
Abstract
Janus kinase (JAK) inhibitors provide limited depth and durability of response in myelofibrosis. We evaluated pelabresib—a bromodomain and extraterminal domain (BET) inhibitor—plus ruxolitinib (a JAK inhibitor) compared with placebo plus ruxolitinib as first-line therapy. In this phase 3 study (MANIFEST-2), JAK inhibitor-naive patients with myelofibrosis were randomized 1:1 to pelabresib 125 mg once daily (QD; 50–175 mg QD permitted) for 14 days followed by a 7-day break (21-day cycle), or to placebo in combination with ruxolitinib 10 or 15 mg twice daily (BID; 5 mg QD–25 mg BID permitted). Primary endpoint was reduction in spleen volume of ≥35% from baseline at week 24. Key secondary endpoints were absolute change in total symptom score (TSS) and TSS50 response (≥50% reduction in TSS from baseline at week 24). The primary endpoint was met in 65.9% of patients randomized to pelabresib–ruxolitinib (n = 214) versus 35.2% to placebo–ruxolitinib (n = 216) (difference, 30.4%; 95% confidence interval (CI), 21.6, 39.3; P < 0.001). Absolute change in TSS was −15.99 versus −14.05 (difference, −1.94; 95% CI, −3.92, 0.04; P = 0.0545) and TSS50 was achieved in 52.3% versus 46.3% (difference, 6.0%; 95 CI, −3.5, 15.5) with pelabresib–ruxolitinib versus placebo–ruxolitinib. Exploratory analyses of proinflammatory cytokine amounts and bone marrow morphology showed greater improvement with the combination. Thrombocytopenia and anemia were the most common treatment-emergent adverse events, occurring in 52.8% (13.2% grade ≥3) versus 37.4% (6.1% grade ≥3) and 44.8% (23.1% grade ≥3) versus 55.1% (36.5% grade ≥3), respectively. Pelabresib in combination with ruxolitinib is well tolerated, improves signs of underlying myelofibrosis pathobiology and provides substantial clinical benefit over standard-of-care JAK inhibitor monotherapy. ClinicalTrials.gov identifier: NCT04603495.
Similar content being viewed by others

Main
Myelofibrosis is a myeloproliferative neoplasm that manifests as aberrant activation of the JAK–STAT signaling pathway, often driven by mutations in JAK2, CALR or MPL1. Cardinal clinical features of myelofibrosis include hepatosplenomegaly, anemia, weight loss, bone pain and myelofibrosis-associated symptoms such as night sweats and fatigue2. Key histopathological features include bone marrow reticulin fibrosis and osteosclerosis, and megakaryocyte proliferation, atypia and tight clustering3,4. JAK inhibitor monotherapy is the standard of care for myelofibrosis in patients with splenomegaly and/or symptoms1,5. However, JAK inhibitors do not consistently resolve pathobiological features, such as molecular markers of clonal burden and disrupted bone marrow morphology, particularly with short-term treatment6,7,8. Therefore, an unmet medical need persists due to limited depth and durability of clinical response, and frequency of treatment-emergent adverse events (TEAEs) with JAK inhibitor monotherapy9.
Aberrant increases in levels of proinflammatory cytokines are a hallmark of myelofibrosis pathogenesis2,10. Such cytokines have a fundamental role in disease establishment and progression, contribute to the constitutional symptom profile of patients and are prognostic of outcomes2,10,11,12. The tumor necrosis factor (TNF)–nuclear factor-κB (NF-κB) signaling network promotes proinflammatory cytokine production in myelofibrosis, with the BET protein BRD4 having a key role in regulating NF-κB-mediated inflammation13,14. In an adoptive transfer mouse model of myelofibrosis, BET inhibition (using the prototypical BET inhibitor JQ1) demonstrated reductions in spleen size, bone marrow fibrosis, proinflammatory cytokine amounts and NF-κB activation, and significantly prolonged survival compared with a vehicle control13. In the same model, BET inhibition with JQ1 in combination with JAK inhibition (using ruxolitinib) demonstrated greater reductions in these parameters than achieved by either drug alone13. These preclinical observations support simultaneous BET and JAK inhibition as a potent therapeutic strategy to exceed the effects of JAK inhibitor monotherapy, and provide a strong rationale to evaluate this approach in patients15.
Pelabresib (CPI-0610) is an investigational, oral, small molecule BET inhibitor under evaluation in clinical trials for patients with myelofibrosis15,16. Data from the phase 2 MANIFEST study (NCT02158858) demonstrated substantial and durable improvements in splenomegaly and symptoms with pelabresib plus ruxolitinib in JAK inhibitor-naive patients with myelofibrosis (n = 84): a reduction in spleen volume of ≥35% was observed in 68% of patients; a ≥50% reduction in symptoms at week 24 was observed in 56% of patients and the combination was generally well tolerated17,18.
Here, we report the primary analysis of the randomized phase 3 MANIFEST-2 study (NCT04603495), evaluating the efficacy and safety of pelabresib–ruxolitinib versus placebo–ruxolitinib in JAK inhibitor-naive patients with myelofibrosis19.
Results
Study design
MANIFEST-2 is a global, phase 3, randomized, double-blind active-control study of pelabresib–ruxolitinib versus placebo–ruxolitinib in JAK inhibitor-naive patients with myelofibrosis (Extended Data Fig. 1). Key eligibility criteria included confirmed diagnosis of myelofibrosis (primary myelofibrosis, postpolycythemia vera myelofibrosis or postessential thrombocythemia myelofibrosis); JAK inhibitor treatment-naive; dynamic international prognostic scoring system (DIPSS) score ≥Int-1; platelet count ≥100 × 109 l−1; spleen volume ≥450 cm3 by magnetic resonance imaging (MRI) or computed tomography (CT); at least two symptoms measurable (score ≥3) or a total symptom score (TSS) of ≥10 using the Myelofibrosis Symptom Assessment Form (MFSAF) v.4.0; peripheral blast count <5%, Eastern Cooperative Oncology Group (ECOG) performance status ≤ 2. The primary endpoint was splenic response at week 24. Key secondary endpoints were absolute change in TSS at week 24 compared with baseline and ≥50% decrease from baseline in TSS response at week 24 (TSS50). Other prespecified secondary endpoints were: percent change in TSS at week 24 compared with baseline; improvement in bone marrow fibrosis by at least one grade at week 24 compared with baseline; splenic response at week 48; TSS50 response at week 48; absolute change in TSS at week 48 compared with baseline; rate of red blood cell (RBC) transfusion over the first 24 weeks of treatment; conversion from RBC transfusion dependence at baseline to independence; categorical change of Patient Global Impression of Change (PGIC) at week 24 compared with baseline; progression-free survival; overall survival; safety (adverse events of all grades and serious adverse events); proportion of patients with transformation to blast phase; pharmacokinetics; descriptive assessment of ruxolitinib plasma concentrations in the presence or absence of pelabresib; duration of splenic response; modified TSS response at week 24 and duration of TSS50 response.
Patients
Between November 2020 and March 2023, 430 patients were enrolled in the MANIFEST-2 study (first patient enrolled, 23 April 2021; last patient enrolled, 2 March 2023) and randomized; 214 to pelabresib plus ruxolitinib and 216 to placebo plus ruxolitinib. At the data cutoff (31 August 2023), two patients in each arm had not received study treatment; 58 patients in the pelabresib–ruxolitinib arm and 54 patients in the placebo–ruxolitinib arm had discontinued study treatment (patient disposition shown in Fig. 1). The median duration on study was 45.5 weeks; 154 patients (72.0%) receiving pelabresib–ruxolitinib and 160 patients (74.1%) receiving placebo–ruxolitinib were continuing treatment. Baseline characteristics in each treatment arm are shown in Table 1.

