
Abstract
Increasing studies have investigated the link between physical activity (PA) and sedentary behavior with venous thromboembolism (VTE) but the existing findings are not consistent and the independent relationship is uncertain. This meta-analysis aimed to comprehensively assess the shape of dose-response relationship between PA and sedentary behavior with VTE and further explore whether the relationship is independent after mutual adjustment. We systematically searched PubMed, Embase and Web of Science from inception to August 1, 2024. PA exposures were converted into MET-h/wk. Categorical meta-analyses and a cubic spline model were performed to evaluate the association between PA, sedentary behavior and VTE. Twenty-five articles including 31 studies were included. A curvilinear dose-response relationship between PA and VTE was observed, with steeper gradients even at lower PA levels. After adjustment for sedentary behavior, higher level of PA was independently associated with a reduced VTE risk (OR = 0.83, 95%CI:0.77–0.89). Based on population attributable fraction analyses, 2.37% (95%CI: 1.90-2.85%) of incident VTE could have been prevented if all adults had achieved half the PA minimum recommended level. A linear dose-response relationship between sedentary behavior and VTE risk was found, and there was a 2% higher risk of VTE (OR = 1.02, 95%CI: 1.00-1.03) for 1 h increment of sedentary behavior per day. After adjustment for PA, sedentary behavior was independently associated with an increased VTE risk (OR = 1.19, 95CI%:1.01–1.39). Our analyses demonstrated PA and sedentary time were indeed independently associated with the risk of VTE after mutually adjusting for sedentary time or PA, highlighting a unique perspective on their individual contributions. Further studies assessing the effects of different combinations of PA and sedentary time for assessing joint effects on VTE are needed.
Similar content being viewed by others

Introduction
Venous thromboembolism (VTE) is a serious condition characterized by blood clots forming in the veins, including pulmonary embolism (PE) and deep vein thrombosis (DVT). As one of the five most prevalent vascular conditions worldwide, VTE is a significant public health concern. It can severely impact daily life, leading to pain, swelling, reduced mobility, and a heightened risk of recurrent thrombotic events. Among adults the lifetime risk of VTE is approximate 8%, and there are nearly 10 million VTE events every year worldwide1,2. It is reported that about 20% of individuals with VTE events die within 1 year3, and VTE is widely regarded to be a substantial contributor to the global burden4,5. Accumulating evidence indicated that VTE is a multifactorial disease6,7 and can be potentially preventable through effective strategies.
Among the modifiable factors, physical activity (PA) is one of the main lifestyle-related factors for VTE that individuals are exposed to daily. Accumulating studies focus on the potential role of PA in the development of VTE, however, the benefit of PA for VTE is an ongoing debate. One meta-analysis of prospective studies has suggested that, compared with people with the lower levels of PA, those with higher PA levels had 13% (95% CI 5%-21%) lower odds of developing VTE8. However, another review without meta-analysis provided diverging results as to the association between high levels of PA and risk of VTE. This review indicated that while several studies have shown an association between high PA levels and an increased risk of VTE, not all studies reached the same conclusion. Therefore, more research using appropriate methodologies is needed to further explore the relationship between PA and VTE risk9. Furthermore, several additional studies have since been published on the association10,11,12 but the findings have been mixed in the absence of an update and a comprehensive meta-analysis. Accurate estimates of a dose-response association between PA and VTE are important and may be not only useful to promote awareness of PA in prevention of VTE but also could be helpful in guiding decisions at the policy level. Nevertheless, existing reviews estimated PA exposure by using binary categorization9, but this approach results in loss of information on PA doses and does not provide the variation in VTE risk across a range of PA doses.
