
Abstract
Previous research on the association between Family Doctor Contract Services (FDCS) and health has only considered a single indicator of health and has not considered the endogeneity of independent variables. This study aimed to evaluate the association from a multidimensional perspective of the health of middle-aged and older people using the instrumental variables method and determine the underlying mechanisms. Using data from the 2018 China Health and Retirement Longitudinal Study surveys, a total of 19,438 sample was obtained. Health was measured by health related-quality of life (HR-QoL), subjective well-being, and cognitive function. The instrumental variables method was used to estimate the association. Mediation analysis was employed to analyze the underlying mechanisms. The results of the instrumental variables method showed a correlation between FDCS and health, such as HR-QoL (η = 33.714, p < 0.01), subjective well-being (η = 1.106, p < 0.05), and cognitive function (η = 4.133, p < 0.05). However, we found no evidence that FDCS improved physical health. We also identified reduced utilization of healthcare services and increased social activities as mediators of the effect of FDCS on health. The Chinese government should improve incentive-based initiatives to improve the quality of FDCS. Moreover, more attention needs to be paid to the multidimensional health of middle-aged and older people, especially vulnerable groups, such as older individuals and those in rural areas.
Similar content being viewed by others

Introduction
The family doctor system has been described by the World Health Organization (WHO) as the “most economical and appropriate” model of health care management recognized in most countries and regions. Family doctors, who provide primary and continuing care for all individuals, include physicians and other medical specialists in primary health care1. As the gatekeepers of residents’ health, family doctors play an important role in promoting hierarchical treatment2, enhancing the accessibility of health services3, and improving health4.
Existing practice and research show a positive association between family doctors and health. For example, in the United States, the family doctor system incorporated health management into community general practitioner services, which was effective in promoting the availability of health care5, reducing maternal mortality6, and informing related health policy and standard setting7. The Family Medicine Group (FMG) model of primary care in Quebec, Canada, revealed a significant relationship between family doctors and emergency department visits as well as hospital admissions8. Practice and research in Tehran also demonstrated that family doctors improved urban public health services9, and strikingly promoted health care access in rural areas10. Treharne et al. found when transgender people received supportive care from their family doctors in New Zealand, they experienced better mental health11.
China’s health care system reform in 2009 laid a good foundation for the implementation of the Family Doctor Contract Services (FDCS) system. Officially implemented in 2016, FDCS aimed to provide the public with a proactive, consistent, comprehensive, and affordable model of health accountability management in China12. At the end of 2021, approximately 1.435 million family doctors had been put in place (3.08 family doctors per 10,000 population), forming 431,000 teams to provide services to residents13. The FDCS services include basic medical care services, public health services, and individualized health management. According to the voluntarily signed contract and standardized service, family doctors establish a long-term service relationship with the families, enhancing the accessibility of contracted FDCS. By the end of 2020, the FDCS contracting rate for key populations increased from 28.33% in 2015 to 75.46%14. Moreover, most participants who contracted FDCS were willing to maintain contracts with their family doctors15. In addition, family doctors provide more than 95% of primary health care in rural China, indicting the services are easy to receive16. FDCS have made significant progress in promoting population health17. Li et al.found a significant and positive association between FDCS and HR-QOL among chronic patients in rural Shandong, China18. Xu et al. evaluated the effect of FDCS on the health management in Chinese type 2 diabetes mellitus patients, they found that patients participated in FDCS had a lower risk of diabetes-related complications than those who did not19. A cross-sectional survey in Shaanxi Province showed that the individuals with a contracted family doctor had significantly higher HR-QoL than those without20.
These studies highlight the importance of family doctors in improving population health. Nevertheless, current studies have some shortcomings. First, a single indicator or regional data is employed to measure population health. Second, current approaches to estimating the association between FDCS and health pay less attention to the endogeneity of family doctors, which may lead to bias. Third, an analysis of the mechanisms underlying the relationship between family doctors and health is lacking. Given the above limitations, this study aimed to: (1) based on national survey data, estimate the association between FDCS and health from a multidimensional perspective in China, (2) use the instrumental variables (IV) method to address the bias due to endogeneity, and (3) analyze the mechanisms underlying the association between FDCS and the health of middle-aged and older people using mediation analysis.
