
Abstract
Dyslipidemia has steadily increased in South Korea over the past two decades, emerging as a major public health concern and key risk factor for cardiovascular disease. Thus, our study aimed to investigate long-term trends in the prevalence, awareness, treatment, and control of dyslipidemia in South Korea, including the COVID-19 pandemic. This study utilized data from nationally representative cross-sectional surveys conducted as part of the Korea National Health and Nutrition Examination Survey from 2005 to 2022, analyzing long-term trends of dyslipidemia among 98,396 individuals aged over 30. Weighted linear and binary logistic regression were performed to calculate the β coefficients, βdiff, and weighted odds ratios with 95% confidence intervals (CIs). Weighted odds ratios were computed for various socioeconomic groups using aggregated data from 2005 to 2022. The prevalence of dyslipidemia increased from 41.30% (95% CI 40.40–42.21) in 2005–2009 to 48.41% (47.36–49.47) in 2020–2022. Awareness increased from 17.87% (16.75–18.99) to 48.90% (47.34–50.47), treatment from 7.10% (6.39–7.80) to 38.19% (36.61–39.76), and control among prevalence from 6.49% (5.79–7.19) to 31.82% (30.33–33.32). Treatment (βdiff, 3.94 [1.97–5.92]) and control among prevalence (βdiff, 3.52 [1.67–5.38]) increased more rapidly during the pandemic. Higher odds of dyslipidemia were associated with male sex, older population, rural residence, high BMI, central adiposity, low education and income levels, smoking, and high-risk alcohol consumption. Lower odds of awareness, treatment, and control among individuals with dyslipidemia were associated with male sex, younger population, rural residence, higher education and income levels, smoking, and high-risk alcohol consumption. Over the past 18 years, the prevalence, awareness, treatment, and control of dyslipidemia have steadily increased, with persistent disparities among socioeconomic groups.
Similar content being viewed by others
Introduction
Cardiovascular diseases (CVD) are one of the leading causes of death and disability worldwide, responsible for approximately 19.7 million deaths and 417 million disability-adjusted life years according to a 2019 study by the World Health Organization1. Dyslipidemia, a main cause of CVD, contributes to approximately one-third of ischemic heart disease and one-fifth of cerebrovascular disease globally, resulting in approximately 2.6 million deaths annually2. Over the past three decades, the prevalence of dyslipidemia has markedly increased worldwide, making it a significant public health concern3.
Since the emergence of the severe acute respiratory syndrome coronavirus 2, there have been numerous global deaths from COVID-19, and many studies have consistently highlighted its negative effects on various diseases4,5. Recent research has indicated that as the severity of COVID-19 infection increases, so does the burden of dyslipidemia6. Therefore, it is crucial to examine trends in the prevalence of dyslipidemia, including during the pandemic. Previous studies in South Korea have shown a steady rise in the prevalence of dyslipidemia, while treatment rates remain low7. Identifying high-risk individuals is essential because early and effective management of dyslipidemia can reduce the burden associated with disease development.
Various studies have been conducted worldwide focusing on the prevalence of dyslipidemia8,9. However, to our knowledge, no research has comprehensively examined the trends in prevalence, awareness, treatment, and control of dyslipidemia, including a pre-pandemic and during-pandemic comparison in South Korea. Therefore, this study aimed to investigate the trends of dyslipidemia in South Korea from 2005 to 2022 by category and compare dyslipidemia trends before and during the COVID-19 pandemic. By comparing different sociodemographic groups, this study aimed to identify vulnerable groups for dyslipidemia, thereby contributing to public health.
Methods
Survey design and participants
This study analyzed long-term trends in dyslipidemia prevalence, awareness, treatment, and control over 18 years. We used data from the Korea National Health and Nutrition Examination Survey (KNHANES), conducted by the Korea Disease Control and Prevention Agency (KDCA) from 2005 to 202210,11,12. The KNHANES utilized a robust multistage stratified cluster sampling design, selecting participants from a wide array of geographic and demographic areas to mirror the national profiles of age, sex, region, and socioeconomic status. In addition, sampling weights were applied to correct for differences in selection probability and non-response, thereby improving the representativeness and generalizability of the study outcomes. This study sought to investigate the dynamics of dyslipidemia and identify groups at higher risk by incorporating a broad set of socioeconomic factors.
The participants of this study were aged 30 years and over who were considered at risk for dyslipidemia, following the guidelines established by prior studies in the field13. Information of participants in the study covered variables such as age, sex, region of residence, body mass index (BMI), educational background, household income, and smoking status10,11. Across the duration of the study, 98,396 individuals were sampled, with yearly breakdowns as follows: 35,005 from 2005 to 2009, 15,610 from 2010 to 2012, 13,440 from 2013 to 2015, 20,601 from 2016 to 2019, and 13,740 from 2020 to 2022, with each segment designed following sampling methodology of KNHANES14. Particular focus was placed on 2020–2022 to delve into the effects of the COVID-19 pandemic. The research protocol was approved by the Institutional Review Boards of the KDCA (2007-02CON-04-P, 2008-04EXP-01-C, 2009-01CON-03-2 C, 2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2 C, 2013-07CON-03-4 C, 2013-12EXP-035 C). All participants provided written informed consent, and the KNHANES was made publicly available for various epidemiological research efforts. Our study adhered to the ethical standards of the Declaration of Helsinki.
