
Abstract
Recent research explores the associations between maladaptive personality constructs proposed by the DSM-5 Alternative Model of Personality Disorders (AMPD) and general psychopathology whereas research on sleep hygiene behaviors and sleep duration is poor. This study first aimed to classify an adult population based on bedtime, mobile phone use before bedtime, and sleep duration. The second aim was to compare the AMPD trait domains including negative affectivity, detachment, antagonism, disinhibition, and psychoticism across the derived clusters. The cross-sectional study consisted of 481 college students from the west of Iran (mean age of 27.7 ± 6.8 years; 69.4% female). Several single items plus the Brief Form of Personality Inventory for DSM-5 were used for data collection. A hierarchical cluster analysis was performed to determine latent categories, and the AMPD domain scores between the clusters were compared using multivariate analysis of variance and post hoc tests. The cluster analysis identified three categories containing a vulnerable group (poor sleep hygiene behaviors but sufficient sleep duration), an unhealthy group (poor sleep hygiene behaviors plus insufficient sleep duration), and a healthy group (good sleep hygiene behaviors plus sufficient sleep duration). The results showed that the clusters significantly differed in all trait domains (except for detachment) and the total average score with higher mean scores, especially for the unhealthy cluster. Our findings highlight the meaningful impact of maladaptive personality traits on unhealthy sleep hygiene behaviors and insufficient sleep. Preventive medicine can identify at-risk populations by screening for maladaptive personality in early adulthood.
Similar content being viewed by others
Introduction
Sleep hygiene behaviors are associated with sleep quality and mental health1. These behaviors are critical in the adult population and should be considered2. Sleep hygiene behaviors include guidelines such as maintaining a regular sleep-wake schedule and avoiding electronic devices like mobile phones before bedtime3. Therefore, bedtime must be set at an appropriate time, as bedtime is a key component of sleep patterns and is crucial for regulating sleep rhythms4. Research indicates that later bedtime is generally associated with adverse health outcomes5. Additionally, bedtime is an influential variable in global health6,7,8.
Modern lifestyle and artificial light at night delay human sleep time, disrupt sleep, and lead to greater intrapersonal changes in sleep timing9 Mobile phones are one of the sources of artificial light, and the increasing prevalence of mobile phone use, especially before sleep, has raised concerns about its detrimental effects on sleep quality and duration. Recent studies10,11 indicate a significant relationship between nighttime mobile phone use and various sleep disorders, including increased sleep latency, reduced total sleep time, and generally poor sleep quality. Short and long sleep durations also are associated with premature mortality, and achieving an optimal sleep duration has been a focus of sleep hygiene guidelines12. The results of a systematic study indicated that a sleep duration of 7–8 h per day has the strongest correlation with health in adults13. Another study found that shorter sleep durations are linked to adverse physical and mental health outcomes14. It has been reported that insufficient sleep duration is related to depression15 However, the role of underlying psychological factors, particularly maladaptive personality traits, in predicting mobile phone use before bedtime and sleep duration remains unknown.
Research literature suggests that problematic mobile phone use is a function of personality traits such as neuroticism, extraversion, openness to experience, and impulsivity16,17. Personality traits such as neuroticism, extraversion, openness, and conscientiousness are also significant predictors of sleep duration18,19. Personality is associated with sleep duration even after controlling for psychiatric and medical conditions, and it may be an additional factor to consider when assessing any patient20. Overall, personality structure significantly influences important aspects of life and plays a crucial role in health-related behaviors and psychopathology21,22. However, current knowledge about the impact of maladaptive personality on sleep patterns and adherence to sleep hygiene behaviors is poor.
In the context of the role of personality traits in sleep behaviors, the five-factor model of personality has previously been emphasized18,23,24, but the role of the DSM-5 Alternative Model of Personality Disorders (AMPD) has not received much attention. The AMPD provides a subsequent approach to understanding personality disorders that contrasts with traditional classification models25. This model organizes maladaptive personality constructs into five broad trait domains including negative affectivity (a tendency toward emotional instability and sensitivity to stress), detachment (an avoidance of emotional intimacy and social interactions), antagonism (a tendency to hostility, selfishness, and exploit others for self-gain), disinhibition (recklessness, irresponsibility, and a willingness to take risks without considering consequences), and psychoticism (a tendency toward unusual beliefs, cognitive distortion, and eccentric behaviors)25 Each domain includes specific aspects that reflect maladaptive personality traits. Studying maladaptive personality traits is crucial for understanding their significant impact on mental health26, interpersonal relationships27, and behavioral outcomes28.