The study opened for enrollment in November 2020; the first patient received their initial treatment on 22 April 2021, and the last patient was enrolled on 2 March 2023. Percentages reported are based on the number of patients randomized (intent-to-treat set). aOther (noncompliance/protocol violation (n = 2 in each arm) or withdrawal of consent (n = 11 in the pelabresib–ruxolitinib arm, and n = 4 in the placebo–ruxolitinib arm)). bTreatment ongoing as of 31 August 2023.
In the pelabresib–ruxolitinib arm, mean (s.d.) daily pelabresib dose in treated patients (N = 212) was 108.4 mg (27.6) and daily ruxolitinib dose was 30.5 mg (16.9). In the placebo–ruxolitinib arm (N = 214), mean (s.d.) ruxolitinib dose was 29.8 mg (12.9).
Efficacy: spleen volume reduction
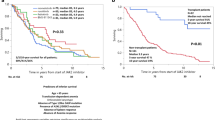
The primary endpoint of reduction in spleen volume of ≥35% at week 24 was observed in a statistically significantly larger proportion of patients in the pelabresib–ruxolitinib arm than in the placebo–ruxolitinib arm; 65.9% versus 35.2%, respectively (Cochran–Mantel–Haenszel difference, 30.4%; 95% CI, 21.6, 39.3; P < 0.001) (Fig. 2a). Mean percentage change in spleen volume at week 24 was −50.6% (95% CI, −53.2, −48.0) in the pelabresib–ruxolitinib arm versus −30.6% (95% CI, −33.7, −27.5) in the placebo–ruxolitinib arm. Spleen volume response rate at week 24 was consistently higher with pelabresib–ruxolitinib across predefined subgroups (Extended Data Fig. 2a). Spleen volume reduction of ≥35% at any time was observed in 172 patients (80%) treated with pelabresib–ruxolitinib and in 108 (50%) treated with placebo–ruxolitinib. Time to splenic response is shown in Fig. 2b. Duration of splenic response is shown in Extended Data Fig. 3a.

a, Percentage change in spleen volume from baseline at week 24, overlaid with the proportion of patients with spleen response (defined as a ≥35% reduction in spleen volume from baseline, by central read). Patients without week 24 change from baseline assessment are not shown and were considered nonresponders for spleen response. Difference between treatment arms was compared by stratified Cochran–Mantel–Haenszel test (performed two-sided Cochran–Mantel–Haenszel test at the alpha level 5%). The exact P value is 1.64 × 10−10. b, Kaplan–Meier time-to-event estimate for spleen response.
Efficacy: patient-reported outcomes
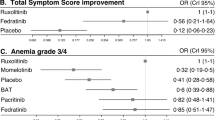
The key secondary endpoint of absolute change in TSS at week 24 demonstrated substantial improvements for patients in both treatment arms, with a trend toward greater benefit with pelabresib–ruxolitinib versus placebo–ruxolitinib. Least squares mean change from baseline at week 24 was −15.99 versus −14.05, respectively (difference, −1.94; 95% CI, −3.92, 0.04; P = 0.0545) (Fig. 3a). The proportion of patients with ≥50% reduction in TSS at week 24 (TSS50; key secondary endpoint) was greater in the pelabresib–ruxolitinib arm, with 52.3% versus 46.3%, respectively (Cochran–Mantel–Haenszel difference, 6.0%; 95% CI, −3.5, 15.5) (Fig. 3b and see Extended Data Fig. 3b for duration of TSS50 response). Reductions were consistent across symptom score domains (Extended Data Table 1). Mean percentage change in TSS from baseline at week 24 was −50.3% (95% CI, −56.6, −44.0) in the pelabresib–ruxolitinib arm versus −45.9% (95% CI, −51.8, −40.0) in the placebo–ruxolitinib arm. Similar trends in symptom scores were observed across predefined subgroups, except for the small subgroup of patients with high-risk (DIPSS) myelofibrosis at baseline (Extended Data Fig. 2b,c). Regarding the self-reported PGIC, 46.9% of patients in the pelabresib–ruxolitinib arm reported their condition as ‘much improved‘ or ‘very much improved’ compared with 50.0% in the placebo–ruxolitinib arm (no statistical comparison performed) (Extended Data Table 2). There was more than a twofold difference in patients achieving both spleen and TSS50 responses at week 24 with pelabresib–ruxolitinib compared with placebo–ruxolitinib (40.2% versus 18.5%) (Extended Data Fig. 4).

a, Absolute change in TSS score from baseline at week 24; patients without week 24 data are not shown. Change from baseline was determined by ANCOVA model using multiple imputation. Least square mean difference was determined from the ANCOVA model using baseline DIPSS, baseline platelet count and baseline spleen volume as factors and baseline TSS as covariate, performed two-sided Cochran–Mantel–Haenszel test at the alpha level 5%. b, Percentage change in TSS score from baseline at week 24, overlaid with the proportion of patients experiencing a TSS50 response. Patients without baseline and week 24 data are not shown. Difference between treatment arms was compared by stratified Cochran–Mantel–Haenszel test (performed two-sided Cochran–Mantel–Haenszel test at the alpha level 5%; weighted 95% CI adjusted across strata).
Efficacy: hemoglobin and transfusions
A numerically greater proportion of patients achieved hemoglobin (Hg) response with pelabresib–ruxolitinib compared with placebo–ruxolitinib, with a persistent difference in hemoglobin over time between treatment arms (Fig. 4). In patients with anemia (Hg <10 g dl−1) at baseline, hemoglobin concentrations were modestly and consistently higher across weeks 2–24 in the pelabresib–ruxolitinib arm versus the placebo–ruxolitinib arm. Transfusions were received during the first 24 weeks on treatment by 27.6% of patients treated with pelabresib–ruxolitinib and 37.5% with placebo–ruxolitinib.

Graph shows the mean change in hemoglobin over time in the overall study population and in the subgroup of patients with anemia (defined as patients with a baseline hemoglobin of <10 g dl−1). Hemoglobin response is defined as a mean increase in hemoglobin from baseline of ≥1.5 g dl−1 in the absence of transfusions during the previous 12 weeks (baseline hemoglobin defined as the last assessment before or on cycle 1 day 1, regardless of blood transfusions). Patients who received transfusions are included in these data. Data are presented as mean ± 95% CI. In accordance with preplanned hierarchical statistical testing, for these data, we report descriptive statistical analyses only.
Disease-relevant proinflammatory cytokines
Changes in proinflammatory cytokines, including NF-κB-regulated cytokines, TNF, interleukin-6 (IL-6), and IL-8 are shown in Extended Data Fig. 5a. Amounts of the NF-κB-regulated cytokines TNF and IL-6 decreased in both treatment arms, with a greater magnitude of reduction observed with pelabresib–ruxolitinib compared with placebo–ruxolitinib. Concentrations of IL-8 decreased in the pelabresib–ruxolitinib arm but increased in the placebo–ruxolitinib arm. Independent of treatment, lower amounts of proinflammatory cytokines were correlated with spleen responses (Extended Data Fig. 6).
