
Abstract
Exposure to atmospheric pollutants and meteorological factors is closely linked to human health risks, however, studies in tropical regions remain limited. Assessment of the associations between air pollutants, meteorological factors, and all-cause emergency department visits in Haikou City was conducted to validate the generalizability of previous findings and uncover novel environment-health linkages. We analyzed 1,041,760 ED visits from January 1, 2018, to December 31, 2021, using a distributed lag non-linear model to assess environmental factors’ health effects and lagged impacts with subgroup analyses stratified by gender and age. Additionally, four sensitivity analyses were conducted to verify the robustness of the findings. The results demonstrated significant nonlinear associations between meteorological factors, air pollutants, and emergency department visit risks in Haikou City. PM₂.₅ and PM₁₀ showed nonsignificant effect magnitudes, while temperature (12–25 °C) and relative humidity (80–85%) exhibited protective effects. Low-concentration SO₂ (< 15 µg/m³) and CO (< 0.5 mg/m³) exposures significantly elevated visit risks, whereas high-concentration NO₂ (> 30 µg/m³) exposure displayed hazardous effects. Stratified analyses revealed: that elevated temperatures disproportionately affected males and children; humidity above 80% conferred protection on males and individuals younger than 34 years; elderly males exhibited heightened sensitivity to O₃ and NO₂ exposures; female children faced increased risks from low-concentration CO exposure, and females aged 15–34 showed specific responses to SO₂ exposure. In the tropical coastal city, PM2.5 and PM10 exhibited no significant associations with all-cause emergency risks, while low-level concentrations of SO2 and CO demonstrated specific effects. Although pandemic measures modified certain exposure scenarios, the core mechanisms underlying environment-health associations remained fundamentally unaltered. These findings provide references for revising air quality standards in tropical coastal regions, suggest incorporating SO₂/CO into health warning systems, and propose a climate-pollution co-regulation paradigm for global cities with similar environmental profiles.
Similar content being viewed by others

Introduction
Since the turn of the 21st century, global attention has increasingly focused on air pollution and meteorological conditions. As of 2019, an alarming 99% of the world’s population lived in areas that did not meet the World Health Organization’s air quality guidelines1. Air pollution poses a significant environmental risk to health, contributing to stroke, heart disease, lung cancer, and respiratory diseases such as asthma. Particulate matter and gaseous pollutants are among the most studied air pollutants, along with metals and organic compounds2,3,4. Meteorological factors also play a crucial role in population health, influencing the occurrence and development of diseases1,5. The exposure-response curve between temperature and mortality generally was J-, V-, or U-shaped6, with unsuitable temperatures in a fatality rate of 7.71% (95% CI: 7.43–7.91%). Unsuitable temperatures typically refer to extreme ranges deviating from the minimum mortality temperature (MMT), a critical metric for evaluating temperature-mortality associations, reflecting long-term climatic adaptation. The geographic distribution of MMTs varies across countries, ranging from 14.2 °C to 31.1 °C, decreasing with latitude7. Due to temperature factors, China has the highest economic burden and mortality8. The combined effects of geographical location, climatic characteristics, and demographic structure lead to significant heterogeneity in the associations between environmental factors and health outcomes across studies9,10. Emergency department data were used to assess more temporally sensitive environmental factors and represent their health effects. Short-term exposure to air pollution, particularly SO2, and CO, is associated with increased emergency visits to hospitals for upper respiratory tract infections. This effect is more severe during the cold season than in the warm season11. This study differs from previous reports, which attributed the health effects of air pollution to multiple factors (e.g., air pollution concentration, population characteristics, and the duration and intensity of exposure to air pollutants). Increasing temperatures have a positive correlation with emergency department visits, with children and people in poor areas experiencing the highest impact12. A study in Beijing on the effect of extreme temperatures on the number of emergency department visits for patients with respiratory diseases showed that, particularly in the elderly (age ≥ 65 years), women were more susceptible to extreme temperatures than men13. Wang et al.14 analyzed a risk assessment of heat and emergency department visits at 18 locations with different climatic characteristics in China and noted that heat had a more severe negative health impact on residents living in southern China, subtropical monsoon climate areas, or counties.
