22,23. In 36 patients with localized rectal cancer who received neoadjuvant chemotherapy and radiation, detectable ctDNA after neoadjuvant therapy was associated with a higher risk of disease progression (HR 6.5, 95% CI: 1.4–30.3, p = 0.02)16. These data are consistent with our findings regarding the associations between the absence of detectable ctDNA after pembrolizumab with pCR (in patients with CRC who underwent surgery) and 3-year EFS and OS rates (in all patients).
As the decision to undergo surgery was determined by the patient and treating physician, the surgical and non-surgical groups of patients have inherent selection bias. Another limitation is the small sample size of the various cohorts analyzed and the single-institution nature of the clinical trial. Only a couple of patients in our analysis had cancer types other than CRC, which limits the applicability of our findings to patients with non-CRC dMMR/MSI-H tumors. Lastly, panel-based ctDNA assays may have lower depth of sequencing coverage and are likely to have worse performance characteristics than dedicated tumor-informed ctDNA assays.
Pembrolizumab monotherapy continues to show favorable outcomes in patients with locally advanced dMMR/MSI-H solid tumors at 3-year follow-up. Our work suggests the feasibility and potential of utilizing ctDNA dynamics as a marker to track response to neoadjuvant immunotherapy in patients with dMMR/MSI-H solid tumors. In the future, “ctDNA-adaptive” clinical trials, in which neoadjuvant immunotherapy regimens are tailored to each patient based on their disease’s response, could be a way to personalize therapeutic regimens to improve survival while minimizing the risk of toxicity associated with systemic therapy. Further, ctDNA may be an important tool to help clinicians and patients decide whether to proceed with surgery or pursue an organ-sparing approach, and serially monitoring ctDNA may improve sensitivity for assessing response when combined with traditional modalities such as imaging and endoscopy.
Methods
Study design and eligibility
In a phase II, investigator-initiated, open-label clinical trial (NCT04082572), 35 patients with locally advanced, histologically confirmed dMMR/MSI-H solid tumors were enrolled. Fifteen were female and 20 were male. Patients were not compensated. Locally advanced disease was defined as a nonmetastatic primary cancer with at least a 20% chance of recurrence with surgical resection alone3. The planned treatment course was pembrolizumab 200 mg intravenously once every three weeks for up to eight cycles, followed by surgical resection. An option for nonsurgical management was provided, in which patients could receive pembrolizumab for 16 cycles, followed by observation. The study was conducted in accordance with the Declaration of Helsinki and with approval from the University of Texas MD Anderson Cancer Center institutional review board.
Blood collection and ctDNA detection
Blood was collected in cell-free DNA (cfDNA) blood collection tubes (Streck Corp, La Vista, NE). The samples were processed within 24 h of collection, and cell-free plasma was frozen at ≤ − 70 degrees Celsius until analysis. ctDNA testing was performed in the CLIA-certified Molecular Diagnostics Laboratory at MD Anderson Cancer Center using a 70-gene liquid biopsy panel (LBP-70), which uses digital next-generation sequencing (NGS) of cell-free circulating DNA isolated from plasma to screen for single-nucleotide variants, insertions/deletions, copy number gains, and gene fusions. The software versions used for this analysis are Illumina NextSeq Control Software 2.1.0, Illumina Realtime Analysis Software 2.4.11, and Bioinformatics Pipeline 3.3.1. Detailed information about signal processing, base calling, alignment, variant calling, and copy number calling are available upon request. Formalin-fixed paraffin-embedded tumor samples and germline peripheral blood mononuclear cells were profiled using a targeted NGS platform. Mutations in ctDNA were considered tumor-specific if they were confirmed with matched tumor tissue profiling (Supplementary Table 1). ctDNA clearance was defined as a reduction in baseline (i.e., prior to pembrolizumab) mutational variant allele frequency (VAF) to a threshold below the LBP−70’s validated limit of detection (i.e., < 0.3% VAF for 30 ng of cfDNA input) in all tissue-matched mutations after treatment with pembrolizumab. Among all 35 patients, ctDNA analysis was performed on 129 samples, with a mean and median of 3.7 and 3 samples per patient. The time points at which blood was collected for ctDNA collection were typically at “baseline” (prior to pembrolizumab), after completion of pembrolizumab, and at various time points over the course of treatment with pembrolizumab.