Theoretical framework
The principal-agent theory is employed in the theoretical framework to explain the association between FDCS and the health of middle-aged and older people. The principal-agent theory has been widely used in the field of medicine to explain the healthcare payment contract21, medical choice22, and the doctor-patient relationship23. This paper applies the principal-agent theory and argues that there is a triple principal-agent relationship in FDCS, as shown in Fig. 1.

Theoretical framework. Author’s analysis.
Solid arrows indicate the actual principal-agent relationship between residents, government, and family doctors. The first principal-agent relationship exists between residents and the government. As residents (the principal) were unable to employ family doctors directly, the government had the responsibility of protecting the public interest. Therefore, the government, as the agent, needed to formulate the FDCS that met the healthy needs of the residents, considering their willingness to contract, to ensure that they could receive more healthcare services from their family doctors.
The second principal-agent relationship exists between the government and family doctors. In China, the government could not provide health care directly, it entrusted family doctors in primary healthcare institutions to meet the needs of residents. The government promotes family doctors to provide services to residents through various means, such as incentives and supervision. In addition, family doctors play the role of the agent to provide health care services to residents directly. Moreover, FDCS currently covers basic medical services, basic public health services, and personalized services24.
The third principal-agent relationship exists between residents and family doctors. Residents act as principals and family doctors as agents. This relationship is characterized by a marked asymmetry of information, with family doctors having sophisticated medical expertise that the residents lack. In addition to information asymmetry, an anxiety asymmetry is also present. This means that when residents believe they might have a serious illness, they delegate their anxiety to their family doctor, providing an alternative explanation for residents seeking medical care25. Therefore, family doctors are obliged to use their skills competently to detect physical abnormalities among residents, alleviate their pain, and cure their illnesses.
Methods
Ethics approval and consent to participate
The China Health and Retirement Longitudinal Study (CHARLS) project was approved by the Peking University Biomedical Ethics Review Committee (IRB00001052-11015). Informed consent was obtained from all the study participants, and the data were anonymized for analysis. All methods were carried out in accordance with relevant guidelines and regulations.
Data source
Data were obtained from the CHARLS, implemented by Peking University, which aimed to collect a nationally representative sample of middle-aged and older people to support aging and health-related research through a structured questionnaire (the data and questionnaire are available at http://charls.pku.edu.cn/). This study only included middle-aged and older people (aged ≥ 45 years) who participated in the survey in 2018. After removing the 228 samples younger than 45 years, a total of 19,438 valid samples were included.
Measures
Independent variable
In this study, the variable “Have you ever receive the paid family doctor services?” from the CHARLS was used to identify residents who had contracted FDCS.
Dependent variables
The dependent variable was health, which includes HR-QoL, subjective well-being, and cognitive function26,27,28. To measure the HR-QoL, a new scale, the Short Form 36 (SF-36), was employed based on the CHARLS questionnaire. It is a 36-question comprehensive health survey that assesses eight health concepts used to define HR-QoL29. The scores of the eight subscales were summarized into a physical component score (PCS) and a mental component score (MCS), with higher PCS or MCS scores indicating higher levels of physical or mental health. Moreover, the variable “Please think about your life as a whole. How satisfied are you with it?” was used to identify the subjective well-being of the sample. Finally, the Mini Mental State Exam (MMSE), the most widely used neuropsychological scale for measuring cognitive function, was used30. In addition, there were missing values for dependent variables, such as HR-QoL (missing values = 1,789), PCS (missing values = 1,676), MCS (missing values = 1,548), subjective well-being (missing values = 1,546), and cognitive function (missing values = 9,997).
Instrumental variable
“The combination of medical and healthcare service” was chosen as the instrumental variable. It was expressed in the CHARLS questionnaire as “Have you ever received the following home and community care services?”.
Mediation variables
In addition, with reference to previous studies31, this study included the underlying mediation variables of healthcare service utilization (whether or not to use outpatient or inpatient services) and whether or not to participate in social activities.
