
Abstract
The growth and development of the maxillofacial complex share a common embryological origin with the cranial base and upper cervical spine; therefore, anomalies in these regions may be linked to variations in the skeletal pattern. This study aimed to evaluate the relationships between the morphological features of the sella turcica bridging, ponticulus posticus, posterior arch deficiency of the first cervical vertebra, known as the atlas, and the cervical vertebral maturation stages and vertical malocclusions. Randomly selected 300 pre-orthodontic treatment patients (aged 7 to 40 years) were divided into groups according to cervical stage (CS1–CS6) and type of vertical malocclusion. According to the study protocol, cephalometric analysis and evaluation of the sella turcica and atlas were performed twice by two researchers under the supervision of a radiologist. Statistical analysis was performed using SPSS 29.0. Sella turcica bridging was significantly more common in postpubertal patients (58.2%; p < 0.05). Ponticulus posticus and sella turcica bridging occurred more frequently in patients with low mandibular plane angle (43.3% and 51.1%, respectively), whereas atlas posterior arch deficiency occurred more frequently in patients with high mandibular plane angle (24.2%). However, only atlas posterior arch deficiency showed significant difference (p < 0.05). According to logistic regression, patients in the CS6 stage were less likely to have type 1 ponticulus posticus and more likely to have type 2 sella turcica bridging (p < 0.05). Patients with low angle were less likely to have atlas posterior arch deficiency (p < 0.05). Sella turcica bridging and atlas posterior arch deficiency are associated with the skeletal pattern and cervical stage. Sella turcica bridging was more prevalent during the postpubertal period, whereas atlas posterior arch deficiency was more prevalent in those with a high mandibular plane angle.
Similar content being viewed by others

Introduction
Orthodontic anomalies, caused by genetic and environmental factors as well as individual habits, affect both physical and mental health1,2. The discussion on the mechanisms of occlusion alterations has been continuing, emphasizing that while the effects of etiological factors remain incompletely understood, increasing attention has been given to the role of environmental factors in the development of malocclusion1. Malocclusion is one of the most common oral health issues affecting individuals worldwide; it impacts speech and aesthetics and significantly contributes to a reduced quality of life2,3,4.
Previous studies have revealed associations between abnormalities in the upper cervical spine and jaw malformations, craniofacial morphology, and malocclusion5,6,7. These relationships may begin in early embryogenesis, where the notochord plays a critical role in the development of both the cervical vertebrae and the cranial base, particularly the basilar part of the occipital bone, which forms the posterior cranial base angle6. The cranial base, linked to the cervical spine through the notochord, probably functions as a developmental connection between the cervical vertebrae and the jaws5,6,7.
Important cervical spine pathologies or normal variants that can be identified on lateral cephalometric radiographs (LCRs) include anomalies in the atlanto-occipital region, such as ponticulus posticus (PP) and atlas posterior arch deficiency (APAD)8. Ponticulus posticus, meaning a “little posterior bridge” in Latin, is also known by various other names in the literature, such as Kimmerle’s anomaly, pons ponticus, canalis arteriae vertebralis, posterior atlantoid foramen, foramen sagittal, atlas bridging, arcuate foramen, posterior ponticulus, foramen retroarticular, and retroarticular ring9,10,11,12. This anomaly is characterized by a complete or incomplete osseous ridge that extends from the posterior aspect of the superior articular process to the posterolateral portion of the superior margin of the posterior arch of the atlas vertebra, traversing the vertebral artery groove10,11. It is caused by calcification of the oblique atlantooccipital ligaments, sometimes referred to as arcuate ligaments9. The formed osseous bridge between the atlas and axis vertebrae can affect neurovascular structures10. It can compress or irritate the suboccipital nerve, sympathetic periarterial plexus, and vertebral artery, potentially leading to health problems12. These symptoms include headaches, neck pain, vertigo, swallowing and speech difficulties, visual disturbances, neurosensory hearing loss, vertebrobasilar insufficiency, dizziness, loss of postural muscle tone, shoulder pain, Barré–Liéou syndrome, vascular issues, and loss of consciousness9,10,11,12,13.
Atlas posterior arch deficiency is a rare anomaly that affects the posterior arch of the atlas14. Even though this deficiency is often asymptomatic and typically discovered incidentally through radiological imaging, it can present in various ways, including neck and head pain, neurological deficiencies, and Lhermitte’s sign14,15. In some cases, cervical myelopathy may also develop14.