Health outcomes
In this study, prevalence, awareness, treatment, control among prevalence, and control among treatment were the independent variables. Total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG) were determined in the assessment of dyslipidemia13. Prevalence of dyslipidemia was defined as the proportion of participants with fasting TC ≥ 240 mg/dL, LDL-C ≥ 160 mg/dL, HDL-C < 40 mg/dL, or TG ≥ 200 mg/dL, or who were currently taking lipid-lowering medication or had previously been diagnosed with dyslipidemia by a physician13. Awareness was determined as the percentage of patients with dyslipidemia who responded “yes” to the question, “Have you ever been told by a doctor or other healthcare professional that you have dyslipidemia?” Treatment was defined as the proportion of people taking lipid-lowering medication within the prevalence group. Control among prevalence was defined as the proportion of people with TC < 240 mg/dL, LDL-C < 160 mg/dL, HDL-C ≥ 40 mg/dL, and TG < 200 mg/dL within the prevalence group. Control among treatment was defined as the proportion of people taking lipid-lowering medication and meeting the criteria of TC < 240 mg/dL, LDL-C < 160 mg/dL, HDL-C ≥ 40 mg/dL, and TG < 200 mg/dL. The response rates for TC, LDL-C, HDL-C, and TG are presented in Table S1.
Covariates
In this study, the covariates included sex, age (30–39 years, 40–49 years, 50–59 years, 60–69 years, and ≥ 70 years), region of residence (urban and rural)15, BMI group (underweight [< 18.5 kg/m2], normal [18.5–22.9 kg/m2], overweight [23.0–24.9 kg/m2], and obese [≥ 25.0 kg/m2]), educational background (elementary school or lower, middle school, high school, and college or higher), household income (lowest, second, third, and highest quartile), smoking status (smoker and non-smoker), waist-to-height ratio (normal and central adiposity), daily calorie intake (low and high), and high-risk drinking (yes and no). The regions of residence of participants were classified as either urban or rural according to their responses in the survey15. Household income was segmented into four quartiles derived from the quartiles of standardized income, utilizing sample household and population statistics from the KNHANES. BMI was designated under categories in line with the criteria set by the Asian-Pacific guidelines15. Waist-to-height ratio was calculated by dividing waist circumference by height. A ratio of < 0.5 was classified as normal, while ≥ 0.5 indicated central adiposity16,17. Daily calorie intake was categorized into two groups, with individuals in the lower 50% of total daily calorie consumption classified as having low intake, while those in the upper 50% were classified as having high intake. High-risk drinking was defined as consuming ≥ 7 drinks per occasion for men or ≥ 5 for women at least twice per week18,19. Participants meeting these criteria were classified as “yes”, while others were classified as “no”. These covariates were identified as potential factors influencing the risk of developing dyslipidemia.
Statistical analysis
Our study implemented a weighted complex sampling method to assess the national prevalence, awareness, treatment, and control of dyslipidemia. Sampling weights were applied to adjust for differential selection probabilities. We used linear and binary logistic regression analyses to estimate β coefficients with 95% confidence intervals (CIs) and weighted odds ratios (wORs) with 95% CIs20. To evaluate changes in trends associated with the COVID-19 pandemic, we divided the study period into pre-pandemic (2005–2019) and pandemic (2020–2022) phases. For each phase, weighted linear regression was used to estimate the annual β coefficients for dyslipidemia indicators. The β difference (βdiff) was then calculated as the difference between the β coefficient during the pandemic and the β coefficient in the pre-pandemic period, thereby quantifying any acceleration, deceleration, or stability in the trends. This approach allows us to directly compare the rates of change across the two periods.
Subgroup analyses were conducted by stratifying participants based on sex, age, region of residence, BMI, educational background, household income, smoking status, waist-to-height ratio, daily calorie intake, and high-risk alcohol consumption. Within these subgroup analyses, the same procedure was applied: β coefficients were estimated for each period and βdiff computed to assess how trends varied across different population segments before and during the pandemic. Furthermore, wORs were calculated using combined data from the entire study period to identify demographic and socioeconomic groups with higher prevalence, awareness, treatment, and control rates of dyslipidemia, thus facilitating a comprehensive comparison. The statistical analyses in our study were performed using SAS software (version 9.4, SAS Institute, Cary, NC, USA), employing a two-sided test, with a P-value of 0.05 or less deemed to indicate statistical significance21.
Results
The comprehensive KNHANES survey included 98,396 participants from 2005 to 2022 after handling missing data (male: 48.76%). Table 1 presents the demographic characteristics of the participants. Figure 1 displays the prevalence, awareness, treatment, and control trends of dyslipidemia among individuals aged 30 years and over for different socioeconomic groups over the past 18 years, segmented into periods before and during the COVID-19 pandemic.

