
Abstract
This data resource provides evidence concerning the prevalence of perceptual alterations of emotional faces amongst individuals experiencing symptoms of insomnia, anxiety, depression, mania, psychotic experiences, and schizotypal tendencies. More specifically, we explored the categorisation accuracy (whether the displayed emotion was correctly identified), misperception (which emotion an incorrect judgment was perceived to be), intensity (extent of the emotion signal strength) and emotional valence (the extent and direction of perceived affect) of six facial expressions of emotion from the Karolinska Directed Emotional Faces database. Complete data from N = 572 respondents are included. The dataset is available to other researchers and is provided on Figshare. Information concerning the data records, usage notes, code availability and technical validation are presented. Finally, we present demographic and correlational data concerning psychiatric symptoms and alterations in the perception of emotional faces.
Similar content being viewed by others

Background and Summary
Social perceptual judgments facilitate the evaluation of another person, particularly when drawing upon emotionally salient information1,2. Individuals use facial, vocal, gestural, and postural cues to communicate emotions to others; whilst also reading such cues to determine another’s’ internal state3,4. Here, visual processing of the human face remains the most prevalent source of information5. Indeed, facial observations provide vital information pertaining to distinguishing characteristics, perceived attractiveness, intended behaviour, and emotional state, without use of language6. Accordingly, the nature of facial expressions serves as a primary source of information in social perception7,8.
Accurate judgments of facially expressed emotion are vital for effective social interactions and non-verbal social judgments. Therefore, perceptual deficits associated with psychiatric symptoms may contribute to negative psychosocial consequences for those involved9. Perceptual alterations of emotional faces are widely established in psychiatric populations at both disorder and symptom level (e.g. insomnia, anxiety, depression, bipolar disorder, anorexia nervosa, schizophrenia)10,11,12,13,14,15.
The present work sought to further examine the prevalence of perceptual alterations of emotional faces amongst individuals experiencing symptoms of insomnia, anxiety, depression, mania, psychotic experiences, and schizotypal tendencies. More specifically, we examined the categorisation accuracy (whether the displayed emotion was correctly identified), misperception (which emotion an incorrect judgment was perceived to be), intensity (the strength of the emotion signal strength) and emotional valence (the extent and direction of perceived affect in relation to intrinsic appeal or repulsion) of all six cross-culturally accepted facial expressions of emotion16.
Methods
Sample and Design
The study was approved by the Sheffield Hallam University Research Ethics Committee (Protocol number: ER28407811), and all participants provided online informed consent. Students from two UK universities were recruited through institutional course participation schemes, social media groups and faculty emails. This resulted in a sample of N = 706 individuals who either began or clicked on a hyperlink to the survey which was delivered using the Qualtrics platform (Qualtrics, Provo, UT). Only complete cases were used in the analysis due to the ethical right to withdraw from the survey at any time. The data were also examined for duplicate responses based on matching IP addresses, where none were found. To maintain participant anonymity, IP addresses were subsequently discarded. In addition, no personally identifying information or contact details were recorded. Rather, subjects provided a memorable keyword at the start of the survey which was to be cited in any request to withdraw data. Therefore, N = 572 respondents (mean age = 21.71 ± 7.30 years, range 18–65, 76% female; 89% student) providing complete data for the variables of interest. All participants reported: normal to corrected-to-normal vision, the absence of prosopagnosia, being ≥18 years old.
Materials
Facial stimuli
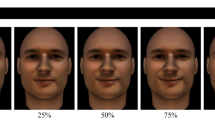
Fifty-six facial photographs of eight individuals (50% female) displaying the emotional expressions of fear, anger, disgust, happiness, sadness, surprise, and neutrality were gathered from the Karolinska Directed Emotional Faces database17. In the present study, we chose to use all six cross-culturally accepted facial expressions of emotion16. These six expressions are commonly used to examine the perception of emotional faces in the context of psychiatric disorder. In line with previous studies controlling for potentially distracting and confounding factors, we cropped the hair and neckline from each image18,19,20,21. Thus, leaving a series of oval-shaped neutral facial images (see Fig. 1).

Example set of facial expressions.