Another cranial base anomaly associated with skeletal malocclusions is sella turcica bridging (STB). It is a concave structure located above the body of the sphenoid bone and is surrounded by the anterior and posterior vertical walls of the bone16. The etiology of this bridge is associated with calcification of the interclinoid ligament or fusion of the anterior and posterior clinoid processes, resulting from their abnormal development9,17. It is an important structure that provides valuable diagnostic information for analysing craniofacial anomalies and offers insights into the pathology of the pituitary gland18. The sella turcica is closely linked to craniofacial growth and development, as its shape is associated with the pituitary gland and neural crest cells, and any abnormality in the pituitary gland can disrupt growth hormone secretion, hindering bone and body development19. Several studies have established a relationship between various conditions and syndromes affecting the craniofacial complex and changes in the size and shape of the sella turcica. These include Williams syndrome, Down syndrome, osteogenesis imperfecta, Axenfeld–Rieger syndrome, cleft lip and palate, trisomy, fragile X syndrome, Cri du Chat syndrome, and lumbosacral myelomeningocele20,21. Other studies have shown a greater prevalence of sella turcica bridging in patients with dental anomalies, including agenesis of the mandibular second premolars and maxillary lateral incisors, dental transposition, and maxillary canine impaction21.
These cervical spine and cranial base pathologies are clinically important for anatomists, radiologists, neurophysicians and neurosurgeons specializing in this region9. These structures can be identified during routine orthodontic radiographic evaluation, as LCRs are commonly used for cephalometry and assessment of cervical maturation stage (CVM)23. The importance of cephalograms in assessing the morphology of the skull, facial structures, and upper cervical spine is unquestionable8,22,24. Because LCRs are inexpensive, simple, and provide sufficient diagnostic information, they can serve as an alternative to three-dimensional imaging in the evaluation of cervical spine and cranial base pathologies.
The current literature suggests that vertebral anomalies may disrupt normal craniofacial growth, potentially contributing to abnormal occlusal relationships and influencing overall craniofacial development22,25,26. These ossification changes may remain asymptomatic during preadolescence and are likely to present symptoms later in life23. Understanding these structures and identifying them in LCRs could help prevent degenerative disorders and serious complications in the future11,23,25. Considering the dynamic and variable nature of individual growth and development, it is important for clinicians to examine the relationship between malocclusions and ossification changes in the cranial base and upper cervical spine at various stages of growth. The aim of this study was to evaluate the relationship between vertical malocclusions, cervical maturation stages, and the morphological features of sella turcica bridging, ponticulus posticus, and atlas posterior arch deficiency.
Methods
The study received ethical approval from the Kaunas Regional Biomedical Research Ethics Committee (No. BE-2-71, 12 June 2024). All methods were performed in accordance with the relevant guidelines and regulations. This study protocol was followed as described in our previous study27.
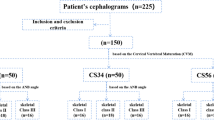
Based on the sample size calculation using the Krejcie and Morgan sample size determination table, the required sample size was determined to be 300. To ensure the reliability of this estimate, the sample size was further calculated using GPower (Version 3.1.9.6) statistical software (GPower©, Heinrich Heine University Düsseldorf, Germany). A power analysis was conducted with the Chi-Square family of tests to detect a small to medium effect size (Cohen’s w = 0.3), with an alpha level of 0.05 and a power of 0.95, which resulted in a required sample size of N = 295.
After a detailed review of the digital archives from the Department of Orthodontics at the Lithuanian University of Health Sciences, the study consisted of 300 randomly selected patients (153 females and 147 males). The age range was 7–40 years (mean 15.10 years, SD 4.84 years).
The inclusion criteria were as follows: healthy patients with no history of orthodontic treatment or surgery and patients with digital dental models and high-quality pretreatment LCRs clearly showing the first four cervical vertebrae and the sella turcica. The exclusion criteria were as follows: patients with syndromic conditions or other developmental abnormalities; patients without digital dental models; or patients with missing or low-quality pretreatment LCRs that did not clearly show the first four cervical vertebrae and the sella turcica.