Bone marrow morphology
Bone marrow samples were assessed for fibrosis, megakaryocytic density and proliferation, and erythropoiesis. At week 24, 192 patients treated with pelabresib–ruxolitinib and 188 patients treated with placebo–ruxolitinib were evaluable for change from baseline in bone marrow fibrosis. Among them, 98 out of 192 (51.0%) and 105 out of 188 (55.9%) patients, respectively, had missing data. Improvement of at least one grade was observed in 18.8% (36 out of 192) of patients treated with pelabresib–ruxolitinib and in 11.2% (21 out of 188) of patiients treated with placebo–ruxolitinib (Extended Data Fig. 5b). Considering only patients with results available at baseline and week 24, improvement of at least one grade was observed in 38.3% (36 out of 94) and 25.3% (21 out of 83) of patients, respectively. There was a greater reduction in density of reticulin fiber (−5.2 (95% CI, −6.9, −3.5) versus −1.0 (95% CI, −2.7, 0.6)) and CD61+ megakaryocytes (−54.5 cells mm−2 (95% CI, −70.8, −38.3) versus −27.4 cells mm−2 (95% CI, −43.0, −11.9)) in the pelabresib–ruxolitinib arm versus placebo–ruxolitinib, respectively (Extended Data Fig. 5c,d and Supplementary Fig. 1). Erythrocyte progenitor cell proportions increased by 11.4% (95% CI, −2.4, 27.2) from baseline at week 24 with pelabresib–ruxolitinib, and decreased by −9.8% (95% CI, −20.6, 2.6) with placebo–ruxolitinib. A greater increase in the proportion of erythrocyte progenitor cells was observed in patients who did not require RBC transfusions compared with patients who did require transfusions (Extended Data Fig. 5e).
Mutational analyses
At baseline, the pattern of driver and high-molecular-risk mutations was broadly comparable between arms, with the exception of higher frequency of ASXL1 and EZH2 in the placebo–ruxolitinib arm (Table 1). Nevertheless, treatment responses with pelabresib–ruxolitinib were independent of driver and high-molecular-risk mutation status (Extended Data Fig. 7). At week 48, a total of 83 of 247 (33.6%) patients with a JAK2 V617F mutation were included in the variant allele fraction (VAF) analysis. There was an early trend towards greater reduction in the JAK2 V617F VAF with pelabresib–ruxolitinib (n = 46; −23.9%), compared with placebo–ruxolitinib (n = 37; −16.8%) (difference, −9.5%; 95% CI, −23.6, 2.9; Supplementary Fig. 2a). Independent of treatment, patients with a spleen response at week 24 (n = 55) had a greater reduction from baseline in the JAK2 V617F VAF compared with nonresponders (n = 28) (Supplementary Fig. 2b).
Safety
In total, 212 patients in the pelabresib–ruxolitinib arm and 214 in the placebo–ruxolitinib arm received treatment and were included in safety analyses. At least one TEAE was experienced by 96.7% (205 out of 212) of patients in the pelabresib–ruxolitinib arm versus 96.7% (207 out of 214) of patients in the placebo–ruxolitinib arm. Most TEAEs were considered related to pelabresib or placebo treatment (77.4% (n = 164 out of 212) versus 74.8% (n = 160 out of 214), respectively) (Extended Data Table 3). The overall frequency of any grade ≥3 TEAEs was lower with pelabresib–ruxolitinib (49.1%) than with placebo–ruxolitinib (57.0%). Mean (s.d.) time to onset for any grade TEAEs was 23 days (45.6) in the pelabresib–ruxolitinib arm and 27 days (45.6) in the placebo–ruxolitinib arm. Time to onset for grade ≥3 was 98 days (123.7) versus 113 days (130.8), respectively.
The most frequent (≥10%) hematological TEAEs (Table 2) in the pelabresib–ruxolitinib arm were thrombocytopenia (composite including preferred terms of thrombocytopenia and platelet count decrease, 52.8% any grade; 13.2% grade ≥3) and anemia (composite including preferred terms of anemia and hemoglobin decrease; 44.8% any grade; 23.1% grade ≥3). In the placebo–ruxolitinib arm, the most frequent (≥10%) hematological TEAEs were anemia (composite term, 55.1%; 36.5% grade ≥3) and thrombocytopenia (composite term, 37.4%; 6.1% grade ≥3).
Cytopenias were managed mostly with dose reduction or interruption, according to guidance provided in the protocol. There were no clinically significant bleeding events associated with grade ≥3 thrombocytopenia. Four patients in the pelabresib–ruxolitinib arm and two patients in the placebo–ruxolitinib arm discontinued treatment due to thrombocytopenia or platelet count decrease, and one patient in each arm discontinued due to anemia or hemoglobin decrease.
Among the nonhematological TEAEs occurring in ≥10% of patients (listed in Table 2), the most frequent were diarrhea in the pelabresib–ruxolitinib arm (23.1%; 0.5% grade ≥3) and constipation in the placebo–ruxolitinib arm (24.3%; 0 grade ≥3). Dysgeusia occurred in 18.4% (0.5% grade ≥3) and 3.7% (0% grade ≥3) of patients in the pelabresib–ruxolitinib and placebo–ruxolitinib arms, respectively (Table 2). The single event of grade ≥3 dysgeusia in the pelabresib–ruxolitinib arm was considered a nonserious event, related to pelabresib; the event was managed by treatment interruption.
TEAEs leading to dose reduction of ruxolitinib, pelabresib or placebo occurred in 51.9% and 44.9% of patients in the pelabresib–ruxolitinib and placebo–ruxolitinib arms, respectively. The most frequent TEAEs resulting in dose reduction were thrombocytopenia (23.1% and 15.0%, respectively), platelet count decrease (17.0% and 13.1%, respectively) and anemia (10.4% and 16.4%, respectively). TEAEs leading to ruxolitinib, pelabresib or placebo dose interruptions occurred in 32.5% and 24.8% in the pelabresib–ruxolitinib and placebo–ruxolitinib arms, respectively. The most frequent TEAEs resulting in dose interruption were thrombocytopenia (6.6% and 4.7%, respectively), COVID-19 (0.9% and 4.2%, respectively), platelet count decrease (3.3% and 1.4%, respectively) and anemia (2.4% and 2.3%, respectively). TEAEs leading to withdrawal of pelabresib or placebo occurred in 12.3% and 7.5% of patients in the pelabresib–ruxolitinib and placebo–ruxolitinib arms, respectively (Supplementary Table 1). TEAEs leading to withdrawal of ruxolitinib occurred in 9.9% of patients in the pelabresib–ruxolitinib arm and in 6.1% of patients in the placebo–ruxolitinib arm. Serious TEAEs occurred in 29.7% of patients in the pelabresib–ruxolitinib arm and 29.4% in the placebo–ruxolitinib arm. The most frequent (≥2%) serious adverse events were pneumonia (3.3% of patients in the pelabresib–ruxolitinib arm and 2.8% of patients in the placebo–ruxolitinib arm) and anemia (2.4% and 2.3%, respectively). There were 11 deaths during treatment (5 in the pelabresib–ruxolitinib arm and 6 in the placebo–ruxolitinib arm). In the pelabresib–ruxolitinib arm, fatal events of pneumonia, sepsis, cardiac arrest, intracranial hemorrhage (attributed to underlying hypertension, considered unrelated to study treatment) and septic shock (co-recorded as a fatal event with pneumonia) were each reported in one patient, except cardiac arrest, which was reported in two patients. In the placebo–ruxolitinib arm, fatal events of pneumonia, sepsis, cardiac failure, road traffic accident, small intestinal obstruction and sudden cardiac death were each reported in one patient. All deaths were assessed as not related to study treatment. One patient died of a road traffic accident and all other deaths had medical history that may have been considered a contributory factor, or were attributable to concurrent disease.
