
Abstract
Coronary artery disease (CAD) is a prevalent and high-mortality condition globally. The awareness regarding adequate oral care in China was insufficient. This study investigates the outcomes of CAD patients in southwest China based on their tooth brushing frequency. A total of 841 CAD patients were selected from a cohort of 32,709 residents. Over a four-year follow-up period, the incidence of three-point major adverse cardiovascular events (3P-MACEs) was evaluated. The results indicated that the hazard ratios (HR) with 95% confidence intervals (CIs) for 3P-MACEs among the three groups of tooth brushing frequency (twice, once, and thrice daily) were: reference, 1.61 (1.09–2.37) (p = 0.017), and 0.49 (0.15–1.62) (p = 0.241). Patients who brushed their teeth only once a day had a 1.71 (1.18–2.46) times higher risk compared to those who brushed twice or more daily (p = 0.004). In conclusion, insufficient tooth brushing frequency appears to be associated with a higher risk of adverse outcomes among CAD patients.
Similar content being viewed by others

Introduction
Coronary artery disease (CAD) is a prevalent chronic condition associated with a high global mortality rate1,2,3,4. The composite endpoint of three-point major adverse cardiovascular events (3P-MACEs), which includes cardiovascular death, myocardial infarction (MI), or stroke, represents an important primary endpoint for cardiovascular outcome trials5,6,7.
Atherosclerosis can lead to the formation of lesions in coronary arteries8. The possible pathogenesis of atherosclerosis encompasses vascular endothelial dysfunction, dyslipidemia, inflammatory and immune responses, and plaque rupture9,10,11,12,13. In addition to age and gender, nine modifiable risk factors—abnormal lipid profiles, smoking, hypertension, diabetes mellitus (DM), abdominal obesity, psychosocial stressors, inadequate fruit and vegetable intake, excessive alcohol consumption, and insufficient physical activity—are responsible for the majority of CAD cases14.
Previous studies have indicated that oral hygiene is closely associated with the morbidity and mortality of cardiovascular diseases (CVDs)15,16,17,18. Some even reported that more frequent tooth brushing could reduce the risk of CVDs effectively19,20. Regrettably, Chinese who brushed their teeth twice a day or more only accounted for 36.8%21. Besides, a national survey highlighted that individuals’ oral health behavior could not match the improvement of knowledge and attitudes in China after decades of oral health education22. Although the exact mechanisms linking poor tooth brushing frequency to CVDs are still not fully understood, it was proved that poor oral hygiene may increase cardiovascular risk by triggering systemic inflammation, raising markers like C-reactive protein (CRP) and fibrinogen23,24, and contributing to endothelial dysfunction through periodontal infections15.
Nevertheless, the existing literature has inadequately addressed the relationship between tooth brushing frequency and CAD in underdeveloped regions of China. Therefore, our study aimed to evaluate the association between tooth brushing frequency and clinical outcomes among residents diagnosed with CAD in southwest China.
Materials and methods
Study design
This project is a sub-project of the National Key R&D Program of China (2018YFC1311400), with data collected from 16 districts and counties in Chongqing, southwest China, under the guidance of the Health Commission and the Center for Disease Control and Prevention from year 2018 to 202025. The Cardiovascular Department of the First Affiliated Hospital of Chongqing Medical University conducted a comprehensive cross-sectional survey of community residents through stratified random sampling, followed by a retrospective follow-up survey on individuals diagnosed with CAD during the initial investigation26.
During the baseline data collection, investigators consisted of healthcare workers from local healthcare facilities. The survey methodology predominantly utilized standardized questionnaires administered through face-to-face interviews and telephone conversations (refer to Supplementary material 1)25,26. To assess the overall stability of living conditions, participants were requested to provide information regarding their daily habitual lifestyles over the past 5 years26,27. They were also instructed to fast for a minimum of 7 h prior to serum blood lipid and glucose tests26, with all requisite testing equipment supplied by community medical facilities.
The follow-up procedures were conducted by a trained research team, and the medical records of the participants were obtained from healthcare providers to serve as confirmation sources. Data entry into the study system was performed by dedicated data entry clerks and subjected to stratified sampling checks to ensure authenticity and reliability.
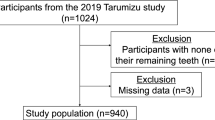
In this initial cross-sectional study, a total of 32,709 residents aged 18 years and older were screened26. Among these, 1124 individuals were diagnosed with CAD, defined as having at least one coronary artery with stenosis ≥ 50%, as determined by percutaneous coronary angiography or computed tomography angiography28, at the time of the survey. 13 subjects were excluded from the analysis due to inaccurate or missing key data. During the observational follow-up period from year 2018 to 2023, 39 participants were excluded due to alterations in their habitual tooth brushing frequency. Additionally, 123 participants were lost to follow-up, 62 declined to continue participating in the study, and 46 died from causes unrelated to CAD or cardiovascular diseases. As a result, a total of 841 CAD patients remained in the study (Fig. 1).