Control variables
The control variables included area, residence, gender, age, marital status, education, household income, insurance, smoke, drink, and chronic diseases. All Variables assignment see Table 1 for details.
Conceptual framework
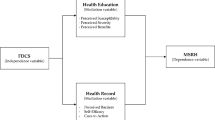
Figure 2 shows the conceptual framework of the study. To address the endogeneity of FDCS, we used “the combination of medical and healthcare service” as an instrumental variable to estimate the association of FDCS with health. In addition, the study hypothesizes that the FDCS affects the health of middle-aged and older people by influencing their “healthcare service utilization” and their “social activities”, which in turn affect their health (including HR-QoL, PCS, MCS, subjective well-being, and cognitive function).

Source: Author’s analysis.
Conceptual framework.
Model setting
This study determined the association of FDCS with health by constructing the following model:
where \(Y\) represents the explanatory variable of individual \(i\) at the points \(t\), representing the health of participants contracted FDCS; \(FDCS\) represents the dummy variable of whether individual \(i\) “received family doctor contract services” at time \(t\), where 1 denotes received and 0 is not received; and \({\upbeta }_{i}\) represents the control variables, \({\upsigma }_{i}\) represents the area fixed effects, and \({\upvarepsilon }_{i}\) represents the random disturbance term.
Instrumental variables method
When used as an explanatory variable, family doctors may cause endogeneity, leading to important information being overlooked when analyzing causality and thus to the overestimation or underestimation of the positive features of FDCS. In addition, population health may be affected by other factors, such as personal habits and the surrounding environment, which are unobservable.
In this study, the IV method was adopted to address endogeneity. It usually uses one or more instrumental variables that are related to the critical explanatory variable but not directly related to the outcome variable to identify the impacts of the exposure variable on the explained variable, which could lead to a consistent estimation. In this study, “the combination of medical and healthcare service” was chosen as instrumental variable. “The combination of medical and healthcare service” is provided by family doctors directly, but it not directly related to the health, so it meets the requirements of the IV method. The following regression model was set up for a two-stage least squares test:
Model (2) represents the first stage of the regression, with the dependent variable being health. \(yiyang\) represents whether the participants received “the combination of medical and healthcare service.” Model (3) represents the results of the second-stage regression, where the dependent variable is family doctors, and \(Statues\_health\_exp\) denotes estimates from the first-stage regression.
Mediation mechanism analysis
Family doctors, through disease screening, may influence the utilization of health care services by middle-aged and older people, which in turn has an impact on their health. Second, through psychological counselling and health education, they may encourage residents to actively participate in social activities, which will expand their social network, prevent social isolation, and in turn affects the health of middle-aged and older people.
To further explore the mechanism of the relationship between FDCS and health, we conducted a mediation effect analysis using health care services utilization and social activities as mediation variables. According to the BK method32, we first tested the effect of FDCS on the health of middle-aged and older people; secondly, we tested the effect of FDCS on the mediation variables (i.e., Health care services utilization and social activities). Finally, we tested the effect of FDCS and the mediation variables on the health of middle-aged and older people. In this case, the test was stopped whenever one of the regression results was not significant, indicating that it could not pass the mediation mechanism test. Based on this, the following model is constructed:
where \({M}_{it}\) represents mediation variables of individual \(i\) at the points \(t\), representing health care services utilization and social activities of middle-aged and older people.
Analytical strategy
All variables were presented as mean and standard deviation (S.D.). The ordinary least-squares (OLS) model was employed to estimate the impact of FDCS on the health of middle-aged and older people. All statistical analyses were performed using STATA statistical software version 15.1. A two-tailed p-value < 0.1 was considered statistically significant.
Results
Descriptive statistics of the sample
Table 2 shows the characteristics of the 19,438 samples. A total of 32.58% lived in the West and 40.15% lived in urban areas. 47.55% were male, and the average age was about 62 years. In addition, 34.44% of the participants had junior high school—level education or above, and 99.39% of the samples lived with their spouse. An overwhelming majority of participants were covered by insurance (97.03%), Nearly 5% of the participants smoked, and 34% drunk. It was reported that 49.29% participants had chronic diseases, 16.47% and 16.88% participants utilized the outpatient services and inpatient services, respectively, and 53.01% participants had social activities. See Table 2 for details.