Before the study, the observers were instructed, and a pilot study of 20 LCRs was performed by two observers under the supervision of an expert radiologist. LCRs were then analysed according to a standardized protocol by a senior dental student and an expert orthodontist under the supervision of a radiologist. The presence and degree of STB, PP, and APAD were assessed twice for each patient using LCRs. Additionally, 20 randomly selected LCRs were reexamined by the same observers after two weeks, and Cohen’s kappa analysis was performed to determine the agreement between the two investigators. The agreement was considered substantial, with a weighted kappa of 0.72.
Lateral cephalometric radiographs were used to evaluate CVM stages, the vertical skeletal pattern, and the prevalence of PP, STB, and APAD. Cephalometric analysis was performed using WebCeph software (AssembleCircle Corp., Seongnam-si, Gyeonggi-do, Republic of Korea).
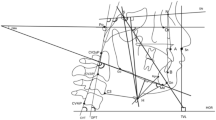
Patients were divided into groups according to the SN‒MP angle (Fig. 1). The SN‒MP angle was evaluated according to Steiner’s analysis28. The Sella (S) is the midpoint of the sella turcica, while the Nasion (Na) is the most anterior point of the frontonasal suture. The SN line is formed by connecting the Sella and Nasion points, representing the anterior cranial base. The Mandibular Plane (MP) is defined by the line extending from the Gonion (Go), located at the angle of the mandible, to the Gnathion (Gn), the most inferior point on the mandibular symphysis, reflecting the inclination of the mandible relative to the cranial base. According to the type of vertical skeletal pattern, the subjects were categorized into three groups: low angle (LA ≤ 28°) (n = 114), normal angle (28° < NA < 36°) (n = 141), and high angle (HA ≥ 36°) (n = 45).

Measurement of the mandibular plane angle (SN-MP) in cephalometric analysis.
The maturation stages of the cervical vertebrae were evaluated following the method outlined by Baccetti et al.29. According to McNamara et al.30, the CS1 and CS2 stages were classified as prepubertal (n = 44), the CS3 and CS4 stages were classified as circumpubertal (n = 104), and the CS5 and CS6 stages were classified as postpubertal (n = 152).
Sella turcica bridging analysis
Sella turcica analysis was performed according to the Leonardi et al.31 standardized scoring scale, and the degree of STB was classified into three types (Fig. 2): Type 1 (no calcification): the length of the sella turcica was equal to or greater than 3/4 of the diameter; Type 2 (partial calcification): less than or equal to 3/4 of sella diameter; Type 3 (complete calcification): only the diaphragm sella was visible on the radiograph.

Types of Sella turcica bridging: no calcification (Type 1, A); partial calcification (Type 2, B); complete calcification (Type 3, C).
Ponticulus posticus analysis
The severity of calcification was assessed by evaluating the lateral cephalometric radiographs (LCRs) and categorized using the standardized scoring scale established by Leonardi et al.31. In this study, partial calcification was further subdivided into two types: open groove and half-open groove. Based on this, the following types were established (Fig. 3): Type 1 (no calcification): no mineralization is observed in the atlanto-occipital ligament; Type 2 (open groove): partial calcification extends from the lateral mass beyond 180°, without reaching the posteromedial margin of the vertebral artery groove; Type 3 (half-open groove): partial calcification extends from the lateral mass beyond 270°, without reaching the posteromedial margin of the vertebral artery groove; Type 4 (complete calcification, full ring): complete bone bridge involving the atlanto-occipital ligament, with complete mineralization extending from the lateral mass to the posteromedial margin of the vertebral artery groove.

Ponticulus posticus types: no calcification (Type 1, A); open groove (Type 2, B); half-open groove (Type 3, C); full ring (Type 4, D).
Atlas posterior arch deficiency analysis
The atlas posterior arch was evaluated based on the presence (Fig. 4A) or absence (Fig. 4B) of the posterior arch, following the methodology proposed by Leonardi et al.32.

Two conditions of the atlas posterior arch: complete (A) and deficient (B).
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics © Version 29.0.0.0) software. The chi-square test was used to examine associations between qualitative independent variables (CVM stage, vertical malocclusions) and the presence of STB, PP, and APAD, with differences in frequency expressed as z scores. The Kolmogorov‒Smirnov test was used to assess the normality of the quantitative variables. The one-sample t test was used to test the null hypothesis. Multinomial logistic regression was used to quantify the influence of predictors (CVM stages and vertical malocclusions) on the outcome variables. Odds ratios expressed the change in odds of being in a nonreference group compared with the reference group, with the goodness-of-fit determined by the Nagelkerke coefficient. Odds ratios and 95% confidence intervals were calculated, and results with p values lower than 0.05 were considered significant.