Disease progression to accelerated phase or transformation to blast phase occurred in 3.3% of patients (7 out of 212) receiving pelabresib–ruxolitinib versus 2.3% (5 out of 214) receiving placebo–ruxolitinib. This assessment was based on local laboratory results, adverse events and documented disease progression. A numerical imbalance was observed in the number of patients with blast phase based on reported disease progression, with 2.4% (5 out of 212) versus 0.5% (1 out of 214) of patients in the pelabresib–ruxolitinib versus placebo–ruxolitinib arms, respectively. One of the five patients treated with pelabresib–ruxolitinib with blast phase according to this assessment was ultimately diagnosed with lymphoproliferative neoplasm and not blast phase transformation of myelofibrosis.
Discussion
The MANIFEST-2 study of pelabresib–ruxolitinib in JAK inhibitor-naive patients with myelofibrosis met its primary endpoint, with 65.9% of patients experiencing spleen response (≥35% volume reduction) at week 24 with the combination. Indeed, the spleen response rate in patients treated with pelabresib–ruxolitinib was approximately double that seen with placebo–ruxolitinib in the MANIFEST-2 study (35.2%; P < 0.001), and in previous studies of JAK inhibitor monotherapy (ranging from 18% to 42%)20,21,22,23,24. Furthermore, symptom improvements were also observed with placebo–ruxolitinib and pelabresib–ruxolitinib, with trends towards further benefit with the combination.
These clinical observations are consistent with the proposed mechanism of action of combined BET and JAK inhibition, and with our understanding of proinflammatory cytokine involvement in myelofibrosis pathogenesis. In line with preclinical findings13, combined BET and JAK inhibition with pelabresib–ruxolitinib treatment in the MANIFEST-2 study led to stronger and more frequent improvements in proinflammatory cytokine amounts than JAK inhibition alone with ruxolitinib. These include NF-κB-regulated cytokines, TNF, IL-6 and IL-8, which have a key role in myelofibrosis pathogenesis and are associated with a detrimental prognosis11,12. IL-8, in particular, has been associated with reduced overall survival11,12; in this study, amounts of IL-8 increased in the placebo–ruxolitinib arm. Consistent with proinflammatory cytokines analysis, improvements in fibrosis and overall bone marrow morphology were also observed to a greater degree in the pelabresib–ruxolitinib arm than in the ruxolitinib–placebo arm. Collectively, these exploratory data indicate a biological benefit of the pelabresib–ruxolitinib combination versus ruxolitinib monotherapy, which supports the clinical benefits.
We observed increased erythrocyte progenitor proportions in the pelabresib–ruxolitinib arm, beyond those observed in the placebo–ruxolitinib arm, which may explain the amelioration of anemia with pelabresib–ruxolitinib25. Reduced transfusions associated with anemia improvements are likely to have a direct benefit on the clinical and economic burden of myelofibrosis26. The clinically and biologically meaningful benefits of the pelabresib–ruxolitinib combination represent valuable short-term outcomes for patients, which may translate into more profound longer-term treatment effects than ruxolitinib monotherapy. A survival benefit would further demonstrate pelabresib–ruxolitinib as a clinically meaningful therapeutic option. Spleen volume reduction and spleen length reduction observed with ruxolitinib treatment have both correlated with an overall survival benefit in patients with myelofibrosis20,27. Durability of response, survival and correlation with clinical outcomes will be further evaluated with ongoing, long-term follow-up of this study.
Similar to the phase 2 MANIFEST study17, safety analyses in the phase 3 MANIFEST-2 study suggest that combining pelabresib with ruxolitinib improves clinical response28, with overall fewer grade 3 or higher adverse events reported with the combination. A higher incidence of thrombocytopenia events was reported for the combination arm versus placebo–ruxolitinib; however, these were well managed with dose modifications, with only one patient in each arm discontinuing study treatment due to thrombocytopenia. Dosing of ruxolitinib was equivalent between the two arms, indicating that dose intensity was unaffected by combining with pelabresib. Constipation adverse events in both treatment arms were reported at higher incidence than observed with ruxolitinib monotherapy in the COMFORT-I (12.9%) and COMFORT-II (12 out of 146 patients) trials, or with other JAK inhibitors (momelotinib pooled analysis, 11.2%)6,20,29. Here, most constipation adverse events were grade 1 or 2, similar to the pelabresib–ruxolitinib cohort of the MANIFEST trial (25%) in which the combination treatment was considered well tolerated17, and less than half in both arms were considered related to pelabresib or placebo. Rates of leukemic transformation were within a similar range to those reported in COMFORT-I (2 out of 155 patients receiving ruxolitinib monotherapy), COMFORT-II (8 out of 146 patients receiving ruxolitinib monotherapy) and SIMPLIFY-I (2 out of 216 patients receiving ruxolitinib monotherapy and 1 out of 214 patients receiving momelotinib monotherapy)6,20,23. Disease transformation observations from the MANIFEST-2 study warrant further biologic evaluation, continued clinical monitoring and additional follow-up.
Although the primary endpoint of spleen volume reduction represents a valuable short-term clinical benefit, one limitation of this study is that we have not yet reported long-term durability of response data. At data cutoff for this primary analysis, long-term durability of response data were not mature. Durability of response and survival data will be investigated in a long-term follow-up of this study. A second limitation is the potential subjectivity and sensitivity restrictions of the MFSAF for assessment of symptoms. However, this instrument captures the broad spectrum of symptoms of myelofibrosis and has been comprehensively validated, which has led to its use in clinical trials for myeloproliferative neoplasm patients30.
In conclusion, pelabresib plus ruxolitinib provided robust clinical benefit, resulting in a statistically significant improvement in the primary endpoint of spleen response, with trends of improvement noted across other principal hallmarks of myelofibrosis, including symptom control, proinflammatory cytokine amounts and bone marrow morphology. The phase 3 MANIFEST-2 study provides important insights into disease biology and modification, supporting the combination of pelabresib plus ruxolitinib for JAK inhibitor-naive patients with myelofibrosis.
Methods
Patients
Eligible adult patients had myelofibrosis (primary, postpolycythemia vera or postessential thrombocythemia) and a spleen volume of ≥450 cm3 by MRI or CT scan, ≥2 symptoms with an average score of ≥3 or an average TSS ≥ 10 over the 7-day period before randomization using MFSAF v.4.0, and a prognostic risk-factor score of intermediate-1 or higher per DIPSS25. Additional inclusion criteria were a platelet count of ≥100 × 109 l−1 in the absence of growth factors or transfusions for the previous 4 weeks, an ECOG performance status of ≤2 and peripheral blast count <5%. Patients were excluded if they had a previous splenectomy, splenic irradiation within 6 months of treatment initiation, received previous treatment with any JAK or BET inhibitors, or were currently candidates for allogeneic hematopoietic stem cell transplant. In this study, a patient’s sex refers to biological attribute; gender was not reported, as there is no analysis related to gender identity.
Study design
In this double-blind active-control study, patients were randomized 1:1 to pelabresib plus ruxolitinib or placebo plus ruxolitinib (Extended Data Fig. 1), by a centralized interactive voice response/interactive web response system. Stratification was based on DIPSS category (intermediate-1 versus intermediate-2 versus high-risk), platelet count (>200 × 109 l−1 versus 100 × 109 –200 × 109 l−1) and spleen volume (≥1,800 cm3 versus <1,800 cm3). Patients randomized to placebo–ruxolitinib could cross over to pelabresib–ruxolitinib if progressive splenomegaly occurred at or after week 24 (defined as enlargement of spleen volume by ≥25% from baseline). All patients, investigators and the sponsor were blinded to treatment allocation with study drugs packaged identically. The study was conducted at sites across North America, Asia, Europe and Australia (Supplementary Table 2).
