
Abstract
This study investigated the effects of Computerized Quadrato Motor Training (CQMT) on balance and executive function in both single- and dual-task conditions for stroke patients. Patients (n = 60) were randomized to three groups: conventional training (CT), exercise training (ET), and interactive motor-cognitive training (IT). All participants underwent CT. Besides, the ET group undertook step training, and the IT group underwent CQMT for four weeks. The assessments comprised balance function, executive function, lower limb strength, as well as self-efficacy of balance control. Balance function was assessed via the Pro-Kin system and standardized scales (Berg Balance Scale [BBS], Tinetti Assessment [POMA]). Executive function was assessed by the Trail Making Test (TMT-A / B) and Stroop test. Dual-task cost (DTC) derived from Timed Up-and-Go Test with/without cognitive loading (TUGT / TUGTcog). Balance self-efficacy was assessed by the Activities-specific Balance Confidence (ABC) Scale, with lower limb strength assessed by Five-Times Sit-to-Stand (FTSTS). After the intervention, the ET significantly showed improvement in the elliptical trajectory area, BBS, and gait performance compared to CT(P < 0.05). The IT group demonstrated significantly greater improvements in balance parameters (swing speed, elliptical trajectory area, trajectory lengths; P < 0.05) and functional outcomes (BBS, POMA, FTSTS, Dual-Task performance, TMT, Stroop, ABC; P < 0.01) compared to both CT and ET. The IT group showed significant positive correlations between TMT improvements and enhanced Dual-ask performance. Our findings demonstrate that CQMT, as an integrative motor-cognitive intervention, significantly improves balance and executive function in stroke patients, thereby filling a critical gap in the clinical application of QMT in stroke rehabilitation research. These findings validate the ‘guided plasticity facilitation’ theory, highlighting CQMT as a cost-effective and broadly applicable clinical training.
Trial registration: The clinical trial was registered on 08/10/2023, with the registration number ChiCTR2300076424.
Similar content being viewed by others


Introduction
More than 2 million new stroke cases reported annually in China, and the overall incidence rate is on the rise1 Stroke is characterized by a high incidence rate, disability rate, recurrence rate, and mortality2 Motor and cognitive impairments are common consequences of stroke, with nearly 50% of stroke patients experiencing balance function deficits three months after the stroke, which significantly affects functional independence and quality of life3 In recent years, the concept of cognitive-motor interference, which is closely related to daily activities, has gained increased attention in the field of rehabilitation medicine4 Numerous studies have indicated that stroke patients exhibit a more significant decline in balance and gait performance during dual tasks involving cognitive-motor interference5.
Balance control is increasingly recognized as a multifaceted process involving the integration of both motor and cognitive networks6 Balance control encompasses two dimensions: orientation and stability. Orientation entails the cognitive processing of information from proprioceptive feedback, the vestibular system, and visual input. Stability, on the other hand, refers to the ability to maintain the amplitude of the center of gravity swing and keep it within the support surface despite spontaneous activation or external interference7 Notably, there is a close association between executive function, posture control, and fall risk8 In real-world functional activities, continual attention to environmental cues is necessary to quickly respond and prompt restoration of balance following posture interference. Thus, it is unsurprising that advanced cognitive functions such as attention, execution, and dual-task processing abilities are essential for optimal balance control9 Due to central and limb dysfunction, stroke often manifests abnormal posture control strategies, including increased body swing amplitude, delayed or reduced expected posture adjustment, asymmetrical weight-bearing, and gait instability, particularly in dual-task situations10,11 Currently, many studies evaluating the impact of rehabilitation training on balance function in stroke patients rely on assessment scales12 However, the ability to maintain the center of pressure (COP) is a crucial systemic parameter in balance control, and the existing evaluation scales fail to provide this aspect13 Our study employs functional performance assessments, scales, and COP to explore the balance performance in stroke patients during both single-task and dual-task conditions in clinical rehabilitation. Given the crucial role of executive function and balance control ability in stroke prognosis, the objective is to examine whether our proposed training intervention has the potential to enhance both the balance and executive function, leading to better motor control.
As evidenced by extensive literature,14,15 the importance of cognitive processes and motor skills in balance control makes the motor-cognitive training based on a “guided plasticity facilitation” framework show great potential16 The mechanisms underlying the synergistic effect of motor-cognitive training can be primarily attributed to two aspects. From a neurobiological standpoint, motor training can facilitate neuronal activity and enhance synaptic plasticity, while cognitive training can guide long-term synaptic plasticity and regulate neural circuits17 Moreover, from the perspective of brain structure and function, the shared neural network involved in motor and cognitive processes promotes enhanced functional coherence within the brain network, and the activation of distinct functional networks facilitates the refinement of specific connections between them18 Motor-cognitive training encompasses three forms: sequential, simultaneous, and interactive. Among these, interactive motor-cognitive training exhibits the most pronounced benefits for enhancing motor ability related to stroke recovery19 But current research on interactive motor-cognitive training predominantly relies on virtual reality systems,20 leaving limited clinical training methods available for this innovative approach. Therefore, a comprehensive review encourages researchers to develop novel, efficient, and clinically applicable methods of interactive motor-cognitive training21.
To address this gap, this study proposes a Computerized Quadrato Motor Training (CQMT)—an adaptation of Quadrato Motor Training (QMT), a protocol originally developed by Patrizio Paoletti to integrate posture-related executive tasks with motor tasks22 CQMT digitally enhances QMT by adapting the speed of computer commands to individuals’ reaction times, thereby retaining the objective and progressive feedback inherent to VR while eliminating high costs and spatial constraints23 However, there is a lack of research investigating its potential utility in stroke rehabilitation.