Results
Demographic characteristics of the sample are presented in Table 1.
The frequency and variations of ponticulus posticus in relation to skeletal age and vertical skeletal pattern are shown in Table 2. PP (types 2, 3, and 4 combined) was most common in postpubertal patients in the CS5 and CS6 stages (48.1%). It occurred more frequently in individuals with a low angle (43.3%) and least frequently in those with a high angle (15.3%). However, the relationships between PP and skeletal age, as well as the vertical skeletal pattern, were not statistically significant (p > 0.05).
The frequency and variations of sella turcica bridging in relation to skeletal age and vertical skeletal pattern are shown in Table 3. STB (types 2 and 3 combined) was significantly more prevalent among postpubertal patients in the CS5 and CS6 stages (58.2%; p = 0.019), and complete bridging was also significantly more common during the postpubertal period (61.7%; p = 0.045). Complete bridging was more common in individuals with a low facial angle (51.1%). However, no significant association was found with the vertical malocclusions (p > 0.05).
The frequency of atlas posterior arch deficiency in relation to skeletal age and the vertical skeletal pattern are shown in Table 4. Patients with a high angle had a significantly greater incidence of deficiency (24.2%) than did those with a complete posterior arch (12.6%) (p = 0.048). APAD was more common in postpubertal patients (45.2%), followed by circumpubertal patients (40.3%). However, it was not significantly associated with CVM stage (p > 0.05).
The associations between the CVM stage, skeletal pattern and PP are presented in Fig. 5. The reference category was type 1 PP. Skeletal age was associated with the presence of PP. Compared with those in the CS6 stage, individuals in the CS5 stage were two times more likely to have an open groove (OR = 2.5, p = 0.027), those in the CS3 stage were three times more likely (OR = 3.2, p = 0.014), and individuals in the CS1 stage were four times more likely (OR = 3.7, p = 0.021). However, no significant association was found between vertical malocclusions and PP (p > 0.05).

Logistic regression analysis of the associations among the cervical maturation stage, vertical skeletal pattern, and PP.
The association between CVM stage, skeletal pattern and STB is presented in Fig. 6. The reference category was type 1 STB. Skeletal age was significantly associated with the presence of STB. Compared with those in the CS6 stage, individuals in the CS3 stage were less likely to have partial bridging (OR = 0.4, p = 0.03). However, no significant association was observed between the vertical skeletal pattern and the STB (p > 0.05).

Logistic regression analysis of the associations between the cervical maturation stage, vertical skeletal pattern, and STB.
The association between CVM stage, skeletal pattern and APAD is presented in Fig. 7. The reference category was the complete atlas posterior arch. Vertical skeletal patterns were significantly associated with the presence of APAD, with low-angle patients being less likely to exhibit APAD than high-angle patients (OR = 0.34, p = 0.003). However, no significant association was found between APAD and CVM stages (p > 0.05).

Logistic regression analysis of the associations between cervical maturation stage, vertical skeletal pattern, and APAD.
Discussion
Early diagnosis and management of health problems in young people, particularly those related to craniofacial development and skeletal growth, are important. Anatomical variations such as ponticulus posticus, sella turcica bridging, and atlas posterior arch deficiency have drawn attention for their potential implications in overall health and craniofacial diagnostics. This study aimed to evaluate the relationship between skeletal patterns, cervical maturation stages, and the morphological features of sella turcica bridging, ponticulus posticus, and atlas posterior arch deficiency.
The maxillofacial complex and the cervical spine originate from neural crest cells33. They influence the development of the neck and shoulders, the process of sella turcica calcification, and the formation and eruption of teeth19. Neural crest cells may contribute to the formation of the sella turcica bridging, as the anterior part of the sella turcica develops from neural crest cells34. These associations might be found in the signalling during early embryogenesis between the notochord, para-axial mesoderm, neural tube, and neural crest5. Developmental alterations in these cells can lead to abnormalities in the sella turcica and the atlas vertebra. Given that these anomalies have the same embryological origin as the maxillofacial complex, they may be associated with alterations in skeletal maloclusions.