Trends in dyslipidemia prevalence, awareness, treatment, and control rates in population aged ≥ 30 years in South Korea, 2005–2022. The dashed line represents the beginning of the year 2020, marking the onset of the COVID-19 pandemic.
Prevalence of dyslipidemia
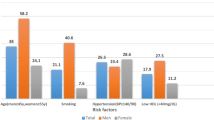
Table 2 shows the trends and differences in the prevalence of dyslipidemia from 2005 to 2022. The weighted prevalence of dyslipidemia increased consistently from 41.30% (95% CI 40.40–42.21) to 48.41% (95% CI 47.36–49.47) between 2005 and 2022. Tables 3 and S3 shows the ORs for the prevalence of dyslipidemia across various socioeconomic groups. Individuals with obesity had significantly higher odds of dyslipidemia (wOR, 5.62 [95% CI 5.01–6.30]). Older population was also significantly associated with increased odds of dyslipidemia (60–69 years: wOR, 3.25; 95% CI 3.07–3.44; ≥70 years: wOR, 2.96; 95% CI 2.81–3.13). Additionally, male sex (wOR, 1.59; 95% CI 1.54–1.65), lower educational background (wOR, 1.95; 95% CI 1.87–2.04]), lower household income (wOR, 1.60; 95% CI 1.52–1.68]), smoking (wOR, 1.46; 95% CI 1.41–1.51]), central adiposity (wOR, 3.14; 95% CI 3.03–3.25]), and high-risk alcohol consumption (wOR, 1.18; 95% CI 1.12–1.25]) were also associated with increased odds of dyslipidemia. As shown in Table S2, the interaction analysis between sex and other covariates revealed that the influence of sex on dyslipidemia prevalence decreased with older population, lower income, and lower education levels, whereas it increased among smokers and high-risk drinkers.
Awareness, treatment, and control of dyslipidemia
Table 2 also shows the trends and differences in awareness, treatment, and control of dyslipidemia. The awareness increased from 17.87% (95% CI 16.75–18.99) to 48.90% (95% CI 47.34–50.47). The treatment began at 7.10% (95% CI 6.39–7.80) and showed a substantial increase over the past 18 years, reaching 38.19% (95% CI 36.61–39.76), with a particularly notable rise during the COVID-19 period (βdiff, 3.94 [95% CI 1.97–5.92]). Likewise, control among prevalence showed a significant increase from 6.49% (95% CI 5.79–7.19) to 31.82% (95% CI 30.33–33.32), with further enhancing of this trend during the pandemic (βdiff, 3.52 [95% CI 1.67–5.38]). In addition, control among treatment steadily increased from 52.55% (95% CI 47.61–57.49) to 74.55% (95% CI 72.56–76.55).
Table 3 shows the ORs for the awareness, treatment, and control of dyslipidemia across various socioeconomic groups using data aggregated from 2005 to 2022. Males had lower awareness (wOR, 0.51 [95% CI 0.48–0.54]), treatment (wOR, 0.51 [95% CI 0.48–0.54]), control among prevalence (wOR, 0.40 [95% CI 0.38–0.43]), and control among treatment (wOR, 0.48 [95% CI 0.43–0.54]). Similarly, smokers had lower awareness (wOR, 0.59 [95% CI 0.56–0.62]), treatment (wOR, 0.59 [95% CI 0.56–0.63]), control among prevalence (wOR, 0.47 [95% CI 0.44–0.50]), and control among treatment (wOR, 0.48 [95% CI 0.43–0.54]). Likewise, high-risk drinkers had lower awareness (wOR, 0.67 [95% CI 0.61–0.72]), treatment (wOR, 0.59 [95% CI 0.53–0.65]), control among prevalence (wOR, 0.55 [95% CI 0.50–0.62]), and control among treatment (wOR, 0.60 [95% CI 0.50–0.73]). Compared to the younger population, the older population had significantly higher awareness (60–69 years: wOR, 10.00 [95% CI 8.80–11.36] and ≥ 70 years: wOR, 8.35 [95% CI 7.34–9.50]), treatment (60–69 years: wOR, 18.62 [95% CI 15.28–22.68] and ≥ 70 years: wOR, 18.36 [95% CI 15.03–22.44]), and control among prevalence (60–69 years: wOR, 11.92 [95% CI 9.89–14.37] and ≥ 70 years: wOR, 11.11 [95% CI 9.22–13.40]). The underweight population had lower awareness and treatment compared to other populations. Overall, awareness, treatment, and control among prevalence showed similar patterns.
Tables S4 to S7 present the ORs and ratio of ORs (RORs) for each socioeconomic subgroup before and during the COVID-19 pandemic. During the pandemic, awareness significantly increased among older adults subgroups (ROR, 3.15 [95% CI 2.27–4.38]), individuals with lower educational background (ROR, 1.81 [95% CI 1.50–2.18]), and those with lower household income (ROR, 1.48 [95% CI 1.22–1.80]). Additionally, control among the total prevalence also showed a significant increase in these subgroups (≥ 70 years: ROR, 1.94 [95% CI 1.24–3.04], elementary school or lower: ROR, 1.49 [95% CI 1.22–1.82], and lowest household income: wOR, 1.36 [95% CI 1.10–1.66]).