Psychometric measures
Insomnia
Insomnia symptoms were assessed using the Insomnia Severity Index (ISI)22. The ISI consists of seven items examining the severity of insomnia symptoms over the past 2 weeks including difficulty initiating and maintaining sleep and awakening too early. Items are scored on a 5-point likert-type scale, with total scores ranging from 0 to 28. Higher scores suggest greater insomnia severity. Total scores between 0 and 7 indicate no clinically significant insomnia, 8 and 14 subthreshold insomnia, 15 and 21 clinical insomnia (moderate severity), and 22 and 28 clinical insomnia (severe). Assessment of internal consistency Cronbach’s alpha) yielded an alpha of α = 0.88.
Anxiety
The 7-item Generalized Anxiety Disorder Scale (GAD-7) is a validated practical self-report anxiety questionnaire used in primary care23. The tool asks respondents how often, during the last 2 weeks, they have been bothered by each of the seven core symptoms of generalized anxiety disorder. Responses choice are 0 = “not at all”; 1 = “several days”; 2 = “more than half the days”; and 3 = “nearly every day”. Total scores range between 0 and 21 with cut offs of ≥5, ≥10, and ≥15 indicating mild, moderate, and severe anxiety levels, respectively. The GAD-7 has been shown to exhibit good reliability, as well as criterion, construct, factorial, and procedural validity23. The Cronbach’s alpha in the current study was α = 0.92.
Depression
The 9-item patient health questionnaire (PHQ-9)24 is a brief self-report depression scale used to assess depressive symptoms in the general population. Each of the nine depressive symptoms corresponds to the depression criteria of the DSM-V25. Respondents are required to indicate how much, during the previous 2 weeks, the symptom has bothered them on a scale of: 0 = “not at all”, 1 = “several days”, 2 = “more than half of the days” or 3 = “nearly every day”. Total scores indicate depression severity and range from 0 to 27 with higher scores indicating higher levels of depression. The scale has been shown to demonstrate good criterion and construct validity23,24. Cronbach’s alpha in the current study was α = 0.91.
Mania
The Mood Disorder Questionnaire (MDQ) was used to examine symptoms of mania (range 0–13)25. Participants provided a response of yes/no when presented with a series of prompting questions. For example, “Has there ever been a time when you were not your usual self and…”. The summation of each item yields a total MDQ score where higher scores indicate increased levels of manic symptoms. The internal consistency of the scale in the present study was α = 0.85. To screen positive for possible bipolar disorder, all three parts of the following criteria should be met based on the initial 13 items and two additional questions. More specifically, participants must answer yes to ≥7 of the thirteen items; indicate cooccurrence of ≥1 items within the same period; and report moderate to serious consequences of the possible episode (i.e., inability to work; family, monetary or legal difficulties; aggressive behaviour).
Psychotic like experiences
The Prodromal Questionnaire 16 (PQ-16) was administered to assess life-time symptoms of psychotic experiences26. It was developed as a brief version of the 92-item Prodromal Questionnaire26 to enable the detection of ultra-high-risk (UHR) patients in routine adult mental health services. Sixteen items evaluate the occurrence of positive/negative symptoms and avolition on a two-point scale (yes/no). In addition, symptom distress is measures on a four-point scale between: 0 = no distress and 3 = severe distress. More specifically, the PQ-16 contains nine items relating to hallucinations; five items relating to delusions; and two negative symptom items. The summation of ‘yes’ item responses yield a total score between 0 and 16, where higher scores indicate an increased number of psychotic symptoms. In adults, a score of ≥6 predicts diagnosis of psychosis with high sensitivity (87%) and specificity (87%)27. Similarly, distress items are summated to create a total prodromal severity scale. The Cronbach’s alpha in the current study was α = 0.85 for total scores and α = 0.90 for severity scores.