Regression results
Table 3 shows the estimated results of the association of FDCS with the health. Participants who received the FDCS had an increase in HR-QoL of 1.084 points (p < 0.05). FDCS significantly increased mental health by 2.196 points (p < 0.01). In addition, participants who received the FDCS had improved subjective well-being and cognitive functioning by 0.087 points (p < 0.01) and 0.354 points (p < 0.01), respectively. See Table 3 for details.
Endogeneity analysis
Table 4 shows the results of the effects of FDCS on the health using the IV method. The F-values for the IV in the first-stage regression results were greater than 10, rejecting the initial hypothesis that the IV was weakly instrumental and demonstrating the validity of the IV. The results showed a correlation between FDCS and the health, including HR-QoL (η = 33.714, p < 0.01), subjective well-being (η = 1.106, p < 0.05), and cognitive function (η = 4.133, p < 0.05). Compared to the results of the OLS regression, FDCS improved HR-QoL, subjective well-being, and cognitive function by 32.63, 1.019, and 3.779 points, respectively, indicating that endogeneity in the model caused the OLS regression to underestimate the association between FDCS and the health. See Table 4 for details.
Analysis of heterogeneity
To further analyze the impact of FDCS on health in detail, we analyzed heterogeneity in terms of age, place of residence, and the presence of chronic diseases. Specifically, FDCS significantly improved the health for those 45 ~ 65 years. Regarding differences in place of residence, FDCS improved the health of rural residents more than that of urban residents overall. Regarding the presence of chronic disease, FDCS improved health improved the health of residents with chronic diseases than counterparts. See Table 5 for details.
Underlying mechanisms
S2 demonstrates the effect of FDCS on the mediation variables. S3 presents the effect of mediation variables on the health. See appendix for details. Table 6 shows the underlying mechanisms between FDCS and the health of middle-aged and older people. In terms of HR-QoL, the coefficient of FDCS increased after the inclusion of the mediation variable of healthcare service utilization (p < 0.05). This indicates that FDCS improved the health by reducing their healthcare service utilization. Regarding subjective well-being, the coefficient and significance level of FDCS increased after the inclusion of the mediation variables of healthcare service utilization (p < 0.01) and social activities (p < 0.05). This implies that FDCS improved health by reducing healthcare service utilization and increasing social activities. In addition, with respect to cognitive function, the coefficient for FDCS increased when the social activities variable was added (p < 0.01). This indicated that FDCS increased the cognitive function by guiding residents to increase social activities. See Table 6 for details.
Discussion
In this study, we found a positive association between FDCS and the health of middle-aged and older people in China. We used IV method to estimate and test the association, which may help to provide a robust and convincing result. Moreover, heterogeneity in the effect of FDCS was present according to age, residence, and presence of chronic diseases. Finally, we conducted a detailed mediation analysis and demonstrated that healthcare service utilization and social activities were important mediating factors.
Principal-agent theory can provide a possible explanation for the result that FDCS significantly improved most health outcomes. FDCS had a significant effect on HR-QoL. The results were similar to those found in the USA, Japan, and rural China18,33,34. In terms of the government, recently health system reforms tend to encourage initial contact with primary healthcare providers in China35, which may substantially affect health. Family doctors are incentivized by government regulation and market accountability in addition to government incentives36. As a result, motivated family doctors are committed to providing high-quality medical services, thus further improving the health. However, similar to another study17, we found no evidence that FDCS led to improvements in physical health. The possible explanation is that the coverage of welfare programs designed by the government only includes government employees rather than family doctors37. Therefore, family doctors with lower salary levels and unequal promotion systems38 often experience burnout39, resulting in low motivation to improve the physical health of middle-aged and older people. Acknowledged information asymmetry and thinking frameworks40 also influence family doctors’ decision-making on the physical health. In addition, one study showed that MCS is more related to HR-QoL than PCS41, and residents with poorer health are more motivated to participate in FDCS42. However, the older the person, the worse the health, the more time and effort family doctors need to improve PCS. The FDCS was implemented after 2016, so residents’ PCS may not be significantly improved in the short period of 2 years.
