
Abstract
The October 29, 2022, Seoul Halloween Crowd Crush (SHCC) caused the loss of 159 lives, making it the deadliest global mass-gathering disaster between 2018 and 2022. Despite the fact that years have passed since the incident, there remains a significant gap in research addressing the mental health of citizens to evaluate their recovery progress. Therefore, in this study, a survey was conducted to assess citizens’ anxiety, depression, post-traumatic stress disorder (PTSD), and well-being after the SHCC. The data were analyzed using t-tests, analysis of variance (ANOVA), correlations, a Kruskal–Wallis test, and post hoc tests. The citizens' well-being differed significantly by victimization status, with direct victims showing languishing well-being (p = .036). PTSD severity level was higher in victims and direct witnesses (p < .001). Victims and direct witnesses exhibited worse outcomes in subjective, social, and psychological well-being as well as in PTSD (p < .001). Well-being exhibited a significant negative correlation with PTSD (r = − .247, p < .001). The results of the analysis suggest the SHCC’s psychological impact has endured not only for victims and direct witnesses but also for media-exposed citizens. Offering continuous psychological support and fostering positive self-perceptions and social interactions are crucial for their recovery and well-being enhancement.
Similar content being viewed by others
Introduction
On October 29, 2022, a catastrophic incident known as the Seoul Halloween Crowd Crush (SHCC) occurred in Itaewon, a commercial district located in the heart of Seoul, South Korea’s capital city. This tragic episode resulted in the loss of 159 precious lives, the highest death toll of any global mass-gathering disaster between the years 2018 and 20221,2. Regrettably, this tragedy was indiscriminately broadcast with unfiltered content through social network services (SNSs)3. Moreover, the tragedy was politicized, shifting the blame to “the individuals who were present” rather than the deficiencies in the social safety net, thereby making the victims and survivors targets of abuse and slander4. In this atmosphere, the tragedy became traumatizing for both survivors and those who experienced it indirectly.
Notably, human-caused disasters such as the SHCC are associated with greater psychological distress than natural disasters5,6. Such disasters can impair mental health, for example, by increasing levels of stress, substance abuse, anxiety, and depression and even developing into post-traumatic stress disorder (PTSD)5,7,8. Moreover, the primary model of PTSD involves memory processing and biological brain changes triggered by threats to one's life or well-being9. Therefore, a comprehensive understanding of an individual's well-being is crucial for addressing the psychological aftermath of such disasters.
Well-being is a multifaceted concept applied in various fields to depict a state of health and happiness, including positive emotions (e.g., contentment, joy), negative emotions (e.g., depression, anxiety), satisfaction with life, fulfillment, and positive functioning10,11, and it can be categorized into subjective, psychological, and social well-being12,13. Subjective well-being refers to positive emotions and life satisfaction. Psychological well-being is characterized by high levels of self-acceptance, positive relationships with others, personal growth, purpose in life, environmental mastery, and individual autonomy14. Finally, social well-being refers to one's assessment of the functioning of the society in which they are embedded12.
In addition, mental health can be distinguished in terms of its presence or absence12,13. Regarding the former, flourishing is defined as the presence of mental health and a state in which an individual feels positive about life and functions well psychologically and socially, while languishing represents the opposite condition. Flourishing refers to well-being, goes beyond recovery to indicate an individual’s return to their baseline psychological state, and is an important concept related to psychological resilience15. Because the SHCC was framed as an accident that occurred with partygoers and was caused by an individual's carelessness, the survivors' interpersonal relationships and emotions were likely affected. Therefore, understanding their subjective, psychological, and social well-being following the SHCC is crucial for their mental health recovery.
