
Abstract
Understanding the distribution of respiratory syncytial virus (RSV) disease burden by more granular age bands in infants is necessary for optimising infant RSV immunisation strategies. Using a Bayesian model, we synthesised published data from a systematic literature review and unpublished data shared by international collaborators for estimating the distribution of infant RSV hospitalisations by month of age. Based on local RSV seasonality data, we further developed and validated a web-based prediction tool for estimating infant RSV hospitalisation distribution by birth month. Although RSV hospitalisation burden mostly peaked at the second month of life and was concentrated in infants under six months globally, substantial variations were noted in the age distribution of RSV hospitalisation among infants born in different months. Passive immunisation strategies should ideally be tailored to the local RSV disease burden distribution by age and birth month to maximise their per-dose effectiveness before a universal immunisation can be achieved.
Similar content being viewed by others

Introduction
Human respiratory syncytial virus (RSV) is a leading pathogen causing acute lower respiratory tract infections in infants and young children1,2. Infants (less than 1 year of age) have a disproportionally high RSV hospitalisation burden; globally in 2019, over 60% (2.2 million) of RSV hospitalisations in children under five years occurred in infants3. The mortality burden of RSV in infants was also substantial, accounting for 65% of RSV-attributable deaths among children under five years3.
Given the high global disease burden of RSV, and the availability of safe and efficacious products for passive immunization of infants, the World Health Organization’s Strategic Advisory Expert Group (SAGE) recently recommended introduction of these products in all member states to prevent severe RSV disease in young infants4. Currently, two RSV passive immunisation products targeting infants have received licensure, including a long-acting monoclonal antibody (nirsevimab) to be administered directly to infants and a maternal vaccine (RSVPreF) for administration in pregnant persons5. With documented duration of protection of five months post dose and through age six months for nirsevimab6 and RSVpreF7, respectively, tailoring implementation of these strategies according to the burden of disease by finer age bands could be considered to help maximise their population level impact. Existing studies from several European countries, Singapore, and Kenya reported a month-by-month age distribution of RSV hospitalisation, consistently showing that the hospitalisation burden of RSV peaked in the second month of life8,9,10. However, no global-level studies were identified that reported the age distribution of RSV hospitalisation burden with similar granularities in age bands.
Moreover, RSV exhibits clear seasonality in most parts of the world and the timing of seasonal epidemics varies by regions (e.g., by latitude)11; as a result, the risk for RSV hospitalisation throughout the first year of life also differed by month of birth relative to the local RSV season. Previous studies showed that infants born 2–3 months before the peak month of RSV season had the highest risk of hospitalisation during infancy12,13. Therefore, further stratification of the age distribution of RSV hospitalisation by birth month is necessary for decision-making regarding RSV immunisation in locations with distinct RSV seasonality.
In this study, we aimed to understand the month-by-month distribution of RSV hospitalisations among infants across the globe and to develop an online prediction tool for regions with varied RSV seasonality to compare the infant RSV hospitalisation risk across different birth months.
Results
Descriptive analysis of the study dataset
A total of 89 studies identified from the systematic literature search met our inclusion criteria (see “Methods”). With the addition of one published study14 identified from expert recommendation, 27 studies identified through re-screening the data in our previously published analysis of global RSV disease burden in young children3,15, and unpublished data from further 18 studies shared by Respiratory Virus Global Epidemiology Network (RSV GEN) collaborators (details in “Methods”), a total of 135 studies were eligible for inclusion (Fig. 1). The majority (129/135, 96%) of included studies had an overall quality assessment score of ≥6 (rated as “Good” or “Very good”; detailed quality assessment results are presented in Supplementary Tables 1–3). For the main analysis of age distribution of RSV hospitalisation, one study16 was excluded as it reported pooled results from multiple countries across different income levels. The remaining 134 studies provided a total of 1,054,869 RSV hospitalisations from 49 countries, including 30 high-income countries (94 datasets; note that a study could include multiple datasets; e.g., a study may provide data for 3 countries at the same time, and the data from each country is considered a separate dataset), 13 upper-middle-income countries (44 datasets), and 6 lower-middle-income countries (8 datasets); no studies were from low-income countries (according to the World Bank country income classification in 2019) (Supplementary Fig. 1). Of these 49 countries, 30 were in the temperate regions (102 datasets), 8 in the sub-tropical regions (29 datasets) and 11 in the tropical regions (15 datasets). Detailed characteristics of the included studies were presented in Supplementary Tables 4–6.

The diagram shows the screening process of eligible data for analysis. *Other reasons included duplication, unavailability of case numbers, model predictions, and not RSV hospitalisation cases. †Identified from expert recommendation, which was deemed eligible per inclusion requirements despite not being identified in the search. ‡Evident from titles or abstracts that the records did not contain data on age distribution of RSV hospitalisation.