Sedentary behavior is highly prevalent in our daily lives13, which is related but distinct from physical inactivity14, considering that someone can meet the PA recommendations despite being highly sedentary throughout the remaining waking hours. Some previous studies found that the associations between sedentary behavior and clinical health outcomes are independent of PA15,16,17. In line with this, it has been shown that prolonged sitting may cause vein compression, thereby reducing blood flow and increasing the risk of VTE18. Importantly, the association between sedentary behavior and VTE have not yet been systematically investigated, and it remains unclear whether PA attenuates the potential association of sedentary behavior with VTE. Whereas there are international public health PA recommendations19, there was insufficient evidence to quantify a sedentary behavior threshold20. Thus, quantitatively synthesizing evidence on sedentary behavior and VTE is required to inform public health officials in creating guidelines.
To bridge the knowledge gap, we conducted an updated and comprehensive systematic review and meta-analysis to investigate the shape of dose-response associations between PA and sedentary behavior with VTE, and whether the relationships of these two exposures with VTE are independent after mutual adjustment. We also further assessed the population attributable fraction (PAF) to estimate potential population changes in VTE that may be prevented by higher PA levels.
Methods
This systematic review was conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)21, The PRISMA checklist is exhibited in Supplementary Table 1. This study was prospectively registered in PROSPERO with the PROSPERO number being CRD42023424994.
Search strategy
A comprehensive search was conducted in electronic databases including PubMed, Web of Science and Embase from inception to August 1, 2024. A list of search terms based on [Title/Abstract] was as follows: (Exercise OR physical *activit* OR sedentary behavior OR recreational activity OR sports OR active transport OR active transportation OR household activity OR housework OR non-exercise activity OR activities of daily living OR physical fitness OR leisure activities) and (Venous Thromboembolic OR deep vein thrombose OR pulmonary embolism OR vein thrombosis OR thrombosis OR thromboembolism OR lung embolism). Besides, we also searched manually the references list of relevant articles and reviews.
Study selection
The following criteria were used to determine if a study was eligible for inclusion: (1) the study design is a cohort, case control or cross-sectional study to assess the relationship between PA or sedentary behavior and VTE; (2) reported effect estimates as hazard ratios (HRs), odds ratios (ORs), or relative risks (RRs) with 95% confidence intervals (CIs); (3) the exposures of interests were physical activity or sedentary behavior. If the data of multiple articles came from the same study, we chose the articles which reported the most informative PA level or had the largest sample size. Two authors independently selected eligible articles based on the title, abstract and full-text assessment. A third author resolved any disagreements.
Data extraction and quality assessment
The following information was extracted including: first author, publication year, study name, study design, location, characteristics of participants, sample size, exposure levels, case number per level of PA and sedentary behavior, total persons or person-years per PA and sedentary behavior level, the duration of follow up, the ORs/RRs/HRs for VTE with 95%CIs for each PA and sedentary behavior category, and adjusted variables in original analyses. The quality assessment of cohort and case-control study were evaluated using the Newcastle –Ottawa (NOS) scale22. Data extraction and quality assessment were independently conducted by the authors (HN. C. and YL).
PA exposure harmonization
A comprehensive PA exposure harmonization was conducted using a common metric in metabolic equivalent task hours per week (MET-h/wk), which could integrate different intensity and duration of PA in a week. The mean intensity of light PA, moderate PA, moderate to vigorous PA and vigorous PA were defined as 3, 4, 4.5 and 8 METs, respectively23. When MET was not provided directly in original articles, PA volume (MET-h/wk) was calculated by multiplying the duration (median or midpoint) of the reported category by its assigned MET value24. If the lowest category of duration or frequency was open-ended, the lower boundary was considered as 0. If the highest category of duration was not reported, the width of the interval was thought to be equal to its neighboring category. If PA frequency per week was only provided, PA frequency per week was converted to h/week by assigning a dose of 45 min per session25. If the duration was not provided, the duration of per session was assumed as 45 min. If the intensity of PA was not provided in the articles, we assigned the intensity as 4.5 METs25. The dose assignment calculations are shown in Supplementary Table 2.