The study flow chart.
The tooth brushing frequency refers to the average daily habitual tooth brushing times over the past 5 years29. CAD residents were categorized into three groups: once, twice, and thrice, based on the distribution characteristics of the data. The primary endpoint was the composite of 3P-MACEs5.
This study was approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University. All participants agreed on the study content and signed informed consent.
Definition of terms
The key demographics and lifestyle factors in this study were defined as follows26,30. Solitary living was characterized by an individual residing an average of 26 or more days per month without companionship. Well-educated referred to an individual who had completed at least a high school education. High income was defined as an average monthly income exceeding 5,000 CNY. The term “CVD family history” indicated the presence of any documented first-degree relative with CVD. Both smoking and alcohol intake involved engaging in these habits at least three times weekly. A salty and greasy diet implied favoring salt-rich foods (e.g. pickles, preserved food) or those abundant in fats (e.g. fried dishes). Favors of vegetables, fruits, and yogurt were defined as the weekly inclination to consume these food items for more than five days. Physical inactivity encompassed engaging in labor or exercise for less than 20 h each week.
The diagnosis of the following diseases necessitates confirmation through medical tests or documents conducted at a secondary or tertiary healthcare facility.
Periodontitis is characterized by chronic or acute inflammation of the periodontal tissues. Its clinical manifestations include gingival redness and swelling, bleeding upon probing, periodontal pocket formation, and tooth mobility31,32, as documented in participants’ medical records or observed during oral examinations.
Hypertension was defined when any one of the three criteria was satisfied: (a) the systolic blood pressure (SBP) ≥ 140 mmHg or (b) the diastolic blood pressure (DBP) ≥ 90 mmHg on multiple occasions during periods of calmed rest or (c) under the use of antihypertensive medication33.
Chinese criteria of weight for adults defined obesity as body mass index (BMI) ≥ 28 kg/m234.
The diagnosis of diabetes mellitus (DM) should follow fasting plasma glucose (FPG) ≥ 7.0 mmol/L, and/or 2 h-post challenge plasma glucose (PG) ≥ 11.1 mmol/L, and/or HbA1c ≥ 48 mmol/mol35, and/or under hypoglycemic drugs use.
Hyperlipidemia was diagnosed as any of the followings : (a) total cholesterol (TC) > 5.7 mmol/L; (b) triglyceride (TG) > 1.7 mmol/L; (c) low density lipoprotein-C (LDL-C) > 3.37 mmol/L; (d) use of lipid-lowering drugs36.
Stroke encompassed both ischemic strokes and hemorrhagic strokes, which had been identified through cranial imaging37.
The diagnosis of MI was made when there was an elevation in serum cardiac markers accompanied by any one of the following: (a) symptoms of myocardial ischemia; (b) new ECG changes; (c) imaging evidence of decreased viable myocardium or abnormal new ventricular wall motion38.
Peripheral artery disease (PAD) was defined as a kind of atherosclerotic disease, affecting the aorta or arteries in lower extremities39.
Atrial fibrillation was detected based on electrocardiogram40.
CAD-caused mortality referred to the occurrence of death or sudden death resulting from CAD or its complications41,42, as confirmed or inferred by medical documentation, while excluding the possibility of other underlying diseases or accidents.
Data analysis
Continuous variables with a normal distribution were expressed as mean ± standard deviation (SD), and one-way analysis of variance (ANOVA) was employed to compare the differences between groups in cases where the variances exhibited homogeneity. Otherwise, the median and inter quartile range (25%-75%) were reported, and the Kruskal–Wallis test was utilized for comparing group differences. Categorical variables were presented as numbers with percentages (n%), and comparison between groups was conducted using Pearson χ2 test.
Considering that the endpoint event of this study is time-dependent, Kaplan–Meier (KM) plots including log-rank tests were utilized to assess the relationship between tooth brushing frequency and outcome events across the three groups. Subsequently, Cox regression analysis was conducted to examine the impact of tooth brushing frequency on outcome events, after adjusting for recognized prognostic factors. In addition, hazard ratio (HR) values with 95% confidence intervals (CI) and p values were calculated. For daily tooth brushing frequency, the group of 2 times per day served as the reference.
Data analyses were performed on IBM SPSS Statistics, version 28 (IBM Corporation, Armonk, NY, USA) and diagrams were generated on Prism version 9. Statistical significance was set as p value < 0.05 (two-sided).
Results
The prevalence of CAD in this population was 3.4% (1124/32,709). We recruited 841 CAD residents, 59.7% of them were female, and the average age of the participants was 69.2 ± 8.2 years old (ranging from 27–92 years). As displayed in Table 1, the distribution of habitual daily brushing frequency (1, 2, 3) was 48.6%, 45.8%, and 5.6% respectively, with no residents reporting zero or more than four times of tooth brushing.