Schizotypal traits
The Short-Form Oxford-Liverpool Inventory of Feelings and Experiences scale examined schizotypal personality traits (O-LIFE)28. The 43-item measure is comprised of four subscales: unusual experiences (12-Items), cognitive disorganisation (11-items), introverted anhedonia (10-items), and impulsive nonconformity (10-items). The unusual experiences subscale examines positive symptoms related to psychosis (i.e., perceptual aberrations, magical thinking, hallucinations). Cognitive disorganisation explores disorganised features of psychosis (i.e., concentration difficulties, impaired decision-making, social anxiety). The introverted anhedonia subscale examines negative schizotypy, primarily characterised by a lack of physical and social pleasure (i.e., intimacy, social activities). Impulsive nonconformity measures diminished self-control (i.e., impulsive, anti-social, eccentric behaviour). All items utilise a two-point scale (yes/no). The summation of ‘yes’ item responses yield a total score for each respective subscale. The Cronbach’s alpha in the current study was α = 0.78 for unusual experiences, α = 0.81 for cognitive disorganisation, α = 0.70 for introverted anhedonia, and α = 0.70 for impulsive nonconformity.
Procedure
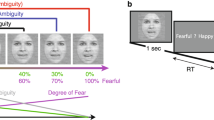
Participants completed an online questionnaire, in which they were presented with the series of fifty-six images in randomized order. For each face displayed, participants were asked to select (categorise) the corresponding emotional expression (fear, anger, disgust, happiness, sadness, surprise, and neutral). Subsequently, participants were asked to rate their perceived intensity and emotional valance on a 100-mm visual analogue scale. The intensity scale was anchored at not very intense and extremely intense. Whereas valence was anchored at extremely negative and extremely positive. Each face was displayed until a response was made. Following the completion of the face-task, participants completed the ISI, GAD-7, PHQ-9, MDQ PQ-16 and O-LIFE. The procedure lasted approximately thirty minutes. An example trial is presented in Fig. 2.

Example trial.
Data Records
The dataset (demographics, psychiatric measures) has been anonymised and both individual datapoints for each psychometric measure and face rating are available in CSV and SAV formats on Figshare (https://doi.org/10.6084/m9.figshare.26397817)29 and as part of the current supplemental information (see Appendix A). For copyright reasons, the original PDF files including scoring information for each measure are not included in the appendix. However, the key scoring information is provided in the aforementioned measures section, and each original measure can be individually examined where necessary. In the current dataset, reverse coding was applied where required. Finally, the total/mean or composite score for each psychiatric symptom and perceptual judgments of emotional faces displaying each expression (accuracy, and intensity) were calculated and included to simplify the usability of the dataset. Descriptions of calculated variables are provided in Table 1. Details of the data cleaning procedure are available in the following section.
Technical Validation
For the current purpose, the SAV file was exported from the Qualtrics online survey platform (Qualtrics, Provo, UT) where the data was cleaned using SPSS v. 29.0 (IBM Corp., Armonk, NT, USA). Total ratings of accuracy were summated for each expression. For each trial, correct responses yielded a score of 1 whereas incorrect responses were scored as 0. Therefore, accuracy scores ranged between 0 to 8, with higher scores indicating greater categorisation accuracy of the assessed expression. Next, mean expression intensity ratings were calculated, and ranged between a possible 0 to 100 score, with higher scores indicating greater intensity ratings. Finally, mean emotional valence ratings were calculated, and ranged between a possible 0 to 100 score, with higher scores indicating more positively valanced ratings. Descriptive statistics for all calculated variables were inspected to ensure that results fell within an expected range. Whilst normality was assessed using histograms, it is vital to consider the inherent skew observed when examining psychiatric symptoms, where a traditional disruption would not be expected. As noted, reliability analysis was performed for each psychometric measure. Here, the internal consistency (Cronbach’s α) of each scale remained acceptable. Examination of internal consistency for the intensity of each expression yielded α values between 0.82–0.92. Examination of internal consistency for the emotional valence of each expression yielded α values between 0.68–0.88. Examination of internal consistency for the categorisation before recoding was α = 0.46–0.67 after recoding. Therefore, the facial stimuli reliably depicted their corresponding expression with a degree of confidence (see Table 2 for each α value). The dataset was carefully inspected for abnormal response patterns and completion times before any formal analyses was conducted. Neither were observed. To facilitate the potential usability and consideration of further analysis of the current data set, the descriptive statistics (means and standard deviations), and Pearson’s bivariate correlations (two-tailed) between expression intensity, emotional valance, categorization accuracy and misperception scores with symptoms of insomnia, anxiety, depression, mania, psychotic experiences, and schizotypal traits are presented in Tables 2, 3 and 4 respectively. Significance was considered at the p < 0.05 level.