Statistical analysis
All statistical analyses were executed by STATA version 12 (Stata Corp, College Station, Texas, USA). For categorical meta-analysis, the ORs and 95% CIs were pooled for highest vs. lowest category of PA and sedentary behavior. Cochran Q test and I2 were used to test the heterogeneity. P < 0.1 was considered as statistical heterogeneity for Q statistics. The value of I2 ranging from 0 to 25% was considered as no heterogeneity, I2 < 50%, 50-75% and > 75% were considered as low, moderate and high heterogeneity, respectively. Fixed effects model was used if I2 < 50% or else the random effects model was employed. Subgroup analyses were performed to estimate the effect across potential factors including sex, age, location, study type, the number of cases, quality score, adjusted for sedentary behavior/PA and adjusted for BMI. Sensitivity analyses were adopted to assess the stability of results by excluding one study at a time. Potential publication bias was assessed by Begg and Mazumdar’s test, Egger’s test and funnel plots. We further conducted trim-and-fill approach to explore the adjusted effect size when there was publication bias.
Studies with at least three exposure categories were included in dose-response analyses. Dose-response relationships were estimated by using the Greenland and Longnecker26 and Orsini27 methods. Studies with at least three exposure categories were included in the analyses. Potential nonlinear relationships between MET-h/wk or sedentary behavior and risk of VTE were evaluated using restricted cubic splines (RCS), with 3 knots located at the 10th, 50th and 90th of the distribution of MET-h/wk or sedentary behavior. The P value for nonlinearity was calculated by testing the null hypothesis that the coefficient of the second spline was equal to zero. Additionally, RR per 10 MET-h/wk increment and per hour of sedentary time increment were calculated using two-stage generalized least squares regression, respectively.
PAF was calculated based on PA exposure levels in population. The PAF was calculated according to Levin’s formula28, and the RR estimates and the prevalence (P) of exposure were required in the formula29.
PAFs were calculated for three WHO recommended levels of PA20, including 5.25 MET-h/wk (which was approximate half the minimum recommended level, 5.625 MET-h/wk), 12 MET-h/wk (which approached the minimally recommended level of 11.25 MET-h/wk), and 22.5 MET-h/wk (the upper bound of recommended levels). The RR is the pooled RR of VTE in dose-response curves associated with PA.
Patient and public involvement
There was no direct patient or public involvement in this review.
Results
Study characteristics
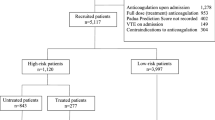
The selection procedure is shown in Fig. 1. Twenty-five articles including 31 studies with 1,787,740 individuals and 37,694 incident cases of VTE were included in present study, including 23 cohort and 8 case-control studies11,12,18,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51. Among the included articles, 21 articles provided the information on PA and VTE, and 5 articles provided sedentary behavior and VTE. The PA/sedentary behavior level in all included studies were assessed by self-reporting. 6 articles were based in America, 17 articles in Europe, 1 article in middle East countries, and 1 article in both America and Europe. The mean quality scores were 7.1. The study characteristics are shown in Table 1.

Results of the study selection process.
PA and VTE
Twenty-one articles including 27 studies with 35,594 VTE cases among 1,692,611 participants were included to evaluate the relationship between PA and VTE. The pooled OR for VTE in highest PA level was 0.83 (95%CI 0.77–0.89), with high heterogeneity (I2 = 79.5%, P < 0.01, shown in Fig. 2A). Although the Begg and Mazumdar’s test did not signal publication bias (Kendall’s tau = 0.11, P = 0.39), the Egger’s test (P = 0.04) suggested existence of publication biases (Fig. 2B). There was no study imputed using the trim-and-fill method, indicating that there was no publication bias and the finding was steady.

A: Forest plot of the pooled effect on VTE for the highest category of PA versus lowest category. B: Funnel plot. C: Sensitivity analysis. D: Dose-response relationship between PA and VTE.
In sensitivity analyses, by eliminating any study each time, the pooled risk did not substantially change, with the summary ORs ranging from 0.81 (95%CI: 0.75–0.89) to 0.84 (95%CI:0.79–0.90), confirming the stability of presenting results (Fig. 2C).