Current study
The results of a meta-analysis indicated that educational interventions aimed at teaching sleep hygiene behaviors have a moderate effect on sleep quality29. This raises the question of why not everyone benefits from these educational efforts. It seems that the reason may lie in the lack of attention to the role of personality traits. Therefore, this study focuses on the role of maladaptive personality constructs from the perspective of DSM-5. On the other hand, recent research explores the associations between maladaptive personality constructs proposed by the AMPD and general psychopathology30,31 whereas research on sleep hygiene behaviors and sleep duration is poor32,33. Thus, understanding the relationship between maladaptive personality and bedtime and sleep duration is particularly important, as it may provide interventions aimed at improving sleep hygiene and enhancing sleep quality among individuals with personality pathology. The present study first aimed to classify an adult population based on bedtime, mobile phone use before bedtime, and sleep duration. We expected cluster analysis to identify and separate groups with healthy and unhealthy sleep behaviors. The second research objective was to compare the AMPD trait domains (i.e., negative affectivity, detachment, antagonism, disinhibition, and psychoticism) across the derived clusters. We expected that scores on some maladaptive trait domains, such as negative affectivity and disinhibition32,33,34,35, would be significantly higher in the clusters with unhealthy sleep behavior than in healthier ones.
Methods
Sample and procedure
The statistical population for this study comprised all college students enrolled at Kermanshah University of Medical Sciences from western Iran in 2024, who were aged between 18 and 53 years. To accommodate potential participant dropout and non-cooperation, an initial sample size of 500 individuals was planned. A questionnaire link was disseminated via WhatsApp and Telegram, yielding 481 completed responses for statistical analysis. Online data collection is becoming increasingly prevalent, especially in sleep medicine research, offering rapid access to large datasets at a reduced cost. While some limitations exist, evidence suggests that online data collection methods maintain comparable validity and reliability to traditional approaches36,37.
Inclusion criteria for participants required them to be at least 18 years old and no older than 55, have completed at least one semester at the university, have no history of psychotic psychiatric disorders such as schizophrenia, and provide full consent to participate. Exclusion criteria eliminated individuals with serious physical diseases affecting participation (e.g., cognitive disorders) and students with non-Iranian nationals. Ethical considerations were paramount, with clear communication of the study’s objectives, voluntary participation, assurance of confidentiality, and the right to withdraw at any stage. Informed consent was obtained from all participants, who signed a consent form. The study protocol was pre-registered by Kermanshah University of Medical Sciences and received ethical approval from the university’s ethics committee (Code: IR.KUMS.REC.1403.365). In the present study, all methods were performed by the relevant guidelines and regulations.
Data collection tools
Personality assessment
Personality Inventory for DSM-5, Brief Form (PID-5-BF), which is adapted from the 220-item PID-538, is a 25-item self-report scale used to evaluate maladaptive personality traits based on the criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). It specifically assesses the five personality trait domains including negative affectivity (i.e., tendency to experience negative emotions like anxiety, depression, and anger), detachment (i.e., withdrawal from social interactions and a lack of emotional responsiveness), antagonism (i.e., hostility, deceitfulness, and a lack of empathy or concern for others), disinhibition (i.e., impulsivity and a lack of self-control, and psychoticism (i.e., unusual perceptions and beliefs, as well as eccentric behavior). Scoring is based on a 4-point Likert scale, ranging from 0 for “completely false” or “often false” to 3 for “completely true” or “often true.” Recent review studies39,40 support the internal and external validity of the PID-5-BF in Iranian populations. In the present study, alpha coefficients were between 0.70 and 0.79 for the subscales and it was 0.91 for the total items (see Table S1).
Assessment of sleep hygiene behaviors
A single-item scale was used to measure mobile phone use before sleep. Participants were asked: “In the past year, have you used your mobile phone and social media one hour before going to bed?” Participants selected one of three options (1 = I never use it, 2 = I use it some nights, and 3 = I use it every night). To assess bedtime, participants were asked: “What time do you usually go to bed at night over the past month?” Respondents entered their desired time. This question was adapted from the Pittsburgh Sleep Quality Index41.
Sleep duration assessment
To measure sleep duration, participants were asked: “How many hours of actual sleep did you get each day over the past month?” Respondents entered their number of hours slept. This question was also adapted from the Pittsburgh Sleep Quality Index41.