Several strengths and limitations of the current data should be noted. The cross-sectional nature limits the ability to draw any definitive explanation when concerning causal relationships. Next, the sample was not homogeneous, including a disproportionate amount of data from young white female respondents. Finally, potential users of the current data should consider limitations associated with subjective assessments which rely on self-reported information. That said, all six cross-culturally accepted facial expressions of emotion were examined16,30, with the inclusion of data concerning the emotional valance and misperception of emotional expressions above the typical inclusion of only accuracy and intensity. Whilst similar studies typically focus on a smaller set of related symptoms, the present data provides perceptual judgments across a large domain of psychiatric symptoms. Often with large scale data collection, studies may employ scales single-item or bespoke in-house scales, which fail to capture symptom severity and specificity31. Accordingly, the current data provides a comprehensive assessment of psychiatric symptoms by using well validated scales with robust psychometric properties.
Usage Notes
Data have been deidentified and are presented in the same manner across data files, which can be imported into most compatible statistical software packages. As noted, the dataset includes all individual datapoints for each de-identifiable psychometric measure and perceptual judgment. For each validated questionnaire, the initial authors scoring instructions were followed to calculate the relevant total, composite, and subscale variables which may be of interest.
Data availability
Data is available on Figshare: https://doi.org/10.6084/m9.figshare.26397817.
Code availability
No custom code was used during the compilation of the dataset.
References
Singer, T., Kiebel, S. J., Winston, J. S., Dolan, R. J. & Frith, C. D. Brain responses to the acquired moral status of faces. Neuron 41, 653–662 (2004).
Todorov, A., Said, C. P., Engell, A. D. & Oosterhof, N. N. Understanding evaluation of faces on social dimensions. Trends in Cognitive Sciences 12, 455–460 (2008).
Sauter, D. A., Eisner, F., Ekman, P. & Scott, S. K. Cross-cultural recognition of basic emotions through nonverbal emotional vocalizations. Proceedings of the National Academy of Sciences 107, 2408–2412 (2010).
Li, J. et al. CAS (ME) 3: A third generation facial spontaneous micro-expression database with depth information and high ecological validity. IEEE Transactions on Pattern Analysis and Machine Intelligence 45(3), 2782–2800 (2022).
Allison, T., Puce, A. & McCarthy, G. Social perception from visual cues: Role of the STS region. Trends in Cognitive Sciences 4, 267–278 (2000).
Haxby, J. V., Hoffman, E. A. & Gobbini, M. I. The distributed human neural system for face perception. Trends in Cognitive Sciences 4, 223–233 (2000).
Akram, U. Perceptual differences in emotionally ambiguous neutral faces among individuals displaying clinically significant insomnia symptoms. Perception 49(10), 1090–1100 (2020).
Axelsson, J. et al. Beauty sleep: Experimental study on the perceived health and attractiveness of sleep deprived people. BMJ 341, c6614 (2010).
Akram, U., Robson, A. & Ypsilanti, A. Sleep-related attentional bias for faces depicting tiredness in insomnia: evidence from an eye-tracking study. Journal of Clinical Sleep Medicine 14(6), 959–965 (2018).
Akram, U. & Stevenson, J. C. Altered perception of emotional faces in young adults experiencing loneliness after controlling for symptoms of insomnia, anxiety and depression. Journal of Affective Disorders Reports 12, 100581 (2023).
Bourke, C., Douglas, K. & Porter, R. Processing of facial emotion expression in major depression: a review. Australian and New Zealand Journal of Psychiatry 44, 681–696 (2010).
Kohler, C. G., Walker, J. B., Martin, E. A., Healey, K. M. & Moberg, P. J. Facial emotion perception in schizophrenia: a meta-analytic review. Schizophrenia bulletin 36(5), 1009–1019 (2010).