A relationship was found between abnormalities in the upper cervical vertebrae and jaw malformations, as well as craniofacial morphology. Arntsen et al. suggested that vertebral anomalies, including posterior arch deficiency of the atlas or ponticulus posticus, may be linked to changes in the skeletal relationships of the maxilla5. In this study, atlas posterior arch deficiency was significantly related to a greater mandibular plane angle. In contrast, Atilla et al. reported that the prevalence of deficient atlas posterior arches was significantly higher in hypodivergent individuals with a low mandibular plane angle compared to those with a high mandibular plane angle8. However, our results are in agreement with those of Ostovarrad et al., who analysed the relationship between cervical spine anomalies and facial types and found that deficiency of the atlas posterior arch was most common in hyperdivergent individuals with a mandibular plane angle of 34° or greater35. Moreover, a previous study revealed that a large cranial base angle is associated with deviations in the morphology of the cervical vertebral column, such as a partial cleft of the posterior arch of the atlas5. These findings show that the mandibular plane angle may be linked to abnormalities in the cervical vertebrae, suggesting that cervical spine anomalies may influence craniofacial development, potentially contributing to malocclusions.
The maxilla and mandible, including the condylar cartilage, originate from tissues derived from the neural crest. During development in the first branchial arch, neural crest cells migrate to the mandible, followed by the maxilla, and then to the nasofrontal region5. Therefore, deviations in the morphology of the cervical vertebral column and craniofacial structures, including the cranial base, may be linked to the development of the jaws, as these structures originate from tissues derived from the neural crest. When evaluating the relationship with the vertical skeletal pattern, complete sella turcica bridging was more common in individuals with a low mandibular plane angle. However, this association was not statistically significant. This finding agrees with that of Atilla et al., who reported no significant relationship between vertical malocclusions and the STB during the adolescent and postadolescent periods8. However, a significant relationship was found in the preadolescent period, with the highest prevalence of complete bridging in low-angle individuals8.
Recent studies have focused on the possible connection between abnormal calcification of the oblique atlantooccipital ligaments and the interclinoid ligament of the sella turcica with age. Current discussions on the relationship between age and the formation of PP or STB are gaining attention. The impact of age on the abnormal calcification of these ligaments is controversial in the literature. Lo Giudice et al. suggested that greater age is not a criterion for the formation of PP and reported that the mean age at which patients first exhibited PP was 10.4 years for the complete form and 9.3 years for the partial form. Additionally, the prevalence of both PP forms was consistently greater during the CS1 stage7. We studied the lateral cephalometric radiographs of 300 patients aged 7–40 years for the presence of PP and STB. Among these patients, the youngest patient with a half-open groove of the PP was 7 years old, and the youngest patient with a full ring was 11 years old. The youngest patient with partial STB was 8 years old, whereas the youngest patient with complete STB was 9 years old. Moreover, in relation to CVM stages, although only STB showed a significant association, both PP and STB were more prevalent in postpubertal patients in the CS5 and CS6 stages. This finding is consistent with the findings of Atilla et al., who reported that the prevalence of complete PP and complete STB increased significantly from the preadolescence period to the postadolescence period8. Erdem et al. also suggested that there may be a relationship between age and PP formation, reporting an increase in the frequency of complete calcification and a decrease in the frequency of partial calcification in older age groups36. These results indicate that while PP and STB can be observed at a young age, progressive calcification of these ligaments, from partial to complete ossification, is possible over time.
Lateral cephalometric radiographs provide diagnostic information about the skull, face, and cervical spine, especially in cases of dental, skeletal, or facial anomalies8,25,37,38. Abnormalities of the cervical spine and cranial base can be identified using radiological methods such as cone beam computed tomography (CBCT) and LCRs39. CBCT allows for more accurate evaluations, as it provides images in a three-dimensional plane, whereas cephalograms are two-dimensional. For this reason, it can be difficult to precisely evaluate the morphological features of the PP and STB on cephalograms, as they may be unilateral or bilateral. Sahoo et al. studied the accuracy of LCRs in assessing the prevalence of PP. CBCT identified 30 cases in the vertebral artery canal, whereas LCRs identified only 26 cases. The results suggest that, in some cases, calcification may not be visible on a cephalogram compared with CBCT40. Although CBCT is more accurate, it is less suitable for initial assessments because of its greater degree of radiation exposure39. In addition, LCRs are more accessible and safer41.