Discussion
Key finding
In this study, we examined a comprehensive longitudinal trend analysis of the prevalence, awareness, treatment, and control of dyslipidemia among a total of 98,396 Korean adults. We observed a consistent increase in dyslipidemia from 2005 to 2022. Awareness and control among treatment continued to show a significant increasing trend, in line with the prevalence of dyslipidemia. Over the past 18 years, the treatment and control rates among individuals with dyslipidemia showed a substantial increasing trend. Notably, during the COVID-19 pandemic, this trend appeared to intensify, with a steeper rise observed in the pandemic period compared to the pre-pandemic period. The prevalence of dyslipidemia was higher among males, older populations, rural residents, those with a higher BMI, lower educational attainment, lower household income, smokers, individuals with central adiposity, and those engaging in high-risk alcohol consumption. Lower awareness, treatment, and control rates among individuals with dyslipidemia were associated with male sex, younger population, rural residency, higher educational attainment, higher household income, smoking, and high-risk alcohol consumption. This study analyzed trends in dyslipidemia, identified the association between the COVID-19 pandemic and high-risk groups, and suggested specific management strategies at the national level.
Comparison with previous studies
Many previous studies have examined the prevalence of dyslipidemia in different countries and regions. Jordan (81.6%; n = 3132) and Ethiopia (66.7%; n = 321) had a higher prevalence than South Korea, while China (31.2%; n = 65,128) had a lower prevalence than South Korea22,23,24. This Chinese study identified common risk factors for dyslipidemia, such as male sex, obesity, and smoking, in line with our research. However, contrary to our findings, a higher prevalence was noted among urban residents24. As of research in China (n = 135,403), the awareness of dyslipidemia was higher than ours (64%; n = 36,958), with similar treatment (18.9%; n = 6993) but lower control among prevalence (7.2%; n = 504)25. Additionally, awareness, treatment, and control among prevalence were higher among females than males, consistent with our findings25.
The substantial differences in prevalence between countries are likely due to variations in ethnicity, dietary habits, lifestyle, and access to healthcare24,26. Previous studies have mainly examined the prevalence and risk factors of dyslipidemia in each region, and some additionally assessed awareness, treatment, and control25,27. However, most studies were generally based on data from a specific year27,28. In contrast, our research has investigated changes over the past 18 years in a large population and analyzed the influence of the COVID-19 pandemic on these trends. We also examined the trends among groups disproportionately affected by the pandemic. Findings from this long-term study should contribute to developing public health policies to manage dyslipidemia across various socioeconomic groups.
South Korea’s trends in dyslipidemia may differ from other nations due to a combination of healthcare system characteristics, lifestyle factors, and genetic predispositions. The country’s universal healthcare system ensures broad access to medical services, including lipid-lowering treatments, which may contribute to higher treatment and control rates compared to nations with less accessible healthcare systems. Additionally, dietary patterns in South Korea have shifted significantly in recent decades, with an increase in processed and high-calorie food consumption, which may uniquely influence dyslipidemia prevalence29,30. Lastly, genetic predispositions specific to East Asian populations, such as differences in lipid metabolism, may affect both prevalence and treatment response31. These factors highlight the need for country-specific public health strategies in managing dyslipidemia.
Plausible underlying mechanisms
In South Korea, the consumption of ultra-processed foods has been increasing30, and physical activity declined during the COVID-19 pandemic32. These factors may have contributed to the rising prevalence of dyslipidemia. Awareness would have increased as public awareness about dyslipidemia and healthcare utilization increased33,34,35. Control among treatments could have increased due to the development of anti-dyslipidemia medications36,37,38.
The treatment and control rates of dyslipidemia have steadily increased, with this trend accelerating during the COVID-19 pandemic. In South Korea, the decline in healthcare utilization due to COVID-19 was relatively lower than the global average34. Instead, heightened awareness about dyslipidemia and health concerns during the pandemic may have contributed to this rapid increase39. Additionally, the expansion of telemedicine services, digital health interventions, and increased accessibility to medication refills may have played a role in improving treatment adherence and disease management during this period34,35. Control among prevalence would have risen as people recognized the need to manage dyslipidemia and began receiving medication treatment. Indeed, control among prevalence has shown a similar trend to the treatment. These indicators are closely related to medication treatment, which can be initiated immediately; therefore, as people became more health-conscious during the pandemic, these measures likely increased immediately.
The risk factors for dyslipidemia included male sex, older population, rural residence, higher BMI, lower education and income levels, and smoking. Male sex was also a risk factor in most other studies. Males may have a higher prevalence because they are more likely to be obese and smoke11,40. Eight sex-biased genes are genetically associated with polygenic dyslipidemia, which puts males at higher risk of dyslipidemia41. In the elderly population, TC and LDL-C levels increase with age, which may increase prevalence42. Lower education and income levels are associated with a higher prevalence of chronic diseases and lower health awareness, which may lead to a higher prevalence of dyslipidemia43. High BMI and smoking are well-known risk factors for dyslipidemia24.