Existing literature has predominantly focused on inland regions in China, particularly heavily industrialized and polluted areas such as North China and the Yangtze River Delta, while research on tropical coastal cities remains limited. As China’s first pilot free trade port city, Haikou presents a distinctive context of rapid urbanization coupled with environmental health challenges, requiring localized research to support policy formulation. Compared to typical industrial cities in China (Supplementary Table S1), Haikou, a tourism-driven city with no heavy industries, exhibits concentrations of five major air pollutants below China’s Class I Ambient Air Quality Standards, except for PM2.5 levels slightly exceeding the Class I threshold. Although certain pollutants (PM2.5, PM10, and O3) remain above WHO-recommended guidelines, their exposure levels are among the lowest in Chinese cities, providing a unique perspective for investigating environmental health effects under non-extreme pollution conditions. Our previous study15 confirmed significant associations between short-term exposures to PM2.5, PM10, O3, elevated temperature, and respiratory disease-related emergency department visits in Haikou, identifying susceptible subgroups such as female children and elderly males. This research provided critical baseline data on environmental health effects under non-extreme pollution conditions in tropical settings. However, two major limitations remain in understanding the environmental drivers of all-cause emergency admissions in tropical regions: (1) the environmental-attributable risks for non-respiratory diseases under non-extreme pollution conditions have not been quantified, and (2) the synergistic health effects between tropical climate and complex pollution exposures in China’s non-industrial cities remain insufficiently elucidated. By extending analyses to all-cause emergency visits and refining age stratification (including a newly identified susceptible subgroup aged 15–34 years), this study aims to validate the generalizability of previous findings while uncovering novel environment-health relationships. It provides evidence for formulating regionally differentiated environmental standards—identifying region-specific sensitive pollutants may yield greater public health benefits than solely pursuing WHO global uniform thresholds.
Materials and methods
Study area and study population
Haikou City (19°31′-20°04′ N, 110°07′-110°42′ E), China’s only tropical coastal provincial capital, exhibits three distinctive features16. First, climatically, it is influenced by monsoons and oceanic regulation, with an annual average temperature of 24.4 °C, average relative humidity exceeding 80%, annual precipitation of approximately 1,664 mm, prolonged sunshine duration, and intense solar radiation. Second, regarding air pollutant characteristics, Haikou consistently ranks among China’s cities with the highest air quality, classified in the lowest pollution tier among 168 key monitored cities, exhibiting a pollution profile dominated by traffic and construction emissions rather than industrial sources. Third, in terms of population dynamics, the city receives over 25 million annual tourists, resulting in seasonal overloads of healthcare resources. The case data used in this study were derived from the medical record information systems of three tertiary A general hospitals in Haikou City. The data covers daily emergency department visits from January 1, 2018, to December 31, 2021, including outpatient and inpatient medical records. The main information extracted from the records includes the patient’s name, age, gender, date of visit, disease category, and current address. This study follows the data collection framework of previous research, including identical hospitals, timeframes, and quality control procedures, but expands the case selection criteria from respiratory diseases (ICD-10: J00-J99) to all-cause emergency visits to comprehensively assess environmental health burdens.
Pollutants and meteorological data
Daily time series data, comprising meteorological and air pollutant concentrations, were collected from January 1, 2018, to December 31, 2021. The meteorological data, including daily mean temperature and daily mean relative humidity, were sourced from the Hainan Meteorological Bureau. The atmospheric pollutant data were obtained from the China Air Quality Online Monitoring Platform (https://www.aqistudy.cn/historydata/) and included daily mean levels of nitrogen dioxide (NO2), ozone (O3), sulfur dioxide (SO2), carbon monoxide (CO), and particulate matter (PM2.5 and PM10), the unit for CO is mg/m³, while other pollutants are measured in µg/m³. The mean concentrations of NO2, SO2, CO, PM2.5, and PM10 represent 24-hour averages. Additionally, the mean concentrations of O3 were based on the maximum 8-hour value.