This study found a significant association between FDCS and subjective well-being. This can be explained by the fact that the government provides family doctors with comprehensive training to improve their skills, competence, and confidence, resulting in reduced dissatisfaction with local medical services among middle-aged and older people and alleviated healthcare inequality43, which in turn improves resident’ subjective well-being. Family doctors could provide better services to the population and maintain independence44. For example, they provide specialized treatment, increasing the continuity of care and reducing admission rates45, thus increasing their subjective well-being.
The results demonstrated that FDCS had a positive effect on the cognitive function of the population. However, previous studies concluded that family doctors are not effective in improving cognitive function due to low levels of knowledge and skills regarding dementia46. A possible explanation for this discrepancy is that the government trains family doctors in dementia care and requires them to provide dementia screening for the population47, which contributes to the early detection and prevention of cognitive impairment. In addition, family doctors showed generally positive attitudes towards people with dementia and put their dementia training into practice, educating and correcting residents’ and their families’ misconceptions about the disease to improve cognitive function.
The results were heterogeneous in terms of age, residence, and presence of chronic diseases. First, the impact of FDCS on health was greater for the population aged < 65 years than for individuals aged 45 ~ 65 years. Health was inversely related to age. Moreover, older people are prone to multiple chronic diseases, and patients with multiple chronic diseases and their family doctors have a higher rate of therapeutic inertia48, which has a negative impact on the health of older people. Second, the impact of FDCS on health was greater for the rural residents than for the urban residents. One possible explanation is that rural areas are often associated with a lack of sufficient and high-quality medical resources and qualified primary care providers49. Therefore, the effects of FDCS are more pronounced for the rural population than for the urban population. Third, FDCS had a greater positive impact on the health of patients with chronic diseases than those without. Family doctors provide targeted health management measures for patients with chronic diseases, such as the provision of chronic disease service packages, health knowledge promotion, and monitoring of health indicators to improve population health.
The mediation results showed that FDCS improved health by influencing healthcare service utilization and social activates. This can be explained by the fact that family doctors able to identify and address health risks in primary healthcare, reducing healthcare service utilization50and further improving health expectations of residents. In addition, FDCS can improve health through influencing resident’ social activities. The results support some previous studies investigating the relationship between various aspects of social relationships and health51,52. Family doctors provide a variety of health interventions, such as exercise guidance and psychological guidance, which could encourage residents to participate in social activities, increase exposure to an interactive environment, facilitate the early detection of cognitive decline, and improve their health.
This study also has several limitations. First, all the data were collected using a self-reporting approach, which may introduce recall bias. In addition, the availability of measured perspectives on population health was limited by the pre-specified questions in the survey, and we did not control for some potential unobserved confounding factors. Finally, this was a cross-sectional study, hence, the data may not be comprehensive enough to identify changes in the association.
Conclusion
FDCS played a positive role in improving the health of middle-aged and older people in China. The government should improve incentive-based initiatives to improve the quality of services and pay more attention to the health of middle-aged and older people. Moreover, more attention needs to be directed toward vulnerable groups, such as older individuals and those in rural China.
Data availability
This data was derived from the CHARLS. They are opened to everyone. Researchers who want to use these data can visit http://charls.pku.edu.cn/. We had added questionnaires content in the appendix.
References
Borders, T. F., Rohrer, J. E., Hilsenrath, P. E. & Ward, M. M. Why rural residents migrate for family physician care. J. Rural Health 16(4), 337–348. https://doi.org/10.1111/j.1748-0361.2000.tb00484.x (2000).
Velasco Garrido, M., Zentner, A. & Busse, R. The effects of gatekeeping: a systematic review of the literature. Scand. J. Prim. Health Care 29(1), 28–38. https://doi.org/10.3109/02813432.2010.537015 (2011).
Moore, A., Frank, C. & Chambers, L. W. Role of the family physician in dementia care. Can Fam Physician. 64(10), 717–719 (2018).
Guan, X., Lan, T., Liao, W., Wu, X. & Pan, J. Exploring the effect of the primary care health workers number on infectious diarrhea morbidity and where the health resources should go. Sci. Rep. 12(1), 6060. https://doi.org/10.1038/s41598-022-10060-y (2022).