Data analysis
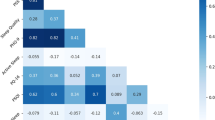
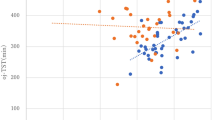
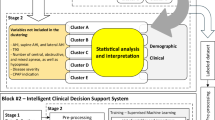
Data analysis for this research was conducted using SPSS-23 software. Descriptive statistics such as mean and standard deviation were used to summarize the data. We also evaluated the non-violation of statistical assumptions such as normality (skewness and kurtosis between − 1 and + 1) for the AMPD domain scales. All statistical tests utilized in the analyses were two-tailed, with a statistical significance at a level of < 0.05. Continuous variable data were reported as means and standard deviations, while categorical data were reported as frequencies and percentages. We also reported Pearson correlation coefficients between the AMPD trait domains and sleep duration. For the main analysis, a hierarchical cluster analysis (Ward method) was used to identify the clusters based on mobile phone use one hour before sleep (categorical data), bedtime (categorical data), and sleep duration (continuous). In this study, we employed hierarchical cluster analysis as the primary method to identify distinct clusters of sleep hygiene behaviors among participants. This approach was chosen because it allows for data exploration without requiring a predetermined number of clusters, making it particularly useful when the optimal number of clusters is uncertain. Additionally, hierarchical clustering offers a visual representation of the clustering process through a dendrogram, which aids in the interpretation and understanding of the results. After adjustment for age differences, the clusters were compared to the mean scores of five domain scales using multivariate analysis of variance.
Results
The sample analyzed consisted of 481 individuals, of whom 334 (69.4%) were female. The mean age of the participants was 27.7 years with a standard deviation of 6.8. Cluster analysis was conducted based on the variables of mobile phone use one hour before sleep, bedtime, and sleep duration, resulting in identify three clusters: (i) poor sleep hygiene behaviors but sufficient sleep duration (vulnerable group: n = 233), (ii) poor sleep hygiene behaviors plus insufficient sleep duration (unhealthy group: n = 123), and (iii) good sleep hygiene behaviors plus sufficient sleep duration (healthy group: n = 125). The characteristics of each cluster are detailed in Table 1.
In the vulnerable group (Cluster I), the majority (about 99%) use their mobile phones every night before going to bed, and most (about 90%) go to bed between 11 PM and 2 AM, with an average sleep duration of 7.9 ± 1.1 h. In the unhealthy group (Cluster II), the majority (about 89%) also use their mobile phones every night before bed, and most (about 75%) go to bed between 11 PM and 2 AM, with an average sleep duration of 5.2 ± 1.1 h, indicating that sleep duration is insufficient. In the healthy group (Cluster III), the majority (about 62%) use their mobile phones some nights before going to bed, and most (about 62%) go to bed between 9 PM and 11 PM, with an average sleep duration of 7.5 ± 1.2 h. The distinguishing feature of the last Cluster compared to the other clusters is that mobile phone use before bedtime is not high, and bedtime is earlier. Additionally, the clusters do not differ significantly in terms of gender characteristics, educational levels, marital status, or smoking habits. However, there are significant differences in the average age.
FIGURE 1.
Figure 1 shows the differences in the AMPD domain scales and the total average score between the clusters. The mean differences in the maladaptive trait scores within each cluster, along with error bars with 95% CI, can be seen in Figure S1. In more detail, Table 2 presents the descriptive data for maladaptive domains of personality and compares the clusters head-to-head to identify significant differences. The results indicate that all maladaptive trait domains of personality (except for detachment) as well as the total average score differ significantly across the clusters. These results showed that the mean score of domain scales is higher in the unhealthy cluster. Pairwise comparisons after adjustment for age differences indicated that there is a significant difference between the healthy and unhealthy groups in all domains except for detachment. There is also a significant difference between the healthy and vulnerable clusters in the disinhibition domain. Descriptive data (minimum, maximum, skewness, and kurtosis) for the PID-5-BF and Pearson correlations between the personality domain scales and sleep duration were indicated in Tables S1 & S2, respectively).

Mean differences in the personality domains between the clusters.
The effect size (η²) in Table 2 represents the proportion of variance in each maladaptive trait domain explained by cluster membership, adjusted for age. Simply put, it shows how much the differences in personality traits are linked to different sleep behavior clusters. A larger effect size signifies a stronger relationship between cluster membership (sleep health behaviors) and a specific personality trait. Based on these results, negative affectivity (η² = 0.044) appears to play a slightly greater role in unhealthy sleep behaviors compared to other traits, with psychoticism (η² = 0.041) following. The overall effect of maladaptive personality traits in predicting unhealthy sleep behaviors is η² = 0.043, which is generally considered a small effect size.
Discussion
In the present study, we identify three clusters based on the variables of mobile phone use one hour before sleep, bedtime, and sleep duration in an adult sample. The first cluster included individuals who had sufficient sleep, with their bedtime between 11 PM and 2 AM, and who had used their mobile phones and social media for one hour before bedtime every night in the past year. The second cluster consisted of individuals who did not have sufficient sleep, with their bedtime also between 11 PM and 2 AM, and who had similarly used their mobile phones and social media for one hour before bedtime every night in the past year. The third cluster included individuals who had sufficient sleep, with their bedtime between 9 PM and 11 PM, and who had used their mobile phones and social media for one hour before bedtime on some nights in the past year. In general, we identified three groups: healthy, unhealthy, and vulnerable, which did not differ mainly in terms of sociodemographic factors. However, only 26% of the sample was from the healthy group, which indicates the prevalence of unhealthy sleep hygiene behaviors and insufficient sleep in the Iranian student population. This finding aligns with previous studies42,43 that emphasize the prevalence of sleep problems among students, showing that sleep issues are a significant concern in this population.