Statistical analysis
In this study, Microsoft Excel 2019 software was utilized to clean and process the raw data, while SPSS 22.0 was employed for descriptive statistics of emergency department case data, air pollution data, and meteorological data. The aim was to investigate the time trend and demographic characteristics of daily emergency department visits, as well as to describe the time trend and distribution characteristics of air pollutants and meteorological factors. Normal tests were carried out for daily emergency department visits, air pollutants, and meteorological factors, revealing that none of them followed a normal distribution. To calculate the correlation coefficients between the number of emergency department visits and air pollutants and meteorological data, RStudio software and Spearman correlation analysis were utilized, and related factors with the number of emergency department visits were selected. Previous studies have established that there are intricate correlations between air pollution and meteorological factors17. To avoid multicollinearity issues, when the absolute value of the correlation coefficient between two air pollutants or two meteorological factors exceeded 0.7, it was deemed to have moderate to high linear correlation18, and thus could not be included in the model simultaneously when constructing it.
The robustness of the findings was validated through four sensitivity analyses. Temporal stratification analysis: The study period was stratified into three intervals—the entire period, pre-COVID-19 pandemic, and pandemic periods—to assess the impact of each factor on all-cause emergency visits while controlling for pandemic interference. Time-variable parameterization testing: The degrees of freedom for time variables were adjusted to test the model’s sensitivity and robustness to assumptions regarding temporal trends. Disease category heterogeneity analysis: All-cause emergency visits were further categorized into circulatory and respiratory disease emergencies to explore differential effects of exposure factors on these two disease groups. Segmented effect validation: Consistency in effect estimates before and during the pandemic was compared to confirm that conclusions were unaffected by data heterogeneity across pandemic periods.
Data analysis was conducted using the R programming language (version 4.2.0), employing the mgcv, splines, dlnm, and ggplot2 packages to establish the DLNM model. The median (P50) of individual factors was employed as the reference value, while the relative risk (RR) value with a 95% confidence interval (95% CI) was used to assess the effect of every single factor on the number of emergency department visits. A two-sided test was conducted, with P < 0.05 being considered statistically significant.
Construction of the distributed lag nonlinear model
Daily emergency department visits were combined with air pollutants and meteorological factors and linked by date. Time series analysis was employed to estimate the overall association for the entire study period (2018 to 2021). The population in Haikou remained relatively stable throughout the study period, and the daily emergency department visits were approximately Poisson distributed. However, due to overdispersion in the data, the standard Poisson method may lead to larger errors. Thus, this study used a quasi-Poisson distribution instead of a Poisson distribution[19,20].
Numerous studies have demonstrated that the effects of environmental factors on human health are nonlinear and hysteretic21,22,23,24. Therefore, a distributed lag nonlinear model with quasi-Poisson distribution was employed in this study to investigate the effects of air pollutants and meteorological factors on emergency department visits.
The central concept of the DLNM is to incorporate cross-bases for the transformation of study variables into generalized additive models that allow simultaneous estimation of exposure effects and lag effects25. In this study, single air pollutants or single meteorological factors were modeled separately, and in the construction of the univariate model, except for the investigated univariate factors, other factors were included in the model as confounders in the form of natural spline functions. To control the long-term trend of time variables, time variables were included in the model in the form of a natural spline function. Additionally, the day-of-week effect and holiday effect were included in the model in the form of a dummy variable and binary variable, respectively, to control the daily visit volume. The final model expression was as follows:
Where log [E (Yt)] is the link function and Yt is the number of emergency department visits on day t; E (Yt) is the mathematical expectation of emergency department visits on day t; α is the intercept of the model; Xt, l is a two-dimensional matrix of the variables studied obtained by the “crossbasis” function in the DLNM model, l indicates the maximum lag days and β is the coefficient of the matrix; ns indicates the use of a natural cubic spline function as a smoothing function to control the effect of confounders, and Timet is a time series variable used to control long-term trends and seasonal effects, df is the degree of freedom, year is the year of study; Xi is other air pollutants or meteorological factors not included in the model; as. factor is a function in R language used to convert the transmitted object into Factor; dowt is a categorical variable that refers to which day of the week has an impact and is included in the model as a dummy variable to control its impact. holidayt is a binary variable used to control the holiday effects.