According to the DSM-516 diagnostic criteria, a person can develop PTSD after experiencing or being exposed to a traumatic event that involves actual or threatened death, serious injury, or harm. This can include directly experiencing the event, witnessing it in person, or learning that it happened to a close friend or family member17. PTSD is strongly associated with negative emotions such as anxiety, depression, and loss18,19. Symptoms usually appear within 3 months of the traumatic event, but for some people, it may take years20, and it can have a significant impact on an individual's life. Therefore, early intervention is critical. The SHCC was a catastrophic human-caused disaster without warning, and the escalating death toll and the indiscriminate dissemination of the scene through the media traumatized not only those who were present but also those who experienced it indirectly. Therefore, it is necessary to identify PTSD in the citizens who were exposed to the tragedy.
Furthermore, understanding the mental health recovery stages post-disaster is imperative. PTSD can have an acute onset within 6 months of a traumatic experience, and around a quarter of individuals may experience delayed PTSD onset more than 6 months after the traumatic event21,22. Moreover, by the 12-month mark, trauma anniversary reactions may occur, leading to the temporary intensification of the trauma23,24,25. Despite the fact that years have passed since the SHCC, there remains a significant gap in research addressing the mental health of citizens to evaluate their recovery progress. Although well-being is crucial, research on post-disaster mental health has primarily focused on PTSD, anxiety, and depression.
Purpose
The purpose of this study is to evaluate mental health, especially in terms of well-being and SHCC-related PTSD, among South Korean citizens after the SHCC.
Method
Participants
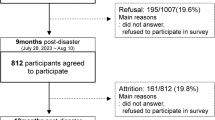
The cross-sectional study comprised participants aged 19–69 years from South Korea who voluntarily agreed to participate and demonstrated an understanding of the purpose and procedures. To ensure a representative sample of mental health among citizens, all those who expressed a willingness to participate in the survey were included, resulting in a total of 1017 participants.
Measures
(a) General characteristics
General characteristics were defined as characteristics related to trauma, including gender, age, alcohol consumption, and SHCC victim/witness status. Traumatic experiences can lead to a loss of control of alcohol consumption, that is, dysregulated drinking26. Moreover, media (indirect) exposure to trauma is associated with several adverse effects such as PTSD, depression, and anxiety27,28. This study also included a question about the respondents’ awareness of the SHCC to ensure that all respondents had been exposed to it either directly or indirectly. Therefore, the items indicating whether the respondent had been a witness to the SHCC were separated into two categories representing “direct” and “indirect” witnesses.
(b) Well-being
The Korean version of the Mental Health Continuum Short Form (K-MHC-SF)29,30 was used. The survey consists of 14 items rated on a 6-point Likert scale from “Never” (0) to “Every day” (5) that measure subjective, social, and psychological well-being. Scores range from 0 to 70, with higher scores indicating higher levels of mental well-being. The MHC tool categorizes well-being based on selected items rather than using cut-off scores to differentiate the severity of mental health. These categories—flourishing, moderately mentally healthy, and languishing—were utilized in the present study.
Flourishing is characterized by high ratings on at least one of the three subjective well-being items and high ratings on at least six psychological and social well-being items, while languishing is characterized by low ratings on at least one of the subjective well-being items and low ratings on at least six psychological and social well-being items. Scores falling outside of these criteria indicate that the respondent is moderately mentally healthy. In a previous study, the reliability for the total was indicated by a Cronbach's alpha value of 0.93, with subscale reliabilities of 0.88 for subjective, 0.90 for social, and 0.81 for psychological 29. In the present study, the overall reliability was indicated by a Cronbach's alpha value of 0.95, with subscale reliabilities of 0.93 for subjective, 0.87 for social, and 0.93 for psychological.
(c) PTSD
The Korean version of the Impact of Event Scale-Revised (IES-R-K)31,32 was used. The scale comprises 22 questions rated on a 5-point Likert scale from “Not at all” (0) to “Very much” (4) to assess PTSD symptoms over the past week. The total score range is 0–88, with higher scores indicating higher PTSD severity. The scale consists of four subscales: hyperarousal, avoidance, intrusion, and sleep disturbances & numbness. Scores up to 17 are considered normal, 18–24 are considered low-risk, and 25 and above are considered high-risk. The Cronbach's alpha values were 0.93 in a previous study31 and 0.96 in this study.