Low awareness, treatment, and control among prevalence are associated with male sex, younger population, rural residence, higher education and income levels, and smoking. These three indicators show similar trends. When diagnosed with dyslipidemia, individuals are more likely to receive treatment, and if treated, they are more likely to achieve control44. Males may have lower awareness due to less frequent healthcare utilization34. Younger populations, often perceiving themselves as low-risk, may not seek screening or treatment, resulting in lower management rates45. Rural residents may face limited access to healthcare services, contributing to lower awareness, treatment, and control rates46.
Interestingly, individuals with higher education and income levels also showed lower awareness and treatment rates. One possible explanation is that they may perceive themselves as being at lower risk due to healthier lifestyles or overall well-being. Additionally, demanding work schedules and different healthcare-seeking behaviors might lead to fewer routine check-ups. These findings suggest the need for targeted public health strategies to encourage regular screenings and risk awareness among this demographic43,47. Obesity is a well-known risk factor for dyslipidemia, so individuals with higher BMI tend to have greater awareness and treatment rates. However, weight loss is often recommended for obese individuals to manage dyslipidemia, meaning that despite higher treatment rates, control rates may not significantly improve48.
During the COVID-19 pandemic, the treatment and control rates of dyslipidemia increased at an accelerated pace. Several potential mechanisms may explain this trend. First, the heightened public awareness of health risks during the pandemic likely led to more proactive management of chronic conditions, including dyslipidemia. Increased concerns over metabolic health, particularly given the association between COVID-19 severity and cardiometabolic disorders, may have driven more individuals to seek medical consultations and adhere to lipid-lowering treatments6. Second, healthcare system adaptations, such as expanded telemedicine services and more flexible prescription regulations, may have improved accessibility to dyslipidemia treatment, facilitating better adherence and follow-up care34. These factors collectively contributed to the observed trend of improved dyslipidemia management during the pandemic.
Strengths and limitations
This study has several limitations due to the inherent characteristics of the KNHANES. First, each variable used in our research is not independent. Because several variables can comprehensively affect dyslipidemia, it is difficult to conclude that one variable directly affects dyslipidemia49. Second, as the KNHANES dataset is derived from a survey, it is inherently subject to individual bias, and the results may be influenced by participants’ recall. To mitigate these limitations, we endeavored to incorporate variables defined by objective measurements, such as blood tests, whenever feasible. Third, when evaluating lipid-lowering medication use, standard research practices often assess adherence based on the past two weeks. However, the KNHANES dataset we used does not specify a two-week period in its questionnaire. Instead, it categorizes medication use into broader timeframes, which may introduce slight inconsistencies in adherence assessment. To address this limitation, we focused on overall trends rather than short-term adherence, allowing for a broader understanding of dyslipidemia management patterns in the population. Finally, since this study only used data from South Korea, there may be limitations in applying our findings to other ethnicities or countries2. Therefore, similar follow-up studies using data from different countries are needed. However, this study has significant strengths. We provide a comprehensive insight into dyslipidemia by examining the prevalence of dyslipidemia with its risk factors over the past 18 years using a large sample in South Korea, as well as awareness, treatment, and control. We also considered the association of COVID-19 with dyslipidemia by observing changes in each trend between the pre-pandemic and the pandemic, suggesting post-pandemic public health policy development.
Clinical policy implications
According to our research, positive indicators such as awareness, treatment, and control of dyslipidemia in South Korea have increased, showing that dyslipidemia is being managed more effectively than before. However, the prevalence continues to rise, necessitating consistent management. To further improve dyslipidemia prevention and treatment outcomes, public health policies should focus on expanding screening programs, particularly for younger adults and high-risk groups such as males, smokers, and individuals with obesity. Additionally, targeted health campaigns and education programs should be developed to increase awareness and encourage proactive management of dyslipidemia. Improving healthcare accessibility in rural areas through telemedicine services and community-based interventions could also help address the lower awareness and treatment rates observed in these populations. Additionally, utilizing predictive modeling to identify populations vulnerable to dyslipidemia and facilitate their management could be beneficial50,51,52. These strategies could strengthen the country’s efforts to reduce the burden of dyslipidemia and its associated cardiovascular risks. The risk factors identified in this study should be used to develop more efficient dyslipidemia management policies. In the case of the older population, there was high awareness, treatment, and control among prevalence, as the risk of dyslipidemia was known to be high. Conversely, the younger population, considered to have a lower risk, has been in a management blind spot, resulting in significantly lower management rates. Therefore, the results of these studies should be utilized to assess the risk levels of each indicator by group and establish policies for effectively managing dyslipidemia53.
Conclusion
Over the past 18 years, the prevalence, awareness, treatment, and control of dyslipidemia in South Korea have significantly increased. During the pandemic, the treatment and control among prevalence showed a faster increasing trend than before. This suggests that the pandemic positively influenced the initiation of pharmacological therapy for dyslipidemia. Since the risk of dyslipidemia varies based on factors such as sex, age, region of residence, BMI, central adiposity, educational background, household income, smoking status, and high-risk alcohol consumption, these factors should be considered to assess individual risks and develop national policies for targeted management of dyslipidemia.