Given that the data are overdispersed, Akaike’s quasi-Poisson information criterion (Q-AIC) was utilized to determine the degrees of freedom of each variable in the model26. Finally, it was determined that the degrees of freedom were 3 for air pollutants or meteorological factors not included in the model and 8 for time variables. Based on previous literature, we set the maximum lag days to 14 days27,28.
Results
Descriptive statistical analysis
Over the study period from January 1, 2018, to December 31, 2021, a total of 1,041,760 emergency department visits were recorded (Table 1). The daily average number of visits to the emergency department was 713. The means of meteorological factors were 25.24 ℃ for temperature, 80.33% for humidity, 5.32 h for sun time, 2.8 m/s for wind speed, and 1004.01 hpa for air pressure. The means of air pollutants were 15.67 µg/m3 for PM2.5, 30.16 µg/m3 for PM10, 11.3 µg/m3 for NO2, 4.62 µg/m3 for SO2, 0.54 mg/m3 for CO, and 77.81 µg/m3 for O3, respectively (Table 2).
Time series analysis
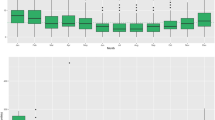
In Fig. 1, the number of emergency department visits increased each year, with a sharp decline observed at the beginning of 2020, which may be attributed to the outbreak of COVID-19. In response to the epidemic, cities across the country were closed, resulting in reduced visits to emergency departments. The average daily temperature and air pressure showed clear seasonal periodicity, with opposite directions of periodic fluctuation. Specifically, the average daily temperature was higher in summer and lower in winter, while air pressure was lower in summer and higher in winter. The average daily wind speed was greater in winter, while no significant periodicity was observed in the average daily relative humidity and average daily sunshine hours. The average daily concentrations of PM2.5, PM10, NO2, and SO2 exhibited similar periodicity and were higher in autumn and winter. Conversely, no significant periodicity was observed in the average daily concentrations of CO and O3.

Time sequence diagram of emergency department visits, meteorological factors, and air pollutants in Haikou City from 2018 to 2021, ED emergency department visits, Temp temperature, RH relative humidity, ST sun time, WS: wind speed, AP air pressure.
Correlation analysis
Spearman’s correlation coefficient is a non-parametric measure that evaluates the correlation between two graded ordinal variables using monotonic equations29. As the data did not follow a normal distribution, Spearman correlation analysis was employed, and the correlation coefficients all passed the t-test, which was statistically significant (P < 0.05). As shown in Supplementary Table S2, daily emergency department visits were positively correlated with sunshine hours (r = 0.08), temperature (r = 0.17), PM10 (r = 0.05), O3 (r = 0.19), as well as NO2 (r = 0.1). Conversely, they were negatively correlated with relative humidity (r = − 0.13), wind speed (r = − 0.07), CO (r = − 0.11), and SO2 (r = − 0.1). Furthermore, no significant correlation was observed between daily emergency department visits and air pressure (r = − 0.04).