The estimated OR was 0.83 (95%CI:0.76–0.91) with BMI adjustment. After adjustment for sedentary behavior, PA was independently associated with a reduced VTE risk (OR = 0.72, 95%CI:0.61–0.85). More details were showed in Table 2.
Sedentary behavior and VTE
Five articles including 7 studies with 101,153 participants and 4234 VTE events were included regarding relationship between sedentary behavior and VTE. Prolonged sedentary behavior was associated with an increased VTE risk (OR = 1.24, 95%CI: 1.05–1.47), with high heterogeneity (I2 = 73.7%, P < 0.01) (Fig. 3A). Inspection of funnel plot (Fig. 3B) suggested existence of publication bias, while there was no indication in the Begg and Mazumdar’s test (Kendall’s tau = 0.43, P = 0.22) and Egger’s test (P = 0.17). Sensitivity analyses did not show substantive change from the pooled risk (Fig. 3C).

A: Forest plot of the pooled effect on VTE for the highest category of sedentary behavior versus lowest category. B: Funnel plot. C: Sensitivity analysis. D: Dose-response relationship between sedentary behavior and VTE.
Sedentary behavior was associated with higher risk of VTE (OR = 1.14, 95%CI:1.02–1.28) after BMI adjustment. After adjustment for PA, sedentary behavior was independently associated with an increased risk of VTE (OR = 1.19, 95CI%:1.01–1.39). More details are shown in Table 2.
Dose-response relationship between PA, sedentary behavior and VTE
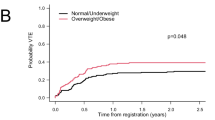
Eleven cohort studies with 22,120 VTE events were included in the dose-response analysis between PA and VTE, which showed a nonlinear dose-response relationship between PA and VTE (Fig. 2D, Pnon−linear<0.01), with steeper association gradients at lower PA volumes. There was the strongest protection against VTE when PA accumulated to 12 MET-h/wk in which, relative to adults not reporting any PA, those accumulating the recommended volume (12 MET-h/wk) had a 13% lower risk of VTE (RR = 0.87, 95%CI:0.84–0.90).
Four studies including 2,535 VTE cases were included restricted cubic spline analysis regarding between sedentary behavior and VTE. As shown in Fig. 3D, a linear dose-response association was present between sedentary behavior and VTE risk and there was a 2% higher risk of VTE for each 1 h increment of sedentary time per day (OR = 1.02, 95%CI: 1.00-1.03).
Potential population impact
Based on PAF analyses, 2.37% (95%CI: 1.90-2.85%) of VTE could be prevented if all adults achieved half the minimally recommended level of PA (5.25 MET-h/wk). Moreover, 2.85% (95%CI: 2.13-3.60%) of VTE could be prevented if all adults reached 12 MET-h/wk of PA, which approached the WHO minimally recommended level of 11.25 MET-h/wk. (Table 3).
Discussion
This systematic review showed a reduced risk of VTE with higher levels of PA and an increased risk of VTE with higher levels of sedentary behavior. A nonlinear dose-response relationship was found between PA and VTE, with a steeper risk reduction of VTE even at levels below the recommendations from WHO. Moreover, the public health impacts of VTE risk associated with changing the population-level PA exposure quantifiably showed a linear dose-response relationship between sedentary behavior and VTE, with a 2% higher risk of VTE with every 1 h increment of sedentary behavior per day. Furthermore, we observed PA and sedentary time were indeed independently associated with the risk of VTE even after mutual adjustment for sedentary time or PA.
Our finding was consistent with a previous meta-analysis study demonstrating that, compared with inactive individuals, there was a 17% reduced risk of VTE with higher PA levels8. In our study, subgroup analyses showed that the VTE risk was attenuated after BMI adjustment but remained significant, and the effect of PA was somewhat stronger in those with higher BMI. Moreover, the protective effect of PA tended to persist after adjusting for sedentary behavior.