Data availability
The data are available upon request. Study protocol and statistical code: Available from DKY (yonkkang@gmail.com). Dataset: Available from the Korea Disease Control Agency (KDCA) through a data use agreement.
Change history
15 July 2025
This article has been updated to amend the license information.
References
Yan, L. D. et al. Spectrum of prevalent cardiovascular diseases in urban Port-au-Prince, Haiti: A population-based cross-sectional study. Lancet Reg. Health – Americas https://doi.org/10.1016/j.lana.2024.100729 (2024).
Pirillo, A., Casula, M., Olmastroni, E., Norata, G. D. & Catapano, A. L. Global epidemiology of dyslipidaemias. Nat. Rev. Cardiol. 18, 689–700. https://doi.org/10.1038/s41569-021-00541-4 (2021).
Liu, T., Zhao, D. & Qi, Y. Global trends in the epidemiology and management of dyslipidemia. J. Clin. Med. https://doi.org/10.3390/jcm11216377 (2022).
Kim, M. S. et al. Long-term autoimmune inflammatory rheumatic outcomes of COVID-19: A binational cohort study. Ann. Intern. Med. 177, 291–302. https://doi.org/10.7326/m23-1831 (2024).
Oh, J. et al. Incident allergic diseases in post-COVID-19 condition: Multinational cohort studies from South Korea, Japan and the UK. Nat. Commun. 15, 2830. https://doi.org/10.1038/s41467-024-47176-w (2024).
Xu, E., Xie, Y. & Al-Aly, Z. Risks and burdens of incident dyslipidaemia in long COVID: A cohort study. Lancet Diabetes Endocrinol. 11, 120–128. https://doi.org/10.1016/s2213-8587(22)00355-2 (2023).
Jin, E. S. et al. Dyslipidemia fact sheet in South Korea, 2022. Diabetes Metab. J. 47, 632–642. https://doi.org/10.4093/dmj.2023.0135 (2023).
Noubiap, J. J. et al. Prevalence of dyslipidaemia among adults in Africa: A systematic review and meta-analysis. Lancet Global Health. 6, e998–e1007. https://doi.org/10.1016/S2214-109X(18)30275-4 (2018).
Lu, Y. et al. Prevalence of dyslipidemia and availability of lipid-lowering medications among primary health care settings in China. JAMA Netw. Open 4, e2127573. (2021).
Oh, J. et al. Hand and oral hygiene practices of South Korean adolescents before and during the COVID-19 pandemic. JAMA Netw. Open 6, e2349249. (2023).
Kim, Y. et al. National trends in body mass index, overweight, and obesity among adults before and during the COVID-19 pandemic in 2009–2021: A representative longitudinal serial study in South Korea. J. Med. Virol. 95, e28958. https://doi.org/10.1002/jmv.28958 (2023).
Yim, Y. et al. Long-term trends in the prevalence of cardiovascular-kidney-metabolic syndrome in South Korea, 2011–2021: A representative longitudinal serial study. Lancet Reg. Health West. Pac. 55, 101474. https://doi.org/10.1016/j.lanwpc.2025.101474 (2025).
Rhee, E. J. Prevalence and current management of cardiovascular risk factors in Korean adults based on fact sheets. Endocrinol. Metab. (Seoul). 35, 85–94. https://doi.org/10.3803/EnM.2020.35.1.85 (2020).
Kang, J. et al. National trends in depression and suicide attempts and COVID-19 pandemic-related factors, 1998–2021: A nationwide study in South Korea. Asian J. Psychiatry. 88, 103727. https://doi.org/10.1016/j.ajp.2023.103727 (2023).
Nguyen, A. et al. Trends in prevalence of asthma and COVID-19 pandemic-related factors in South Korea: A post-hoc analysis. Life Cycle. 4, e1. https://doi.org/10.54724/lc.2024.e1 (2024).
Ashwell, M., Gunn, P. & Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 13, 275–286. https://doi.org/10.1111/j.1467-789X.2011.00952.x (2012).
Gibson, S. & Ashwell, M. A simple cut-off for waist-to-height ratio (0·5) can act as an indicator for cardiometabolic risk: Recent data from adults in the health survey for England. Br. J. Nutr. 123, 681–690. https://doi.org/10.1017/s0007114519003301 (2020).
Oh, K. et al. Korea National health and nutrition examination survey, 20th anniversary: Accomplishments and future directions. Epidemiol. Health. 43, e2021025. https://doi.org/10.4178/epih.e2021025 (2021).
Choi, S., Bahk, J., Park, S., Oh, K. & Jung-Choi, K. Smoking, drinking, and physical activity among Korean adults before and during the COVID-19 pandemic: A special report of the 2020 Korea National health and nutrition examination survey. Epidemiol. Health. 44, e2022043. https://doi.org/10.4178/epih.e2022043 (2022).
Lee, S. W. Regression analysis for continuous independent variables in medical research: Statistical standard and guideline of life cycle committee. Life Cycle. 2, e3. https://doi.org/10.54724/lc.2022.e3 (2022).