Based on the results of our study, it can be said that sleep hygiene and sleep quantity pose a major challenge among university students. By recognizing the prevalence of these issues and examining effective interventions, efforts can be made to promote healthier sleep habits in this population and ultimately improve their academic success and quality of life. Additionally, since sleep is a fundamental factor for stabilizing, processing, and functioning in memory and learning44, and learning is highly important for the student population, future research should focus more on the factors related to sleep hygiene and sleep quantity among students. Given that the level of mobile phone and internet usage before sleep was high in the sample studied, along with a significant number not going to bed at appropriate times, it can be concluded that aspects of sleep hygiene are not being followed by students. Therefore, creating and implementing educational workshops centered on sleep hygiene tailored for university students should be prioritized by student affairs planners. These programs should emphasize the importance of reducing mobile phone use before sleep and establishing a regular sleep schedule. By addressing the specific needs of each identified cluster in our study, these programs can help mitigate the negative effects of poor sleep hygiene.
We also found that the clusters differed significantly in terms of maladaptive personality traits (except for detachment), with the average of these traits being higher in the second cluster. This indicates that maladaptive personality traits are associated with insufficient sleep duration and also play a role in sleep hygiene behaviors. According to the findings of a previous study45, adolescents with higher levels of problematic technology use reported greater overall personality pathology (especially antagonism domain) compared to other groups. Another study showed the role of negative affectivity and antagonism domains in problematic mobile phone use46. However, no studies were found that examined the role of maladaptive personality traits in mobile and internet use before sleep. Also, no studies have been conducted on the relationship between maladaptive personality traits and sleep duration. However, previous studies have shown that some personality traits such as neuroticism, disinhibition, and emotional temperaments are significantly correlated to sleep quality and problems35,47,48.
Previous studies specifically aimed to investigate the relationship between the constructs of the five-factor model of personality and sleep duration19,23. For instance, the results of a study showed that higher conscientiousness was associated with longer sleep duration and earlier timing, as well as greater stability in total sleep time. Higher extraversion was linked to a later bedtime, shorter sleep duration, and greater variability in sleep timing, while neuroticism, agreeableness, and openness to experience had no significant relationship with sleep duration or scheduling19. The results of other studies indicated that sleep patterns—including sleep duration, frequency of nightmares, dream contents, sleep deprivation, sleep continuity, insomnia severity, and sleep problems—are related to personality traits23,49. Personality traits also can influence life functioning, health outcomes, life satisfaction, academic performance, and career planning among students50. Given that our research sample consisted of college students, it can be said that these effects are explicable considering the nature of sleep hygiene variables and sleep quantity. On the other hand, it is stated that personality traits act as important predictors of many outcomes51, with sleep duration being one of these outcomes.
Specifically, we found that scores of negative affectivity, antagonism, disinhibition, and psychoticism are higher in the unhealthy than healthy group. The disinhibition score was also higher in the vulnerable than in the healthy group. Adults with high levels of negative affectivity often experience anxiety and emotional distress, which can lead to difficulties in falling asleep and maintaining restful sleep. Recent research52,53,54 shows that neuroticism/negative affectivity is strongly associated with poor sleep quality. This can lead to increased rumination and stress, making it challenging to establish a healthy sleep routine. Therefore, from this perspective, the nature of negative affectivity being similar to neuroticism makes this finding understandable. Our findings, highlighting the significant role of negative affectivity in predicting poor sleep hygiene, align with previous research examining the relationship between Type D personality and both sleep hygiene and insomnia55,56. The increased vulnerability associated with Type D personality, characterized by high negative affectivity and social inhibition, appears to involve this mechanism. We recommend that psychotherapists employ non-pharmacological approaches such as cognitive-behavior therapy and acceptance and commitment therapy to help these individuals manage rumination and negative emotions before sleep, addressing the potential use of mobile phones as an avoidance strategy.