Kyle, S. D., Beattie, L., Spiegelhalder, K., Rogers, Z. & Espie, C. A. Altered emotion perception in insomnia disorder. Sleep 37, 775–783 (2014).
Lembke, A. & Ketter, T. A. Impaired recognition of facial emotion in mania. American Journal of Psychiatry 159(2), 302–304 (2002).
Pollatos, O., Herbert, B. M., Schandry, R. & Gramann, K. Impaired central processing of emotional faces in anorexia nervosa. Psychosomatic Medicine 70, 701–708 (2008).
Ekman P., Friesen W. V. Pictures of facial affect. Palo Alto, CA: Consulting Psychologists Press, 1976.
Lundqvist, D., Flykt, A., and Öhman, A. (1998). The Karolinska Directed Emotional Faces - KDEF, CD ROM from Department of Clinical Neuroscience, Psychology section, Karolinska Institutet. ISBN:91-630-7164-9.
Akram, U. et al. Sleep-related attentional bias for tired faces in insomnia: evidence from a dot-probe paradigm. Behaviour research and therapy 103, 18–23 (2018).
Akram, U., Sharman, R. & Newman, A. Altered perception of facially expressed tiredness in insomnia. Perception 47(1), 105–11 (2018). Jan.
Duchaine, B. C., Parker, H. & Nakayama, K. Normal recognition of emotion in a prosopagnosic. Perception 32(7), 827–838 (2003).
Ferrari, C., Oldrati, V., Gallucci, M., Vecchi, T. & Cattaneo, Z. The role of the cerebellum in explicit and incidental processing of facial emotional expressions: a study with transcranial magnetic stimulation. Neuroimage 169, 256–264 (2018).
Bastien, C. H., Vallières, A. & Morin, C. M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep medicine 2(4), 297–307 (2001).
Spitzer, R. L., Kroenke, K., Williams, J. B. & Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of internal medicine 166(10), 1092–1097 (2006).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ‐9: validity of a brief depression severity measure. Journal of general internal medicine 16(9), 606–613 (2001).
American Psychiatric Association DS, American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American psychiatric association; 2013 May 22.
Ising, H. K. et al. The validity of the 16-item version of the Prodromal Questionnaire (PQ-16) to screen for ultra high risk of developing psychosis in the general help-seeking population. Schizophrenia Bulletin 38, 1288–1296 (2012).
Loewy, R. L., Bearden, C. E., Johnson, J. K., Raine, A. & Cannon, T. D. The prodromal questionnaire (PQ): Preliminary validation of a self-report screening measure for prodromal and psychotic syndromes. Schizophrenia Research 79, 117–125 (2005).
Mason, O. & Claridge, G. The Oxford-Liverpool Inventory of Feelings and Experiences (O-LIFE): further description and extended norms. Schizophrenia research 82(2-3), 203–211 (2006).
Akram, U. & Stevenson, J. S. Altered emotion perception in insomnia, anxiety, depression, mania, psychotic experiences and schizotypal symptoms. Figshare https://doi.org/10.6084/m9.figshare.26397817 (2024).
Aviezer, H. et al. Angry, disgusted, or afraid? Studies on the malleability of emotion perception. Psychological Science 19(7), 724–32 (2008).
Hom, M. A., Joiner, T. E. Jr & Bernert, R. A. Limitations of a single-item assessment of suicide attempt history: Implications for standardized suicide risk assessment. Psychological Assessment 28(8), 1026 (2016).
Hirschfeld, R. M. A. et al. Development and validation of a screening instrument for Bipolar Spectrum Disorder: The mood disorder questionnaire. American Journal of Psychiatry 157, 1873–1875 (2000).
Acknowledgements
No funding was received for this research.
Author information
Authors and Affiliations
Contributions
The experiment was designed and conceived by U.A. and J.S. Data was collected by U.A. and J.S. An initial version of the manuscript was written by U.A. Following, input was sought from J.S.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Akram, U., Stevenson, J. Altered emotion perception in insomnia, anxiety, depression, mania, psychotic experiences and schizotypal symptoms: a dataset. Sci Data 11, 990 (2024). https://doi.org/10.1038/s41597-024-03736-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41597-024-03736-9