Yon, D. K. et al. Indoor exposure and sensitization to formaldehyde among Inner-City children with increased risk for asthma and rhinitis. Am. J. Respir. Crit. Care Med. 200, 388–393. https://doi.org/10.1164/rccm.201810-1980LE (2019).
Pengpid, S. & Peltzer, K. Prevalence, awareness, treatment, and control of dyslipidemia and associated factors among adults in Jordan: Results of a National cross-sectional survey in 2019. Prev. Med. Rep. 28, 101874. https://doi.org/10.1016/j.pmedr.2022.101874 (2022).
Gebreegziabiher, G., Belachew, T., Mehari, K. & Tamiru, D. Prevalence of dyslipidemia and associated risk factors among adult residents of Mekelle City, Northern Ethiopia. PLoS ONE. 16, e0243103. https://doi.org/10.1371/journal.pone.0243103 (2021).
Xi, Y. et al. Prevalence of dyslipidemia and associated risk factors among adults aged ≥ 35 years in Northern China: A cross-sectional study. BMC Public. Health. 20, 1068. https://doi.org/10.1186/s12889-020-09172-9 (2020).
Opoku, S. et al. Awareness, treatment, control, and determinants of dyslipidemia among adults in China. Sci. Rep. 11, 10056. https://doi.org/10.1038/s41598-021-89401-2 (2021).
Abuzhalihan, J. et al. Prevalence of dyslipidemia in students from Han, Uygur, and Kazakh ethnic groups in a medical university in Xinjiang, China. Sci. Rep. 9, 19475. https://doi.org/10.1038/s41598-019-55480-5 (2019).
Pengpid, S. & Peltzer, K. National high prevalence, and low awareness, treatment and control of dyslipidaemia among people aged 15–69 years in Mongolia in 2019. Sci. Rep. 12, 10478. https://doi.org/10.1038/s41598-022-14729-2 (2022).
Gao, H. et al. Prevalence of dyslipidemia and associated risk factors among adult residents of Shenmu City, China. PLoS ONE. 16, e0250573. https://doi.org/10.1371/journal.pone.0250573 (2021).
Yang, Y. S., Han, B. D., Han, K., Jung, J. H. & Son, J. W. Obesity fact sheet in Korea, 2021: Trends in obesity prevalence and obesity-Related comorbidity incidence stratified by age from 2009 to 2019. J. Obes. Metab. Syndr. 31, 169–177. https://doi.org/10.7570/jomes22024 (2022).
Lee, H. et al. Long-term trends and patterns in ultra-processed food consumption among Korean adults from 1998 to 2022. Sci. Rep. 15, 4131. https://doi.org/10.1038/s41598-025-88489-0 (2025).
Dumitrescu, L. et al. Genetic determinants of lipid traits in diverse populations from the population architecture using genomics and epidemiology (PAGE) study. PLoS Genet. 7, e1002138. https://doi.org/10.1371/journal.pgen.1002138 (2011).
Park, S. et al. National trends in physical activity among adults in South Korea before and during the COVID-19 pandemic, 2009–2021. JAMA Netw. Open 6, e2316930. (2023).
Lee, H. J., Jang, S. I. & Park, E. C. The effect of increasing the coinsurance rate on outpatient utilization of healthcare services in South Korea. BMC Health Serv. Res. 17, 152. https://doi.org/10.1186/s12913-017-2076-8 (2017).
Yoo, K. J. et al. The road to recovery: Impact of COVID-19 on healthcare utilization in South Korea in 2016–2022 using an interrupted time-series analysis. Lancet Reg. Health West. Pac. 41, 100904. https://doi.org/10.1016/j.lanwpc.2023.100904 (2023).
Bae, J. H. et al. Public awareness of dyslipidemia among the Korean population: A survey study. J. Lipid Atheroscler. 12, 307–314. https://doi.org/10.12997/jla.2023.12.3.307 (2023).
Cho, S. M. J. et al. Dyslipidemia fact sheets in Korea 2020: An analysis of nationwide Population-based data. J. Lipid Atheroscler. 10, 202–209. https://doi.org/10.12997/jla.2021.10.2.202 (2021).
Chang, Y. & Robidoux, J. Dyslipidemia management update. Curr. Opin. Pharmacol. 33, 47–55 (2017).
Arvanitis, M. & Lowenstein, C. J. Dyslipidemia. Ann. Intern. Med. 176, ITC81–ITC96 (2023).
Wilson, J. M., Lee, J. & Shook, N. J. COVID-19 worries and mental health: The moderating effect of age. Aging Ment Health. 25, 1289–1296. https://doi.org/10.1080/13607863.2020.1856778 (2021).
Chang, Y., Kang, H. Y., Lim, D., Cho, H. J. & Khang, Y. H. Long-term trends in smoking prevalence and its socioeconomic inequalities in Korea, 1992–2016. Int. J. Equity Health. 18, 148. https://doi.org/10.1186/s12939-019-1051-x (2019).