As presented in Table 2, CAD participants who brushed their teeth once a day exhibited lower levels of education and income, higher proportions of consuming a salty diet, more likely to experience periodontitis and tooth loss, elevated levels of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C), but lower levels of high-density lipoprotein cholesterol (HDL-C). On the other hand, individuals who brushed their teeth twice daily or more had a reduced likelihood of having a CVD family history, and showed higher preferences for vegetables, fruits, and yogurt, and tended to brush their teeth both in the morning and at night. They also had greater height and weight. However, among the three groups, gender, solitary living, smoking habits, alcohol consumption, greasy diet intake, and physical inactivity were comparable. Additionally, they all had similar ages, body mass index (BMI), heart rate values, blood pressure readings, triglyceride levels, and fasting glucose concentrations.
According to Table 3, at baseline, participants with CAD who brushed their teeth once a day had a lower prevalence of stroke and a lower proportion of lipid-lowering drugs use. Apart from this, there were no significant differences in comorbidity and medication use among the three groups at baseline. However, during follow-up, individuals who brushed their teeth once a day had the highest rate of 3P-MACEs (18.1%), new stroke (5.4%) and CAD-related death (7.8%), and a lower proportion of lipid-lowering drugs use. There were no notable differences in the prevalence of new MI or the use of anti-hypertensive, anti-hyperglycemic, and anti-thrombotic drugs among the three groups. Over the four-year follow-up period, 121 cases (14.4%) within the general cohort were found to suffer from 3P-MACEs, with 31 new stroke cases (3.7%), 68 new MI cases (8.1%), and 42 deaths (5.0%) attributed to CAD.
The KM curves in Fig. 2 revealed that compared to a daily tooth brushing frequency of 2 times, individuals who brushed their teeth only once had a significantly higher probability of 3P-MACEs, with an HR of 1.66 (95% CI: (1.14–2.41) (log rank p = 0.008).

Comparison of the 3P-MACEs incidence across the three groups by Kaplan-Meier survival curves.
After multivariate adjustments, Cox regression analysis presented in Fig. 3 revealed the HR with 95% CIs among the three groups of tooth brushing frequency (2, 1, and 3 times per day), for 3P-MACEs were: reference, 1.61 (1.09–2.37) (p = 0.017), and 0.49 (0.15–1.62) (p = 0.241) (seen in Table 4); for new stroke: reference, 2.51 (1.08–5.80) p = 0.032), and 1.09 (0.13–8.97) p = 0.935) (Supplementary Table 1); for new MI: reference, 1.05 (0.63–1.76) (p = 0.852), and 0.70 (0.20–2.46) (p = 0.580) (Supplementary Table 2); for CAD-related death: reference, 3.83 (1.69–8.66) (p = 0.001), and 1.37 (0.25–7.46) p = 0.714) (Supplementary Table 3).

Association between tooth brushing frequency with 3P-MACEs and its components by multivariate Cox regression analysis.
After being divided into two groups (1, ≥ 2) based on tooth brushing frequency, individuals who brushed their teeth once a day had an increased risk of 3P-MACEs in the majority of subgroups, with an overall HR of 1.71 (1.18–2.46) (p = 0.004) (Fig. 4).

Subgroups analysis (adjusted by age) for 3P-MACEs between the two groups.
Discussion
The present study was a retrospective analysis conducted on residents diagnosed with CAD in southwest China. The key findings were: (1) Only 51.4% of the participants reported brushing their teeth twice or more daily. (2) The prevalence of CAD among the general population was found to be 3.4%. Additionally, over a four-year follow-up period, the incidence rates of 3P-MACEs, new stroke, new MI, and CAD-caused mortality were observed to be 14.4%, 3.7%, 8.1%, and 5.0%, respectively. (3) Inadequate tooth brushing frequency may potentially increase the risk of 3P-MACEs.
Oral health promotion has attracted increased attention from the public in China43. However, approximately 19.3% of Chinese suffered from severe periodontal diseases in 201944. Our study found that the prevalence of periodontitis was 34.4%, and 13.7% of the residents who had missing teeth. This was only a rough investigation and analysis, the actual prevalence rate could be definitely higher than this, as some residents had never visited an oral medical institution. Besides, only less than 20% of Chinese adults had a good understanding of periodontal diseases, which revealed that the Chinese population’s cognition of oral health has not significantly developed over the years45. From another perspective, public health strategies regarding periodontal health remained insufficient45. Until 2021, in the primary care services of the public health department, the procedures for diagnosis and management of periodontal diseases were incomplete46. Curative and rehabilitation oral health care was still not covered in health benefits packages for Chinese citizens, only routine and preventive oral care was provided46.