Treatment
Pelabresib or matching placebo was administered orally at a starting dose of 125 mg orally once daily for 14 consecutive days, followed by a 7-day break (21-day cycle). Pelabresib or placebo dose could be increased for lack of spleen response after four cycles in 25 mg increments, up to 175 mg once daily. Ruxolitinib was administered orally at an initial dose of either 10 mg or 15 mg twice daily depending on baseline platelet counts (5 mg twice daily lower than the approved dose), with a mandatory 5 mg per dose increase after one cycle if prespecified criteria were met. Ruxolitinib dose could be further increased for lack of spleen response by 5 mg per dose increments, up to 25 mg twice daily, provided adequate blood counts. To manage adverse events, both treatments could be dose reduced to a minimum of 50 mg once daily for pelabresib–placebo and 5 mg once daily for ruxolitinib.
Endpoints
The primary endpoint was spleen response, defined as a reduction of ≥35% in spleen volume from baseline at week 24 by independent central review. Spleen volume was measured using MRI or CT, performed during screening and every 12 weeks from the first day of treatment, with MRI being the preferred method.
Key secondary endpoints were (1) absolute change in TSS from baseline, and (2) TSS50, defined as reduction of ≥50% from baseline in TSS; both at week 24 using MFSAF v.4.0. MFSAF was completed electronically daily until 12 weeks after end of treatment.
Other secondary endpoints included percentage change in TSS at week 24, duration of spleen response, improvement in bone marrow fibrosis by at least one grade from baseline at week 24, rate of transfusions over the first 24 weeks of treatment, category change of PGIC at week 24 from baseline using a single question completed weekly until 12 weeks after end of treatment, rate of transformation to blast phase (acute myeloid leukemia) and safety (adverse events, regardless of attribution, were assessed according to National Cancer Institute Common Terminology Criteria for Adverse Events v.5.0).
Exploratory endpoints included percentage change in spleen volume at week 24, hemoglobin response (≥1.5 g dl−1 mean increase in hemoglobin from baseline in the absence of transfusions during the previous 12 weeks), time to spleen response, assessment of myelofibrosis-related features associated with response (including bone marrow morphology and hematopoietic cell populations), changes in proinflammatory cytokines (measured by a bead-based multiplex assay from plasma obtained pretreatment at baseline and at week 24) and molecular response.
Bone marrow biopsy assessment
Bone marrow biopsy was performed at baseline and every 24 weeks on treatment (reduced to every 48 weeks after week 72), and assessed by a local hematopathologist for fibrosis grading according to the European classification26. Disease progression to accelerated phase was defined as at least two consecutive peripheral blast counts of 10–19% or a bone marrow myeloblast of 10–19%. Transformation to blast phase was defined as a bone marrow blast count of ≥20% or a peripheral blood blast count of ≥20% associated with an absolute blast count of ≥1 × 109 l−1 that persists for at least 2 weeks. Three stained slides used for local review and six to ten unstained slides were provided for central pathology review and exploratory analyses. Central bone marrow immunohistochemistry staining was conducted for reticulin fiber density, CD61+ megakaryocytes, and CD71+ erythrocyte progenitor cells. Digital images were analyzed by an automated quantitative cell-specific detection analysis.
Mutant allele burden evaluation
Mutational analyses were conducted centrally from peripheral whole blood samples at baseline and at week 48 by targeted next-generation sequencing with the Rapid Heme Panel v.3 assay.
Statistical analysis
For the primary and key secondary endpoint of TSS50, response rates were compared using the Cochran–Mantel–Haenszel test controlling for baseline prognostic score (DIPSS Int-1, Int-2, High), platelet count (100–200 × 109 l−1 versus >200 × 109 l−1) and spleen volume (<1,800 cm3 versus ≥1,800 cm3). An analysis of covariance (ANCOVA) model was used to analyze the continuous key secondary endpoint of absolute change in TSS, controlling for baseline prognostic score (DIPSS Int-1, Int-2, High), platelet count (100–200 × 109 l−1 versus >200 × 109 l−1) and spleen volume (<1,800 cm3 versus ≥1,800 cm3) and baseline TSS. SAS v.9.4 was used to assess the impact of missing data. Hypothesis tests were performed sequentially: primary endpoint of spleen response; key secondary endpoint of absolute change in TSS; key secondary endpoint of TSS50. Formal testing for statistical significance was halted if the P value was greater than 0.05 for a given endpoint. Descriptive statistics are used to report other secondary endpoints and exploratory analyses.
Assuming respective spleen/TSS50 response rates of 62%/57% with pelabresib–ruxolitinib and 29%/42.2% with placebo–ruxolitinib20,27, a sample size of approximately 400 patients (200 in each treatment arm) was estimated to provide over 99% power for testing the primary endpoint and 81% power for the key secondary endpoint of TSS50 using the two-group continuity corrected χ2 test, with a 5% two-sided significance level and accounting for 2% nonevaluable patients. The sample size provided 90% power to test the key secondary endpoint of absolute change in TSS, assuming a treatment difference of 4 points based on reported median percentage changes. Mixed models for repeated measures were used to estimate the percentage change from baseline in proinflammatory cytokines, reticulin fiber density, erythrocyte progenitor cell proportions and JAK2 V617F VAF. A mixed model for repeated measure controlling for treatment was used to estimate the relative concentrations in proinflammatory cytokines according to spleen response (≥35% reduction in spleen volume).
Continuous variables were summarized with descriptive statistics and categorical variables were summarized by numbers and percentages of patients, with two-sided 95% CIs as appropriate. The primary analysis took place after all randomized patients completed their week 24 visit or prematurely discontinued.
Study oversight
The study protocol can be found at https://cdn.clinicaltrials.gov/large-docs/95/NCT04603495/Prot_000.pdf. The date of preregistration was 10 October 2020. See Supplementary Table 3 for a list of protocol amendments. The MANIFEST-2 study was sponsored by Constellation Pharmaceuticals, a Novartis Company (formally part of MorphoSys). The study was approved by the institutional review board or independent ethics committee at each participating center and conducted in accordance with the International Council for Harmonisation E6 Guideline for Good Clinical Practice, which originates from the Declaration of Helsinki. All patients provided written informed consent. Patients did not receive compensation for their participation in the study. Data were analyzed and interpreted by the sponsors in collaboration with the authors. The first and senior authors prepared the first draft of the manuscript with assistance from a medical writer employed by Syneos Health, and funded by MorphoSys, a Novartis Company. All authors reviewed the manuscript and confirmed the accuracy and completeness of the data.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Novartis is committed to sharing with qualified external researchers, access to patient-level data and supporting clinical documents from eligible studies. These requests are reviewed and approved by an independent review panel on the basis of scientific merit. All data provided is anonymized to respect the privacy of patients who have participated in the trial in line with applicable laws and regulations. This trial data availability is according to the criteria and process described on https://www.clinicalstudydatarequest.com/.
References
Yacoub, A., Twardowski, N., Britt, A. & Shraim, N. SOHO state of the art updates and next questions | early intervention in myelofibrosis: where are we and does it matter? Clin. Lymphoma Myeloma Leuk. 24, 506–511 (2024).
Tefferi, A. Primary myelofibrosis: 2023 update on diagnosis, risk‐stratification, and management. Am. J. Hematol. 98, 801–821 (2023).
Arber, D. A. et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 127, 2391–2405 (2016).
Ng, Z. Y., Fuller, K. A., Mazza‐Parton, A. & Erber, W. N. Morphology of myeloproliferative neoplasms. Int. J. Lab. Hematol. 45, 59–70 (2023).
Bose, P. & Verstovsek, S. JAK inhibition for the treatment of myelofibrosis: limitations and future perspectives. Hemasphere 4, e424 (2020).