RSV hospitalisation by chronological month of age
The model-synthesised results by country-income level showed that the burden of RSV hospitalisations during infancy first increased then decreased with increasing months of age. In high-income and upper-middle-income countries, the proportion of RSV hospitalisations was highest at 1– < 2 month of age with the corresponding proportion of 20.6% and 18.0% (95% credible interval: 19.4–21.7 and 16.0–20.2), respectively, while in lower-middle-income countries/low-income countries, the proportion peaked at 2– < 3 months of age (15.5%, 11.1–19.8) (Fig. 2). In lower-middle-income countries/low-income countries, more than 60% of the RSV hospitalisations during infancy occurred by the age of 6 months (64.4%, 95% credible interval: 61.5–67.5) and this proportion was even higher in upper-middle-income (70.3%, 68.7–72.1) and high-income countries (75.6%, 74.5–76.6) (Fig. 2 and Supplementary Table 7). The distribution of RSV hospitalisation by age was also generally consistent from year to year (Supplementary Fig. 2). Sensitivity analyses that only included studies reporting PCR confirmed RSV and that excluded studies with low quality yielded similar results to the main analysis (Supplementary Fig. 3).

A shows the age-specific proportion and B shows the age-cumulative proportion, by country income level. Lines indicate the medians and shaded areas indicate 95% credible intervals. HICs High-income countries, UMICs Upper-middle-income countries, LMICs Lower-middle-income countries, LICs Low-income countries. Source data are provided as a Source Data file.
To further verify that the age of peak RSV hospitalisation was not a model artefact, as an ad-hoc verification analysis, we performed a descriptive analysis of 54 studies with had available data for each month of age (i.e., not combining any months of age in reporting) with no modelling. Over three quarters of these studies (41/54, 75.9%) had highest RSV hospitalisation proportion at 1– < 2 month; among the rest of the studies, seven and six studies had the highest proportion of hospitalisation at 0– < 1 month and at 2– < 3 months, respectively (Supplementary Fig. 4). When stratifying the analysis by latitudinal group, the peak RSV hospitalisation consistently occurred at 1– < 2 month of age although in tropical regions, the proportion of RSV hospitalisations at 1– < 2 months was lower than in sub-tropical and temperate regions (Supplementary Fig. 5). When stratifying the analysis by both country income level and latitudinal group, all regions had the highest proportion of RSV hospitalisations at 1– < 2 month, except for lower-middle-income countries/low-income countries in tropical region, which had the highest proportion at 2– < 3 month (Fig. 3). The model for lower-middle-income countries/low-income countries in the sub-tropical regions and temperate regions did not reach convergence due to limited data, and therefore, the results were not presented (all original trace plots of individual models can be found in Supplementary Figs. 6–10). When stratified by country income level, variations remained small in the age distribution across different latitudinal regions.

Lines indicate the medians and shaded sections indicate 95% credible intervals. HICs High-income countries, UMICs Upper-middle-income countries, LMICs Lower-middle-income countries, LICs Low-income countries. Source data are provided as a Source Data file.
Development and validation of the prediction tool
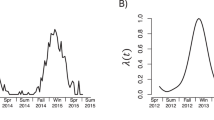
For developing the prediction tool for RSV hospitalisation by birth month, we considered two key independent determinants at the population level: chronological month of age, which reflects the changes in inherent susceptibility to RSV diseases, and RSV circulation in the community (i.e., seasonality), which is external factor that determines the risk of exposure to RSV. As a child experiences varying levels of RSV circulation at varying age, RSV hospitalisation distribution by birth month is jointly determined by local RSV seasonality and chronological month of age (see “Methods”). As RSV hospitalisation distribution by chronological month of age was already estimated earlier in this study, the prediction would require only information on local RSV seasonality (Fig. 4).

A shows an example of the relationship between distribution of RSV hospitalisation by chronological month of age and month of birth. B explains how the RSV hospitalisation distribution by birth month is estimated in this study.
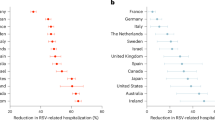
Among 25 studies that had available data on both RSV seasonality (for prediction) and RSV hospitalisation by birth month (for validation), we found that the prediction model had overall consistent distribution of RSV hospitalisations by birth month with the observed data, although the absolute proportion estimates for some of the birth months were different (Fig. 5 and Supplementary Fig. 11). The model-predicted peak birth month (i.e., birth month with the highest proportion of RSV hospitalisations in the first year of life) was consistent with the actual peak birth month in 11 (44%) of the studies; 10 studies (40%) had a difference of one month between the model-predicted peak birth month and the observed peak birth month.

The top three figures show the linear regression analysis (means and 95% confidence intervals) and Pearson’s correlation coefficients between the model-predicted and observed results across different study sites stratified by country income level; points in purple indicated a selected site with the highest number of RSV hospitalisations in the first year of life for demonstration, with the corresponding bottom figure showing the comparison between model-predicted (in red, medians and 95% prediction intervals) and observed (in blue) values. HICs High-income countries, UMICs Upper-middle-income countries, LMICs Lower-middle-income countries, LICs Low-income countries. Source data are provided as a Source Data file.