Estimating the dose-response relationship using a harmonized approach can address limitations of the existing evidence that lacks specific doses of PA on VTE. Using a harmonized approach, we showed for the first time that there was a nonlinear dose-response relationship in the association between PA and VTE, in which a steeper risk reduction of VTE was found even at levels below the recommendations from WHO. Of note, if population levels of PA achieved half the recommended volume equal to 75 min/week of moderate-to-vigorous PA (5.25 MET-h/wk), then 2.37% of VTE incidents would potentially have been prevented. Collectively, the observed relationships demonstrate potential benefits for initially starting with small amounts of PA and gradually increasing over time, which could provide further insights into the development of public health interventions.
Regarding sedentary behavior, the present study supported and extended existing evidence demonstrating a positive association between sedentary behavior and VTE. However, our study extended these studies and further evaluated the shape of the relationship quantitatively, which provided insights and associations with greater precision. Patterns of the relationship suggested a linear dose-response with a 2% higher risk of VTE with every 1 h increment of sedentary behavior per day. This is in line with a previous study showing that sedentary behavior increased the mortality of cardiovascular disease independent of PA52. Similarly, the pooled estimated effect from four independent studies on sedentary time after adjustment for PA indeed suggested the independent detrimental effect of sedentary behavior on VTE, providing further perspectives into the interaction between sedentary behavior and PA on the development of VTE53. The present finding on VTE are further in line with the guidelines issued by the WHO, stating that adults should limit the time of sedentary behavior and replace with PA of any intensity. In addition, previous subgroup analyses stratified by levels of PA indicated that longer sedentary time had particularly adverse effects in populations with lower levels of physical activity but the effects were eliminated with at least 1 h of moderate intensity PA per day52. And there were also some previous studies focused on the divergence association between the specific domains of sedentary behavior and health outcomes54,55. We were unable to stratify subgroups according due to the limited available data leading to uncertainty regarding joint effects for combinations of PA with sedentary behavior. A future study is required to assess the interaction between PA and sedentary behavior on the risk VTE.
Although the mechanisms cannot explain the observed associations, numerous physiological mechanisms support the potential effect of PA and sedentary behavior in VTE incidence. PA could improve circulation of blood vessels and lower the odds of blood stagnation in the lower extremities, thereby reducing the risk of VTE56. In addition, PA could confer protection via anti- inflammatory mechanisms since a physically active lifestyle is known to interrupt inflammatory processes and generally lower the risk of an elevated inflammatory status57. On the other hand, sitting time can increase the levels of circulating inflammatory factors and hemostatic parameters, which increase VTE risk, especially deep vein thrombosis58. Moreover, the prolonged sitting time can inhibit the venous blood returning from the lower limbs and further promote venous stasis59,60. Sitting for a long time can weaken the muscle contraction, affecting the metabolism and blood vessel health, all of which lead to the development of VTE.
The present study has several strengths. This is the first dose-response meta-analysis that includes more original studies with a larger sample size to qualify the relationship using a novel harmonized exposure measurement, which reported how the risk of VTE varies along with the PA exposure used as a continuous variable. Second, sensitivity analyses further indicated the stability of the present findings. And detailed subgroup analyses were separately conducted and stratified with and without some adjusted potential confounders including BMI, PA for sedentary behavior, sedentary behavior for PA, thereby providing valuable insights for prevention strategies considering these variables. There are also some limitations that should be noted. Firstly, the assessment of PA and sedentary behavior in most included studies relied on single-time, self-reported measurements, which may lead to inaccurate association estimates. Future studies utilizing objective devices that measure PA and capturing trajectories of exposure are required to examine the associations. Secondly, almost all of the included studies are observational designed rather than interventional studies, which does not allow for inferences about causality. Thirdly, there were insufficient studies in dose-response analysis and subgroup analysis to distinguish the effect of different types of sedentary behavior with diverse domains of PA on VTE.