In conclusion, while interactive cognitive-motor training has gained research traction, its clinical implementation often relies on complex equipment like VR, lacking simple and accessible clinical training approaches. In this context, QMT training, a novel approach that integrates cognitive elements into motor skills, holds promise for clinical application. However, it has not been tested in stroke patients. To address this gap, this study proposes CQMT and applies it to stroke patients. By progressively reducing instruction time to challenge patients’ reaction times, CQMT not only maintains the objectivity, personalization, and progressive nature of VR training,23 but also enhances clinical practicality. Considering stroke patients often experience balance and executive function deficits, QMT’s cognitive components are related to posture control,24 which may outperform conventional motor training. Therefore, our study aims to compare the effects of CQMT on (a) balance function (primary outcomes) and (b) executive function (secondary outcomes) in comparison with exercise training and conventional training. This study hypothesized that both groups would improve their balance performance, whereas CQMT would enhance a higher degree of balance performance and executive performance, aligning with the viewpoint regarding the synergistic effects of interactive motor-cognitive training25.
Materials and methods
Study design
This study adopted a single-blind, parallel, randomized controlled trial design, ensuring that evaluators and data collectors remained unaware of the trial grouping throughout the study. Data collection occurred at two distinct time points: pretest and posttest. The study was approved by the Ethics Committee (2023-SR-384). Furthermore, the trial was registered in the Chinese Clinical Trial Registry with the code ChiCTR2300076424. The study follows the CONSORT reporting checklist26.
Participants
This study included stroke admitted to the Rehabilitation Medicine Department of the First Affiliated Hospital of Nanjing Medical University from October 2023 to February 2024. The inclusion criteria were (1) Patients with stable vital signs, experiencing a first-time onset of stroke, and post-stroke duration > 1 month; (2) Individuals aged between 18 and 80 years; (3) Walking capacity (with or without assistance ≥ 10 m); (4) Mini-Mental State Examination score ≥ 24 points, indicating the ability to comprehend and cooperate in completing training tasks; (5) Willingness to participate in the trial after being adequately informed. Exclusion criteria included: (1) Pre-existing balance dysfunction before stroke onset (i.e., musculoskeletal disorders, vestibular problems, head injuries, previous strokes, or cardiovascular conditions that significantly impair balance); (2) Presence of severe comorbidities such as heart, liver, kidney, or brain failure; (3) Diagnosis of cognitive and mental disorders; (4) Inability to complete training tasks due to sensory impairments (e.g., blindness, deafness, severe language disorders); (5) Lack of willingness to engage in the evaluation process.
Randomization, allocation concealment, and blinding
To examine whether CQMT, as an interactive motor-cognitive training, can lead to enhancements in both balance and executive function over exercise training and conventional training. According to the Cochrane Handbook,27 Stroke patients meeting the inclusion criteria were randomly allocated to one of three groups: the placebo control group provided with conventional rehabilitation training (CT), the active control group given the exercise training (ET), the experimental group engaged in interactive motor-cognitive training (IT). Each group comprised 20 cases. Sequentially numbered, opaque, sealed envelopes containing allocation cards were prepared by research assistants uninvolved in recruitment. Following baseline assessments, the trial coordinator opened envelopes in numerical order to reveal group allocation. Outcome assessors were blinded to group assignments throughout the study period.
Interventions
Conventional rehabilitation training (CT)
The CT group received standard rehabilitation training, encompassing comprehensive exercises targeting hemiplegic limbs, balance, center of gravity transfer training, and activities of daily living. The training regimen consisted of two sessions per day, each lasting 40 min, conducted five times per week over 4 weeks.
Exercise training (ET)
The ET group underwent step training in addition to conventional rehabilitation. This intervention involved patients standing within a 50 cm x 50 cm square and engaging in sequential forward, backward, left, right, and diagonal stepping exercises. Following the FITT principle, the exercise frequency was set at five sessions per week, with perceived exercise intensity ranging from 6 to 9 points on Borg’s PRE scale. Each session lasted 15 min and was conducted five times per week over 4 weeks, focusing exclusively on exercise training.
Interactive motor-cognitive training (IT)
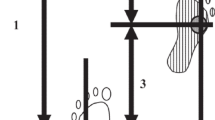
The IT group participated in modified interactive motor-cognitive training, referred to as Computerized Quadrato Motor Training (CQMT), alongside conventional rehabilitation. During this training, participants stood at the starting corner of a 50 cm x 50 cm square and received computer-generated commands based on their reaction time, as shown in Fig. 1. These commands generated using E-Prime 3.0 psychological experimental programming software, directed participants to move towards different corners, incorporating forward, backward, left, right, or diagonal movements. The training protocol comprised 12 action commands (4 corners x 3 directions) and one non-motion command (e.g. “4–4” indicates remaining stationary at corner #4). The IT group also followed the FITT principle with training sessions lasting for 15 min and the same frequency and intensity as other groups (5 days/week; 4 weeks; Borg RPE 6–9). The training type is interactive motor-cognitive training, employing a gradual and personalized approach. Reaction time was quantified using E-Prime 3.0. Command parameters were algorithmically adjusted to ensure a minimum trial accuracy of 80% for participants. If participants achieved ≥ 95% accuracy in the preceding session, command presentation intervals decreased by 100 ms / day to maintain challenge thresholds while avoiding cognitive overload. Therapists closely monitored all groups, implementing safety measures to reduce the risk of falls and ensure participants’ well-being throughout the intervention period.

Computerized Quadrato Motor Training. The upper part of the figure illustrates the training paradigm. Participants performed computer-cued multidirectional movements (forward/backward/lateral/diagonal) within a 50 × 50 cm square, responding to real-time reaction-dependent commands. The lower part of the figure displays the motor commands. The 13-command system (12 directional and 1 static) was generated and validated using E-Prime 3.0.