Pearson correlation analyses of model-predicted with actual cumulative proportions of RSV hospitalisations by birth month were highly correlated, consistently across different income levels, with the correlation coefficient ranging from 0.84 in lower-middle-income countries/low-income countries to 0.90 in high-income countries (Fig. 5). High correlation results remained when further stratifying the correlation analysis by each chronological age (Supplementary Fig. 12).
Prediction of RSV hospitalisation by birth month
Using country-specific RSV seasonality data, we predicted the distribution of RSV hospitalisation by birth month in 33 countries. We found that the age distribution of RSV hospitalisation differed substantially by birth months (Supplementary Fig. 13). The month of age with highest RSV hospitalisation also varied substantially by month of birth relative to the local RSV season. Among the 12 calendar birth months, only a median of three birth months (IQR: 2–4) had the highest RSV hospitalisation risk at the second month of life across 33 countries; beyond the first six months of age, the highest RSV hospitalisation risk occurred over a median of four birth months (IQR: 3–5).
The age-cumulative infant RSV hospitalisation burden also varied substantially by birth months, except for Suriname and Yemen, both in the tropical region (Fig. 6). The risk ratios between the birth month with the highest cumulative proportion of RSV hospitalisations and the birth month with the lowest cumulative proportion of RSV hospitalisations for the first 6 months of life ranged from 1.79 (95% prediction interval: 1.45–2.26) in Yemen to 44.54 (20.74–116.79) in Morocco; the risk ratios for the first year of life ranged from 1.27 (1.16–1.40) in Yemen to 3.49 (3.21–3.79) in Uruguay (Supplementary Table 8). Compared to the month-by-month RSV activity, the birth month with the highest cumulative proportion of RSV hospitalisations in the first year of life was generally 1–3 months ahead of the peak RSV hospitalisation calendar month. At the latitudinal group level, the risk ratios for 0– < 6 months and for 0– < 12 months were highest in the temperate region (24.58, 95% prediction interval: 3.1–42.67; and 3.13, 1.62–3.58, respectively), followed by the sub-tropical region (16.53, 5.34–70.88; and 2.62, 1.68–3.73, respectively), and were lowest in the tropical region (4.24, 1.72–12.34; and 1.77, 1.25–2.63, respectively).

The figure presents predicted cumulative proportion in the first six month of life and first year of life by birth month, based on the proportion of RSV hospitalisations by calendar month as model input, stratified by latitudinal group. Source data are provided as a Source Data file.
Discussion
In this study, we conducted a systematic analysis to estimate month-by-month age distribution of RSV hospitalisations among infants from a global perspective. We showed the burden of RSV hospitalisations during infancy first increased then decreased with increasing months of age, with more than 60% of the RSV hospitalisations occurring in the first six months. RSV hospitalisation burden peaked at 1– < 2 month in high-income and upper-middle-income countries and at 2– < 3 months in lower-middle-income countries/low-income countries, while latitudinal-group stratified analysis showed a consistent peak at 1– < 2 months. The validated prediction tool for RSV hospitalisation burden by birth month could be used by countries without age-granular primary RSV hospitalisation data to understand how RSV hospitalisation burden was distributed by chronological month of age and by month of birth, and to refine RSV passive immunisation strategies specific to their local context. By predicting the RSV hospitalisation burden by birth month across 33 countries, we revealed the important role of birth month relative to the local RSV season in determining the risk for hospitalisation, in the temperate and sub-tropical regions, as well as in most of the countries in the tropics albeit to a lesser extent.
As expected, the hospitalisation burden decreased with increase in age after the second or third month of life, which corresponds with the steady development of an infant’s immune system and respiratory tract17,18. For the first month of life, the relatively lower RSV hospitalisation burden compared to the second month might be due to protection from maternal-transferred RSV antibodies acquired through prior maternal infection which may have rapidly declined by the second month of life19,20; limited exposure to individuals/settings outside the home in the first few weeks of life may also be a factor. RSV hospitalisation burden peaked mostly at the second month of life across income levels and latitudinal regions, and were consistent from year to year, suggesting that RSV immunisation targeting protection for the first few months of life could be impactful. However, there were some regional variations: RSV hospitalisation burden peaked one month of age older in lower-middle-income countries/low-income countries and was less concentrated in the first six months of life in lower-middle-income countries/low-income countries and in the tropical regions. In resource-poor settings, such as the lower-middle-income countries/low-income countries in this study, the possible effect of survivors21 could explain the later peak and smaller proportion of RSV hospitalisation in the younger age groups; infants who were at higher risks for RSV hospitalisation might have died at a younger age in these resource-poor settings. Variations in the peak RSV burden by country income level were consistently observed in our previous study3. In the tropical settings, RSV circulation and transmission patterns differed from temperate settings11, which could affect maternal RSV-specific antibody level although there were no available serology studies for further verification of this speculation.