Bindman, A. B. & Majeed, A. Primary care in the United States: Organisation of primary care in the United States. BMJ 326(7390), 631–634. https://doi.org/10.1136/bmj.326.7390.631 (2003).
Kozhimannil, K. B. & Westby, A. What family physicians can do to reduce maternal mortality. Am. Fam. Physician. 100(8), 460–546 (2019).
Phillips, R. L. Jr. et al. A Family Medicine Health Technology Strategy for Achieving the Triple Aim for US Health Care. Fam Med 47(8), 628–635 (2015).
Carter, R., Lévesque, J. F., Harper, S. & Quesnel-Vallée, A. Measuring the effect of Family Medicine Group enrolment on avoidable visits to emergency departments by patients with diabetes in Quebec Canada. J. Eval Clin. Pract. 23(2), 369–376. https://doi.org/10.1111/jep.12627 (2017).
Sohrabi, M. R., & Albalushi, R. M. Clients' satisfaction with primary health care in Tehran: A cross-sectional study on Iranian Health Centers. J Res Med Sci. 16(6), 756–762. (2011).
Lankarani, K. B., Alavian, S. M. & Haghdoost, A. A. Family physicians in Iran: Success despite challenges. Lancet 376(9752), 1540–1541. https://doi.org/10.1016/S0140-6736(10)62029-6 (2010).
Treharne, G. J., Carroll, R., Tan, K. K. H. & Veale, J. F. Supportive interactions with primary care doctors are associated with better mental health among transgender people: Results of a nationwide survey in Aotearoa/New Zealand. Fam. Pract. 39(5), 834–842. https://doi.org/10.1093/fampra/cmac005 (2022).
Shang, X. et al. Residents’ awareness of family doctor contract services, status of contract with a family doctor, and contract service needs in Zhejiang Province, China: A cross-sectional study. Int. J. Environ. Res. Public Health 16(18), 3312. https://doi.org/10.3390/ijerph16183312 (2019).
Statistical bulletin on the development of health care in China in 2021 https://www.gov.cn/xinwen/2022-07/12/content_5700670.htm, (2021).
National Health and Family Planning Commission: Transcript of the press conference of the National Health Council on 23 July 2021. http://www.nhc.gov.cn/xcs/s3574/202107/ea10acafc7d1493d820f6789c51cf571.shtml, 16 May 2024. (2021).
Wang, C. et al. Residents’ willingness to maintain contracts with family doctors: A cross-sectional study in China. J Gen. Intern. Med. 36(3), 622–631. https://doi.org/10.1007/s11606-020-06306-y (2021).
Qing-Yan, S. I. Challenges and solutions for training about contractual Services for on-site Primary Physicians before transferring to the position of family doctors. Chin. Gen. Pract. 7, 22 (2018).
Wang, L. & Liu, W. Effects of Family Doctor Contract Services on the Health-Related Quality of Life Among Individuals with Diabetes in China: Evidence From the CHARLS. Front Public Health https://doi.org/10.3389/fpubh.2022.865653 (2022).
Li, Z. et al. Family doctor contract services and health-related quality of life among patients with chronic diseases in rural China: What is the role of socioeconomic status?. Int. J. Equity Health 20(1), 191. https://doi.org/10.1186/s12939-021-01530-2 (2021).
Xu, C. et al. The Impact of a Family Doctor Contract Service on Outcomes for Type 2 Diabetes Patients in Zhejiang Province. Asia Pac. J. Public Health 34(6–7), 643–648. https://doi.org/10.1177/10105395221113778 (2022).
Lai, S. et al. The effects of family physician-contracted service on health-related quality of life and equity in health in China. Int. J. Equity Health 20(1), 15. https://doi.org/10.1186/s12939-020-01348-4 (2021).
Vera-Hernández, M. Structural estimation of a principal-agent model: Moral hazard in medical insurance. Rand. J. Econ. 34(4), 670–693 (2003).