Although CBCT provides three-dimensional imaging and allows more detailed evaluations, LCRs remain a standard diagnostic method routinely performed on patients before orthodontic treatment. While anatomical structures such as the PP, STB, and APAD are often asymptomatic, their early identification is crucial, as they may be associated with potential degenerative changes and complications in the future. Understanding the factors associated with the development of these anatomical structures is important, as it could help in predicting their occurrence. Furthermore, although PP and STB can be observed at a young age, the progressive calcification of these ligaments, which transitions from partial to complete ossification, may occur over time. Therefore, patients exhibiting morphological anomalies of the cervical vertebrae or cranial base during growth should be referred to a team of healthcare specialists to develop individualized treatment plans to prevent health problems in the future. This study has some limitations. One limitation is the substantial agreement between the investigators. Further research with improved evaluator calibration is needed to enhance the reliability and consistency of the measurements. Moreover, future studies evaluating the morphology of the cranial base using the cranial base angle (SN-Ba) measurement could improve the understanding of the relationship between the vertical skeletal pattern and ossification changes in the cranial base and upper cervical spine.
Conclusions
The presence of atlas posterior arch deficiency was significantly associated with vertical malocclusions, which occurred more frequently in patients with a high mandibular plane angle. Sella turcica bridging was significantly more prevalent during the postpubertal period across different cervical maturation stages, suggesting a potential relationship between age and abnormal ligament calcification. Given that sella turcica bridging is asymptomatic and typically occurs postpuberty, early detection using lateral cephalometric radiographs is essential for predicting potential risks, including alterations in craniofacial growth and the development of skeletal anomalies, as well as enabling comprehensive monitoring.
Data availability
The data used in this study are available from the corresponding author upon reasonable request.
Abbreviations
- CS:
-
Cervical stage
- LCR:
-
Lateral cephalometric radiograph
- PP:
-
Ponticulus posticus
- APAD:
-
Atlas posterior arch deficiency
- STB:
-
Sella turcica bridging
- CVM:
-
cervical maturation
- SD:
-
Standard deviation
- LA:
-
Low angle
- NA:
-
Normal angle
- HA:
-
High angle
- CBCT:
-
Cone beam computed tomography
References
Peng, H. et al. Craniocervical posture in patients with skeletal malocclusion and its correlation with craniofacial morphology during different growth periods. Sci. Rep. 14, 5280. https://doi.org/10.1038/s41598-024-55840-w (2024).
Lone, M. I. et al. Dissecting the complexity of skeletal-malocclusion-associated phenotypes: mouse for the rescue. Int. J. Mol. Sci. 24, 2570. https://doi.org/10.3390/ijms24032570 (2023).
Claudino, D. & Traebert, J. Malocclusion, dental aesthetic self-perception and quality of life in a 18 to 21 year-old population: a cross-sectional study. BMC Oral Health. 13, 3. https://doi.org/10.1186/1472-6831-13-3 (2013).
Zohud, O. et al. Towards genetic dissection of skeletal class III malocclusion: a review of genetic variations underlying the phenotype in humans and future directions. J. Clin. Med. 12, 3212. https://doi.org/10.3390/jcm12093212 (2023).
Arntsen, T. & Sonnesen, L. Cervical vertebral column morphology related to craniofacial morphology and head posture in preorthodontic children with class II malocclusion and horizontal maxillary overjet. Am. J. Orthod. Dentofac. Orthop. 140, e1–e7. https://doi.org/10.1016/j.ajodo.2010.10.021 (2011).
Sadler, T. W. Embryology of neural tube development. Am. J. Med. Genet. C Semin Med. Genet. 135C, 2–8. https://doi.org/10.1002/ajmg.c.30049 (2005).
Lo Giudice, A., Caccianiga, G., Crimi, S., Cavallini, C. & Leonardi, R. Frequency and type of ponticulus posticus in a longitudinal sample of nonorthodontically treated patients: relationship with gender, age, skeletal maturity, and skeletal malocclusion. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 126, 291–297. https://doi.org/10.1016/j.oooo.2018.05.001 (2018).
Atilla, A. O., Ozturk, T. & Yagci, A. Comparison of cervical vertebral anomalies and Sella turcica bridging in different growth stages with various vertical skeletal growth patterns. Surg. Radiol. Anat. 43, 117–125. https://doi.org/10.1007/s00276-020-02566-9 (2020).