(d) Anxiety
The Korean version of the Generalized Anxiety Disorder 7 (K-GAD-7)33,34 was used. This scale includes seven items rated on a 4-point Likert scale from “Not at all” (0) to “Nearly every day” (3) with a score range of 0–21. Scores of 0–4 are categorized as normal, while scores of 5–9, 10–14, and 15–21 are categorized as mild, moderate, and severe anxiety, respectively. The reliability was indicated by Cronbach’s alpha values of 0.9134 in a previous study and 0.93 in the present study.
(e) Depression
The Patient Health Questionnaire-9 (PHQ-9) scale35,36 was used. The scale comprises nine items rated on a 4-point Likert scale from “Not at all” (0) to “Nearly every day” (3) with a total score range of 0–27 points. Scores of 0–4 are considered normal, while scores of 5–9 , 10–19, and 20–27 are considered to reflect mild, moderate, and severe depression, respectively. The reliability of the scale was indicated by Cronbach's alpha values of 0.81 in a previous study35 and 0.92 in this study.
Data collection
An online survey was conducted for five days, from July 28 to August 1, 2023, through a survey company (Korea Research Co.). The survey took approximately 15 min to complete.
Data analysis
Data analysis was performed using SPSS Statistics for Mac, version 29.0.2.0. Effect sizes were measured using Cohen's d, which was calculated using the R programming language (version 4.4.1; R Core Team, 2024). General characteristics and mental health variables were analyzed using mean and standard deviation, independent t-tests, and analysis of variance (ANOVA). Tukey’s HSD (honestly significant difference) test was used as a post hoc test. Normality was assessed using the Shapiro–Wilk test. However, differences between victims were analyzed using the Kruskal–Wallis test, and post hoc tests were performed using the Mann–Whitney U test. Pearson's correlation was used to analyze the correlation among well-being, PTSD, anxiety, and depression. Differences in total and subscale scores for well-being and PTSD between victims and witnesses were tested using independent t-tests. Cronbach's alpha values determined the reliability of all scales.
Bias
The question "Do you understand that this survey is specifically about the Seoul Halloween crowd crush?" was asked to ensure that the survey was focused on SHCC-related trauma and, therefore, free from any external bias that may have arisen from another trauma event. This question helped to gather accurate and reliable data to better understand the impact of the SHCC.
Results
General characteristics and mental health variables
Significant differences in well-being were found by gender (p < 0.001) (Table 1). By age, those aged 40–59 years had significantly higher PTSD scores than those aged 19–29 years (p = 0.003). Regarding alcohol, the group that increased their consumption had the lowest well-being scores and significantly higher PTSD, anxiety, and depression scores (p < 0.001). There were no significant differences in mental health in terms of general characteristics variables between direct and indirect victims (e.g., those whose family members, relatives, or acquaintances were victimized). Still, both groups had significantly higher PTSD, anxiety, and depression (p < 0.001) and lower well-being (p = 0.007) scores than non-victims. Regarding SHCC witnesses, those who witnessed it firsthand (directly) had significantly lower well-being scores (p = 0.003) and higher PTSD, anxiety, and depression (p < 0.001) scores than those who only heard about it through the media (indirectly).