Conclusion
The present systematic review found that PA and sedentary time were indeed independently associated with the risk of VTE after mutually adjusting for sedentary time or PA. The dose-response relationship curves suggested a sharp risk reduction of VTE even below the recommended levels of PA, and potentially a slight risk increase beyond a higher PA threshold, suggested by the restricted cubic splines (RCS) model. There was a 2% higher VTE risk for 1 h increments in sedentary behavior per day. The findings therefore have substantial implications, which could inform national policy and intervention strategies in optimizing and promoting the benefits of promoting PA as well as synergistically reducing sedentary behaviors. Further cohort studies and randomized controlled trials assessing the effects of different combinations and types of PA and sedentary times using objective devices for assessing joint effect of PA and sedentary time on VTE are needed.
Supplemental information.
Supplemental information can be found in the attachment.
Data availability
All data are available in the main text or as a supplementary file. Additional requests can be made to the corresponding author upon reasonable request.
References
Lutsey, P. L. & Zakai, N. A. Epidemiology and prevention of venous thromboembolism. Nat. Rev. Cardiol.20, 248–262 (2023).
Bell, E. J. et al. Lifetime risk of venous thromboembolism in two Cohort studies. Am. J. Med.129 (3), 339e319–339e326 (2016).
Søgaard, K. K. et al. 30-year mortality after venous thromboembolism: a population-based cohort study. Circulation. 130 (10), 829–836 (2014).
Khan, F. et al. Venous thromboembolism. Lancet. 398 (10294), 64–77 (2021).
Noumegni, S. R. et al. Cardiovascular Mortality after venous thromboembolism: a Meta-analysis of prospective cohort studies. Semin Thromb. Hemost.48 (4), 481–489 (2022).
Rosendaal, F. R. Venous thrombosis: a multicausal disease. Lancet. 353 (9159), 1167–1173 (1999).
Gregson, J. et al. Cardiovascular Risk factors Associated with venous thromboembolism. JAMA Cardiol.4 (2), 163–173 (2019).
Kunutsor, S. K. et al. Physical activity and risk of venous thromboembolism: systematic review and meta-analysis of prospective cohort studies. Eur. J. Epidemiol.35 (5), 431–442 (2020).
Danin-Mankowitz, H. et al. The risk of venous thromboembolism and physical activity level, especially high level: a systematic review. J. Thromb. Thrombolysis. 52 (2), 508–516 (2021).
Hu, M., Wang, X. & Yang, Y. Causal relationship between moderate to vigorous physical activity and venous thromboembolism. J. Thromb. Thrombolysis55, 576–583 (2023).
MacDonald, C. J. et al. Association between cardiovascular risk-factors and venous thromboembolism in a large longitudinal study of French women. Thromb. J.19 (1), 58 (2021).
Yuan, S. et al. Lifestyle factors and venous thromboembolism in two cohort studies. Thromb. Res.202, 119–124 (2021).
Hajna, S. et al. Descriptive epidemiology of changes in objectively measured sedentary behaviour and physical activity: six-year follow-up of the EPIC-Norfolk cohort. Int. J. Behav. Nutr. Phys. Act.15 (1), 122 (2018).
Mielke, G. I. Relevance of Life Course Epidemiology for Research on Physical Activity and Sedentary Behavior. J. Phys. Act. Health. 19 (4), 225–226 (2022).
Bowden Davies, K. A. et al. Physical activity and Sedentary Time: Association with Metabolic Health and Liver Fat. Med. Sci. Sports Exerc.51 (6), 1169–1177 (2019).
Tarp, J. et al. Joint associations of physical activity and sedentary time with body mass index: a prospective study of mortality risk. Scand. J. Med. Sci. Sports33, 693–700 (2022).
Oh, W. et al. High physical activity alleviates the adverse effect of higher sedentary time on the incidence of chronic kidney disease. J. Cachexia Sarcopenia Muscle. 14 (1), 622–631 (2023).
Johannesen, C. D. L. et al. Sedentary work and risk of venous thromboembolism. Scand. J. Work Environ. Health. 46 (1), 69–76 (2020).