Harrison, C. N. et al. Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis. Leukemia 30, 1701–1707 (2016).
Deininger, M. et al. The effect of long-term ruxolitinib treatment on JAK2p.V617F allele burden in patients with myelofibrosis. Blood 126, 1551–1554 (2015).
Levavi, H., Hoffman, R. & Marcellino, B. K. JAK inhibitors in the treatment of myelofibrosis. Clin. Adv. Hematol. Oncol. 20, 456–467 (2022).
Vainchenker, W. et al. Recent advances in therapies for primary myelofibrosis. Fac. Rev. 12, 23 (2023).
Mondet, J., Hussein, K. & Mossuz, P. Circulating cytokine levels as markers of inflammation in Philadelphia negative myeloproliferative neoplasms: diagnostic and prognostic interest. Mediators Inflamm. 2015, 670580 (2015).
Tefferi, A. et al. Circulating interleukin (IL)-8, IL-2R, IL-12, and IL-15 levels are independently prognostic in primary myelofibrosis: a comprehensive cytokine profiling study. J. Clin. Oncol. 29, 1356–1363 (2011).
Dunbar, A. et al. CXCL8/CXCR2 signaling mediates bone marrow fibrosis and represents a therapeutic target in myelofibrosis. Blood 141, 2508–2519 (2023).
Kleppe, M. et al. Dual targeting of oncogenic activation and inflammatory signaling increases therapeutic efficacy in myeloproliferative neoplasms. Cancer Cell 33, 29–43.e7 (2018).
Brown, J. D. et al. NF-κB directs dynamic super enhancer formation in inflammation and atherogenesis. Mol. Cell 56, 219–231 (2014).
Mascarenhas, J., Gerds, A. & Verstovsek, S. Paradigm shift: combination BET and JAK inhibition in myelofibrosis. Leukemia 35, 3361–3363 (2021).
Albrecht, B. K. et al. Identification of a benzoisoxazoloazepine inhibitor (CPI-0610) of the bromodomain and extra-terminal (BET) family as a candidate for human clinical trials. J. Med. Chem. 59, 1330–1339 (2016).
Mascarenhas, J. et al. MANIFEST: pelabresib in combination with ruxolitinib for Janus kinase inhibitor treatment-naive myelofibrosis. J. Clin. Oncol. 41, 4993–5004 (2023).
Gupta, V. et al. Matching-adjusted indirect comparison of pelabresib/ruxolitinib combination vs JAKi monotherapy in myelofibrosis. Blood Adv. 7, 5421–5432 (2023).
Harrison, C. N. et al. Phase III MANIFEST-2: pelabresib + ruxolitinib vs placebo + ruxolitinib in JAK inhibitor treatment-naive myelofibrosis. Future Oncol. 18, 2987–2997 (2022).
Verstovsek, S. et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N. Engl. J. Med. 366, 799–807 (2012).
Harrison, C. et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N. Engl. J. Med. 366, 787–798 (2012).
Pardanani, A. et al. Safety and efficacy of fedratinib in patients with primary or secondary myelofibrosis: a randomized clinical trial. JAMA Oncol. 1, 643–651 (2015).
Mesa, R. A. et al. SIMPLIFY-1: a phase III randomized trial of momelotinib versus ruxolitinib in Janus kinase inhibitor–naïve patients with myelofibrosis. J. Clin. Oncol. 35, 3844–3850 (2017).
Mascarenhas, J. et al. Pacritinib vs best available therapy, including ruxolitinib, in patients with myelofibrosis. JAMA Oncol. 4, 652 (2018).
Passamonti, F. et al. Anemia in myelofibrosis: current and emerging treatment options. Crit. Rev. Oncol. Hematol. 180, 103862 (2022).
Gerds, A. T., Harrison, C., Thompson, S., Snopek, F. & Pemmaraju, N. The burden of illness and the incremental burden of transfusion dependence in myelofibrosis in the United States. Blood 140, 3974–3975 (2022).
Miller, C. B. et al. Practical measures of clinical benefit with ruxolitinib therapy: an exploratory analysis of COMFORT-I. Clin. Lymphoma Myeloma Leuk. 17, 479–487 (2017).
Verstovsek, S., Mesa, R. A., Livingston, R. A., Hu, W. & Mascarenhas, J. Ten years of treatment with ruxolitinib for myelofibrosis: a review of safety. J. Hematol. Oncol. 16, 82 (2023).
Verstovsek, S. et al. Momelotinib long-term safety and survival in myelofibrosis: integrated analysis of phase 3 randomized controlled trials. Blood Adv. 7, 3582–3591 (2023).
Daskalopoulou, C. et al. Myelofibrosis symptom assessment form total symptom score version 4.0: measurement properties from the MOMENTUM phase 3 study. Qual. Life Res. https://doi.org/10.1007/s11136-024-03855-1 (2024).
Acknowledgements
We thank all the patients and their families, trial site coordinators and members of the MANIFEST-2 study team. We also thank C. Davies and N. Griffiths of Syneos Health for medical writing support that was funded by MorphoSys US Inc., a Novartis Company, in accordance with Good Publication Practice guidelines (https://www.ismpp.org/gpp-2022). The development of pelabresib was funded in part by the Leukemia and Lymphoma Society. The MANIFEST-2 study was supported by Constellation Pharmaceuticals, a Novartis Company.
Author information
Authors and Affiliations
Contributions
M.H., S.-K.K., A.-M.J., Q.L., R.B., B.B. and J.M. contributed to the conception and/or design of the study and the development of the study protocol. R.K.R., S.G., D.C., E.A., P.B., A.T.G., A.M.V., F.P., S.-E.L., V.G., A.L., S.T.O., A.T.K., A.P., A.Á.-L., R.M., J.-J.K., M.T., J.M.S., D.L., C.N.H. and J.M. enrolled and treated patients. M.H., S.-K.K., A.-M.J., Q.L., R.B. and B.B. performed data/statistical analysis. All authors participated in data interpretation, manuscript writing and reviewing, and approved the final manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors report the following competing interests. R.K.R. has received grants from MorphoSys/Constellation, Ryvu, Stemline and Zentalis, consultation fees from GlaxoSmithKline, Incyte, AbbVie, BMS-Celgene, Novartis, Zentalis, Promedior, CTI, Blueprint, Stemline, Galectco, PharmEssentia, Disc Medicines, Sunimoto Dainippon, Servier, Karyopharm and Cogent Bio, honoraria fees from Karyopharm, Sunimoto Dainippon and Protagonist, participated on a Data Safety Monitoring Board or Advisory Board for Disc Medicines and Merck, and received advisory fees from the MPN Research Foundation. D.C. has received consultation fees from Janssen, honoraria fees from Astellas, Amgen, BMS, Janssen, AstraZeneca and AbbVie, and support for attending meetings and/or travel from Gilead Sciences, Ryvu Therapeutics and AbbVie. E.A. has received consulting/advisory board fees from Ascentage, BMS, GlaxoSmithKline, Incyte, MorphoSys/Novartis, Pfizer and Takeda. P.B. has received research support from MorphoSys to his institution for the conduct of this clinical trial, institutional grants from Incyte, BMS, CTI BioPharma (a Sobi company), MorphoSys, Kartos, Telios, Karyopharm, Sumitomo, Janssen, Geron, Ionis, Disc, Blueprint and Cogent; consultation fees from Incyte, BMS, CTI BioPharma (a Sobi company), GlaxoSmithKline, AbbVie, MorphoSys, Karyopharm, Sumitomo, PharmaEssentia, Morphic, Jubilant, Ionis, Disc, Blueprint, Cogent, Ono and Novartis; honoraria fees from Incyte, Sumitomo, GlaxoSmithKline, PharmaEssentia, AbbVie, CTI BioPharma (a Sobi company) and Novartis; holds a study steering committee membership with Blueprint, Geron and Karyopharm, a steering committee membership with Sumitomo, Keros, GlaxoSmithKline and Karyopharm and a leadership role in a scientific advisory board with PharmaEssentia; is an advisory board member for Raythera; and had received MD Anderson Cancer Center Support grant P30 CA016672 from the National Institutes of Health (National Cancer Institute). A.T.G. has received consulting fees from Novartis (MorphoSys), PharmaEssentia, GlaxoSmithKline (Sierra Oncology), Sobi (CTI Biopharma), AbbVie, Merck (Imago Biosciences), Kartos, Telios, BMS, Rain Oncology, Disc Medicine and Agios. A.M.V. has received honoraria fees from Incyte, Novartis, AbbVie, GlaxoSmithKline, BMS, MorphoSys and AOP, participated on a Data Safety Monitoring Board or Advisory Board from Incyte, Novartis, AOP, MorphoSys and Roche. F.P. has received consultation and honoraria fees from Novartis, Celgene, AOP, Sierra Oncology and CTI. S.