Differences in well-being status and PTSD severity according to victim/witness status
In the following analyses, direct and indirect victims were both considered victims (Yes). PTSD severity was significantly associated with both being a victim and being a witness, being high in victims and direct witnesses (p < 0.001) (Fig.1). Moreover, among victims, 81.5% were at high risk for PTSD, while 4.6% scored normal. Conversely, among non-victims, 59.7% scored normal, while 28.5% were still at high risk for PTSD. Among direct witnesses who experienced the crush firsthand, 91.7% were at high risk for PTSD. In contrast, those who had indirectly witnessed the crush via the media had the highest proportion of normal scores at 56.7%. However, similar to non-victims, 31.1% of indirect witnesses were also at high risk for PTSD. Victims exhibited significantly poorer well-being status than non-victims, indicating that well-being status differed significantly depending on whether the respondent was a victim or non-victim (p = 0.036) (Fig.1). In the victim category, 50.8% were categorized as languishing and only 4.6% as flourishing. For non-victims, 39.0% were categorized as languishing and 14.8% as flourishing, the latter proportion being nearly three times higher than that for victims. There was no significant difference in well-being between direct and indirect witnesses (p = 0.062).

Differences in well-being status and PTSD severity according to victim/witness.
Differences in well-being subfactors and PTSD according to victim/witness status
Victims and direct witnesses exhibited worse outcomes in all items of well-being and its subfactors (subjective, social, and psychological) (p < 0.001) (Table 2). Specifically, direct witnesses scored 7.33 ± 4.09 in psychological well-being, while indirect witnesses scored 13.14 ± 6.79, indicating nearly a twofold difference. Both victims and direct witnesses showed significantly higher PTSD and PTSD subfactor (hyperarousal, avoidance, intrusion, and sleep disturbances & numbness) scores than indirect witnesses (p < 0.001). Direct witnesses had a mean PTSD score of 42.33 ± 13.31, more than twice that of non-victims and indirect witnesses. Hyperarousal and avoidance showed especially high scores among victims and direct witnesses (p < 0.001).
Correlations among well-being, PTSD, anxiety, and depression
Well-being exhibited significant negative correlations with PTSD, anxiety, and depression, showing medium effect sizes for anxiety and depression (r = − 0.451 to − 0.247, p < 0.001) (Table 3). PTSD showed positive correlations with anxiety and depression, with large effect sizes (r = 0.592 to 0.596, p < 0.001).
When well-being was examined according to its subfactors, subjective, social, and psychological well-being were significantly negatively correlated with PTSD, anxiety, and depression (r = − 0.489 to − 0.190, p < 0.001). All subfactors showed medium effect sizes for depression (r = − 0.489 to − 0.369), whereas social well-being exhibited a small effect size for PTSD (r = − 0.190).
Discussion
The present study examined the mental health of South Korean citizens who experienced the SHCC on October 29, 2022, focusing on well-being and PTSD. The SHCC left 159 victims, many of whom witnessed it with their own eyes. The lamentations of victims and witnesses have largely been suppressed37. Moreover, based on the present research's results, it is evident that they have not yet recovered mentally. The findings suggest four points of discussion.
First, the mental health differences by the general characteristics of alcohol consumption and age revealed the unique features of the SHCC. In particular, alcohol consumption was associated with significantly lower well-being and higher anxiety and depression. Traumatized people tend to experience impairment in terms of alcohol use that may lead to alcohol use disorder26,38. In the present study, however, PTSD scores were significantly higher for individuals who consumed less alcohol. This result may be due to the specific context of the SHCC: when the crush occurred, terms such as “party,” “drink,” and “drugs” were emphasized. The 2022 Halloween event was the first in 3 years following the COVID-19 suspension. However, from 2018 to 2022, drug offenses among Koreans in their 30s increased by 109%, leading to an intensive crackdown on drugs39. Consequently, victims' drug use, partying, and drinking were highlighted as causes of the SHCC. For example, a local councilor posted messages such as, "Weren’t they foolish to go to Itaewon that night? Should we even care about people who were there just to have fun? Incidents like this can't happen without drugs being involved4". This atmosphere led citizens with SHCC-related PTSD to consciously avoid alcohol. Next, in terms of age, victims of the SHCC were mainly young adults; however, PTSD scores were significantly higher for those aged 40–59 than for those aged 19–29. This finding that PTSD was more severe in the older generation than in those within the same age group as the victims is unusual, and it is likely attributable to the fact that the parents of the SHCC victims were in the 40–59 age range.