It was recommended that tooth brushing more than twice per day was significant for preventing caries47, before bedtime and on other occasions48,49. According to the Adult Oral Survey 2021 in the UK, approximately 77% of adults (16 years and over) reported brushing their teeth at least twice daily, while 20% indicated they brushed once per day. Only 2% stated they brushed their teeth less frequently than once a day50. In the last 5 years, studies about Chinese citizens’ oral care, oral hygiene, and tooth brushing habits were limited. Therefore, according to newly published data from the 4th national oral health epidemiology survey in 2016, oral diseases remained highly prevalent in China43. Nevertheless, access to specialized dental care was limited for most citizens, and many individuals found it unaffordable because of restricted insurance coverage43. Although the study population was limited, our research observed that 78.8% of residents brushed their teeth in the morning, whereas 70.0% did so in the evening. Notably, nearly half of the respondents did not meet the recommended frequency for tooth brushing. This phenomenon exhibited residents’ neglect of oral health to some degree.
The incidence of CAD has rapidly increased over the past two decades, and the estimated number of CAD patients in China for the year 2022 was 11.39 million51, making it the second leading cause of death52,53,54. Consequently, this has imposed a substantial economic burden on society55,56. The main findings of our study align with the results documented in the existing literature, that a reduced daily frequency of tooth brushing may increase adverse cardiovascular outcomes29,57,58,59,60,61.
For instance, Oliveira et al. reported that CAD had the highest proportion of cardiovascular events caused by poor oral hygiene, they reported an HR for fatal CVD of 2.40 (1.50–4.00) for tooth brushing less than once a day within 8.1 follow-up years23. In addition, research by Zhuang et al.24 and Zhou et al.57 discovered that less tooth brushing frequency was associated with an increased risk of all-cause mortality. Similarly, Matsui et al.’s research proved that insufficient frequency and short duration of tooth brushing (< twice/day and < 2 min/procedure) were associated with a higher risk of major adverse cardiovascular events including acute MI, with an HR of 3.06 (1.24–7.63)15. A prior study by Chang et al. analyzed 206,602 individuals indicating that frequent tooth brushing (≥ 3 times/day) was associated with a reduced stroke risk (HR: 0.80; 95% CI 0.75–0.85; p < 0.001)58. Additionally, individuals who brushed their teeth more frequently were reported to have lower 10-year cardiovascular risk59. Moreover, a systematic review also highlighted a significant negative correlation between the frequency of tooth brushing and CVD risk35. These findings further support the link between poor periodontal health status and an elevated risk of CVD23.
In contrast, our study, which featured a 4-year follow-up period, demonstrated that CAD participants who brushed their teeth once daily had a significantly higher HR for new stroke events and CAD-related mortality, compared to those who brushed twice daily. Furthermore, those who brushed once daily exhibited an elevated risk of 3P-MACEs.
Conversely, although the group that brushes once daily has the highest incidence of new-onset MI (8.6%), our findings did not reveal that tooth brushing frequency had a remarkable influence on the incidence of new-onset MI among CAD residents. This may be attributed to the fact that our study population exclusively comprised CAD patients from southwest China, with MI cases limited to newly occurring events. Additionally, the CAD patient group may have exhibited a lower propensity to initiate and adhere to anti-platelet and lipid-lowering medications both at baseline and during follow-up after diagnosis. During the follow-up period, the research team may also provide additional medical advice to reduce the likelihood of progression to MI. However, this does not negate the potential benefits of regular oral hygiene behaviors such as tooth brushing.
Owing to the inherent limitations of the research design, it was not feasible to provide a detailed description of the oral hygiene characteristics of the population or to adjust for relevant confounding factors. Individuals with varying tooth brushing frequencies exhibit differences in demographic, social, psychological, economic, and physical conditions. Nevertheless, based on the aforementioned literature and our study findings, multi-factor correction analyses were conducted across different regions and populations, yielding consistent conclusions. Particularly, in our subgroup analysis, most subgroups demonstrated that less frequent tooth brushing was associated with 3P-MACEs, suggesting this was not a random occurrence. Therefore, we posit that reduced frequency of tooth brushing is likely to constitute a significant potential risk factor for adverse cardiovascular events.
The exact physiological mechanisms linking tooth brushing frequency to cardiovascular events are not yet fully understood. Nevertheless, there were researches revealing that insufficient tooth brushing frequency was closely associated with periodontitis60,61.
In Cho et al.’s study60, the frequency of tooth brushing made a significant impact on the classification of periodontal conditions. Compared with the healthy group, participants with severe periodontal disease showed a higher incidence of 26% for acute MI (HR: 1.26, 95% CI 1.13–1.42)60. During 10 years, acute MI presented more in people with severe periodontal conditions than people with no severe periodontal conditions (healthy or moderate periodontal conditions): 1.0% vs. 0.7%60.