Data analysis
The distribution of each continuous variable was summarized by its mean, median, and range. The distribution of each categorical variable was summarized in terms of its frequencies and percentages. The associations between categorical variables were compared using Fisher’s exact test. Kaplan-Meier methods were used to estimate unadjusted time-to-event EFS and OS. OS was defined as the time from the first cycle of pembrolizumab until death or censored at the last follow-up. EFS was defined as the time from the first cycle of pembrolizumab until disease progression or death, or censored at the last follow-up. Log-rank tests were used to compare each time-to-event variable between groups. P-values of < 0.05 (two-sided) were considered significant. All computations were carried out in SAS version 9.4 and R version 4.2.1.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Due to constraints related to patient privacy and institutional regulations, we cannot publicly share the source data file, targeted sequencing data, and code used in this manuscript. Researchers seeking further details may contact the corresponding author. Requests will be considered on a case-by-case basis in accordance with ethical and legal obligations. All remaining data can be found in the article and supplementary files.
References
Chalabi, M. et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat. Med. 26, 566–576 (2020).
Cercek, A. et al. PD-1 Blockade in mismatch repair–deficient, locally advanced rectal cancer. N. Engl. J. Med. 386, 2363–2376 (2022).
Ludford, K. et al. Neoadjuvant pembrolizumab in localized microsatellite instability high/deficient mismatch repair solid tumors. J. Clin. Oncol. 41, 2181–2190 (2023).
Jia, W., Gao, Q., Han, A., Zhu, H. & Yu, J. The potential mechanism, recognition and clinical significance of tumor pseudoprogression after immunotherapy. Cancer Biol. Med. 16, 655–670 (2019).
Colle, R. et al. Pseudoprogression in patients treated with immune checkpoint inhibitors for microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer. Eur. J. Cancer 144, 9–16 (2021).
Fox, D. A. et al. Endoscopic and imaging outcomes of PD-1 therapy in localised dMMR colorectal cancer. Eur. J. Cancer 194, 113356 (2023).
Swanton, C. Intratumor heterogeneity: Evolution through space and time. Cancer Res. 72, 4875–4882 2012.
Kotani, D. et al. Molecular residual disease and efficacy of adjuvant chemotherapy in patients with colorectal cancer. Nat. Med. 29, 127–134 (2023).
Tie, J. et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage II colon cancer. N. Engl. J. Med. 386, 2261–2272 (2022).
Kato, S. et al. 105P Dynamic change in blood derived variant allele frequency as a predictive marker for response from checkpoint inhibitor based therapies among metastatic solid tumours. Annals Oncol. 31, https://doi.org/10.1016/j.annonc.2020.08.225 (2020).
Chalabi, M. et al. LBA7 Neoadjuvant immune checkpoint inhibition in locally advanced MMR-deficient colon cancer: The NICHE-2 study. Annals Oncol. 33, https://doi.org/10.1016/j.annonc.2022.08.016 (2022).
Verschoor, Y. L. et al. Neoadjuvant atezolizumab plus chemotherapy in gastric and gastroesophageal junction adenocarcinoma: the phase 2 PANDA trial. Nat. Med. 30, 519–530 (2024).
Fujiwara, Y. et al. Treatment-related adverse events, including fatal toxicities, in patients with solid tumours receiving neoadjuvant and adjuvant immune checkpoint blockade: a systematic review and meta-analysis of randomised controlled trials. Lancet Oncol. 25, 62–75 (2024).
Magbanua, M. J. M. et al. Circulating tumor DNA in neoadjuvant-treated breast cancer reflects response and survival. Ann. Oncol. 32, 229–239 (2021).
Zhou, J. et al. Serial circulating tumor DNA in predicting and monitoring the effect of neoadjuvant chemoradiotherapy in patients with rectal cancer: A prospective multicenter study. Clin. Cancer Res. 27, 301–310 (2021).
Khakoo, S. et al. MRI tumor regression grade and circulating tumor DNA as complementary tools to assess response and guide therapy adaptation in rectal cancer. Clin. Cancer Res. 26, 183–192 (2020).