Although the overall findings on the age distribution of RSV hospitalisation favoured a birth dose approach for implementing RSV monoclonal antibodies, we showed that the risks for RSV hospitalisation could also vary substantially by month of birth due to the seasonal activity of RSV. The differences in the proportion of RSV hospitalisations during the first six months of age between birth months could be over 20 times in the temperate region, 16 times in the sub-tropical region, and 4 times in the tropical region. The findings highlighted the importance for identifying high-risk month of birth and high-risk months of age window for infant RSV immunisation strategy. For example, countries such as Spain adopted a seasonal with catch-up immunisation strategy for nirsevimab, which was essentially a combination of birth dose (for those born during the RSV season) and catch-up dose (for those born outside the RSV season and younger than 6 month at the onset of RSV season)22. However, such recommendation required RSV epidemiology data by finer age bands of infants and by birth month, which could be limited in other countries, particularly among low- and middle-income countries. Therefore, we developed an open-access prediction tool that requires minimal local RSV activity data to reconstruct the RSV hospitalisation burden distribution by chronological month of age and calendar month of birth. The prediction tool demonstrated good predictability across different income levels and could be used by countries or regions that had limited RSV epidemiology data to identify high-risk birth cohorts and high-risk chronological age windows for prioritisation of RSV immunisation programmes to maximise their per-dose effectiveness. The tool could also be used to identify which pregnant people (based on month of expected delivery) should be prioritized for vaccination if year-round use of RSVpreF in pregnancy is not possible.
There were several limitations in this study. First, due to limited data of RSV hospitalisation burden by granular age bands, we were unable to estimate the age distribution in low-income countries separately. We speculated that the age distribution of RSV hospitalisation in low-income countries could be similar to that in lower-middle-income countries as they both had relatively high infant mortality rates. Second, there were heterogeneities across the included studies, including case definition, admission criteria, RSV testing criteria and methodology. However, we do not believe that these factors had a substantial impact on the estimated age distribution as our sensitivity analysis that included only PCR-confirmed RSV hospitalisation and excluded lower-quality studies yielded similar findings. Despite the varied reported age bands in individual studies, we developed a Bayesian approach that was less restrictive to the available age bands in individual studies, reducing potential publication bias and selection bias at the study level. Third, our prediction tool assumed that RSV seasonality was stable from year to year for simplicity; for countries with substantial year-on-year variations in RSV season onset (such as biennial patterns), the predicted results should be interpreted with caution. Moreover, we assumed that testing practice was stable enough to reflect the true local RSV seasonal patterns; when testing practice varied within a year, further work may consider incorporating other forms of RSV seasonality data, such as RSV testing positivity proportion. Fourth, while the external validation results showed that the model had overall consistent distribution of RSV hospitalisations by birth month with the observed data, discrepancy remained in the absolute proportion estimates for some of the birth months, which might potentially stem from variations in the number of births across different calendar months that were not accounted for in the model due to data scarcity. Nonetheless, such discrepancy did not compromise the potential public health implication of the model, which essentially relied on identifying birth cohorts with higher RSV hospitalisation proportion (rather than the precise absolute proportion). Moreover, we considered only RSV hospitalisation in this study, the more severe layer of the RSV disease spectrum, while RSV disease burden in the community and primary-care settings can be also important for decision-making in the implementation of RSV immunisations. Lastly, as current recommendation of RSV immunisation for the first year of life is based on whether infants are born during RSV season (i.e., the birth dose) or whether infants are relatively young when experiencing their first RSV season (i.e., the catch-up dose), regardless of perceived individual-level risk factors such as prematurity and comorbidities (which is more relevant to the recommendation for the second year of life, beyond the scope of this study). our study focused only on the overall distribution of RSV hospitalisation burden at the general population level, and did not intend to predict individual risks for RSV hospitalisation that could also be driven by individual-level risk factors.
Despite these limitations, our study improves the understanding of month-by-month distribution of RSV hospitalisation in infants in different income and latitudinal settings and provides further insights into the interplay between chronological month of age and month of birth relative to local RSV seasonality in determining the risk for RSV hospitalisation in infants. These findings have important implications for refining infant RSV immunisation strategy according to the local context of RSV hospitalisation burden and seasonality characteristics. For resource-poor countries with limited RSV epidemiology data, the developed open-access prediction tool in this study could be used to identify high-risk birth cohorts and high-risk chronological month of age windows for prioritisation for RSV immunisation strategy before affordable universal immunisation can be applied.