Regarding antagonism and disinhibition, it can be said that these trait domains are associated with irresponsible and impulsive behaviors35, which can negatively impact sleep hygiene. Individuals who exhibit high levels of self-disinhibition may engage in irregular sleep hours or substance use (e.g., alcohol or stimulants), both of which can severely disrupt normal sleep patterns57. Therefore, strategies to enhance self-control and reduce impulsivity related to sleep behaviors are advised for individuals with externalizing personality pathology. These may include establishing firm bedtime routines, restricting access to stimulating activities like mobile phone use before bed and utilizing stimulus control techniques to reinforce the connection between the bed and sleep. Considering psychoticism, it can be said that this trait domain may be related to unusual thought patterns58, which can interfere with the ability to relax and fall asleep. Individuals with high levels of psychoticism may experience strange thoughts or intense anxiety while trying to sleep, leading to reduced sleep duration59. Overall, considering the confirmed role of maladaptive personality traits in sleep quantity and adherence to sleep hygiene, increasing mental health services on campus to address maladaptive personality characteristics related to sleep quality and quantity should be prioritized.
Limitations
While our study provides valuable insights into the relationship between mobile phone use, sleep hygiene, and personality traits among university students, there were several limitations. First, our study was cross-sectional in nature, which limits our ability to draw causal conclusions about the relationships between personality traits, sleep quantity, and sleep hygiene. Longitudinal studies are needed to better understand how the amount and timing of mobile phone use and personality traits affect sleep over time. Second, the data for this study were collected through self-reporting. Relying on self-reported measures to assess sleep patterns and mobile phone use may introduce bias, as participants might overestimate or underestimate their behaviors due to social desirability or recall bias. Third, the sample studied may not represent all student populations, as it was limited to a specific demographic and geographic region (Kermanshah, Iran). Future research should examine more diverse samples to enhance generalizability. Fourth, we did not include clinical populations with established psychiatric disorders, which suggests caution in generalizing findings to these populations. Fifth, despite single items being expedient to data collection, they lack the comprehensiveness and nuance of established sleep hygiene scales. Future research should employ validated multi-item scales to provide a more thorough and reliable assessment of sleep hygiene practices. Finally, while we examined maladaptive personality traits, other factors affecting sleep—such as lifestyle choices, environmental factors, and physical health—were not thoroughly investigated.
Conclusion
We aimed to classify an adult population based on bedtime, mobile phone use before bedtime, and sleep duration, and to compare the AMPD trait domains including negative affectivity, detachment, antagonism, disinhibition, and psychoticism across the derived clusters. The cluster analysis identified three independent categories containing a vulnerable group (poor sleep hygiene behaviors but sufficient sleep duration), an unhealthy group (poor sleep hygiene behaviors plus insufficient sleep duration), and a healthy group (good sleep hygiene behaviors plus sufficient sleep duration). The results showed that the clusters significantly differed in all trait domains (except for detachment) and the total average score with higher mean scores, especially for the unhealthy cluster. Our findings highlight the meaningful impact of maladaptive personality domains on unhealthy sleep hygiene behaviors and insufficient sleep. Overall, our study contributes to the growing evidence linking mobile phone use to poor sleep hygiene among students and highlights the role of maladaptive personality in this relationship. While our study utilizes the AMPD model, providing a more nuanced understanding of specific personality traits, the convergence of these results underscores the importance of addressing underlying personality factors when treating sleep disorders. Future research should investigate the specific pathways through which various personality traits influence sleep behaviors and assess the effectiveness of targeted psychotherapies in improving sleep outcomes. Preventive medicine can identify at-risk populations by screening for maladaptive personality in early adulthood.
Data availability
Data will be available upon request from the corresponding author (s_komasi63@yahoo.com).
Abbreviations
- AMPD:
-
Alternative model of personality disorders
- DSM-5:
-
Diagnostic and statistical manual of mental disorders, fifth edition
- PID-5-BF:
-
Personality Inventory for DSM-5, Brief Form
References
Strong, C. et al. Sleep hygiene behaviours in Iranian adolescents: An application of the theory of planned behavior. J. Sleep. Res. 27, 23–31. https://doi.org/10.1111/jsr.12566 (2018).
Zhang, C. Q., Fang, R., Zhang, R., Hagger, M. S. & Hamilton, K. Predicting hand washing and sleep hygiene behaviors among college students: Test of an integrated social-cognition model. Int. J. Environ. Res. Public. Health. 17, 1209. https://doi.org/10.3390/ijerph17041209 (2020).
McAlpine, T., Mullan, B. & Clarke, P. J. F. Assessing the daily association of sleep hygiene behaviours with sleep: A between and within persons approach. J. Behav. Med. 47, 255–270. https://doi.org/10.1007/s10865-023-00448-0 (2024).
Wang, L. et al. The relationship between sleep onset time and cardiometabolic biomarkers in Chinese communities: A cross-sectional study. BMC Public. Health. 20, 374. https://doi.org/10.1186/s12889-020-08516-9 (2020).