Current evidence indicates that chronic bacteremia and low-grade systemic inflammation associated with periodontitis may significantly contribute to the development of atherosclerosis and related CVDs62. Elevated levels of CRP are strongly correlated with the incidence of cardiovascular metabolic diseases and have adverse effects on individuals with pre-existing cardiovascular conditions63. Systemic inflammation or immune responses elicited by periodontal infections can result in increased concentrations of white blood cells, CRP, and pro-inflammatory cytokines, thereby exacerbating the inflammatory state and potentially increasing the risk of cardiovascular events29,64. Moreover, periodontal pathogens can directly adhere to endothelial cells and colonize atherosclerotic plaques, leading to plaque instability and possibly triggering thrombotic events associated with atherosclerosis64. Research has demonstrated that enhancing oral hygiene practices can reduce levels of inflammatory markers such as CRP, further inhibiting the role of oral bacteria in driving systemic inflammation63,65.
Our research indicates that individuals who brush their teeth once daily exhibit a higher prevalence of periodontitis and tooth loss, suggesting suboptimal oral hygiene practices. We hypothesize that these individuals might have elevated levels of inflammatory mediators in their blood, although this could not be confirmed through blood tests in this present study. Furthermore, those with less frequent brushing habits tend to have lower educational attainment and income levels, this demographic is also less likely to engage in healthy lifestyles. Lastly, despite the established protective effects of lipid-lowering drugs against cardiovascular events66,67, these patients present relatively higher cholesterol levels and lower utilization rates of lipid-lowering medications, thereby diminishing the potential protective benefits. In conclusion, these hypotheses may elucidate the observed association in our study population between less frequent tooth brushing among CAD patients and an increased risk of 3P-MACEs.
Study strengths
We are one of the limited number of studies that have examined the prognosis of CAD residents with varying tooth-brushing habits in Southwest China. Our data sources are robust and the follow-up duration is substantial (4 years). While no direct interventions were implemented, this study has facilitated awareness among residents regarding the significance of proper oral hygiene. Furthermore, it has provided healthcare professionals with valuable insights to assist CAD patients in modifying unhealthy lifestyles.
Limitations
Despite the significant contributions of our research, several limitations should be acknowledged. (1) The study sample, although derived from a large epidemiological dataset, was confined to patients with a definitive diagnosis of CAD in the southwest region of China, resulting in a relatively limited sample size and geographical scope. Consequently, further large-scale, multi-regional studies are warranted to validate our findings. (2) This study adopted a retrospective design rather than a prospective one. Although we endeavored to adjust for confounding factors influencing cardiovascular prognosis based on existing literature, inherent limitations of retrospective studies may still introduce biases. Factors such as the event rate, sample size, and unmeasured covariates could potentially affect the results. (3) Our analysis focused solely on tooth brushing frequency, unable to consider other important aspects such as brushing technique, duration, or quality, nor did it examine the diagnosis and treatment of oral diseases. The absence of this information might introduce bias into our results. Additionally, unlike some other studies that included individuals with zero tooth brushing frequency as a reference group, our study lacked such a cohort due to the nature of our sample. Therefore, future research should aim to address these limitations through carefully designed prospective studies involving diverse populations.
Conclusions
Our study suggests that, among CAD residents in southwest China, a lower tooth brushing frequency (once a day) appeared to an increased risk of 3P-MACEs, new onset stroke, and mortality caused by CAD, however, there is no significant association between tooth brushing frequency and the onset of new MI.
Data availability
The dataset used and analyzed in this study is available from the corresponding author [GL] upon reasonable request.
References
Malakar, A. K. et al. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol. 234, 16812–16823. https://doi.org/10.1002/jcp.28350 (2019).
Khera, A. V. & Kathiresan, S. Genetics of coronary artery disease: Discovery, biology and clinical translation. Nat. Rev. Genet. 18, 331–344. https://doi.org/10.1038/nrg.2016.160 (2017).
McCullough, P. A. Coronary artery disease. Clin. J. Am. Soc. Nephrol. CJASN 2, 611–616. https://doi.org/10.2215/CJN.03871106 (2007).
Roth, G. A. et al. Global, regional, and National Burden of Cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 70, 1–25. https://doi.org/10.1016/j.jacc.2017.04.052 (2017).
Bosco, E., Hsueh, L., McConeghy, K. W., Gravenstein, S. & Saade, E. Major adverse cardiovascular event definitions used in observational analysis of administrative databases: A systematic review. BMC Med. Res. Methodol. 21, 241. https://doi.org/10.1186/s12874-021-01440-5 (2021).
Sharma, A. et al. Impact of regulatory guidance on evaluating cardiovascular risk of new glucose-lowering therapies to treat type 2 diabetes mellitus: lessons learned and future directions. Circulation 141, 843–862. https://doi.org/10.1161/CIRCULATIONAHA.119.041022 (2020).
El Sanadi, C. E., Ji, X. & Kattan, M. W. 3-point major cardiovascular event outcome for patients with T2D treated with dipeptidyl peptidase-4 inhibitor or glucagon-like peptide-1 receptor agonist in addition to metformin monotherapy. Ann. Transl. Med. 8, 1345. https://doi.org/10.21037/atm-20-4063 (2020).