Outcome measures
The study assessed all outcome measures at week 0 (baseline) and week 4 across three groups. The primary outcome measure was balance performance, including static balance function assessment, the Limit of Stability Test (LOS), and dynamic balance assessment via the Pro-Kin Balance Evaluation Training System (Model PK-254). Balance standardized scales were obtained using the Berg Balance Scale (BBS) and Tinetti Performance-Oriented Mobility Assessment (POMA). Secondary outcome measures was executive function, assessed by the Trail Making Test (TMT-A / B) and Stroop test. Dual-task cost (DTC) derived from Timed Up-and-Go Test with / without cognitive loading (TUGT / TUGTcog). Additionally, Balance self-efficacy was assessed by the Activities-specific Balance Confidence (ABC), with lower limb strength assessed by Five-Times Sit-to-Stand (FTSTS).
Balance function
Pro-kin balance evaluation
The Pro-Kin Balance Evaluation system assesses static balance function using a pressure-sensitive tablet to measure the Center of Pressure (COP) with participants’ eyes open (EO) and closed (EC). The evaluation includes four parameters: elliptical trajectory area (mm2, trajectory lengths (mm), and the average swing speed in the anterior-posterior (AP) and medial-lateral (ML) directions (mm/sec). The elliptical trajectory area reflects the envelope area of the COP trajectory, providing insights into posture stability through the range of center of mass sway. The average sway speed in different directions is calculated by dividing the total displacement of COP in each direction by the total time, with higher speeds indicating larger swaying amplitudes and unstable posture control. Trajectory lengths refer to the path length of the COP trajectory during the testing process, whereby a longer trajectory length indicates a greater amplitude of center of gravity swing28.
The static balance assessment requires participants to stand on a pressure plate, aligning their heels with the A5 axis, positioning their second toes corresponding to the A2 and A8 axes, and ensuring that the highest point of the arch overlaps with the line connecting A3 and A7. During the test, the patient should face straight ahead, keep their upper limbs naturally relaxed, and position them on both sides of the body as much as possible. They should undergo two 30-second trials with their eyes open and closed, respectively. Prior to the formal test, it is recommended to have the patient practice once to ensure full comprehension of the evaluation method and process.
The Limit of Stability Test (LOS) entails calibrating the four pistons of the balance instrument to convert a pressure plate into an inclined moving plate. Participants are instructed to visually track a yellow flashing light projected on a screen while executing center of gravity transfers in eight anatomically defined directions. By systematically evaluating the boundaries of stability across these diverse directions, the assessment enables the identification of the specific orientations posing the greatest risk of instability and falls. Participants should position their feet parallel to their shoulders, maintain an erect posture, and endeavor to displace their center of gravity as far as possible from the initial position to accurately pursue the moving light stimulus. As a precautionary measure, a therapist should position themselves behind the participant to ensure safety throughout the test. The resultant data comprises an 8-quadrant motion trajectory and the normative ranges defined as 75–100%.
BBS
The BBS developed by Kathryn Berg in 1989, is a widely used assessment tool for evaluating balance function in stroke patients. It comprises 14 items covering activities such as sitting, standing, and turning. Each item is scored on a scale of 0–4, with a total score of 56. A score below 45 indicates an increased risk of falling. The Berg scale demonstrates good reliability and validity29.
POMA
The POMA scale is a performance-oriented mobility balance tool consisting of two components: balance and gait. The balance tests encompass static sitting, posture control when rising from a chair, maintaining standing balance with eyes open and closed, and completing a 360-degree turn. Gait testing includes assessment of gait initiation, path, symmetry, continuity, support area, and swing amplitude. Within the stroke population, POMA is an effective tool for dynamic balance assessment, with a minimum detectable change (MDC) of 6 points30.
Executive function
TMT (The trail making test)
The Trail Making Test (TMT) introduced by Partington and Leiter in 1938, comprises two parts: TMT-A and TMT-B. In TMT-A, participants connect randomly arranged numbers from 1 to 25 in numerical order as quickly as possible. In TMT-B, they connect numbers and letters in an alternating order (e.g., 1-A-2-B) as quickly as possible. Prior to each test, participants receive practice to ensure comprehension. During the formal test, completion time is recorded for each section, with a maximum allowable time of 300 s. TMT-A evaluates attention and visual scanning, while TMT-B assesses executive function components such as working memory, inhibition, and task switching. The derived d value (d = TMTA-TMTB) evaluates psychological flexibility and task-switching ability31.
Computerized stroop task
The Computerized Stroop Task measures cognitive processing speed and executive function. Participants respond to color words displayed on a computer screen by identifying whether the color matches the word’s meaning. Stimuli can be congruent (e.g., the word “red” written in red) or incongruent (e.g., the word “red” written in green). The E-Prime software is utilized for task protocol design to record the reaction time (RT) and the correct responses by the participants. The Stroop interference effect, calculated as the difference in reaction times between incongruent and congruent stimuli, reflects conflict monitoring ability and executive function32.
Dual-task performance
The TUGT, developed by Podsiadlo in 1991, evaluates mobility and fall risk in stroke patients. Participants are instructed to sit in a chair with a backrest, then stand up, walk for 3 m, turn around, and return to the chair to sit down. The average time from three trials is calculated. It is widely used to assess mobility and fall risk in stroke patients33.
An adaptation of the TUGT, the Timed Up and Go Test Cognitive (TUGTcog) incorporates a cognitive task alongside the mobility assessment. Participants perform the TUGT while simultaneously engaging in mental arithmetic by subtracting 7 from a randomly selected number. Perform both tasks simultaneously with equal attention to walking and cognitive performance. The average completion time from three trials is recorded. The dual-task cost (DTC) is computed using the formula DTC = (TUGTcog - TUGT) / TUGT × 100%, providing insight into the impact of cognitive load on mobility performance34.