Analysis by DLNM
Based on the results of Spearman correlation analysis, PM2.5 (r = 0.04) and PM10 (r = 0.05) showed no significant association with emergency department visits. Further multivariate linear screening revealed a high linear correlation between PM2.5 and PM10 (r = 0.91), while PM2.5 (r = -0.53) and PM10 (r = -0.47) exhibited significant negative correlations with temperature. Based on the predetermined threshold (r ≥ 0.7), PM2.5 and PM10 were separately included in the final model for DLNM analysis, but their lag effects showed no statistical significance (complete results are presented in Supplementary Tables S3 and S4). Daily average temperature, daily average relative humidity, NO2, SO2, CO, and O3 were incorporated into the model for analysis, with results reported using the median values of each factor as reference. In Fig. 2, a peak visit risk was observed when the temperature was 8.5 ℃ with a lag of 3 days (RR = 1.065, 95% CI: 1.020–1.112) and when the temperature was 33 ℃ with a lag of 9 days (RR = 1.021, 95% CI: 1.003–1.039). For relative humidity, a peak visit risk was observed at 36% with a lag of 3 days (RR = 1.055, 95% CI: 0.989–1.124). Regarding air pollutants, a peak visit risk was observed when the average daily concentrations of NO2 were 40 µg/m3 and 41 µg/m3, respectively, at lag2 and lag10 (RR = 1.028, 95% CI: 0.980–1.081) and (RR = 1.054, 95% CI: 1.007–1.102), respectively. Furthermore, a peak visit risk was observed when the average daily concentrations of SO2, CO, and O3 were 14 µg/m3, 0.2 mg/m3, and 205 µg/m3, respectively, at lag3, lag10, and lag8 (RR = 1.045, 95% CI: 1.006–1.086), (RR = 1.019, 95% CI: 1.003–1.035), and (RR = 1.027, 95% CI: 0.993–1.061), respectively.

The three-dimensional graphs of the relative risks of emergency department visits with different contributing factors versus lag days from 2018 to 2021, with the median of each factor as the reference value.
In Fig. 3, the effect of each factor on emergency department visits exhibited a lag effect from day 0 throughout the lag period. Specifically, when the temperature was within 8.5 ℃-25 ℃, a lower temperature was associated with a lower visit risk at lag0-lag2. For relative humidity within 36-60%, a lower relative humidity was associated with a lower visit risk at lag0-lag1, lag5-lag9, and lag12-lag14. Regarding air pollutants, the average daily concentration of NO2 at 25–41 µg/m3 was associated with a higher visit risk at lag0-lag4. The average daily concentration of SO2 at 10–23 µg/m3 was associated with a higher visit risk at lag12-lag14. Moreover, the average daily concentration of O3 at 150–207 µg/m3 was associated with a higher visit risk at lag0-lag2. Conversely, the average daily concentration of CO at 0.2–0.4 mg/m3 was associated with a higher visit risk with a lag of 0–6 days, and a smaller concentration was associated with a higher visit risk. Overall, these findings suggest that temperature, relative humidity, and air pollutant concentrations have a significant impact on emergency department visits, and their effects exhibit a lag effect over time.

Contour graphs of different contributing factors on emergency department visits at different lag days from 2018 to 2021, red areas indicate hazardous effects and blue areas indicate protective effects, with the median of each factor as the reference value.
In Fig. 4, the effect curve between average daily temperature and emergency department visits exhibited a “V” pattern, with the lowest risk of visits observed at a temperature of 17 ℃ (RR = 0.795, 95% CI: 0.738–0.856). Regarding relative humidity, a visit risk increase was observed in the range of 75-80%, while a decrease in visit risk was observed in the range of 80-85%. For air pollutants, a concentration of NO2 greater than 30 µg/m3 was associated with a higher visit risk. The effect curve between SO2 and emergency department visits exhibited an “inverted V” pattern, with the greatest visit risk observed when the average daily concentration was 15 µg/m3 (RR = 1.457, 95% CI: 1.126–1.885). Moreover, the effect curve between CO and emergency department visits exhibited an “S” pattern, with the greatest visit risk observed when the average daily concentration of CO was 0.2 mg/m3 (RR = 1.191, 95% CI: 1.072–1.323). However, no statistically significant effect of O3 on emergency department visits was observed. These findings suggest that temperature, relative humidity, and air pollutant concentrations have complex and nonlinear effects on emergency department visits. Specifically, the effect curves exhibit different patterns for different factors, highlighting the importance of considering multiple factors when assessing the risk of emergency department visits.

Exposure-response curves (red solid lines) and 95% confidence intervals (grey areas) between different contributing factors and relative risks of emergency department visits from 2018 to 2021, with the median of each factor as the reference value.