Faxon, D. P. et al. Atherosclerotic vascular disease conference: Writing Group III: Pathophysiology. Circulation 109, 2617–2625. https://doi.org/10.1161/01.CIR.0000128520.37674.EF (2004).
Crea, F., Camici, P. G. & Bairey Merz, C. N. Coronary microvascular dysfunction: An update. Eur. Heart J. 35, 1101–1111. https://doi.org/10.1093/eurheartj/eht513 (2014).
Hansson, G. K. Inflammation, atherosclerosis, and coronary artery disease. N Engl. J. Med. 352, 1685–1695. https://doi.org/10.1056/NEJMra043430 (2005).
Weber, C. & Noels, H. Atherosclerosis: Current pathogenesis and therapeutic options. Nat. Med. 17, 1410–1422. https://doi.org/10.1038/nm.2538 (2011).
Steinberg, D. & Witztum, J. L. Oxidized low-density lipoprotein and atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 30, 2311–2316. https://doi.org/10.1161/ATVBAHA.108.179697 (2010).
Frohlich, J. & Al-Sarraf, A. Cardiovascular risk and atherosclerosis prevention. Cardiovasc. Pathol. 22, 16–18. https://doi.org/10.1016/j.carpath.2012.03.001 (2013).
Yusuf, S. et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 364, 937–952. https://doi.org/10.1016/S0140-6736(04)17018-9 (2004).
Matsui, S. et al. Poor tooth brushing behavior is associated with high risk of cardiovascular events: A prospective observational study. Int. J. Cardiol. 350, 111–117. https://doi.org/10.1016/j.ijcard.2021.12.056 (2022).
Wang, Y. et al. Associations of oral hygiene with incident hypertension and type 2 diabetes mellitus: A population based cohort study in Southwest China. J. Clin. Hypertens. (Greenwich, Conn) 24, 483–492. https://doi.org/10.1111/jch.14451 (2022).
Persson, G. R. & Imfeld, T. Parodontitis und Herz-kreislaufkrankheiten [Periodontitis and cardiovascular disease]. Ther. Umschau. Rev. Ther. 65, 121–126. https://doi.org/10.1024/0040-5930.65.2.121 (2008).
Sanz, M. et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 47, 268–288. https://doi.org/10.1111/jcpe.13189 (2020).
Park, S. Y. et al. Improved oral hygiene care attenuates the cardiovascular risk of oral health disease: A population-based study from Korea. Eur. Heart J. 40, 1138–1145. https://doi.org/10.1093/eurheartj/ehy836 (2019).
Liu, Y. et al. Association between the frequency of tooth brushing and the risk of cardiovascular disease: A systematic review and meta-analysis. Angiology 23, 33197231219836. https://doi.org/10.1177/00033197231219836 (2024).
Chang, Q. et al. Decomposing socioeconomic inequalities in dental caries among Chinese adults: Findings from the 4th national oral health survey. BMC Oral Health 23, 372. https://doi.org/10.1186/s12903-023-03037-4 (2023).
Li, M. et al. Comparison of oral health behaviour between dental and non-dental undergraduates in a university in southwestern China–exploring the future priority for oral health education. BMC Oral Health 20, 249. https://doi.org/10.1186/s12903-020-01232-1 (2020).
de Oliveira, C., Watt, R. & Hamer, M. Toothbrushing, inflammation, and risk of cardiovascular disease: Results from Scottish Health Survey. BMJ 340, c2451. https://doi.org/10.1136/bmj.c2451 (2010).
Zhuang, Z. et al. Associations of toothbrushing behaviour with risks of vascular and nonvascular diseases in Chinese adults. Eur. J. Clin. Invest. 51, e13634. https://doi.org/10.1111/eci.13634 (2021).
He, J. & He, Q. Association between sleep duration and hypertension among adults in Southwest China. Glob Heart. 17, 10. https://doi.org/10.5334/gh.1100 (2022).
Li, J., Lu, Y., Zhang, X. & Liu, G. Associations between sleep duration and cardiometabolic diseases among residents in Southwest China. Nat. Sci. Sleep. 16, 1121–1130. https://doi.org/10.2147/NSS.S466283 (2024).
Wendel-Vos, G. C. et al. Lifestyle factors of a five-year community-intervention program: The Hartslag Limburg intervention. Am. J. Prev. Med. 37, 50–56. https://doi.org/10.1016/j.amepre.2009.03.015 (2009).
Schmidt, S. E. et al. Coronary artery disease detected by low frequency heart sounds. Cardiovasc. Eng. Technol. 13, 864–871. https://doi.org/10.1007/s13239-022-00622-6 (2022).
Kobayashi, D., Mizuno, A., Mitsui, R. & Shimbo, T. Frequency of daily tooth brushing and subsequent cardiovascular events. Coron. Artery Dis. 31, 545–549. https://doi.org/10.1097/MCA.0000000000000882 (2020).