Lower limb strength
The Five Times Sit-to-Stand (FTSTS) test assesses lower limb strength and functional capacity. Participants sit in armless chairs set at a standardized height (43–45 cm) with knees bent at a 90-degree angle and arms crossed over their torso. Upon verbal instructions from the evaluator, participants stand up and sit down as quickly as possible for five consecutive repetitions. Three trials are conducted, and the average time is calculated. The FTSTS provides a simple effective method for quantifying lower limb strength35.
Balance confidence
The Activities Specific Balance Confidence Scale (ABC) developed by Powell and Myers in 1995, comprises 16 items assessing individuals’ confidence in performing various daily activities. Participants rate their confidence level on a scale ranging from 0 (indicating no confidence) to 100 (indicating complete confidence). Each item not applicable or difficult to imagine is omitted from scoring, with a minimum of 12 items required for a valid score. The final score is obtained by summing the ratings and dividing by the number of items. The ABC scale primarily evaluates individuals’ self-efficacy in maintaining balance during daily activities36.
Sample size
The sample size was determined based on the effect size observed in a previous study by Cho et al.37 investigating the impact of motor-cognitive training on balance improvement in stroke patients. Using a mean difference of 0.81 and a standard deviation of 0.3, with an alpha of 0.05 and 80% statistical power, PASS software estimated a minimum of 14 participants per group. Accounting for a 20% dropout rate, the final sample size was adjusted to 54 participants.
Statics analysis
Statistical analyses were performed using SPSS 26.0 software. Categorical variables were analyzed with frequency distributions and chi-square tests. All continuous variables were presented as mean (M) ± standard deviation (SD) and the normality was screened by the Kolmogorov-Smirnov test. Normally distributed variables were analyzed using one-way analysis of variance (ANOVA) for intergroup comparisons. Non-parametric data were compared using the Kruskal-Wallis test. Post-hoc comparisons, including the LSD test method for homogeneous variance and Tamhane’s T2 method for heterogeneous variance, were applied when significant differences were detected between groups. Intragroup comparisons before and after treatment were conducted using paired t-tests or Wilcoxon signed-rank test. Statistical significance was set at P < 0.05. A generalized estimating equation (GEE) was used to evaluate the differences in the changes between the groups across the pre-test and post-test periods (i.e. group*time interaction effect). Effect sizes (partial eta squared, η2 were calculated according to Cohen’s criteria,38 with values ≥ 0.2, ≥ 0.5, and ≥ 0.8 indicating small, moderate, and large effects, respectively. Furthermore, we conducted Spearman correlation analysis (pre-post change) to explore the differences in the relationship between cognitive and balance indicators.
Results
A total of 60 stroke patients participated in this study, with detailed recruitment procedures outlined in Fig. 2. Table 1 summarizes the demographic and clinical characteristics of the three patient groups, indicating no significant difference (see Supplementary Tab S1).

Flow chart.
Balance
Pro-kin
An interaction between groups and time was observed on the Pro-kin test. In the intra-group comparison, the IT group showed significant improvements in all parameters (P < 0.001) during the eye-open and eye-closed conditions, while the ET group and CT group only exhibited limited improvements in the elliptical trajectory area (P < 0.05). The inter-group comparison revealed that the IT group demonstrated significantly better improvement in average swing speed in ML directions (P < 0.001), swing speed in AP directions (P < 0.05) and trajectory lengths (P < 0.05) in both eye-open and eye-closed conditions compared to the other groups. However, in terms of the elliptical trajectory area, the IT group showed slightly better improvement compared to the CT group in both conditions (P < 0.001), with significant enhancement only observed in the eyes-closed conditions compared to the ET group (P = 0.005). The Limit of Stability (LOS) test showed significant improvements in stability limits for all groups compared to the pre-test condition (P < 0.001). The IT also showed enhanced LOS test compared to CT (P = 0.048).
BBS
The results from the BBS revealed an interaction effect between groups and time (Wald χ2 = 83.373, P < 0.001). Specifically, the CT group increased from 41.25 ± 3.49 to 43.55 ± 4.22, the ET group demonstrated progress from 41.85 ± 2.68 to 45.75 ± 2.95, and the IT group exhibited an improvement from 41.30 ± 3.34 to 49.95 ± 3.6. IT exhibited significantly superior BBS improvements compared to both ET and CT (P < 0.001), while post-hoc comparisons indicated marginal significance between ET and CT (P = 0.05).
POMA
In the POMA test, IT and MT exhibited substantial enhancements in balance and gait performance (P < 0.001), while CT showed no difference in gait performance (P = 0.336). This study found a trend toward an interaction between groups and time on the POMA test. The post-hoc comparisons showed that the IT group demonstrated a remarkable trend in balance scores (from 10.30 ± 1.81 to 13.80 ± 1.77), gait scores (from 4.90 ± 1.33 to 9.70 ± 2.85), and total scores (from 15.25 ± 2.95 to 23.50 ± 3.78), surpassing both the CT and ET groups (P < 0.001). Whereas the ET group only showed significantly better improvement in gait performance compared to the CT group (P = 0.012).
Executive performance
TMT
The time*group interaction effect was significant (P < 0.01) in the TMT test. The results of the TMT indicated notable enhancements in both the IT group and the ET group across various parameters (TMT-A, TMT-B, TMT B-A) compared to pre-treatment (P < 0.001), while the CT group showed no difference. Importantly, the post-hoc comparisons indicated that the IT group demonstrated a significantly superior improvement in TMT-A, TMT-B, and TMT B-A compared to the CT group and the ET group (P < 0.01), supporting a significant main effect of the group.