In Supplementary Figure S1, the effect plots of each factor on emergency department visits by gender were found to be similar. Hypothermia had a greater impact on emergency department visits in men. When the temperature was at 17 °C, the lowest risk of visits was (RR = 0.800, 95% CI: 0.741–0.864) and (RR = 0.814, 95% CI: 0.744–0.889), respectively. Additionally, a relative humidity greater than 80% was associated with a reduction in the number of male emergency department visits. The impact of NO2 on male emergency department visits was also observed. Regarding women, the effect of SO2 on emergency department visits exhibited the greatest visit risk at an average daily concentration of SO2 of 15 µg/m3 (RR = 1.421, 95% CI: 1.079–1.870) and (RR = 1.507, 95% CI: 1.113–2.039), respectively. Furthermore, a low concentration of CO (< 0.4 mg/m3) was found to affect women, while O3 was found to affect men.
In Supplementary Figure S2, the effects of low temperature (< 15 ℃), low relative humidity (< 50%), high concentration of NO2 (> 30 µg/m3), and high concentration of O3 (> 150 µg/m3) on the elderly (> 65 years) were assessed, as well as the effects of high temperature (> 25 ℃) and CO on children (0–14 years). Furthermore, the effect of SO2 on people aged 15–34 years was evaluated, with the greatest visit risk observed when the concentration was 20 µg/m3 (RR = 2.196, 95% CI: 1.168–4.129). Regarding relative humidity, a value greater than 80% was associated with a reduction in emergency department visits for individuals aged 0–14 years and 15–34 years. These findings suggest that relative humidity is protective in reducing emergency department visits for these age groups.
In this study, the 5th, 25th, 75th, and 95th percentiles of Haikou temperature and relative humidity, as well as the 10th and 90th percentiles of air pollutants, were selected to calculate the RR and 95% CI of specific factors for emergency department visits at different lag days using the median as the reference value.
In Table 3, the visit risk was found to be lowest when the temperature was 17 ℃ with a cumulative lag of 14 days (RR = 0.796, 95% CI: 0.736–0.860), while the visit risk was highest when the humidity was 75% at cumulative lag0-14d (RR = 1.022, 95% CI: 1.006–1.037). Supplementary Table S5 revealed that when the concentration of SO2 was at 3 µg/m3 with a cumulative lag of 0–7 days, the highest visit risk was observed (RR = 1.030, 95% CI: 1.015–1.046). Moreover, when the CO concentration was at 0.4 mg/m3 with a cumulative lag of 14 days, the highest visit risk was observed (RR = 1.035, 95% CI: 1.010–1.061). However, NO2 and O3 were found to be statistically insignificant at specific concentration values.
In Fig. 5, the optimal lag period was assessed, and it was found that a 1 ℃ increase in temperature and a 1% increase in relative humidity increased the risk of emergency department visits by 1.019% (95% CI: 1.012-1.027%) and 0.999% (95% CI: 0.998-1.000%), respectively. Moreover, a 10 µg/m3 increase in NO2, SO2, and O3 concentrations and a 0.5 mg/m3 increase in CO concentrations were found to increase the risk of emergency department visits by 1.010% (95% CI: 0.964-1.057%), 1.419% (95% CI: 1.137-1.770%), 0.995% (95% CI: 0.937-1.057%), and 1.004% (95% CI: 0.995-1.014%), respectively.

The relative risks and 95% confidence intervals of increasing percentage of emergency department visits by different contributing factors at different lag days from 2018 to 2021, with the median of each factor as the reference value.
In Supplementary Table S6, analyzed by gender and age, during the optimal lag period, with a 1 ℃ increase in temperature and a 1% increase in relative humidity, a 10 µg/m3 increase in NO2, SO2, and O3 concentrations, and a 0.5 mg/m3 increase in CO concentration, the percentage increase in the risk of emergency department visits is as follows. The increase of 1 °C in temperature may have a more significant impact on emergency department visits among males and children, while a 1% increase in humidity does not show significant differences based on gender or age. A 10 µg/m³ increase in NO2 concentration may have a greater effect on males and children, while a 10 µg/m³ increase in SO2 concentration may have a greater effect on females and children.