Li, D., Su, M., Guo, X., Zhang, W. & Zhang, T. The effect of medical choice on health costs of middle-aged and elderly patients with chronic disease: Based on principal-agent theory. Int. J. Environ. Res. Public Health 19(13), 7570. https://doi.org/10.3390/ijerph19137570 (2022).
Langer, A., Schröder-Bäck, P., Brink, A. & Eurich, J. The agency problem and medical acting: an example of applying economic theory to medical ethics. Med. Health Care Philos. 12(1), 99–108. https://doi.org/10.1007/s11019-008-9138-y (2009).
Li, L., He, X. & Zhang, C. The impact of public policy of family doctor contracting on medical expenses from the perspective of residents at community level in China. Front. Psychol. https://doi.org/10.3389/fpsyg.2022.972904 (2023).
Buchanan, A. Principal/agent theory and decision making in health care. Bioethics 2(4), 317–333 (1988).
Hao, X., Yang, Y., Gao, X. & Dai, T. Evaluating the Effectiveness of the Health Management Program for the Elderly on Health-Related Quality of Life among Elderly People in China: Findings from the China Health and Retirement Longitudinal Study. Int. J. Environ. Res. Public Health 16(1), 113. https://doi.org/10.3390/ijerph16010113 (2019).
Zhao, L., Zhang, K., Gao, Y., Jia, Z. & Han, S. The relationship between gender, marital status and depression among Chinese middle-aged and older people: Mediation by subjective well-being and moderation by degree of digitization. Front. Psychol. https://doi.org/10.3389/fpsyg.2022.923597 (2022).
Olazarán, J. et al. Mild cognitive impairment and dementia in primary care: the value of medical history. Fam Pract. 28(4), 385–392. https://doi.org/10.1093/fampra/cmr005 (2011).
Ware, J., Snoww, K., Kosinski, M. A., & Gandek, B. G. SF-36. Health survey: manual and interpretation guide. Health Assess. Lab (1993).
Folstein, M. F., Folstein, S. E. & McHugh, P. R. Mini-mental state A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12(3), 189–198. https://doi.org/10.1016/0022-3956(75)90026-6 (1975).
Snyder, et al. Cocreative customer practices: effects of health care customer value cocreation practices on well-being. J. Bus. Res. https://doi.org/10.1016/j.jbusres.2016.07.006 (2017).
Baron, R. M. & Kenny, D. A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 51(6), 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173 (1986).
Arwert, H. J., Groeneveld, I. F., Vliet Vlieland, T. P. M. & Meesters, J. J. L. Health Care Use and Its Associated Factors 5–8 Years after Stroke. J. Stroke Cerebrovasc. Dis. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.104333 (2019).
Yokokawa, D. et al. Relationship between the presence of primary care physicians and health-related quality of life. J. Gen. Fam. Med. 23(2), 87–93. https://doi.org/10.1002/jgf2.490 (2021).
Zhou, Z. et al. Evaluating the effect of hierarchical medical system on health seeking behavior: A difference-in-differences analysis in China. Soc. Sci. Med. https://doi.org/10.1016/j.socscimed.2020.113372 (2021).
Xu, X., Zhou, L., Ampon-Wireko, S. & Quansah, P. E. Assessing the mediating role of motivation in the relationship between perceived management support and perceived job satisfaction among family doctors in Jiangsu province China. Hum. Resour. Health 21(1), 71. https://doi.org/10.1186/s12960-023-00849-x (2023).
Li, X. et al. The primary health-care system in China. Lancet 390(10112), 2584–2594. https://doi.org/10.1016/S0140-6736(17)33109-4 (2017).
Wang, A. et al. How surface acting affects turnover intention among family doctors in rural China: The mediating role of emotional exhaustion and the moderating role of occupational commitment. Hum. Resour. Health 21(1), 3. https://doi.org/10.1186/s12960-023-00791-y (2023).
Ye, J. et al. Burnout among obstetricians and paediatricians: A cross-sectional study from China. BMJ Open https://doi.org/10.1136/bmjopen-2018-024205 (2019).
Arrow, K. J. Uncertainty and the welfare economics of medical care. Bull. World Health Organ. 82(2), 141–149 (2004).