McDuff, S. G. R. et al. Circulating tumor DNA predicts pathologic and clinical outcomes following neoadjuvant chemoradiation and surgery for patients with locally advanced rectal cancer. JCO Precis Oncol. https://doi.org/10.1200/po.20.00220 (2021).
Tie, J. et al. Serial circulating tumour DNA analysis during multimodality treatment of locally advanced rectal cancer: A prospective biomarker study. Gut. 68, 663–671 (2019).
Vidal, J. et al. Clinical impact of presurgery circulating tumor DNA after total neoadjuvant treatment in locally advanced rectal cancer: A biomarker study from the GEMCAD 1402 trial. Clin. Cancer Res. 27, 2890–2898 (2021).
Murahashi, S. et al. Serial circulating tumour DNA analysis for locally advanced rectal cancer treated with preoperative therapy: prediction of pathological response and postoperative recurrence. Br. J. Cancer 123, 803–810 (2020).
Yue, D. et al. Circulating tumor DNA predicts neoadjuvant immunotherapy efficacy and recurrence-free survival in surgical non-small cell lung cancer patients. Transl. Lung Cancer Res. 11, 263–276 (2022).
Radovich, M. et al. Association of circulating tumor DNA and circulating tumor cells after neoadjuvant chemotherapy with disease recurrence in patients with triple-negative breast cancer. JAMA Oncol. 6, 1410–1415 (2020).
Cailleux, F. et al. Circulating tumor DNA after neoadjuvant chemotherapy in breast cancer is associated with disease relapse. JCO Precis Oncol. https://doi.org/10.1200/po.22.00148 (2022).
Acknowledgements
We thank the enrolled patients, study support staff, treating clinicians, and investigators for their invaluable contributions to this research.
Author information
Authors and Affiliations
Contributions
Conception and design: Michael LaPelusa, Kaysia Ludford, Wei Qiao, Van Morris, Scott Kopetz, Michael Overman Financial support: Michael Overman Administrative support: Michael Overman Collection and assembly of data: Michael LaPelusa, Wei Qiao, Bryan Iorgulescu, Francis San Lucas, Kaysia Ludford, Michael Overman Data analysis and interpretation: Michael LaPelusa, Wei Qiao, Bryan Iorgulescu, Francis San Lucas, Deepak Bhamidipati, Kaysia Ludford, Michael Overman Manuscript writing: All authors Final approval of manuscript: All authors Accountable for all aspects of the work: All authors.
Corresponding author
Ethics declarations
Competing interests
Scott Kopetz has ownership interest in Lutris, Frontier Medicines, Navire and is a consultant for Genentech, Merck, Boehringer Ingelheim, Bayer Health, Pfizer, Mirati Therapeutics, Flame Biosciences, Carina Biotech, Frontier Medicines, Replimune, Bristol-Myers Squibb-Medarex, Amgen, Tempus, Harbinger Oncology, Zentalis, AVEO, Tachyon Therapeutics, Agenus, Revolution Medicines, Kestrel Therapeutics, Roche, Arcus Biosciences, AstraZeneca Pharmaceuticals, BeiGene, Clasp Therapeutics, Cytovation, Dewpoint Therapeutics, Marengo Therapeutics, SageMedic, Servier, Sibylla, T-Cypher Bio, XAIRA, AmMax Bio, Ikena, and receives research funding from, Guardant Health, Genentech/Roche, EMD Serono, Amgen, Lilly, Daiichi Sankyo, Pfizer, Boehringer Ingelheim, BridgeBio, Zentalis, BioMed Valley, Johnson & Johnson, BMS, Cardiff, Jazz Pharmaceuticals, Frontier Medicines. Michael Overman is a consultant for Merck, Roche, BMS, Astrazeneca, Janssen, Pfizer, Summit, Nouscom, and Amgen. The other authors have no relevant competing interests to disclose.
Peer review
Peer review information
Nature Communications thanks Jun Gong, and the other anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
LaPelusa, M., Qiao, W., Iorgulescu, B. et al. Long-Term Efficacy of Pembrolizumab and the Clinical Utility of ctDNA in Locally Advanced dMMR/MSI-H Solid Tumors. Nat Commun 16, 4514 (2025). https://doi.org/10.1038/s41467-025-59615-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-025-59615-3