-E.L. declares no personal or financial conflicts of interests related to this manuscript, has received consulting/advisory board fees from BMS, GSK, Novartis and PharmaEssentia, and received an institutional grant from PharmaEssentia. V.G. has received grants from AbbVie and Novartis, consultation fees from GlaxoSmithKline, Incyte, AbbVie, BMS-Celgene and Novartis, honoraria fees from GlaxoSmithKline, Novartis and AbbVie, support for attending meetings and/or travel from GlaxoSmithKline and participated on a Data Safety Monitoring Board or Advisory Board from BMS-Celgene, Incyte, Daichii-Sankyo, AbbVie, Novartis and GlaxoSmithKline. A.L. has received consulting fees from AOP and Sanofi, honoraria fees from Grifols, Incyte, Novartis, Amgen, Pfizer, BMS, Sanofi and SOBI, support for attending meetings and/or travel from Sanofi and BeiGene, and participated on a Data Safety Monitoring Board or Advisory Board for MorphoSys, Amgen, Protagonist, Grifols, SOBI, Novartis and Sanofi. S.T.O. has received consulting fees from Novartis, Kartos Therapeutics, Disc Medicine, Blueprint Medicines, AbbVie, Constellation/MorphoSys, CTI BioPharma, Bristol Myers Squibb, Geron, GlaxoSmithKline/Sierra Oncology, Cogent and Incyte. A.T.K. has received institutional grants from MorphoSys, Novartis, BMS, GlaxoSmithKline, Protagonist, Geron and Janssen, consultation fees from AbbVie, MorphoSys and Karyopharm, honoraria fees from PharmaEssentia, Incyte, BMS and CTI Biopharma, support for attending meetings and/or travel support from PharmaEssentia, and participated on a Data Safety Monitoring Board or Advisory Board with Incyte. A.P. has received consulting fees from Sanofi and Sobi, honoraria fees from Sobi, Sanofi, Pfizer, Incyte, Alexion, Takeda, Novartis and BMS, and support for attending meetings and/or travel from Alexion, Sobi and Sanofi. A.A.-L. received honoraria fees from AOP Health for participating in an advisory board and from Novartis and GSK for lectures. R.M. has received grants for research support from MorphoSys, CTI, BMS, Genentech, AbbVie, Incyte and GlaxoSmithKline, and consultation fees from MorphoSys, Incyte, BMS, Novartis, CTI and GlaxoSmithKline. J.-J.K. has received consultation fees from Novartis, AbbVie and GlaxoSmithKline, honoraria fees from Novartis, AOP Health and BMS, support for attending meetings and/or travel from Novartis, and participated on a Data Safety Monitoring Board or Advisory Board from Incyte. M.T. has received advisory board fees from Novartis and Sumitomo, and research funding from BMS. J.M.S. received institutional research support from Constellation/MorphoSys, advisory board fees from Constellation/MorphoSys, grants from AbbVie (for research support, research support to institution, advisory board), SDP Oncology (for research support, research support to institution, advisory board), Karyopharm (for research support to institution, advisory board), Morphic (for research support), PharmaEssentia (for research support to institution, advisory board) and Protagonist (for research support to institution, advisory board), and consultation fees from SDP Oncology, Morphic, PharmaEssentia and Calico. D.L. has received consultation fees from AbbVie, Takeda and Novartis, honoraria fees from AbbVie, Roche, Novartis and Takeda, support for attending meetings and/or travel from AbbVie and Roche, and participated on a Data Safety Monitoring Board or Advisory Board from AbbVie. M.H. is an employee of Constellation Pharmaceuticals, a Novartis Company. S.-K.K. is an employee of MorphoSys GmbH, Planegg, Germany, a Novartis Company. A.-M.J. is an employee of MorphoSys GmbH, Planegg, Germany, a Novartis Company. Q.L. is an employee of MorphoSys US Inc., Boston, MA, USA, a Novartis Company. R.B. is an employee of MorphoSys GmbH, Planegg, Germany, a Novartis Company. B.B. was an employee of Constellation Pharmaceuticals, Boston, MA, USA, a Novartis Company, and holds stock with Pfizer, Moderna, Eli Lily, Exelixis and Verastem. C.N.H. has received institutional grants from Constellation and Novartis, consultation fees from Novartis, MSD, Karyopharm, AOP, GlaxoSmithKline, BMS, Sobi, Galecto and CTI, honoraria fees from Novartis, MSD, Karyopharm, Sobi, GlaxoSmithKline and BMS, support for attending meetings and/or travel from Novartis, participated on a Data Safety Monitoring Board or Advisory Board for BMS and Galecto, leadership role with Blood Cancer UK (Trustee; unpaid), EHA (Deputy Editor-in-Chief remunerated) and MPN Voice (Medical Director; unpaid), and holds stock or stock options with Chakana Medical Limited. J.M. has received grants from Incyte, Novartis, Geron, BMS, AbbVie, CTI/SOBI, Karyopharm, Disc Medicines, Ajax, PharmaEssentia and Kartos, consultation fees from Incyte, CTI/SOBI, BMS, MorphoSys, GlaxoSmithKline, AbbVie, Novartis, Roche, Merck, Pfizer, Geron, Karyopharm, PharmaEssentia, Disc Medicines, Blueprint Medicines, Keros, Galecto and Sumitomo, support for attending meetings and/or travel from Kartos, and participated on a Data Safety Monitoring or Advisory Board with Galecto and Incyte. The remaining author(s) declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Simon Mendez-Ferrer and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Saheli Sadanand and Jean Nakhle, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 MANIFEST-2 study design.
*Patients enrolled in the placebo plus ruxolitinib arm could cross over to the pelabresib plus ruxolitinib arm if progressive splenomegaly occurred at or after 24 weeks of treatment (defined as enlargement of spleen volume by at least 25% compared with baseline); there were no crossovers as of 31 August 2023. †The starting dose for pelabresib was 125 mg QD and protocol-defined dose modifications based on AEs and treatment response allowed a dose range between 50 mg and 175 mg QD. ‡Ruxolitinib was started at 10 mg BID (baseline platelet count 100–200 × 109/L) or 15 mg BID (baseline platelet count >200 × 109/L) with a mandatory dose increase by 5 mg BID after one cycle and a maximum dose of 25 mg BID as per the label. AE, adverse event; BID, twice daily; CT, computed tomography; DIPSS, Dynamic International Prognostic Scoring System; ET, essential thrombocythemia; Int-1, Intermediate-1; Int-2, Intermediate-2; MRI, magnetic resonance imaging; MFSAF, Myelofibrosis Symptom Assessment Form; PV, polycythemia vera; QD, once daily; TSS, total symptom score; TSS50, ≥50% TSS reduction from baseline.