Sensitivity analyses
The segmented sensitivity analysis revealed that, at specific values of different factors, effect estimates from the full-period and segmented models were generally consistent in direction, with minimal variability, indicating a low risk of distortion in core conclusions due to pandemic-related data (Supplementary Tables S7-S10). Temperature, humidity, and O3 demonstrated similar effect estimates during the entire period and pre-pandemic period, whereas NO2, SO2, and CO exhibited comparable effect estimates during the entire period and pandemic period (Supplementary Figures S3 and S4). To verify the robustness of the model, sensitivity analysis results (Supplementary Figures S5 and S6) were generated by varying the degrees of freedom (df = 7–10) for the time variable to plot 3D effect diagrams of lagged impacts of different factors on emergency department visits. The results demonstrated that when adjusting the degrees of freedom for the time variable, the effect plots remained similar, indicating appropriate parameter settings and model stability. The disease category heterogeneity analysis demonstrated that temperature and O3 were significantly associated with both all-cause and disease-specific emergency visits. Ozone exhibited the strongest association with respiratory disease emergencies and ranked second in circulatory system diseases (Supplementary Table S11). High temperature (29 °C) showed acute effects on all-cause and respiratory emergencies, concentrated within 0–2 lag days. In contrast, ozone (94 µg/m³) displayed a significant delayed effect on cardiovascular emergencies at a 7-day lag, highlighting the need for long-term exposure monitoring (Supplementary Table S12). Analysis of environmental factors associated with cardiovascular disease-related emergency visits revealed that low temperature, elevated PM10, and NO2 increased cardiovascular emergency risks. The dose-response relationship between O3 and cardiovascular emergencies approximated a U-shaped curve (Supplementary Figures S7 and S8).
Discussion
This study found that even in Haikou, one of the least polluted cities in China, major air pollutants and temperature still exhibited significant health effects. This suggests that China’s environmental air quality standards may underestimate the sensitivity of populations in tropical regions to low-dose pollution. There is a need to develop climate-zone-specific risk assessment models, and future studies should incorporate temperature-humidity-pollutant interaction terms.
Consistent with previous specialized studies on respiratory diseases15, this study identified O3 and NO2 as significant risk factors for all-cause emergency admissions, while the effects of PM2.5 and PM10 did not reach significance (P > 0.05). In Haikou, a tropical region, despite higher PM2.5 and PM10 concentrations (relative to WHO guideline thresholds), their health impacts were less pronounced, potentially reflecting a ‘tropical paradox’ This may be explained by the fact that in high-humidity environments, airborne particles more readily absorb moisture, increasing their size—i.e., PM2.5 and PM10 mass concentrations may rise. However, their primary component is sea salt, which exhibits lower toxicity, leading to less severe overall health impacts compared to regions where PM2.5 toxicity is driven by heavy metals30. Future studies should validate this hypothesis through composition-resolved toxicity assessments. This discrepancy may also stem from the etiological heterogeneity of all-cause emergency admissions, as particulate matter predominantly drives respiratory events31, while other systemic diseases are more influenced by meteorological factors. The disease category heterogeneity analysis revealed that the strong association between O3 and respiratory emergencies aligns with its potent oxidative properties and airway inflammatory mechanisms32. Notably, O3’s secondary but significant effect on cardiovascular diseases may originate from its potential pathways inducing systemic oxidative stress, endothelial dysfunction, and hypercoagulability33. In contrast, the acute effects of high temperature (29 °C) on all-cause and respiratory emergencies (0–2 day lag) reflect rapid pathological processes involving the breach of physiological compensation thresholds under heat stress, while its preferential respiratory impact may relate to heat-induced increases in mucosal permeability and allergen dispersion. The 7-day lagged cardiovascular effects of O3 suggest health risks potentially emerging through cumulative tissue damage or delayed immune modulation, consistent with findings from European multi-city studies documenting delayed associations between O3 exposure and myocardial infarction risks34. It is recommended to incorporate lag-effect adjustment parameters into existing air quality warning systems, particularly emphasizing mid-to-long-term health surveillance following high O3 episodes. The positive associations of low temperature, PM10, and NO2 with cardiovascular emergencies likely conform to classical pathways involving cold-induced vasoconstriction, particle-driven atherosclerosis progression, and NO2-mediated endothelial dysfunction33.