The stroop test
The Stroop test revealed a significant group*time interaction on the reaction time of incongruent condition and congruent condition (P < 0.001). Among three groups, only the IT group demonstrated significant improvement in response time under both congruent and incongruent conditions after training (P < 0.01), with ET group having nearly significance on the reaction time of incongruent conditions (P = 0.058). Additionally, both the IT group and ET group showed significant improvement in Stroop score compared to pre-treatment (P < 0.001), and the post-hoc comparisons confirmed IT’s superiority over ET in conflict resolution efficiency (P = 0.46).
Dual-task performance
Significant group*time interactions were observed for TUGT (Wald χ²=226.100, P < 0.001), TUGTcog (Wald χ²=451.481, P < 0.001), and DTC (Wald χ²=64.352, P < 0.001). All groups demonstrated significant post-intervention improvements in TUGT and TUGTcog (P < 0.05). However, only the IT group showed enhanced DTC, whereas other groups exhibited deterioration. Specifically, IT demonstrated superior efficacy compared to CT and ET across all measures (P < 0.01). But ET showed no significant improvement in TUGT, TUGTcog, and DTC performance compared to CT (P > 0.05).
Lower limb strength
Significant group*time interactions were observed for FTSTS (Wald χ²=19.240, P < 0.001). The findings from the FTSTS indicated a reduction in testing time for all three groups post-intervention, suggesting an improvement in lower limb strength. Specifically, the IT group demonstrated a decrease from 18.58 ± 1.95 to 14.34 ± 2.41 s, which was significantly superior to both the CT group and the ET group (P < 0.05).
Balance confidence
Significant group*time interactions were observed for FTSTS (Wald χ²=35.896, P < 0.001). After the intervention, both the IT and ET groups showed a significant increase in balance confidence (P < 0.001). Inter-group comparisons revealed that only the IT group exhibited a more significant increase than the ET group (P = 0.010) and the CT group (P = 0.001). These findings suggest that CQMT can enhance balance confidence more effectively than the other training.
Correlation analysis
In the IT group, improvements in TMT (TMT-A, TMT-B, and TMT B-TMTA) were significantly correlated with dual-task performance gains (TUGTcog and DTC) (P < 0.05). No significant correlations were observed in the ET group and CT group (P > 0.05) (see Table 2).
Table 3 summarizes the outcomes of post-intervention effects, group*time interactions, and ANOVA results. Additionally, within-group intervention effects are detailed in Supplementary Tab S2, with post-hoc analyses presented in Supplementary Tab S3. All outcomes are visualized in Fig. 3.

Trends in the changes in parameters between the groups.
Discussion
In recent years, motor-cognitive training for stroke patients has garnered considerable attention among researchers, emerging as a novel research focus19 In light of this, integrating this training into clinical practice is a more critical consideration21 In response to the limitations of existing interactive motor-cognitive training, which often relies on complex equipment such as VR and the underutilization of QMT in stroke rehabilitation, this study has computerized the QMT training to meet the needs of clinical practice. This study assesses the impact of CQMT training on balance and executive functions in stroke patients, aiming to provide a simple and feasible clinical training solution.
Effectiveness of CQMT on balance performance
The differential therapeutic outcomes between the interventions revealed critical neurorehabilitation mechanisms underlying post-stroke recovery. Compared to ET, IT demonstrated a greater reduction in swing speed and trajectory length during the eyes-open condition. This phenomenon can be attributed to CQMT’s adaptive instruction time reduction protocol, which accelerates sensorimotor processing speed. This is supported by prior evidence that faster reaction times and more rapid motor responses correlate with improved motor control in stroke survivors39 Notably, the superiority of IT over CT or ET in eyes-closed static balance parameters likely originates from QMT’s framework, which restores stroke-impaired proprioceptive function. Given that stroke survivors frequently rely on visual compensation for balance due to proprioceptive deficits, notably demonstrated in eyes-closed balance assessments40 CQMT directly targets these sensorimotor integration deficits by challenging movement direction perception and eliciting rapid postural adjustments. Furthermore, findings suggest that eyes-closed balance performance engages striatal dopaminergic pathways,41 offering novel mechanistic insights into QMT’s therapeutic effects.
Clinically, these balance improvements translate to functional gains, as evidenced by CQMT’s significantly greater enhancements in BBS, POMA, and FTSTS versus ET. CQMT’s optimized balance and gait performance may be mediated through three training-induced adaptations: (1) refined step strategy via real-time motor command synchronization, (2) enhanced trunk control through motor response optimization, and (3) improved weight-bearing symmetry via muscle coactivation regulation42,43,44,45.
Effectiveness of the CQMT on executive performance
The motor-cognitive training’s synergistic effects reveal fundamental differences in neuroplasticity induction between IT and ET. As CQMT embedded executive elements within motor training, IT demonstrated significantly greater improvements compared to ET in TMT and Stroop test, which are sensitive measures of executive function46,47 Given that executive functions are critical for dual-task performance,48 while both groups showed comparable improvements in TUGT completion time, only IT demonstrated superior dual-task cost reduction. This differential outcome can explained by the significant positive correlation observed between TMT performance (reflecting information processing speed and cognitive flexibility49 and DTC reduction exclusively in the IT group. The observed correlation suggests that CQMT’s integration of motor-cognitive elements enhances frontoparietal neural circuit connectivity and boosts synaptic transmission efficiency, thereby specifically improving dual-task performance through optimized resource allocation50 This interpretation is further supported by prior neuroimaging evidence indicating that QMT reinforces the structural integrity of the corpus callosum, a critical bridge in the brain’s hemispheric networks, which facilitates synchronized cognitive-motor processing during dual-task51 In contrast, ET’s exclusive focus on motor automaticity resulted in reduced TUGT completion times but paradoxically increased DTC. This phenomenon aligns with the principle that purely motor training enhances stereotyped movement patterns without developing the cognitive reserve necessary for task-switching efficiency52,53.