Second, the well-being and PTSD severity results indicated that most of the victims and witnesses were still in poor condition, meaning they remained affected by the crush despite the time that had passed. Specifically, half of the victims (50.8%) were languishing, and the majority were at high risk for PTSD (81.5%). Similarly, 75% of the direct witnesses were languishing, and 90% were at high risk for PTSD, whereas only 8.3% were considered normal. The total well-being score and those for subjective, social, and psychological well-being were significantly low in both victims and direct witnesses.
In particular, the low subjective well-being scores could be attributed to the personal responsibility attached to the SHCC. After the SHCC, some of the public formed the opinion that certain individuals and a general lack of order caused the disaster. A survey conducted by Korea Gallup, a credible survey organization, confirmed that 14% of people believed the crush was the fault of certain individuals40. The argument of personal responsibility made the victims of the tragedy feel that they were responsible for their suffering, which led to feelings of guilt and remorse for victims and witnesses and resulted in negative emotions such as anxiety and depression. According to a meta-analysis, trauma-related guilt has important clinical implications for the onset and persistence of PTSD symptoms41. Negative perceptions and feelings about oneself can affect one's relationships with others, affecting psychological well-being, which refers to one's communication and interaction with others14,42. The guilt stemming from the SHCC resulted in not only emotional isolation but also isolation from others. Furthermore, this condition can lead to a negative perception of society, which results in low social well-being.
Moreover, the total PTSD scores and all the PTSD subfactor scores were significantly high in both victims and direct witnesses, showing the most significant gap in the avoidance subfactor. This also demonstrates the SHCC's uniqueness. According to the meta-analysis of19, avoidance has a substantial association with PTSD. Moreover, more specific events are more traumatizing. As the SHCC happened at a very specific place and time, it can easily stimulate their memory and arouse their trauma. In short, the victims and direct witnesses are at high risk of suffering from lingering traumatic memories, which highlights the urgent need for psychological support to help them overcome their trauma.
Third, continuous monitoring with psychological support for witnesses as well as victims is essential to decrease PTSD and enhance well-being. According to most guidelines, the primary recommended treatment for PTSD is psychotherapy43. The direct and indirect witness groups had significantly higher PTSD, anxiety, and depression scores and lower well-being scores than non-victims. Moreover, the direct witnesses reported significantly higher scores for PTSD, anxiety, and depression than the indirect witnesses. However, while the media witnesses’ PTSD scores indicated that they were at high risk for PTSD, their anxiety and depression scores were at normal levels. This result suggests the possibility of public indirect trauma related to the SHCC. Notably, when the SHCC occurred, the scene was broadcast through a personal SNS, and the people in the crush livestreamed the event without censorship. As a result, there was no gatekeeper to protect people from witnessing the pain and death44. This kind of media exposure might have aroused indirect trauma in the people who watched it, as experiencing disasters through the media is also traumatic45,46. Therefore, to promote well-being and relieve PTSD, monitoring mental status and providing psychological support are vital not only for the victims but also for those who were exposed to the media coverage of the event.
Finally, significant negative correlations were found among well-being, PTSD, anxiety, and depression, providing clues as to how to promote citizens’ mental health. Similarly, all the well-being subfactors were found to have negative correlations with PTSD, anxiety, and depression. In particular, the correlations between subjective well-being, PTSD, anxiety, and depression suggest that helping individuals express and evaluate their emotions positively can help alleviate PTSD, anxiety, and depression. Symptoms of PTSD contribute to the erosion of self-perceptions, which implies that increasing positive self-perceptions and emotions can help reduce PTSD47. PTSD is closely linked to adverse emotional states, including anxiety and depression18,19. Victims may feel guilty for being there or being unable to save others; therefore, it is necessary to help them feel positive emotions instead of trauma-related guilt. Moreover, the psychological well-being aspect of well-being suggests that interactions may help people overcome SHCC-related PTSD. Interactions with others can help alleviate PTSD by reducing anxiety and depression, allowing people to experience psychological recovery. One notable example is self-help groups, which are informal groups that provide mutual support and help individuals get organized and act. These groups are effective in dealing with PTSD and community rehabilitation48,49. Social interactions may also help promote victims’ social well-being. As the victims and direct witnesses of the crush may have felt like they had no choice but to choose isolation to avoid negative social framing, they must be able to form self-help groups where they can share their trauma and memories to improve their well-being and recover from SHCC-related PTSD.