Extended Data Fig. 2 Spleen (central read) response and symptom score at week 24 according to pre-defined subgroups.
A) Shows spleen response (defined as ≥35% reduction in spleen volume), according to subgroups. (B) Shows the mean absolute change in TSS from baseline to week 24, according to subgroups. (C) Shows the TSS50 response rate at week 24, according to subgroups. Data are presented as mean value ± 95% CI. CI, confidence interval; DIPSS, Dynamic International Prognostic Scoring System; LS, least squares; MF, myelofibrosis; PET-MF, post-essential thrombocythemia myelofibrosis; PMF, primary myelofibrosis; PPV-MF, post-polycythemia vera myelofibrosis; Resp, number of responders; TSS, total symptom score; TSS50, ≥50% TSS reduction from baseline.
Extended Data Fig. 3 Duration of spleen and TSS50 responses.
(A) Shows Kaplan–Meier estimate of duration of spleen response by central read, defined as the time from first spleen response ( ≥ 35% reduction in spleen volume) until a spleen volume reduction of <35% from baseline and an increase of >25% from nadir was first documented. Median duration of response using Kaplan–Meier was not estimable in either treatment arm at the data cut-off. The median duration of follow-up of splenic response was 27.143 weeks (95% CI: 24.143, 36.143) in the pelabresib–ruxolitinib arm and 25.429 weeks (95% CI: 24.143, 35.857) in the placebo–ruxolitinib arm. (B) Shows Kaplan–Meier estimate of the duration of symptom response, defined as the time from onset of TSS50 response until the time at which a < 50% reduction in TSS from baseline and an increase of ≥25% from nadir is first observed. These data are not mature. TSS, total symptom score; TSS50, ≥50% TSS reduction from baseline.
Extended Data Fig. 4 Dual spleen and symptom responses.
SVR35, ≥35% reduction in spleen volume; TSS50, ≥50% reduction in total symptom score.
Extended Data Fig. 5 Pro-inflammatory cytokines, bone marrow morphology, and erythrocyte progenitors.
For exploratory endpoints, we report descriptive statistical analyses only. (A) shows the mean change in inflammatory cytokines from baseline at week 24. Data are presented as mean change from baseline ± 95% CI. *NF-κB – set included B2M, CRP, CD40-L, hepcidin, IL-6, IL-12p40, MIP-1 beta, MPIF-1, RANTES, TNFR2, TNF, and VCAM-1. (B) shows the secondary endpoint change in reticulin fibrosis grade (graded according to the WHO classification) by central read at week 24. Percentages are based on the number of patients with bone marrow assessments in the intent-to-treat population at each timepoint; non-evaluable patients are those who are ongoing study treatment and have not yet reached that timepoint or opted out of bone marrow assessment. (C) shows the change in megakaryocytes (CD61 + ) density from baseline in the bone marrow at week 24, overlayed with individual observations. Density assessed by digital pathology. The horizontal line within the boxplot indicates the mean. The lower and upper ends of the box represent the 25th and 75th percentiles, respectively. The boxplot whiskers indicate the Tukey interval. (D) shows examples of immunohistochemistry stainings for megakaryocytes (CD61 + ) representative for observed mean changes of megakaryocyte densities in samples from a single patient randomized to pelabresib–ruxolitinib and a single patient randomized to placebo-ruxolitinib, respectively. There were 117 patients in the pelabresib–ruxolitinib arm and 129 patients in the placebo-ruxolitinib arm with megakaryocyte density data. Immunohistochemistry staining was performed, and digital images analyzed by an automated quantitative cell-specific detection analysis. (E) shows the percentage change in erythrocyte progenitors (CD71+ cells) in the bone marrow according to treatment arm and red blood cell transfusions, overlayed with individual observations. Red blood cell transfusions refer to the number of patients who received any red blood cell transfusion between week 20 and week 24 on treatment. The horizontal line within the boxplots indicates the mean. The lower and upper ends of the box represent the 25th and 75th percentiles, respectively. The boxplot whiskers indicate the Tukey interval. The y-axis encompasses the 99 percentiles of all values. B2M, beta-2 microglobulin; CI, confidence interval; CRP, C-reactive protein; CD40-L, CD40 ligand; IL, interleukin; MIP, macrophage inflammatory protein; MPIF, myeloid progenitor inhibitory factor; NF-κB, Nuclear factor kappa B; RANTES, regulated upon activation, normal T-cell expressed and secreted; TNF, tumor necrosis factor; TNFR, TNF receptor; VCAM, vascular cell adhesion molecule; WHO, World Health Organization.
Extended Data Fig. 6 Change in pro-inflammatory cytokine levels according to spleen response ( ≥ 35% reduction in spleen volume).
Figure shows the mean relative difference in inflammatory cytokine changes from baseline at week 24 in patients with spleen response compared to patients without spleen response. Data are presented as mean relative difference ± 95% CI. For exploratory endpoints, we report descriptive statistical analyses only. *NF-κB set included B2M, CRP, CD40-L, hepcidin, IL-6, IL-12p40, MIP-1 beta, MPIF-1, RANTES, TNFR2, TNF, VCAM-1. B2M, beta-2 microglobulin; CI, confidence interval; CRP, C-reactive protein; IL, interleukin; MIP, macrophage inflammatory protein; MPIF, myeloid progenitor inhibitory factor; NF-κB, nuclear factor kappa B; RANTES, regulated upon activation, normal T cell expressed and secreted; TNF, tumor necrosis factor; TNFR, TNF receptor; VCAM, vascular cell adhesion protein.
Extended Data Fig. 7 Impact of driver and high-molecular risk mutations at baseline on clinical response rates at week 24.
Data are presented as mean value ± 95% CI. *HMR mutations include ASXL1, EZH2, IDH1, IDH2, SRSF2, and U2AF1 mutations. †Clopper–Pearson 95% CI. ASXL1, ASXL transcriptional regulator 1; CALR, calreticulin; CI, confidence interval; EZH2, enhancer of zeste 2 polycomb repressive complex 2 subunit; HMR, high molecular risk; IDH1/2, isocitrate dehydrogenase 1/2; JAK2, Janus kinase 2; MPL, MPL proto-oncogene, thrombopoietin receptor; SRSF2, serine and arginine rich splicing factor 2; SVR35, ≥35% reduction in spleen volume from baseline; U2AF1, U2 small nuclear RNA auxiliary factor 1; WT, wild type.
Supplementary information
Supplementary Information
Supplementary Figs. 1 and 2 and Tables 1–3; CONSORT 2010 checklist.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Rampal, R.K., Grosicki, S., Chraniuk, D. et al. Pelabresib plus ruxolitinib for JAK inhibitor-naive myelofibrosis: a randomized phase 3 trial. Nat Med 31, 1531–1538 (2025). https://doi.org/10.1038/s41591-025-03572-3
Received:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/s41591-025-03572-3
This article is cited by
-
The evolving landscape of epigenetic target molecules and therapies in myeloid cancers: focus on acute myeloid leukemia and myeloproliferative neoplasms
Leukemia (2025)
-
Emerging Therapeutic Approaches for Anemia in Myelofibrosis
Current Hematologic Malignancy Reports (2025)
-
Highlights from MPN Asia 2025: Advances in Molecular Pathogenesis and Therapeutic Strategies in Myeloproliferative Neoplasms
Current Hematologic Malignancy Reports (2025)