Zhang, Y. et al. Transcriptional profiling of human liver identifies sex-biased genes associated with polygenic dyslipidemia and coronary artery disease. PLoS ONE. 6, e23506 (2011).
Zhang, Y. et al. Association between cumulative low-density lipoprotein cholesterol exposure during young adulthood and middle age and risk of cardiovascular events. JAMA Cardiol. 6, 1406–1413. https://doi.org/10.1001/jamacardio.2021.3508 (2021).
Zajacova, A. & Lawrence, E. M. The relationship between education and health: Reducing disparities through a contextual approach. Annu. Rev. Public. Health. 39, 273–289. https://doi.org/10.1146/annurev-publhealth-031816-044628 (2018).
Berberich, A. J. & Hegele, R. A. A modern approach to dyslipidemia. Endocr. Rev. 43, 611–653. https://doi.org/10.1210/endrev/bnab037 (2021).
Alkerwi, A., Pagny, S., Lair, M. L., Delagardelle, C. & Beissel, J. Level of unawareness and management of diabetes, hypertension, and dyslipidemia among adults in Luxembourg: Findings from ORISCAV-LUX study. PLoS ONE. 8, e57920 (2013).
Kim, H. S. et al. Comparison between urban and rural mortality in patients with acute myocardial infarction: A nationwide longitudinal cohort study in South Korea. BMJ Open 10, e035501 (2020).
Alkerwi, A., Pagny, S., Lair, M. L., Delagardelle, C. & Beissel, J. Level of unawareness and management of diabetes, hypertension, and dyslipidemia among adults in Luxembourg: Findings from ORISCAV-LUX study. PLoS ONE. 8, e57920. https://doi.org/10.1371/journal.pone.0057920 (2013).
Nussbaumerova, B. & Rosolova, H. Obesity and dyslipidemia. Curr. Atheroscler. Rep. 25, 947–955 (2023).
Chang, Y., Kang, H. Y., Lim, D., Cho, H. J. & Khang, Y. H. Long-term trends in smoking prevalence and its socioeconomic inequalities in Korea, 1992–2016. Int. J. Equity Health 18, 1–10 (2019).
Azarafza, M., Azarafza, M. & Tanha, J. COVID-19 Infection Forecasting based on Deep Learning in Iran. medRxiv, 2020.2005.2016.20104182 https://doi.org/10.1101/2020.05.16.20104182 (2020).
Azarafza, M., Azarafza, M. & Akgün, H. Clustering method for spread pattern analysis of corona-virus (COVID-19) infection in Iran. MedRxiv 2020.2005.2022.20109942 https://doi.org/10.1101/2020.05.22.20109942 (2020).
Nanehkaran, Y. A. et al. The predictive model for COVID-19 pandemic plastic pollution by using deep learning method. Sci. Rep. 13, 4126. https://doi.org/10.1038/s41598-023-31416-y (2023).
Sun, X. et al. Dietary and other lifestyle factors and their influence on non-communicable diseases in the Western Pacific region. Lancet Reg. Health West. Pac. 43, 100842. https://doi.org/10.1016/j.lanwpc.2023.100842 (2024).
Funding
This research was supported by grants from the Ministry of Science and ICT (MSIT), Korea, under the ITRC (Information Technology Research Center) support program (IITP-2024-RS-2024-00438239); the Bio & Medical Technology Development Program of the National Research Foundation funded by the MSIT (RS-2023-00262002); and the Basic Science Research Program through the National Research Foundation funded by the Ministry of Education (RS-2024-00460379). The funders had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Author information
Authors and Affiliations
Contributions
Dr. DKY had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version of the manuscript before submission. Study concept and design: Hyeseung Lee, Seokjun Kim, YS, JH, Smith Lee, and DKY; acquisition, analysis, or interpretation of data: Hyeseung Lee, Seokjun Kim, YS, JH, Smith Lee, and DKY; drafting of the manuscript: Hyeseung Lee, Seokjun Kim, YS, JH, Smith Lee, and DKY; critical revision of the manuscript for important intellectual content: all authors; statistical analysis: Hyeseung Lee, Seokjun Kim, YS, JH, Smith Lee, and DKY; study supervision: DKY. DKY supervised the study and served as a guarantor. Hyeseung Lee, Seokjun Kim, and YS contributed equally as the first authors. JH, LS and DKY contributed equally as corresponding authors. The corresponding author attests that all listed authors meet the authorship criteria and that no one meeting the criteria has been omitted.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical statement
The research protocol was approved by the Institutional Review Boards of the KDCA (2007-02CON-04-P, 2008-04EXP-01-C, 2009-01CON-03-2 C, 2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2 C, 2013-07CON-03-4 C, 2013-12EXP-035 C). All participants provided written informed consent, and the KNHANES was made publicly available for various epidemiological research efforts. Our study adhered to the ethical standards of the Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lee, H., Kim, S., Son, Y. et al. National trends in dyslipidemia prevalence, awareness, treatment, and control in South Korea from 2005 to 2022. Sci Rep 15, 16148 (2025). https://doi.org/10.1038/s41598-025-00354-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-00354-2