Global strategy of. diet, physical activity and health. [Published (2010). http://whqlibdoc.who.int/publications/2010/9789241599979_eng.pdf. Accessed February 19, 2019].
Bull, F. C. et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med.54 (24), 1451–1462 (2020).
Shamseer, L. et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Bmj. 350, g7647 (2015).
Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol.25 (9), 603–605 (2010).
Ainsworth, B. E. et al. Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011; 43(8):1575–1581. (2011).
Hartemink, N. et al. Combining risk estimates from observational studies with different exposure cutpoints: a meta-analysis on body mass index and diabetes type 2. Am. J. Epidemiol.163 (11), 1042–1052 (2006).
Liu, X. et al. Dose-response Association between Physical Activity and Incident Hypertension: a systematic review and Meta-analysis of Cohort studies. Hypertension. 69 (5), 813–820 (2017).
Greenland, S. & Longnecker, M. P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol.135 (11), 1301–1309 (1992).
Orsini, N. et al. Meta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and software. Am. J. Epidemiol.175 (1), 66–73 (2012).
Levin, M. L. The occurrence of lung cancer in man. Acta Unio Int. Contra Cancrum. 9 (3), 531–541 (1953).
Lin, C. K. & Chen, S. T. Estimation and application of population attributable fraction in ecological studies. Environ. Health. 18 (1), 52 (2019).
Bergendal, A. et al. Risk factors for venous thromboembolism in pre-and postmenopausal women. Thromb. Res.130 (4), 596–601 (2012).
Lindqvist, P. G., Epstein, E. & Olsson, H. The relationship between lifestyle factors and venous thromboembolism among women: a report from the MISS study. Br. J. Haematol.144 (2), 234–240 (2009).
Olson, N. C. et al. American Heart Association’s life’s simple 7 and risk of venous thromboembolism: the reasons for Geographic and racial differences in stroke (REGARDS) study. J. Am. Heart Assoc.4 (3), e001494 (2015).
van Stralen, K. J. et al. The relationship between exercise and risk of venous thrombosis in elderly people. J. Am. Geriatr. Soc.56 (3), 517–522 (2008).
Evensen, L. H. et al. Repeated assessments of physical activity and risk of incident venous thromboembolism. J. Thromb. Haemost. 16 (11), 2208–2217 (2018).
Wattanakit, K. et al. Association between cardiovascular disease risk factors and occurrence of venous thromboembolism. A time-dependent analysis. Thromb. Haemost. 108 (3), 508–515 (2012).
Kim, J. et al. Interaction of a genetic risk score with physical activity, physical inactivity, and body mass index in relation to venous thromboembolism risk. Genet. Epidemiol.42 (4), 354–365 (2018).
Nymberg, P. et al. Self-rated health and venous thromboembolism among middle-aged women: a population-based cohort study. J. Thromb. Thrombolysis. 49 (3), 344–351 (2020).
Kunutsor, S. K. et al. Leisure-time cross-country skiing and the risk of venous thromboembolism: a prospective cohort study. Eur. J. Prev. Cardiol.28(10), 1138–1141 (2021).
Solli, H. et al. Physical activity as an effect modifier of the Association between Obesity and venous thromboembolism: a Danish Population-based Cohort Study. Clin. Epidemiol.12, 1361–1370 (2020).
Nymberg, P. et al. Association between self-rated health and venous thromboembolism in Malmö Preventive Program: a cohort study. Prev. Med.159, 107061 (2022).
Armstrong, M. E. et al. Frequent physical activity may not reduce vascular disease risk as much as moderate activity: large prospective study of women in the United Kingdom. Circulation. 131 (8), 721–729 (2015).
Johansson, M. et al. Physical activity and risk of first-time venous thromboembolism. Eur. J. Prev. Cardiol.26 (11), 1181–1187 (2019).
Lutsey, P. L. et al. Correlates and consequences of venous thromboembolism: the Iowa women’s Health Study. Am. J. Public. Health. 100 (8), 1506–1513 (2010).