Chaput, J. P. et al. Sleep timing, sleep consistency, and health in adults: A systematic review. Appl. Physiol. Nutr. Metab. 45, S232–S247. https://doi.org/10.1139/apnm-2020-0032 (2020).
Zhao, S. et al. Sleep timing and the prevalence of hypertension in middle-aged and older populations: The sleep heart health study. BMC Psychiatry. 24, 715. https://doi.org/10.1186/s12888-024-06174-4 (2024).
Ma, M. et al. Association of sleep timing with all-cause and cardiovascular mortality: the sleep heart health study and the osteoporotic fractures in men study. J. Clin. Sleep. Med. 20, 545–553. https://doi.org/10.5664/jcsm.10926 (2024).
Yan, B. et al. Sleep timing May predict congestive heart failure: A community-based cohort study. J. Am. Heart Assoc. 10, e018385. https://doi.org/10.1161/JAHA.120.018385 (2021).
Taillard, J., Sagaspe, P., Philip, P. & Bioulac, S. Sleep timing, chronotype and social jetlag: impact on cognitive abilities and psychiatric disorders. Biochem. Pharmacol. 191, 114438. https://doi.org/10.1016/j.bcp.2021.114438 (2021).
Lemola, S., Perkinson-Gloor, N., Brand, S., Dewald-Kaufmann, J. F. & Grob, A. Adolescents’ electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age. J. Youth Adolesc. 44, 405–418. https://doi.org/10.1007/s10964-014-0176-x (2015).
Chehri, A., Shetabi, M., Khazaie, H. & Zakiei, A. Sleep hygiene and sleep quality in Iranian adolescents during the COVID-19 pandemic. BMC Psychol. 11, 125. https://doi.org/10.1186/s40359-023-01165-8 (2023).
Windred, D. P. et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: A prospective cohort study. Sleep 47, zsad253. https://doi.org/10.1093/sleep/zsad253 (2024).
Chaput, J. P. et al. Sleep duration and health in adults: An overview of systematic reviews. Appl. Physiol. Nutr. Metab. 45, S218–S231. https://doi.org/10.1139/apnm-2020-0034 (2020).
Chaput, J. P. et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 41, S266–282. https://doi.org/10.1139/apnm-2015-0627 (2016).
Liu, Y. et al. Oral Microbiome diversity shapes the association between sleep duration and depression. Front. Neurol. 15, 1442557. https://doi.org/10.3389/fneur.2024.1442557 (2024).
Takao, M. Problematic mobile phone use and big-five personality domains. Indian J. Community Med. 39, 111–113. https://doi.org/10.4103/0970-0218.132736 (2014).
Carvalho, L. F., Sette, C. P. & Ferrari, B. L. Problematic smartphone use relationship with pathological personality traits: Systematic review and meta-analyzes. Cyberpsychol J. Psychosoc Res. Cyberspace. https://doi.org/10.5817/cp2018-3-5 (2018).
Butkovic, A., Vukasovic, T. & Bratko, D. Sleep duration and personality in Croatian twins. J. Sleep. Res. 23, 153–158. https://doi.org/10.1111/jsr.12101 (2014).
Mead, M. P., Persich, M. R., Duggan, K. A., Veronda, A. & Irish, L. A. Big 5 personality traits and intraindividual variability in sleep duration, continuity, and timing. Sleep. Health. 7, 238–245. https://doi.org/10.1016/j.sleh.2020.11.008 (2021).
Vincent, N., Cox, B. & Clara, I. Are personality dimensions associated with sleep length in a large nationally representative sample? Compr. Psychiatry. https://doi.org/10.1016/j.comppsych.2008.07.007 (2009). 158 – 63.
Kang, W., Steffens, F., Pineda, S., Widuch, K. & Malvaso, A. Personality traits and dimensions of mental health. Sci. Rep. 13, 7091. https://doi.org/10.1038/s41598-023-33996-1 (2023).
Komasi, S. et al. Comprehensive meta-analysis of associations between temperament and character traits in Cloninger’s Psychobiological theory and mental disorders. J. Int. Med. Res. 50 https://doi.org/10.1177/03000605211070766 (2022).
Guerreiro, J. et al. The relationship between big five personality traits and sleep patterns: A systematic review. Nat. Sci. Sleep. 16, 1327–1337. https://doi.org/10.2147/NSS.S467842 (2024).
Hintsanen, M. et al. Five-factor personality traits and sleep: Evidence from two population-based cohort studies. Health Psychol. 33, 1214–1223. https://doi.org/10.1037/hea0000105 (2014).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (Vol. 5, No. 5) (American psychiatric association, 2013).
Lawton, E. M. & Oltmanns, T. F. Personality pathology and mental health treatment seeking in a community sample of older adults Personal Ment Health. 7, 203–212. https://doi.org/10.1002/pmh.1198 (2013).