Tassoker, M., Kok, H. & Ozcan, S. Investigation of the relationship between Sella Turcica Bridge and ponticulus posticus: a lateral cephalometric study. Int. J. Morphol. 35, 337–344 (2017).
Lombardo, C. et al. Ponticulus posticus and skeletal malocclusion: a pilot study in a Southern Italian pre-orthodontic court. Open. Med. 19 https://doi.org/10.1515/med-2024-0965 (2024).
Macrì, M., Rendina, F., Feragalli, B., Pegreffi, F. & Festa, F. Prevalence of ponticulus posticus and migraine in 220 orthodontic patients: a cross-sectional study. Biology 12, 471. https://doi.org/10.3390/biology12030471 (2023).
Schilling, J., Schilling, A. & Galdames, I. S. Ponticulus posticus on the posterior arch of atlas: prevalence analysis in asymptomatic patients. Int. J. Morphol. 28, 317–322 (2010).
Ratnaparkhi, M. M. et al. Co-relation between presence of ponticulus posticus on the lateral cephalogram with cervical pain and vertigo. Eur. J. Mol. Clin. Med. 7, 4047–4053 (2021).
Kim, M. S. Anatomical variant of atlas: arcuate foramen, occipitalization of atlas, and defect of posterior arch of atlas. J. Korean Neurosurg. Soc. 58, 528–533 (2015).
Fang, Y. et al. The first histological observation of a C1 posterior arch defect. Folia Morphol. 82, 386–390 https://doi.org/10.5603/fm.a2022.0035Gökçe G, Morphometric assessment of the sella turcica in different morphologic types of class II malocclusion: a retrospective study. Acıbadem Univ Sağlık Bilim Derg. 2022;13(1):112–118. (2022).
Gökçe, G. & Yavan, M. A. Morphometric assessment of the Sella turcica in different morphologic types of class II malocclusion: a retrospective study. Acıbadem Univ. Sağlık Bilim Derg. 13 (1), 112–118 (2022).
Kaya, Y., Öztaş, E., Goymen, M. & Keskin, S. Sella turcica bridging and ponticulus posticus calcification in subjects with different dental anomalies. Am. J. Orthod. Dentofac. Orthop. 159, 627–634 (2021).
Yohana, W. & Oscandar, F. Prevalence of bridging Sella turcica in orthodontic patients using lateral cephalometry. J. Int. Dent. Med. Res. 17, 3 (2024).
Yan, S. et al. A CBCT investigation of the Sella turcica dimension and Sella turcica bridging in different vertical growth patterns. J. Clin. Med. 12, 1890. https://doi.org/10.3390/jcm12051890 (2023).
Roomaney, I. A. & Chetty, M. Sella turcica morphology in patients with genetic syndromes: a systematic review. Orthod. Craniofac. Res. 24, 194–205. https://doi.org/10.1111/ocr.12426 (2021).
Sato, D. & Endo, T. Size and bridging of the Sella turcica in Japanese orthodontic patients with tooth agenesis. Odontology 108, 730–737. https://doi.org/10.1007/s10266-020-00508-w (2020).
Anusuya, V., Sharan, J. & Jena, A. K. A study of cervical vertebra anomalies among individuals with different sagittal and vertical facial growth patterns. J. Craniovertebral Junction Spine. 11, 75–80. https://doi.org/10.4103/jcvjs.JCVJS_51_20 (2020).
Adisen, S. R., Adisen, M. Z. & Ozdiler, F. E. The evaluation of the relationship between cervical vertebral anomalies with skeletal malocclusion types and upper airway dimensions. CRANIO® 38, 149–157. https://doi.org/10.1080/08869634.2018.1503136 (2018).
Blásquez, J. C. G. Assessment of the ponticulus posticus based on the skeletal relationship in strict lateral radiographs. Imaging Radiat. Res. 4, 55. https://doi.org/10.24294/irr.v4i1.1736 (2008).
Sobouti, F. et al. Associations across 22 dental and craniovertebral anomalies or variations, sagittal skeletal relationships, and vertical growth patterns: a comprehensive epidemiological study of 43 dentoskeletal traits. BMC Oral Health. 23, 877. https://doi.org/10.1186/s12903-023-03504-y (2023).