Potential mechanisms of QMT
QMT integrates motor skills of physical coordination and motor responses with cognitive skills like working memory and attention, creating synergistic effects9 Specifically: First, EEG studies demonstrate that QMT’s integration of motor and cognitive skills enhances brain connectivity and synergistically promotes neural plasticity,54 with motor training exerting a “promoting effect” and cognitive training providing a “guiding effect”17 Secondly, QMT induces a synergistic increase in gray matter within the cerebellum (motor coordination) and dorsolateral prefrontal cortex (executive function), providing evidence of its synergistic effects55 As indirect structural connectivity between the cerebellum and frontal-parietal cortices is essential for post-stroke recovery,56 QMT’s coordinated gray matter expansion in these regions provides a neuroanatomical basis for motor-cognitive rehabilitation. Third, QMT activates molecules such as BDNF, enhancing brain plasticity in cognitive and motor domains57 Given the well-documented BDNF deficiency in stroke patients,58 QMT promotes neuronal repair by upregulating BDNF expression.
Promising applications of CQMT
This study proposed CQMT as a novel integrative motor-cognitive training approach for post-stroke rehabilitation, addressing three critical gaps in existing research. First, while prior studies validated QMT’s efficacy in dyslexic rehabilitation and neuroplasticity enhancement in healthy populations,55,59,60 this study is the first to demonstrate comparable efficacy in post-stroke populations, expanding QMT’s therapeutic scope. Second, our study reveals CQMT’s distinct cost-space advantages over VR-based integrative motor-cognitive training approaches, establishing its viability as a broadly applicable intervention particularly suited for resource-constrained settings with limited infrastructure21,61,62 Third, this study validates the Guided Plasticity Facilitation Theory,17 which posits that synergistic integration of motor and cognitive domains generates neuroplastic adaptations critical for functional recovery. Collectively, these findings suggest CQMT’s potential as a low-cost, broadly applicable intervention, making it an attractive choice for clinical and non-clinical settings.
Limitations
This study has several limitations. First, the final cohort predominantly comprised male patients due to the clinical characteristics of our inpatient population at the study center. This demographic constraint limits the generalizability of the findings to female populations. Second, the inclusion criteria required MMSE scores ≥ 24, potentially excluding patients with cognitive impairment. Future studies should enroll stroke patients across the cognitive spectrums to comprehensively evaluate intervention effectiveness on motor and cognitive functions, while also comparing QMT’s efficacy against standard cognitive rehabilitation. Third, although behavioral outcomes demonstrated clinically significant improvements, direct neuroimaging evidence confirming the intervention’s neuroplastic effects remains lacking. Subsequent research should incorporate multimodal neuroimaging to elucidate mechanistic pathways.
Conclusion
Our findings demonstrated the superior efficacy of Computerized Quadrato Motor Training (CQMT) over exercise training (ET) in enhancing balance, executive function, and dual-task performance among stroke survivors, thereby filling a critical gap in the clinical application of QMT in stroke rehabilitation research. This study highlights the clinical efficacy of CQMT in stroke rehabilitation, demonstrating that its therapeutic benefits establish CQMT as a cost-effective and broadly applicable intervention across clinical and community rehabilitation settings, particularly given its hardware independence from virtual reality systems. This study advances neurorehabilitation practice by validating a novel motor-cognitive integration paradigm through CQMT implementation in stroke rehabilitation.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
S, W. et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 18, (2019).
Liu, L. et al. Analysis of burden changes of ischemic stroke in China from 1990 to 2019. Chin. J. Evid. Based Med. 22 (09), 993–998 (2022).
Ullberg, T., Zia, E., Petersson, J. & Norrving, B. Changes in functional outcome over the first year after stroke: an observational study from the Swedish stroke register. Stroke 46, 389–394 (2015).
Pang, M. Y. C. et al. Dual-Task exercise reduces Cognitive-Motor interference in walking and falls after stroke. Stroke 49, 2990–2998 (2018).
Wang, X. Q. et al. Cognitive motor interference for gait and balance in stroke: a systematic review and meta-analysis. Eur. J. Neurol. 22, 555–e37 (2015).
At, S., Kd, H. & S, J. Effect of cognitive task complexity on dual task postural stability: a systematic review and meta-analysis. Exp. Brain Res. 240, (2022).
Horak, F. B. Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age Ageing. 35 (Suppl 2), ii7–ii11 (2006).
Yogev-Seligmann, G., Hausdorff, J. M. & Giladi, N. The role of executive function and attention in gait. Mov. Disord. 23 329–342; quiz 472 (2008).
Montero-Odasso, M. & Speechley, M. Falls in cognitively impaired older adults: implications for risk assessment and prevention. J. Am. Geriatr. Soc. 66, 367–375 (2018).
Rice, J. et al. Greater Cognitive-Motor interference in individuals Post-Stroke during more complex motor tasks. J. Neurol. Phys. Ther. 46, 26–33 (2022).
Tasseel-Ponche, S., Yelnik, A. P. & Bonan, I. V. Motor strategies of postural control after hemispheric stroke. Neurophysiol. Clin. 45, 327–333 (2015).
Chen, S. C., Lin, C. H., Su, S. W., Chang, Y. T. & Lai, C. H. Feasibility and effect of interactive telerehabilitation on balance in individuals with chronic stroke: a pilot study. J. Neuroeng. Rehabil. 18, 71 (2021).
Muir, J. W., Kiel, D. P., Hannan, M., Magaziner, J. & Rubin, C. T. Dynamic parameters of balance which correlate to elderly persons with a history of falls. PLoS One. 8, e70566 (2013).