Conclusion
The psychological impact of the SHCC has endured not only for victims and direct witnesses but also for the media-exposed citizens who witnessed it indirectly. These citizens report low well-being and are at high risk for PTSD, and they need ongoing monitoring as well as psychological support to alleviate PTSD and promote well-being. Concerning this point, offering continuous psychological support and fostering positive self-perceptions and social interactions are crucial for their recovery and well-being enhancement.
Implications and limitations
Regarding limitations, this study was conducted on ordinary citizens, which limited its ability to represent those who were greatly affected by the SHCC. Moreover, because victims/direct witnesses were not intentionally recruited, the study included only 10 direct victims and 12 direct witnesses, leading to an unbalanced sample. Additionally, since the study was conducted through a survey company, participants may have been motivated by compensation. Lastly, it was challenging to control for exogenous variables such as life stress.
Future research should focus on conducting qualitative studies to explore the experiences of these individuals since the disaster, aiming to assist them in their recovery. Ultimately, despite these limitations, the present study examined the mental health of citizens who experienced the SHCC before the first anniversary of its occurrence to identify their needs and inform the future direction of psychological support.
Data availability
Data are available upon reasonable request. Please contact the corresponding author for data requests.
References
Ministry of the Interior and Safety. Ministry of the Interior and Safety, Disaster Safety Management Headquarters Itaewon Incident Briefing. https://www.mois.go.kr/frt/bbs/type010/commonSelectBoardArticle.do?bbsId=BBSMSTR_000000000008&nttId=96678 (2022).
Sharma, A. et al. Global mass gathering events and deaths due to crowd surge, stampedes, crush and physical injuries—Lessons from the Seoul Halloween and other disasters. Travel Med. Infect. Dis. 52, 102524 (2023).
Yeung, J. & Rebane, T. ‘Somebody is going to die’: How Seoul’s deadly Halloween crush unfolded. In CNN (2022).
Kim, J. Y. Mourning for Itaewon Halloween tragedy. Inter-Asia Cult. Stud. https://doi.org/10.1080/14649373.2023.2209439 (2023).
Makwana, N. Disaster and its impact on mental health: A narrative review. J. Fam. Med. Prim. Care 8, 12 (2019).
Sederer, L. I. Are human made disasters different?. Epidemiol. Psychiatr. Sci. https://doi.org/10.1017/S2045796011000710 (2012).
Aten, J. D. et al. The psychological study of religion and spirituality in a disaster context: A systematic review. Psychol. Trauma 11, 34 (2019).
First, J. M. Post-traumatic stress and depression following disaster: Examining the mediating role of disaster resilience. Front. Public Health 12, 13 (2024).
Hobfoll, S. E., Gaffey, A. E. & Wagner, L. M. PTSD and the influence of context: The self as a social mirror. J. Pers. 88, 11 (2020).
CDC. Well-being concepts | HRQOL | CDC. Well-Being Concepts 1–1. Preprint https://www.cdc.gov/hrqol/wellbeing.htm (2018).
Chutiyami, M. et al. COVID-19 pandemic and overall mental health of healthcare professionals globally: A meta-review of systematic reviews. Front. Psychiatry. https://doi.org/10.3389/fpsyt.2021.804525 (2022).
Keyes, C. L. M. The mental health continuum: From languishing to flourishing in life. J. Health Soc. Behav. 43, 103 (2002).