Ghadimi, M. H., Amini, F., Hamedi, S. & Rakhshan, V. Associations among Sella turcica bridging, atlas arcuate foramen (ponticulus posticus) development, atlas posterior arch deficiency, and the occurrence of palatally displaced canine impaction. Am. J. Orthod. Dentofac. Orthop. 151, 513–520. https://doi.org/10.1016/j.ajodo.2016.08.024 (2017).
Lekavičiūtė, R., Šopagienė, D., Razukevičius, D., Trakinienė, G. & Lopatienė, K. The relationship between orthodontic malocclusion and morphological features of Sella Turcica bridging and ponticulus posticus. Medicina 60, 1853. https://doi.org/10.3390/medicina60111853 (2024).
Steiner, C. C. Cephalometrics for you and me. Am. J. Orthod. 39, 729–755. https://doi.org/10.1016/0002-9416(53)90082-7 (1953).
Baccetti, T., Franchi, L. & McNamara, J. A. Jr. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 11, 119–129 (2005).
McNamara, J. A. & Franchi, L. The cervical vertebral maturation method: a user’s guide. Angle Orthod. 88, 133–143. https://doi.org/10.2319/111517-787.1 (2018).
Leonardi, R., Barbato, E., Vichi, M. & Caltabiano, M. A Sella turcica Bridge in subjects with dental anomalies. Eur. J. Orthod. 28, 580–585. https://doi.org/10.1093/ejo/cjl032 (2006).
Leonardi, R., Barbato, E., Vichi, M. & Caltabiano, M. Skeletal anomalies and normal variants in patients with palatally displaced canines. Angle Orthod. 79, 727–732. https://doi.org/10.2319/082408-448.1 (2009).
Di Venere, D. et al. Calcification of the atlanto-occipital ligament (ponticulus posticus) in orthodontic patients: a retrospective study. Healthc. (Basel). 10, 1234. https://doi.org/10.3390/healthcare10071234 (2022).
Roomaney, I. A. & Chetty, M. Sella turcica morphology in patients with genetic syndromes: protocol for a systematic review. JMIR Res. Protoc. 9, e16633. https://doi.org/10.2196/16633 (2020).
Ostovarrad, F. et al. Cephalometric evaluation of the relationship between cervical vertebral morphology and anomalies and the cranial base angle in different facial types and skeletal classes. Odovtos Int. J. Dent. Sci. 26, 227–235 (2024).
Erdem, S., Gündüz, K. & Kasap, P. Evaluation of the ponticulus posticus. J. Anat. Soc. India. 72, 2 (2023).
Tripodi, D. et al. Ponticulus posticus: clinical and CBCT analysis in a young Italian population. Eur. J. Paediatr. Dent. 20, 219–223. https://doi.org/10.23804/ejpd.2019.20.03.10 (2019).
Li, G., Wang, Q. & Wang, G. Torticollis, facial asymmetry, local pain, and Barré-Liéou syndrome in connection with one-sided ponticulus posticus: a case report and review of the literature. Orthop. Surg. 14, 1235–1240. https://doi.org/10.1111/os.13267 (2022).
Karaman, A. Evaluation of the relationship between Sella turcica bridging and dental anomalies. J. Dent. Indones. 28, 76–81 (2021).
Joshi, V. et al. Evaluation of prevalence and characteristics of ponticulus posticus among Japanese adults: a comparative study between CBCT imaging and lateral cephalogram. Orthod. Waves. 77, 134–141 (2018).
Alqahtani, H. Association between Sella turcica bridging and congenitally missing maxillary lateral incisors. J. Dent. Sci. 15, 59–64. https://doi.org/10.1016/j.jds.2019.07.004 (2020).
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
RL—participated in data collection and analysis, wrote the main manuscript text, prepared figures, performed statistical analyses. DŠ—supervision of research, guidance on data collection. GT—contributed to conception, interpretation of data, revision of the manuscript. KL—supervision of research, contributed to data collection, analysis of data and results, article editing, revision of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Kaunas Regional Biomedical Research Ethics Committee (No. BE-2-71, 12 June 2024). All methods were performed in accordance with the relevant guidelines and regulations. The need of patient informed consent was waived by Kaunas Regional Biomedical Research Ethics Committee because of the retrospective study design.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lekavičiūtė, R., Šopagienė, D., Trakinienė, G. et al. The relationship between vertical malocclusions and ossification changes in the cranial base and upper cervical spine. Sci Rep 15, 17466 (2025). https://doi.org/10.1038/s41598-025-02547-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-02547-1