Sarvimäki, A. & Stenbock-Hult, B. Quality of life in old age described as a sense of well-being, meaning and value. J. Adv. Nurs. 32, 1025–1033. https://doi.org/10.1046/j.1365-2648.2000.01568.x (2000).
Yang, S. et al. Do older people with cardiovascular-metabolic multimorbidity prefer to sign contracts for family doctor services? Evidence from a cross-sectional study in rural Shandong China. BMC Geriatr. 21(1), 579. https://doi.org/10.1186/s12877-021-02543-w (2021).
Huang, S., Yin, A., Liu, Q. & Sun, X. Can the implementation of family doctor contracted service enable the elderly to utilize primary health care services more equally? empirical evidence from Shandong China. BMC Prim Care. 23(1), 31. https://doi.org/10.1186/s12875-022-01630-0 (2022).
Sabbah, I., Drouby, N., Sabbah, S., Retel-Rude, N. & Mercier, M. Quality of life in rural and urban populations in Lebanon using SF-36 health survey. Health Qual. Life Outcomes. 1, 30. https://doi.org/10.1186/1477-7525-1-30 (2003).
Sutarsa, I. N., Kasim, R., Slimings, C., Bain-Donohue, S. & Barnard, A. Effects of employing primary care doctors in hospital to improve the quality of care and health outcomes of rural patients: A systematic scoping review. Aust. J. Rural Health. 29(4), 492–501. https://doi.org/10.1111/ajr.12779 (2021).
Wang, M. et al. Knowledge, attitudes and skills of dementia care in general practice: A cross-sectional study in primary health settings in Beijing China. BMC Fam. Pract. 21(1), 89. https://doi.org/10.1186/s12875-020-01164-3 (2020).
Wang, M. et al. The needs of informal caregivers and barriers of primary care workers toward dementia management in primary care: A qualitative study in Beijing. BMC Fam. Pract. 19(1), 201. https://doi.org/10.1186/s12875-018-0890-7 (2018).
Man, F. Y., Chen, C. X., Lau, Y. Y. & Chan, K. Therapeutic inertia in the management of hyperlipidaemia in type 2 diabetic patients: A cross-sectional study in the primary care setting. Hong Kong Med. J. 22(4), 356–364. https://doi.org/10.12809/hkmj154667 (2016).
Chen, C., Xu, R. H., Wong, E. L. & Wang, D. The association between healthcare needs, socioeconomic status, and life satisfaction from a Chinese rural population cohort, 2012–2018. Sci. Rep. 12(1), 14129. https://doi.org/10.1038/s41598-022-18596-9 (2022).
Sawicki, O. A. et al. Strong and sustainable primary healthcare is associated with a lower risk of hospitalization in high risk patients. Sci. Rep. 11(1), 4349. https://doi.org/10.1038/s41598-021-83962-y (2021).
Kuiper, J. S. et al. Social relationships and risk of dementia: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res. Rev. 22, 39–57. https://doi.org/10.1016/j.arr.2015.04.006 (2015).
Evans, I. E. M., Martyr, A., Collins, R., Brayne, C. & Clare, L. Social isolation and cognitive function in later life: A systematic review and meta-analysis. J. Alzheimers Dis. 70(s1), S119–S144. https://doi.org/10.3233/JAD-180501 (2019).
Acknowledgements
We would like to acknowledge the CHARLS team for providing the data.
Funding
This study was funded by the National Natural Science Foundation of China (72164031&72204128). The funding bodies had no role in the design of the study or collection, analysis, and interpretation of data, and they did not contribute to the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
WZ participated in the study design, data analysis and interpretation, and was the primary person responsible for drafting the manuscript. MS contributed to study design, data analysis, and reviews. DL conceived of the study design, participated in data analysis, and revision. FY and ZL participated in revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, W., Su, M., Li, D. et al. The association between family doctor contract services and the health of middle-aged and older people in China: an instrumental variables analysis. Sci Rep 14, 16229 (2024). https://doi.org/10.1038/s41598-024-65621-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-65621-0
This article is cited by
-
Impact of family doctor contracted services on the health of migrants: a cross-sectional study in China
Scientific Reports (2024)