Holst, A. G., Jensen, G. & Prescott, E. Risk factors for venous thromboembolism: results from the Copenhagen City Heart Study. Circulation. 121 (17), 1896–1903 (2010).
van Stralen, K. J. et al. Regular sports activities decrease the risk of venous thrombosis. J. Thromb. Haemost. 5 (11), 2186–2192 (2007).
West, J. et al. A case-control study of seated immobility at work as a risk factor for venous thromboembolism. J. R Soc. Med.101 (5), 237–243 (2008).
Kubota, Y. et al. TV viewing and incident venous thromboembolism: the atherosclerotic risk in communities Study. J. Thromb. Thrombolysis. 45 (3), 353–359 (2018).
Engbers, M. J. et al. Functional impairment and risk of venous thrombosis in older adults. J. Am. Geriatr. Soc.65 (9), 2003–2008 (2017).
Shapiro, M. et al. Venous thromboembolism among physically active young adult females. Res. Pract. Thromb. Haemost. 7 (8), 102236 (2023).
Isiozor, N. M. et al. Life’s essential 8 is associated with atherosclerotic cardiovascular disease but not venous thromboembolism in men: a prospective cohort study. Ann. Med.55 (1), 2233894 (2023).
Wändell, P. et al. Risk of venous thromboembolism in relation to high physical activity level in men over 27 year follow up. J. Thromb. Thrombolysis (2024).
Ekelund, U. et al. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta-analysis of data from 850 060 participants. Br. J. Sports Med.53 (14), 886–894 (2019).
Ekelund, U. et al. Joint associations of accelero-meter measured physical activity and sedentary time with all-cause mortality: a harmonised meta-analysis in more than 44 000 middle-aged and older individuals. Br. J. Sports Med.54 (24), 1499–1506 (2020).
Patterson, R. et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur. J. Epidemiol.33 (9), 811–829 (2018).
Buffey, A. J. et al. The Acute effects of interrupting prolonged sitting time in adults with Standing and Light-Intensity Walking on Biomarkers of Cardiometabolic Health in adults: a systematic review and Meta-analysis. Sports Med.52 (8), 1765–1787 (2022).
Loh, R. et al. Effects of interrupting prolonged sitting with physical activity breaks on blood glucose, insulin and triacylglycerol measures: a systematic review and Meta-analysis. Sports Med.50 (2), 295–330 (2020).
Cho, S. M. J. et al. Association between physical activity and inflammatory markers in community-dwelling, middle-aged adults. Appl. Physiol. Nutr. Metab.46 (7), 828–836 (2021).
Parsons, T. J. et al. Physical activity, sedentary behavior, and inflammatory and hemostatic markers in men. Med. Sci. Sports Exerc.49 (3), 459–465 (2017).
Hamer, M., Smith, L. & Stamatakis, E. Prospective association of TV viewing with acute phase reactants and coagulation markers: English Longitudinal Study of Ageing. Atherosclerosis. 239 (2), 322–327 (2015).
Paterson, C. et al. The effects of Acute exposure to prolonged sitting, with and without interruption, on vascular function among adults: a Meta-analysis. Sports Med.50 (11), 1929–1942 (2020).
Funding
This work was supported by the State Scholarship Fund of the China Scholarship Council, File No. 202308080037. The funding sources had no role in study design, data analysis and interpretation of data, the writing of manuscript, or the decision to submit the paper for publication.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization: CW and BH; Literature search: YL and CT; Quality assessment: YL and HC; Data extraction: YL and HC; Data analysis: GD, YL and GW; CW, CT and GW wrote the manuscript draft; BR, MLH, CT revised the manuscript. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, G., Han, B., Dai, G. et al. Role of physical activity and sedentary behavior in venous thromboembolism: a systematic review and dose-response meta-analysis. Sci Rep 14, 22088 (2024). https://doi.org/10.1038/s41598-024-73616-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-73616-0