Methods
Data sources
Systematic literature review
We conducted a systematic literature review (PROSPERO registration: CRD42023424014) to identify published data on the age distribution of RSV diseases in infants. We searched four electronic databases, including EMBASE (Ovid), MEDLINE (Ovid), Global Health (Ovid) and Web of Science for studies published between January 1, 1995 and December 31, 2023, without language restrictions. The literature search used the following terms (with synonyms and closely related words): “respiratory syncytial virus”, “bronchiolitis”, “pneumonia”, “respiratory infection”, “incidence”, “morbidity”, “burden” and “epidemiology” (detailed search strategy is in Supplementary Methods 1).
We included studies that reported the incidence of laboratory-confirmed RSV hospitalisations for the complete first year of life; the reported estimates should have enough granularity in terms of months of age to help understand the month-by-month distribution of RSV disease, defined as at least one age group with an age interval of ≤3 months. Moreover, to be eligible, each study should have reported ≥100 RSV cases in the first year of life to ensure the robustness of the estimates. Studies that focused exclusively on high-risk infants (e.g., preterm, those with comorbidities, HIV-positive, etc.) or on nosocomial infections, or studies that only focused on the period following the onset of the coronavirus disease 2019 (COVID-19) pandemic (given the possible impact on the age distribution of RSV cases in infants23) were excluded. Studies identified by expert recommendation were also considered.
For eligible studies, a tailored data extraction spreadsheet was used to collect the relevant information, including characteristics of the study (such as country and setting, study period, income group, clinical diagnosis, testing approach, and granularity of age groups), and the number of RSV cases in each reported age band in the first year of life. The literature screening and data extraction were done independently by two review teams (team 1: LG and FM; team 2: SK and AC), with any disagreements arbitrated by YL.
Respiratory virus global epidemiology network
We included previously published data of RSV disease burden that were shared by members of the Respiratory Virus Global Epidemiology Network (RSV GEN)3,15. RSV GEN was previously established to collect unpublished data on RSV epidemiology (including re-analysis of published data), applying common case definitions and approaches to data analysis. RSV GEN comprises principal investigators of RSV-related studies who maintain full access to their respective study data. All contributed studies have obtained necessary ethical approvals, with shared data being provided exclusively in an aggregate form. As most of these data provided information on only five age groups of infants (0– < 1 m, 1– < 3 m, 3– < 6 m, 6– < 9 m and 9– < 12 m), we also wrote to RSV GEN members and requested more granular data on RSV hospitalisation using a new data request form. The data requested included month-by-month age distribution of RSV hospitalisations, seasonality of RSV hospitalisation and RSV hospitalisations by birth month. For any datasets with ≥1000 RSV hospitalisations, we also collected month-by-month age distribution of RSV hospitalisations by different calendar years as well as by birth months.
Quality assessment
For the included published and unpublished studies, two review teams (team 1: LG and FM; team 2: SK and AC) conducted the quality assessment independently, using a modified quality scoring form based on our previous published study on global disease burden of RSV in young children3 (Supplementary Methods 2). The quality scoring form included five questions that assessed the selection process of study subjects, testing practice, age representation, age group granularity and data accessibility. Each question was scored 0, 1 or 2 points, with the total score for the five questions ranging from 0 to 10 points. Total scores of 0–3, 4–5, 6–7 and 8–10 points corresponded to four levels of overall quality: poor, fair, good, and very good, respectively.
Data analysis
Overview
There were three parts of data analysis in this study: the first part estimated RSV hospitalisation distribution by chronological month of age; the second part developed and validated a prediction tool for estimating RSV hospitalisation distribution by birth month; the third part predicted the RSV hospitalisation distribution in different countries (Fig. 7).

The study consists of three parts: the first part estimates RSV hospitalisation distribution by month of age; the second part develops and validates a prediction tool for estimating RSV hospitalisation distribution by birth month; the third part predicts the RSV hospitalisation distribution in different countries.
Estimating RSV hospitalisation by chronological month of age
The outcome of interest for this analysis was the proportion of RSV hospitalisations by each month of age in the first year of life. Given the possible impact of COVID-1923, only data before January 1, 2020 were included. As indicated in previous global estimates of RSV disease burden3, we assumed the age distribution of RSV hospitalisations to vary mostly by country income and conducted data synthesis separately according to the World Bank country income classification for the median year of study24, as the main analysis. Briefly, for each stratum of country income, a hierarchical Bayesian model was used for data synthesis of the proportion of RSV hospitalisations by each month of age in the first year of life (the first month was defined as 0– < 28 days) while accounting for between-study variations, as shown in the formula below:
where \(s\) denotes each study (from the same stratum of country income); \({\vec{p}}_{s}\) denotes the proportion of RSV hospitalisations in each of the 12 months of age for each study, which follows a Dirichlet distribution; \({\vec{Y}}_{s}\) and \({N}_{s}\) are the RSV hospitalisation counts in each month of age and totally in the first year of life; α, as the concentration parameter of the Dirichlet distribution, represents the heterogeneity among studies within the same country income stratum. Here, α was set to a fixed value of 100, which was informed by a separate Dirichlet regression of a subset of our dataset that had available RSV hospitalisation counts for each month of age. \(\vec{p}\) denotes the proportion of RSV hospitalisations in each of the 12 months of age for each stratum of country income, which was the primary parameter of interest.