Liu, G. et al. Association of age at menarche with obesity and hypertension among southwestern Chinese women: A new finding. Menopause 25, 546–553. https://doi.org/10.1097/GME.0000000000001027 (2018).
Tonetti, M. S., Greenwell, H. & Kornman, K. S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol. 89(Suppl 1), S159–S172. https://doi.org/10.1002/JPER.18-0006 (2018).
Mehrotra, N. & Singh, S. Periodontitis (StatPearls, 2022).
Browne, L. D. et al. Prevalence, awareness, treatment, and control of hypertension in community-dwelling older adults with chronic kidney disease: The Irish longitudinal study on ageing. Clin. Kidney J. 17, sfae184. https://doi.org/10.1093/ckj/sfae184 (2024).
Hu, H. et al. BMI, waist circumference and all-cause mortality in a middle-aged and elderly Chinese population. J. Nutr. Health Aging 22, 975–981. https://doi.org/10.1007/s12603-018-1047-z (2018).
ElSayed, N. A. et al. 2. Classification and diagnosis of diabetes: Standards of care in diabetes-2023. Diabetes Care 46, S19–S40. https://doi.org/10.2337/dc23-S002 (2023).
Awadji, F. B. et al. Association between testosterone/estradiol ratio and risk of cardiometabolic diseases in women at menopause transition age. Clin. Exp. Obstet. Gynecol. 49, 260. https://doi.org/10.31083/j.ceog4912260 (2022).
Lee, E. C. et al. Utility of exosomes in ischemic and hemorrhagic stroke diagnosis and treatment. Int. J. Mol. Sci. 23, 8367. https://doi.org/10.3390/ijms23158367 (2022).
Thygesen, K. et al. Fourth universal definition of myocardial infarction (2018). J. Am. Coll. Cardiol. 72, 2231–2264. https://doi.org/10.1016/j.jacc.2018.08.1038 (2018).
Krawisz, A. K., Raja, A. & Secemsky, E. A. Femoral-popliteal peripheral artery disease: From symptom presentation to management and treatment controversies. Prog. Cardiovasc. Dis. 65, 15–22. https://doi.org/10.1016/j.pcad.2021.02.004 (2021).
Zimetbaum, P. Atrial fibrillation. Ann. Intern. Med. 166, ITC33–ITC48. https://doi.org/10.7326/AITC201703070 (2017).
Duggan, J. P., Peters, A. S., Trachiotis, G. D. & Antevil, J. L. Epidemiology of coronary artery disease. Surg. Clin. North Am. 102, 499–516. https://doi.org/10.1016/j.suc.2022.01.007 (2022).
Fadah, K. & Payan-Schober, F. Physical activity and mortality in patients with coronary artery disease. Curr. Cardiol. Rep. 25, 663–667. https://doi.org/10.1007/s11886-023-01890-x (2023).
Zhou, X. et al. Oral health in China: From vision to action. Int. J. Oral Sci. 10, 1. https://doi.org/10.1038/s41368-017-0006-6 (2018).
Jain, N., Dutt, U., Radenkov, I. & Jain, S. WHO’s global oral health status report 2022: Actions, discussion and implementation. Oral Dis. 30, 73–79. https://doi.org/10.1111/odi.14516 (2024).
Zhao, Q. et al. Periodontal health: A national cross-sectional study of knowledge, attitudes and practices for the public oral health strategy in China. J. Clin. Periodontol. 46, 406–419. https://doi.org/10.1111/jcpe.13082 (2019).
Noncommunicable Diseases, Rehabilitation and Disability (NCD). Oral Health China 2022 country profile. World Health Organization. (2022). https://www.who.int/publications/m/item/oral-health-chn-2022-country-profile
Kumar, S., Tadakamadla, J. & Johnson, N. W. Effect of toothbrushing frequency on incidence and increment of dental caries: A systematic review and meta-analysis. J. Dent. Res. 95, 1230–1236. https://doi.org/10.1177/0022034516655315 (2016).
Marinho, V. C., Higgins, J. P., Sheiham, A. & Logan, S. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 203, CD002278. https://doi.org/10.1002/14651858.CD002278 (2003).
Glenny, A. M. et al. Development of tooth brushing recommendations through professional consensus. Int. Dent. J. 74, 526–535. https://doi.org/10.1016/j.identj.2023.10.018 (2024).
Office for Health Improvement and Disparities. Adult oral health survey 2021: Health-related behaviours. GOV.UK https://www.gov.uk/government/statistics/adult-oral-health-survey-2021/adult-oral-health-survey-2021-health-related-behaviours#contents (2024).
The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2022: An updated summary. Biomed. Environ. Sci. BES. 36, 669–701 https://doi.org/10.3967/bes2023.106 (2023).
Yang, G. et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet (London, England). 381, 1987–2015. https://doi.org/10.1016/S0140-6736(13)61097-1 (2013).