Scarmagnan, G. S. et al. Benefits of a Dual-Task training on motor and cognitive functions in Community-Dwelling older adults: A controlled clinical trial. Am. J. Phys. Med. Rehabil. https://doi.org/10.1097/PHM.0000000000002352 (2023).
Yu, H. X. et al. Effect of cognitive function on balance and posture control after stroke. Neural Plast. 2021 6636999 (2021).
Bamidis, P. D. et al. A review of physical and cognitive interventions in aging. Neurosci. Biobehav Rev. 44, 206–220 (2014).
Herold, F., Hamacher, D., Schega, L. & Müller, N. G. Thinking while moving or moving while Thinking - Concepts of Motor-Cognitive training for cognitive performance enhancement. Front. Aging Neurosci. 10, 228 (2018).
Lu, Y. et al. Recent advances on the molecular mechanisms of exercise-induced improvements of cognitive dysfunction. Transl Neurodegener. 12, 9 (2023).
Huber, S. K., Knols, R. H., Arnet, P. & de Bruin, E. D. Motor-cognitive intervention concepts can improve gait in chronic stroke, but their effect on cognitive functions is unclear: A systematic review with meta-analyses. Neurosci. Biobehav Rev. 132, 818–837 (2022).
Fishbein, P., Hutzler, Y., Ratmansky, M., Treger, I. & Dunsky, A. A. Preliminary study of Dual-Task training using virtual reality: influence on walking and balance in chronic poststroke survivors. J. Stroke Cerebrovasc. Dis. 28, 104343 (2019).
G, P. & Ed, B. P, W., K, M. Cognitive and cognitive-motor interventions affecting physical functioning: a systematic review. BMC Geriatr. 11, (2011).
Ben-Soussan, T. D., Glicksohn, J. & Berkovich-Ohana, A. From cerebellar activation and connectivity to cognition: A review of the Quadrato motor training. Biomed. Res. Int. 2015 954901 (2015).
Fissler, P., Küster, O., Schlee, W. & Kolassa, I. T. Novelty interventions to enhance broad cognitive abilities and prevent dementia: synergistic approaches for the facilitation of positive plastic change. Prog Brain Res. 207, 403–434 (2013).
Leshem, R., De Fano, A. & Ben-Soussan, T. D. The implications of motor and cognitive Inhibition for hot and cool executive functions: the case of quadrato motor training. Front. Psychol. 11, 940 (2020).
Kraft, E. Cognitive function, physical activity, and aging: possible biological links and implications for multimodal interventions. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 19, 248–263 (2012).
Schulz, K. F., Altman, D. G. & Moher, D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J. Pharmacol. Pharmacother. 1, 100–107 (2010).
Cumpston, M. et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst. Rev. 10, ED000142 (2019).
Zhai, X. et al. Effects of Robot-Aided rehabilitation on the ankle joint properties and balance function in stroke survivors: A randomized controlled trial. Front. Neurol. 12, 719305 (2021).
Downs, S., Marquez, J. & Chiarelli, P. The Berg balance scale has high intra- and inter-rater reliability but absolute reliability varies across the scale: a systematic review. J. Physiother. 59, 93–99 (2013).
Canbek, J., Fulk, G., Nof, L. & Echternach, J. Test-retest reliability and construct validity of the Tinetti performance-oriented mobility assessment in people with stroke. J. Neurol. Phys. Ther. 37, 14–19 (2013).
Llinàs-Reglà, J. et al. Trail Mak. Test. Assess. 24, 183–196 (2017).
Periáñez, J. A., Lubrini, G., García-Gutiérrez, A. & Ríos-Lago, M. Construct validity of the Stroop Color-Word test: influence of speed of visual search, verbal fluency, working memory, cognitive flexibility, and conflict monitoring. Arch. Clin. Neuropsychol. 36, 99–111 (2021).
Zak, M. et al. Functional capacity and dual-task cost in the institutionalized older adults, both affected and unaffected by mild cognitive impairment. Eur. Rev. Aging Phys. Act. 18, 16 (2021).
Bock, O. Dual-task costs while walking increase in old age for some, but not for other tasks: an experimental study of healthy young and elderly persons. J. Neuroeng. Rehabil. 5, 27 (2008).
de Abreu, D. C. C., Porto, J. M., Tofani, P. S., Braghin, R. & de M, B. Freire junior, R. C. Prediction of reduced gait speed using 5-Time Sit-to-Stand test in healthy older adults. J. Am. Med. Dir. Assoc. 23, 889–892 (2022).
Zhang, D. et al. The Chinese short version of the Activities-Specific balance confidence scale: its validity, reliability, and predictive value for future falls in Community-Dwelling older adults. Clin. Interv Aging. 17, 1483–1491 (2022).
Cho, K. H., Lee, K. J. & Song, C. H. Virtual-reality balance training with a video-game system improves dynamic balance in chronic stroke patients. Tohoku J. Exp. Med. 228, 69–74 (2012).
Cohen, J. The analysis of variance. In (ed Cohen, J.) Statistical Power Analysis for the Behavioral Sciences (2nd ed., 273–406). Hillsdale, NJ: Lawrence Erlbaum. (1988).
Mansfield, A., Inness, E. L., Wong, J. S., Fraser, J. E. & McIlroy, W. E. Is impaired control of reactive stepping related to falls during inpatient stroke rehabilitation? Neurorehabil Neural Repair. 27, 526–533 (2013).
Treger, I., Mizrachi, N. & Melzer, I. Open-loop and closed-loop control of posture: Stabilogram-diffusion analysis of center-of-pressure trajectories among people with stroke. J. Clin. Neurosci. 78, 313–316 (2020).
Cham, R., Perera, S., Studenski, S. A. & Bohnen, N. I. Striatal dopamine denervation and sensory integration for balance in middle-aged and older adults. Gait Posture. 26, 516–525 (2007).