The advantage of this model was the ability to explicitly account for any combined age groups reported in some studies (for example, studies that combined the second month and third month into a 1– < 3 months age group in the reported estimates), by collapsing these categories for likelihood estimation, rather than excluding the entire study and compromising statistical efficiency. The model also accounted for heterogeneity among studies within the same country income stratum. More details about the model can be found in Supplementary Methods 3.
Given the variations in RSV epidemic patterns at different latitudes11, as secondary analysis, we stratified the analysis above by latitudinal group (temperate region, latitudes above 35° North or above 35° South; sub-tropical region, latitudes between 23.5 and 35° North or latitudes between 23.5 and 35° South; and tropical region, latitudes between 23.5 North and 23.5° South) as well as simultaneously by country income and latitudinal group. We further performed an exploratory analysis comparing year-on-year differences in the age distribution of RSV hospitalisations using data from RSV GEN. For sensitivity analyses, we excluded studies with total quality scores less than 6; and we also excluded studies that did not confirm RSV infection status with polymerase chain reaction (PCR).
Development and validation of a prediction tool for estimating RSV hospitalisation by birth month
We developed a prediction model to estimate the burden of RSV hospitalisation at different months of age for infants born in each month of the year. This was based on the assumption that RSV hospitalisation distribution by birth month was determined by two independent factors, namely chronological age (an inherent factor indicating susceptibility to RSV disease) and local RSV seasonality (an external factor indicating level of exposure to RSV); an illustrative example of this model is presented in Supplementary Methods 4. Under this assumption, the proportion of RSV hospitalisations per birth month was the product of the proportion of RSV hospitalisations by chronological month of age (based on the estimates of RSV hospitalisation distribution by age in the main analysis) and the proportion of RSV by calendar month of the year to be provided externally for the region of interest (Fig. 4). The age-specific proportion (\({r}_{j}^{k}\)) and age-cumulative proportion (\({r}_{J}^{k}\)) of RSV hospitalisations for a given birth month \(k\) could be estimated by:
where \({q}_{j}\) is the posterior estimate of the age-specific proportion of RSV hospitalisation in this study; \(\vec{p}\) denotes the proportion of RSV cases in each calendar month of a year, which is simulated from a Dirichlet-Multinomial conjugate model, with a uniform \({Dirichlet}({\mathrm{1,1}},\ldots,1)\) prior to represent no prior preference for any months. The posterior distribution of the proportions is then Dirichlet (1 + y₁, 1 + y₂, ..., 1 + y₁₂), where yi are the observed case counts from external data sources.
To validate the prediction, we compared the predicted infant RSV hospitalisation by birth month with the observed data obtained from the following sources: published data from five European countries (national hospital registries of Scotland, Denmark, Finland, Netherlands, and Norway)13, published data from Chongqing, China25 with additional data shared by the authors, and unpublished data shared by RSV GEN collaborators. For each birth month, both the cumulative proportion of RSV hospitalisations and the age-in-month-specific proportion of RSV hospitalisations were compared. Pearson correlation analysis was conducted to compare the predicted values and the observed values across different birth months, further stratified by country income classification.
Moreover, we developed a web-based user interface for accessing the prediction tool, freely available at https://idem.njmu.edu.cn/shiny/RSVbirthmonth/. End users are required to input the month-by-month number of RSV cases (i.e., the seasonality data) for the region/country of interest; then, based on the age distribution of RSV cases obtained in this study, the application will return the predicted results in two forms. The first shows the hospitalisation burden (as a proportion) by each month of age and each birth month. The second shows the cumulative hospitalisation burden (as a proportion) across different months of age by birth month. The user manual for the online prediction tool can be found in Supplementary Methods 5.
Predicting RSV hospitalisation distribution by birth month
Using nationwide RSV seasonality data (aggregated across multiple years) included in our previous global respiratory virus seasonality study11 and those shared by RSV GEN collaborators, we predicted the cumulative proportion of RSV hospitalisations in the first six month of life as well as in the first year of life by birth month in different countries. Furthermore, we calculated the risk ratio between the month of birth with the highest cumulative proportion of RSV hospitalisations and the month of birth with the lowest cumulative proportion of RSV hospitalisations to understand the variations in RSV hospitalisation risk between different birth months. In addition, for 12 calendar birth months, we summarised the number of birth months for which had the highest proportion of RSV hospitalisations in the second month of age or in 6– < 12 months of age for each country, and calculated the median and quartile for all the countries.