Zhang, G. et al. Burden of Ischaemic heart disease and attributable risk factors in China from 1990 to 2015: Findings from the global burden of disease 2015 study. BMC Cardiovasc. Disord. 18, 18. https://doi.org/10.1186/s12872-018-0761-0 (2018).
Huang, J., Zeng, Q., Pan, X., Guo, X. & Li, G. Projections of the effects of global warming on the disease burden of ischemic heart disease in the elderly in Tianjin, China. BMC Public Health 19, 1465. https://doi.org/10.1186/s12889-019-7678-0 (2019).
Song, X., Lan, L., Zhou, T., Yin, J. & Meng, Q. Economic burden of major diseases in China in 2013. Front. Public Health 9, 649624. https://doi.org/10.3389/fpubh.2021.649624 (2021).
Chen, P. et al. Economic burden of myocardial infarction combined with dyslipidemia. Front. Public Health 9, 648172. https://doi.org/10.3389/fpubh.2021.648172 (2021).
Zhou, B. J. et al. Association of oral health with all-cause and cause-specific mortality in older Chinese adults: A 14-year follow-up of the Guangzhou Biobank Cohort study. J. Glob. Health 14, 04111. https://doi.org/10.7189/jogh.14.04111 (2024).
Chang, Y., Woo, H. G., Lee, J. S. & Song, T. J. Better oral hygiene is associated with lower risk of stroke. J. Periodontol. 92, 87–94. https://doi.org/10.1002/JPER.20-0053 (2021).
Moon, M. G. et al. Association between toothbrushing and cardiovascular risk factors: A cross-sectional study using Korean National Health and Nutrition Examination Survey 2015–2017. BMC Oral Health 24, 4. https://doi.org/10.1186/s12903-023-03775-5 (2024).
Cho, H. J. et al. Severe periodontal disease increases acute myocardial infarction and stroke: A 10-year retrospective follow-up study. J. Dent. Res. 100, 706–713. https://doi.org/10.1177/0022034520986097 (2021).
Jung, Y. S., Kim, Y. S. & Kim, K. R. Association between multimorbidity and periodontal disease in Korean adults: A nationwide cross-sectional cohort study. Int. J. Dent. Hyg. 22, 376–383. https://doi.org/10.1111/idh.12785 (2024).
Brun, A. et al. parodontite : Un risque sous-estimé des maladies cardiovasculaires [Periodontitis : An underestimated risk of cardiovascular diseases]. Med. Sci. M/S. 40, 35–41. https://doi.org/10.1051/medsci/2023193 (2024).
Church, L. et al. Impact of oral hygiene practices in reducing cardiometabolic risk, incidence, and mortality: A systematic review. Int. J. Environ. Res. Public Health 21, 1319. https://doi.org/10.3390/ijerph21101319 (2024).
Qu, H. & Zhang, S. Association of cardiovascular health and periodontitis: A population-based study. BMC Public Health 24, 438. https://doi.org/10.1186/s12889-024-18001-2 (2024).
Frisbee, S. J., Chambers, C. B., Frisbee, J. C., Goodwill, A. G. & Crout, R. J. Association between dental hygiene, cardiovascular disease risk factors and systemic inflammation in rural adults. J. Dent. Hyg. JDH. 84, 177–184 (2010).
Michaeli, D. T., Michaeli, J. C., Albers, S., Boch, T. & Michaeli, T. Established and emerging lipid-lowering drugs for primary and secondary cardiovascular prevention. Am. J. Cardiovasc. Drugs Drugs Devices Other Interv. 23, 477–495. https://doi.org/10.1007/s40256-023-00594-5 (2023).
Mourikis, P. et al. Lipid lowering therapy in cardiovascular disease: From myth to molecular reality. Pharmacol. Ther. 213, 107592. https://doi.org/10.1016/j.pharmthera.2020.107592 (2020).
Acknowledgements
We would like to express our gratitude to the team of National Key R&D Program of China (2018YFC1311400) for providing invaluable data. We also extend our sincere appreciation for the support and contribution of the local medical personnel to this study, as well as the active participation of research subjects.
Funding
This study is supported by: (1) the “Tomorrow Cup” Education and Teaching Reform Research of International Medical College, Chongqing Medical University, with grant number 2023–01. (2) the CQMU Program for Youth Innovation in Future Medicine (W0010).
Author information
Authors and Affiliations
Contributions
G.L designed, conducted, and analyzed the experiments, derived the models, and interpreted the data. R.F.M, R.Y.W, Y.D.L and B.Q.W contributed to the implementation of the study. Z.H.T and T.Q collaborated with G.L in writing the manuscript. B.H and S.X.L provided superior guidance and conducted advanced review for this work. All authors critically reviewed and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University. All the participants were informed of the study content and signed informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tang, Z., Qiu, T., Ma, R. et al. The influence of habitual tooth brushing frequency on individuals diagnosed with coronary artery disease. Sci Rep 15, 18463 (2025). https://doi.org/10.1038/s41598-025-01910-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01910-6