Keyes, C. L. M. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 73, 7 (2005).
Ryff, C. D. & Keyes, C. L. M. The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 69, 34 (1995).
Tay, P. K. C. & Lim, K. K. Psychological resilience as an emergent characteristic for well-being: A pragmatic view. Gerontology. https://doi.org/10.1159/000509210 (2020).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Publishing, 2013).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. https://doi.org/10.1176/appi.books.9780890425596 (American Psychiatric Association, 2013).
National Institute of Mental Health. Post-Traumatic Stress Disorder.
Miethe, S., Wigger, J., Wartemann, A., Fuchs, F. O. & Trautmann, S. Posttraumatic stress symptoms and its association with rumination, thought suppression and experiential avoidance: A systematic review and meta-analysis. J. Psychopathol. Behav. Assess. https://doi.org/10.1007/s10862-023-10022-2 (2023).
Samhsa,. TIP 57: Trauma informed care in behavioral health services, a review of the literature. J. Can. Acad. Child Adolesc. Psychiatry 23, 45 (2014).
Serra, R. et al. Post-traumatic stress disorder trajectories the year after COVID-19 hospitalization. Int. J. Environ. Res. Public Health 19, 21 (2022).
Smid, G. E., Mooren, T. T. M., Van Der Mast, R. C., Gersons, B. P. R. & Kleber, R. J. Delayed posttraumatic stress disorder: Systematic review, meta-analysis, and meta-regression analysis of prospective studies. J. Clin. Psychiatry https://doi.org/10.4088/JCP.08r04484 (2009).
Chow, A. Y. M. Anticipatory anniversary effects and bereavement: Development of an integrated explanatory model. J. Loss Trauma 15, 20 (2010).
Kim, E. J. et al. A retrospective and prospective follow-up study of psychological distress in the Danwon High School survivors of the Sewol ferry disaster. Psychiatry Investig. 15, 22 (2018).
Bruce, M. J. & Matsuo, H. “Burned into my brain:” Trauma anniversary reactions examined from a qualitative perspective. J. Loss Trauma 27, 101 (2022).
Patock-Peckham, J. A. et al. Dimensions of childhood trauma and their direct and indirect links to PTSD, impaired control over drinking, and alcohol-related-problems. Addict. Behav. Rep. 12, 722 (2020).
Houston, J. B., Spialek, M. L. & First, J. Disaster media effects: A systematic review and synthesis based on the differential susceptibility to media effects model. J. Commun. 68, 4 (2018).
Astill Wright, L. et al. Associations among psychosis, mood, anxiety, and posttraumatic stress symptoms: A network analysis. J. Trauma Stress 36, 2 (2023).
Lim, Y., Ko, Y., Shin, H. & Cho, Y. Psychometric evaluation of the Mental Health Continuum-Short Form (MHC-SF) in South Koreans. Korean J. Psychol. Gen. 31, 369–386 (2012).
Keyes, C. L. M. et al. Evaluation of the mental health continuum-short form (MHC-SF) in Setswana-speaking South Africans. Clin. Psychol. Psychother. 15, 181 (2008).
Lim, H. K. et al. Reliability and validity of the Korean version of the impact of event scale-revised. Compr. Psychiatry 50, 385 (2009).
Weiss, D. S. The impact of event scale: Revised. In Cross-Cultural Assessment of Psychological Trauma and PTSD. 219–238 https://doi.org/10.1007/978-0-387-70990-1_10 (Springer 2007).
Spitzer, R. L., Kroenke, K., Williams, J. W. & Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166, 38 (2006).
Seo, J. G. & Park, S. P. Validation of the Generalized Anxiety Disorder-7 (GAD-7) and GAD-2 in patients with migraine. J. Headache Pain 16, 33 (2015).
Park, S.-J., Choi, H.-R., Choi, J.-H., Kim, K. & Hong, J. P. Reliability and validity of the Korean version of the Patient Health Questionnaire-9 (PHQ-9). Anxiety Mood 6, 629 (2010).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 73 (2001).