Ng, S. S. & Hui-Chan, C. W. The timed up & go test: its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Arch. Phys. Med. Rehabil. 86, 1641–1647 (2005).
Ortega-Bastidas, P., Gómez, B., Aqueveque, P. & Luarte-Martínez, S. Cano-de-la-Cuerda, R. Instrumented timed up and go test (iTUG)-More than assessing time to predict falls: A systematic review. Sens. (Basel). 23, 3426 (2023).
Ferreira, V. et al. Interactive video gaming improves functional balance in poststroke individuals: Meta-Analysis of randomized controlled trials. Eval Health Prof. 43, 23–32 (2020).
Xiao, T. et al. Correlation between cognition and balance among Middle-Aged and older adults observed through a Tai Chi intervention program. Front. Psychol. 11, 668 (2020).
Graf, P., Uttl, B. & Tuokko, H. Color- and picture-word Stroop tests: performance changes in old age. J. Clin. Exp. Neuropsychol. 17, 390–415 (1995).
Sánchez-Cubillo, I. et al. Construct validity of the trail making test: role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J. Int. Neuropsychol. Soc. 15, 438–450 (2009).
Killane, I. et al. Relative association of processing speed, short-term memory and sustained attention with task on gait speed: a study of community-dwelling people 50 years and older. J. Gerontol. Biol. Sci. Med. Sci. 69, 1407–1414 (2014).
Raichlen, D. A. et al. Effects of simultaneous cognitive and aerobic exercise training on dual-task walking performance in healthy older adults: results from a pilot randomized controlled trial. BMC Geriatr. 20, 83 (2020).
A, S. & Ed, B. R, A., F, G. Adaptations of prefrontal brain activity, executive functions, and gait in healthy elderly following exergame and balance training: A randomized-controlled study. Front. Aging Neurosci. 8, (2016).
Pellegrino, M., Ben-Soussan, T. D. & Paoletti, P. A. Scoping review on movement, neurobiology and functional deficits in dyslexia: suggestions for a Three-Fold integrated perspective. Int. J. Environ. Res. Public. Health. 20, 3315 (2023).
Zhu, C. & Han, J. The higher, more complicated: the neural mechanism of hierarchical task switching on prefrontal cortex. Brain Sci. 12, 645 (2022).
Wolff, S. B. E., Ko, R. & Ölveczky, B. P. Distinct roles for motor cortical and thalamic inputs to striatum during motor skill learning and execution. Sci. Adv. 8, eabk0231 (2022).
Lasaponara, S. et al. Increased alpha band functional connectivity following the quadrato motor training: A longitudinal study. Front. Hum. Neurosci. 11, 282 (2017).
Ben-Soussan, T. D., Berkovich-Ohana, A., Piervincenzi, C., Glicksohn, J. & Carducci, F. Embodied cognitive flexibility and neuroplasticity following quadrato motor training. Front. Psychol. 6, 1021 (2015).
Sotelo, M. R., Kalinosky, B. T., Goodfriend, K., Hyngstrom, A. S. & Schmit, B. D. Indirect structural connectivity identifies changes in brain networks after stroke. Brain Connect. 10, 399–410 (2020).
Paoletti, P., Pellegrino, M. & Ben-Soussan, T. D. A Three-Fold integrated perspective on healthy development: an opinion paper. Brain Sci. 13, 857 (2023).
Øverberg, L. T. et al. Plasma levels of BDNF and EGF are reduced in acute stroke patients. Heliyon 8, e09661 (2022).
Ben-Soussan, T. D. et al. Changes in cerebellar activity and inter-hemispheric coherence accompany improved reading performance following quadrato motor training. Front. Syst. Neurosci. 8, 81 (2014).
Ben-Soussan, T. D. & Glicksohn, J. Gender-Dependent changes in time production following quadrato motor training in dyslexic and normal readers. Front. Comput. Neurosc. 12, 71 (2018).
Lloréns, R., Noé, E., Colomer, C. & Alcañiz, M. Effectiveness, usability, and cost-benefit of a virtual reality-based telerehabilitation program for balance recovery after stroke: a randomized controlled trial. Arch. Phys. Med. Rehabil. 96, 418–425e2 (2015).
Laver, K. E. et al. Virtual reality for stroke rehabilitation. Cochrane Db. Syst. Rev. 2018 CD008349 (2017).
Funding
This trial received support from the Jiangsu Province Key Research and Development Program (Grant number BE2021012-4), Zhejiang Provincial Medical and Health Science and Technology Program(Grant number 2025KY367), Zhejiang Provincial Traditional Chinese Medicine Health Science and Technology Program(2025ZL567). The funding bodies had no role in the study design, data colection, analysis and interpretation of data.
Author information
Authors and Affiliations
Contributions
Study concept and design: Cunshu Wu, Yun Yang and Guangxu Xu; Acquisition of data: Cunshu Wu, Rong Cao and Kailin Qian; Analysis and interpretation of data: Wenjie Jin and Jun Lu; Drafting of the manuscript: Cunshu and Yun Yang; Critical revision of the manuscript for important intellectual content: Yun Yang and Guangxu Xu.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethnic approval
This study was approved by the Ethics committees of the first affiliated hospital of Nanjing Medical University, Nanjing, Jiangsu Province (No.2023-SR-384). The study was conducted according to the principles of the Declaration of Helsinki. Informed consent was obtained from all participants. Participants were informed about the purpose of the research and could withdraw from the study at any time.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, C., YunYang, Jin, W. et al. The application of computerized quadrato motor training in enhancing balance and executive performance in stroke patients. Sci Rep 15, 18850 (2025). https://doi.org/10.1038/s41598-025-02145-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-02145-1