Statistical software and checklist
All data analyses and visualisations were done in the R software (version 4.2.2). This systematic literature review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Data from systematic literature review are publicly available and cited appropriately in this article. Data from the Respiratory Virus Global Epidemiology Network are not publicly available as the use of these data is restricted to this study only. Access requests can be sent to Prof. You Li (you.li@njmu.edu.cn). Response to requests can be expected within 10 working days. Source data for Figs. 2, 3, 5 and 6 are provided with this paper. Source data are provided with this paper.
Code availability
The R codes used in this analysis (include codes for online tool) are available on GitHub (https://github.com/Glinnnng/Age_distribution_infants)26; prediction tool is freely available at https://idem.njmu.edu.cn/shiny/RSVbirthmonth/.
References
Pneumonia Etiology Research for Child Health (PERCH) Study Group. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study. Lancet 394, 757–779 (2019).
Bénet, T. et al. Microorganisms associated with pneumonia in children <5 years of age in developing and emerging countries: the GABRIEL pneumonia multicenter, prospective, case-control study. Clin. Infect. Dis. 65, 604–612 (2017).
Li, Y. et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet 399, 2047–2064 (2022).
World Health Organization. Strategic Advisory Group of Experts on Immunization (SAGE). https://www.who.int/news-room/events/detail/2024/09/23/default-calendar/sage_meeting_september_2024 (2024).
Pecenka, C. et al. Respiratory syncytial virus vaccination and immunoprophylaxis: realising the potential for protection of young children. Lancet 404, 1157–1170 (2024).
Hammitt, L. L. et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N. Engl. J. Med. 386, 837–846 (2022).
Kampmann, B. et al. Bivalent prefusion F vaccine in pregnancy to prevent RSV illness in infants. N. Engl. J. Med. 388, 1451–1464 (2023).
Nyawanda, B. O. et al. Estimates of the national burden of respiratory syncytial virus in Kenyan children aged under 5 years, 2010−2018. BMC Med. 21, 122 (2023).
Tam, C. C. et al. Burden and cost of hospitalization for respiratory syncytial virus in young children, Singapore. Emerg. Infect. Dis. 26, 1489–1496 (2020).
Reeves, R. M. et al. Respiratory syncytial virus-associated hospital admissions in children younger than 5 years in 7 European countries using routinely collected datasets. J. Infect. Dis. 222, S599–s605 (2020).
Li, Y. et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: a systematic analysis. Lancet Glob. Health 7, e1031–e1045 (2019).
Li, Y., Batinović, E., Milić, P. & Markić, J. The role of birth month in the burden of hospitalisations for acute lower respiratory infections due to respiratory syncytial virus in young children in Croatia. PLoS ONE 17, e0273962 (2022).
Wang, X. et al. Respiratory syncytial virus-associated hospital admissions and bed days in children <5 years of age in 7 European countries. J. Infect. Dis. 226, S22–s28 (2022).
Buchan, S. A. et al. Estimating the incidence of first RSV hospitalization in children born in Ontario, Canada. J. Pediatric Infect. Dis. Soc 12, 421–430 (2023).
Shi, T. et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet 390, 946–958 (2017).
Vandendijck, Y. et al. Measuring respiratory syncytial virus infection severity in hospitalized children using the Pediatric Respiratory Syncytial Virus Electronic Severity and Outcome Rating System (PRESORS). Influenza Other Respir. Viruses 16, 1091–1100 (2022).
Iñiguez Osmer, F. & Sánchez, I. Development of the respiratory system. In Pediatric Respiratory Diseases: A Comprehensive Textbook (eds. Bertrand, P. & Sánchez, I.) 5–15 (Springer International Publishing, Cham, 2020).
Murphy, K., Travers, P. & Walport, M. Janeway’s Immunobiology (Janeway’s Immunobiology, 2014).
Langel, S. N., Blasi, M. & Permar, S. R. Maternal immune protection against infectious diseases. Cell Host Microbe 30, 660–674 (2022).
Buchwald, A. G. et al. Respiratory syncytial virus (RSV) neutralizing antibodies at birth predict protection from RSV illness in infants in the first 3 months of life. Clin. Infect. Dis. 73, e4421–e4427 (2021).
World Health Organization. Newborn Mortality. https://www.who.int/news-room/fact-sheets/detail/newborn-mortality (2024).
Ares-Gómez, S. et al. Effectiveness and impact of universal prophylaxis with nirsevimab in infants against hospitalisation for respiratory syncytial virus in Galicia, Spain: initial results of a population-based longitudinal study. Lancet Infect. Dis. 24, 817–828 (2024).
Cong, B. et al. Changes in the global hospitalisation burden of respiratory syncytial virus in young children during the COVID-19 pandemic: a systematic analysis. Lancet Infect. Dis. 24, 361–374 (2024).
World Bank Data Team. New Country Classifications by Income Level: 2019-2020. https://blogs.worldbank.org/opendata/new-country-classifications-income-level-2019-2020.