Magee, C. & Biesanz, J. C. Toward Understanding the relationship between personality and well-being States and traits. J. Pers. 87, 276–294. https://doi.org/10.1111/jopy.12389 (2019).
Ringwald, W. R. et al. Role of pregaming motives in accounting for links between maladaptive personality traits and drinking consequences. Pers. Disord. 13, 192–197. https://doi.org/10.1037/per0000540 (2022).
Murawski, B., Wade, L., Plotnikoff, R. C., Lubans, D. R. & Duncan, M. J. A systematic review and meta-analysis of cognitive and behavioral interventions to improve sleep health in adults without sleep disorders. Sleep. Med. Rev. 40, 160–169. https://doi.org/10.1016/j.smrv.2017.12.003 (2018).
Komasi, S. et al. The maladaptive domains according to the alternative model of personality disorders (AMPD) criterion B in patients with affective disorders and temperamental triads related to these domains: two unique profiles. BMC Psychol. 11, 83. https://doi.org/10.1186/s40359-023-01122-5 (2023).
Vaysi, A. et al. Replicability of the five-factor structure of DSM-5 and ICD-11 trait systems and their associations with binge eating and bipolar spectrum psychopathology. Personal Ment Health. 18, 122–137. https://doi.org/10.1002/pmh.1600 (2024).
Khazaie, H. et al. The sensitivity of the ICD-11 trait model to the symptoms of clinical disorders in young adults. Personal Ment Health. 18, 271–283. https://doi.org/10.1002/pmh.1618 (2024).
Khazaie, H., Rezaei, F., Zakiei, A., Faridmarandi, B. & Komasi, S. How are poor sleepers with other clinical conditions affected by maladaptive personality traits? A neural network-based analysis. Front. Psychiatry. 15, 1392525. https://doi.org/10.3389/fpsyt.2024.1392525 (2024).
Zakiei, A. et al. Personality and sleep psychopathology: associations between the DSM-5 maladaptive trait domains and multiple sleep problems in an adult population. Personal Ment Health. 19, e70008. https://doi.org/10.1002/pmh.70008 (2025).
Somma, A. et al. Executive functioning and personality traits in insomnia disorder: A preliminary report on the clinical importance of objective and subjective reduction of total sleep time. Mediterr. J. Clin. Psychol. 8, (2020).
Uygur, O. F. et al. Validity and reliability of the Turkish version of the Glasgow sleep effort scale. Sleep. Med. 98, 144–151. https://doi.org/10.1016/j.sleep.2022.06.022 (2022).
Meia-Via, M. S., Marques, D. R., Espie, C. A., da Silva, C. F. & Allen Gomes, A. Psychometric properties of Glasgow sleep effort scale in Portuguese Language. Psychol. Assess. 28, e12–e18. https://doi.org/10.1037/pas0000178 (2016).
Krueger, R. F., Derringer, J., Markon, K. E., Watson, D. & Skodol, A. E. Initial construction of a maladaptive personality trait model and inventory for DSM-5. Psychol. Med. 42, 1879–1890. https://doi.org/10.1017/S0033291711002674 (2012).
Komasi, S., Sellbom, M. & Hopwood, C. J. Research on the alternative model for personality disorders (AMPD) in Iran: A narrative literature review. Indian J. Psychol. Med. https://doi.org/10.1177/02537176241281888 (2024).
Komasi, S., Kerber, A. & Hopwood, C. A meta-analysis of the structural validity of original and brief versions of the personality inventory for DSM-5 in Iran. Iran. J. Psychiatry. 20, 126–141. https://doi.org/10.18502/ijps.v20i1.17406 (2025).
Buysse, D. J., Reynolds, C. F. 3rd, Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213. https://doi.org/10.1016/0165-1781(89)90047-4 (1989).
Seoane, H. A. et al. Sleep disruption in medicine students and its relationship with impaired academic performance: A systematic review and meta-analysis. Sleep. Med. Rev. 53, 101333. https://doi.org/10.1016/j.smrv.2020.101333 (2020).
Lund, H. G., Reider, B. D., Whiting, A. B. & Prichard, J. R. Sleep patterns and predictors of disturbed sleep in a large population of college students. J. Adolesc. Health. 46, 124–132. https://doi.org/10.1016/j.jadohealth.2009.06.016 (2010).
Gutiérrez Pérez, M. L., Lugo Machado, J. A., Lozano Lavado, V. & Navarro Pimiento, D. C. Sleep and learning: A systematic review. Int. Arch. Otorhinolaryngol. 28, e657–e661. https://doi.org/10.1055/s-0043-1777294 (2024).