Lee, H.-E. Social disaster and death of others: Why was the pain and death of the Itaewon disaster excluded from daily life?. Korean Assoc. Cult. Stud. 11, 23–41 (2023).
Sonnier, H., Alex Brake, C., Flores, J. & Badour, C. L. Posttraumatic stress and hazardous alcohol use in trauma-exposed young adults: Indirect effects of self-disgust. Subst. Use Misuse 54, 13 (2019).
Koh, Y.-S. Suggestions to improve treatment rehabilitation systems for drug abusers in Korea. Corr. Welf. Soc. Korea 84, 1–27 (2023).
Korean Gallup. Gallup Korea Daily Opinion (G20221111). https://www.gallup.co.kr/gallupdb/reportContent.asp?seqNo=1338 (2022).
Kip, A., Diele, J., Holling, H. & Morina, N. The relationship of trauma-related guilt with PTSD symptoms in adult trauma survivors: A meta-analysis. Psychol. Med. https://doi.org/10.1017/S0033291722001866 (2022).
Blasco-Belled, A. & Alsinet, C. The architecture of psychological well-being: A network analysis study of the Ryff Psychological Well-Being Scale. Scand. J. Psychol. 63, 75 (2022).
Merians, A. N., Spiller, T., Harpaz-Rotem, I., Krystal, J. H. & Pietrzak, R. H. Post-traumatic stress disorder. Med. Clin. N. Am. https://doi.org/10.1016/j.mcna.2022.04.003 (2023).
Hong, S.-C. Social media and the media in the wake of the Itaewon tragedy. Kwanhun J. 65, 50–58 (2023).
Pfefferbaum, B., Palka, J. M. & North, C. S. Associations between news media coverage of the 11 September attacks and depression in employees of New York city area businesses. Behav. Sci. 11, 25 (2021).
Neria, Y. & Sullivan, G. M. Understanding the mental health effects of indirect exposure to mass trauma through the media. JAMA 306, 1374–1375. https://doi.org/10.1001/jama.2011.1358 (2011).
Keshet, H., Foa, E. B. & Gilboa-Schechtman, E. Women’s self-perceptions in the aftermath of trauma: The role of trauma-centrality and trauma-type. Psychol. Trauma 11, 86 (2019).
Lewis, C. E. et al. Internet-based guided self-help for posttraumatic stress disorder (PTSD): Randomized controlled trial. Depress. Anxiety 34, 4 (2017).
World Health Organization. Community-Based Rehabilitation: CBR Guidelines. (World Health Organization, 2010).
Acknowledgements
The researchers are grateful to the citizens who participated in the study and to Korea Research Co. for their assistance in data collection.
Funding
This research was supported by a National Research Foundation of Korea grant funded by the Korean government (2023R1A2C2003043).
Author information
Authors and Affiliations
Contributions
The authors’ contributions to the paper were as follows: Y.J. was responsible for the study's conception and design. Both Y.J. and H.I. contributed to the data collection. Y.J. and H.I. carried out the analysis and interpretation of the results. H.I. prepared the draft manuscript and produced the figures and tables. Both authors reviewed the results and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical considerations
This study was approved by the C University Ethics Committee (IRB No. 1041078-20221129-HR-019) and was conducted in accordance with the Declaration of Helsinki. The researchers explained the study to the participants. Informed consent was obtained from all the study participants. The participants were informed that their data would be used solely for research purposes and that anonymity and confidentiality would be maintained. Moreover, they were informed that they could withdraw their participation at any time without penalty. Participants were compensated through the survey company.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Choi, YJ., Namgung, HI. Still in there—citizens’ well-being and PTSD after Seoul Halloween crowd crush in Korea: a cross-sectional study. Sci Rep 14, 20537 (2024). https://doi.org/10.1038/s41598-024-71631-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-71631-9