Li, T. et al. Defining RSV epidemic season in southwest China and assessing the relationship between birth month and RSV infection: A 10-year retrospective study from June 2009 to May 2019. J. Med. Virol. 95, e28928 (2023).
Guo, L. Respiratory syncytial virus hospitalisation by chronological month of age and by birth month in infants. Age_distribution_infants, https://doi.org/10.5281/zenodo.15593411 (2025).
Acknowledgements
The study is supported by the PROMISE project, which has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (under grant agreement number 101034339), and WHO through a grant from the Bill & Melinda Gates Foundation (number INV-005318). The Joint Undertaking receives support from the EU’s Horizon 2020 research and innovation programme and the European Federation of Pharmaceutical Industries and Associations. The authors alone are responsible for the views expressed in this Article, and they do not necessarily represent the views, decisions, or policies of the institutions with which the authors are affiliated. The Joint Undertaking is not responsible for any use that may be made of the information contained within this. The study was funded through CDC Interagency Agreement: 18FED1812054IPD. The study protocol (NAMRU6 2016.0007) was approved by the U.S. Naval Medical Research Unit SOUTH (NAMRU-SOUTH) Institutional Review Board in compliance with all applicable federal regulations governing the protection of human subjects. Y.L. acknowledged grant support from the National Natural Science Foundation of China (No. 82473692). The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention. The views expressed in this manuscript are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the U.S. Government. Some authors are federal employees of the United States government. This work was prepared as part of our official duties. Title 17 U.S.C. 105 provides that “copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a U.S. Government work as work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties.
Author information
Authors and Affiliations
Consortia
Contributions
Y.L. and H.N. conceptualised the study. L.G. and Y.L. co-led the literature review with contributions from F.M., A.C., and S.K. L.G. led data analysis with inputs from Y.L. L.G. led data interpretation and wrote the first draft with inputs from Y.L. and H.Z. T.B., M.C., J.-S.C., R.F., C.G., T.H., S.H., E.N.K., J.K., E.L., J.M., H.M., J.M., B.R., C.R., Q.W., M.W. and C.F.Y. contributed to collection of unpublished research data, data interpretation, and critically reviewed the initial manuscript. All members of Respiratory Syncytial Virus Global Epidemiology Network (RSV GEN) contributed to data collection and reviewed the manuscript for intellectual content. All authors read and approved the final draft for submission. L.G. and Y.L. had full access to and verified the aggregated study data for analysis in this study, and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Competing interests
H.N. reports grants from the Innovative Medicines Initiative, related to the submitted work; grants from WHO, the National Institute for Health Research, Pfizer, and Icosavax; and personal fees from the Gates Foundation, Pfizer, ReViral, GSK, Merck, Icosavax, Sanofi, Novavax and AbbVie, outside the submitted work. Y.L. reports grants by GSK, MSD and WHO; and personal fees from Pfizer, MSD and WHO, outside the submitted work. C.F.Y. reports grants from National Medical Research Council Singapore and Wellcome Trust, and funding to attend conferences and honorarium from Pfizer, Sanofi, Moderna and Takeda, outside the submitted work. T.H. reports grants from EC IHI (PROMISE) consortium, personal fees from MSD, Pfizer and Sanofi, and participation on data safety monitoring boards for Sanofi, MSD, Moderna and Pfizer, outside the submitted work. J.W.K. reports grants from National Institutes of Health, Merck Sharp and Dohme Corporation, National Science Foundation, Centers for Disease Control and Prevention and Greenwall Foundation, and participation on data safety monitoring boards for Enhancing the Diabetes Prevention Program to promote weight loss among non-responders in a community-based lifestyle intervention funded by National Institute of Diabetes and Digestive and Kidney Diseases, outside the submitted work. M.T.C. reports grants from The Bill and Melinda Gates Foundation and personal fees from Sanofi, outside the submitted work. E.L. reports grants from MSD R&D (China), outside the submitted work. H.C.M. reports grants from Sanofi-Aventis Australia and Merck Sharp and Dohme Australia, and participation on data safety monitoring boards for Advisory Boards for Merck Sharp and Dohme Australia, Pfizer and Sanofi, outside the submitted work. BAR participation on data safety monitoring boards for GSK Flu treatment in infants chairing a DSMB, and hold leadership roles as the Chair of the ISIRV Epidemiology Group and as a board member of ESGREV, outside the submitted work. All other authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Chris McKennan and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Guo, L., Kenmoe, S., Miyake, F. et al. Respiratory syncytial virus hospitalisation by chronological month of age and by birth month in infants. Nat Commun 16, 6109 (2025). https://doi.org/10.1038/s41467-025-61400-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-61400-1
This article is cited by
-
Taxonomy of the Full Health and Societal Value of Maternal Vaccination to Prevent Infant Respiratory Syncytial Virus Disease
Infectious Diseases and Therapy (2026)