Amendola, S., Spensieri, V., Biuso, G. S. & Cerutti, R. The relationship between maladaptive personality functioning and problematic technology use in adolescence: A cluster analysis approach. Scand. J. Psychol. 61, 809–818. https://doi.org/10.1111/sjop.12664 (2020).
Marciano, L., Schulz, P. J. & Camerini, A. L. How smartphone use becomes problematic: application of the ALT-SR model to study the predicting role of personality traits. Comput. Hum. Behav. 119, 106731 (2021).
Zakiei, A. et al. Associations between sleep disturbances, personality traits and self-regulation in a sample of healthy adults. J. Clin. Med. 13, 2143. https://doi.org/10.3390/jcm13072143 (2024).
Akram, U., Stevenson, J. C., Gardani, M., Allen, S. & Johann, A. F. Personality and insomnia: A systematic review and narrative synthesis. J. Sleep. Res. 32, e14031. https://doi.org/10.1111/jsr.14031 (2023).
Komasi, S. et al. Associations between both adaptive and maladaptive personality constructs and emotional load and content of adult Dreams. Indian J. Psychol. Med. https://doi.org/10.1177/02537176241235367 (2024).
Liu, M., Cai, J., Chen, H. & Shi, L. Association of personality traits with life and work of medical students: An integrative review. Int. J. Environ. Res. Public. Health. 19, 12376. https://doi.org/10.3390/ijerph191912376 (2022).
Parks-Leduc, L., Feldman, G. & Bardi, A. Personality traits and personal values: A meta-analysis. Pers. Soc. Psychol. Rev. 19, 3–29. https://doi.org/10.1177/1088868314538548 (2015).
Kim, H. N. et al. Association between personality traits and sleep quality in young Korean women. PLoS One. 10, e0129599. https://doi.org/10.1371/journal.pone.0129599 (2015).
Zhao, D., Wang, H., Feng, X., Lv, G. & Li, P. Relationship between neuroticism and sleep quality among asthma patients: The mediation effect of mindfulness. Sleep. Breath. 23, 925–931. https://doi.org/10.1007/s11325-019-01814-6 (2019).
Allen, M. S., Magee, C. A. & Vella, S. A. Personality, hedonic balance and the quality and quantity of sleep in adulthood. Psychol. Health. 31, 1091–1107. https://doi.org/10.1080/08870446.2016.1178745 (2016).
Uygur, O. F. et al. Type D personality to insomnia: sleep reactivity, Sleep effort, and sleep hygiene as mediators. Front. Psychiatry. 14, 1160772. https://doi.org/10.3389/fpsyt.2023.1160772 (2023).
Akram, U. et al. The relationship between type D personality and insomnia. Sleep. Health. 4, 360–363. https://doi.org/10.1016/j.sleh.2018.04.005 (2018).
Giordano, A., Di Ponzio, M. & Cicolin, A. Psychological interventions in behavioral sleep medicine: an overview for clinicians and psychologists. Ann. Psychiatry Treat. 6, 33–48 (2022).
Widiger, T. A. & Crego, C. HiTOP thought disorder, DSM-5 psychoticism, and five factor model openness. J. Res. Pers. 80, 72–77. https://doi.org/10.1016/j.jrp.2019.04.008 (2019).
Keskin, G., Gümüşsoy, S. & Taşdemir Yiğitoğlu, G. The relationship between sleep quality and fear of COVID-19, anxiety, personality traits in working women. Work https://doi.org/10.3233/WOR-230724 (2024).
Acknowledgements
We acknowledge the Sleep Disorders Research Center (Kermanshah University of Medical Sciences) and Mind GPS Institute (Kermanshah) for improving the quality of the scientific content of this work.
Funding
This research project has not received any financial support from any person or organization.
Author information
Authors and Affiliations
Contributions
A.Z. H.K. and S.K. collaboratively designed and conducted the study. A.Z. collected and analyzed the data and prepared first draft with the support of H.K. and S.K. The critical review process was performed by H.K. and S.K. All authors have seen and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants gave informed consent to participate and study protocol was approved by the ethics committee of the Kermanshah University of Medical Sciences (Code: IR.KUMS.REC.1403.365).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.

Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zakiei, A., Khazaie, H. & Komasi, S. The role of the DSM-5 maladaptive personality traits in adherence to sleep hygiene behaviors and sleep duration. Sci Rep 15, 16196 (2025). https://doi.org/10.1038/s41598-025-01308-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01308-4
Keywords
This article is cited by
-
Comparing DSM-5 Pathological Personality Traits in Youths With ADHD, Subthreshold ADHD, and Healthy Controls Using the Personality Inventory for DSM-5 (PID-5): A Network Analysis Study
Journal of Autism and Developmental Disorders (2025)

{kind=link}