In terms of total effect difference, the results of this study showed that temperatures between 12 ℃ and 25 ℃ decreased emergency department visits, which was consistent with the results of previous studies14,34 This validates the protective effect of the intermediate temperature range (12–25 °C), which approximates the human thermal neutral zone, where no additional metabolic heat production or dissipation is required, thereby reducing cardiovascular and respiratory system stress. Studies indicate that extreme temperatures may elevate blood viscosity and exacerbate inflammatory responses, triggering cardiovascular, cerebrovascular, and respiratory diseases36. Moderate temperatures likely mitigate the acute risks of these conditions. In tropical regions with year-round high temperatures, lower temperatures are often associated with higher wind speeds or precipitation, which reduce concentrations of pollutants such as PM2.5 and ozone, thereby mitigating respiratory irritation. Additionally, the activity of vectors for certain mosquito-borne diseases diminishes at lower temperatures, potentially reducing infection risks. When the humidity ranges between 80% and 85%, the number of emergency department visits decreases, which is inconsistent with previous findings37. This may be associated with the unique climatic adaptation in tropical regions and pollutant-meteorological interactions. First, long-term exposure to high humidity may enhance physiological tolerance to heat and moisture among local residents through improved sweat evaporation efficiency and optimization of mucosal defense mechanisms38. Second, high humidity may indirectly reduce pollutant-related health risks by promoting particle deposition and suppressing ozone formation. Notably, discrepancies between this phenomenon and prior research findings may reflect geographical heterogeneity in humidity-related health effects, as baseline climatic conditions can significantly alter risk thresholds of environmental factors39. Future studies should combine personalized exposure monitoring with disease-stratified analyses to further elucidate these mechanisms. High concentrations of NO2 (> 30 µg/m3) resulted in an increased risk of emergency department visits, consistent with previous findings40. NO2 is a major oxidative gaseous pollutant in the atmosphere and can cause systemic oxidative damage and airway inflammation41,42. This study found an increasing trend in emergency risk when O3 concentrations exceeded 120 µg/m³, with confidence intervals encompassing 1, though the trend aligns with most studies43,44. The non-significance of this result may stem from the following factors. First, the limited number of exposure days with O3 > 120 µg/m³ in Haikou reduced statistical power. Second, O3 effects may be amplified through synergistic interactions with high temperatures, but the absence of interaction term analysis in this study might underestimate its true risk. Additionally, long-term exposure to higher background O3 levels in tropical populations may reduce sensitivity through behavioral adaptations (e.g., minimizing outdoor activities during peak heat periods). Future research should expand sample sizes and incorporate multi-city data to further validate the uniqueness of O3 health effects in tropical regions. Notably, the effect directions of SO2 and CO in this study contradicted reports from industrial cities45,46,47,48. Building on prior respiratory studies, we hypothesize that secondary aerosol conversion of SO2 under tropical marine climates may enhance its toxicity, while high temperatures accelerate CO dispersion yet amplify low-concentration exposure effects through thermal stress synergism. This suggests that environmental health risk assessments in low-pollution areas require integrated meteorology-pollutant interaction models. This study found that the cumulative lag effects of temperature, humidity, SO2, and CO persisted for up to 14 days, demonstrating greater significance compared to single-day lag models, which may reflect progressive pathological mechanisms of environmental exposure. First, the chronic toxicity of SO2 and CO requires cumulative activation of oxidative stress and inflammatory pathways. CO inhibits cytochrome C oxidase, leading to mitochondrial dysfunction49, with effects becoming pronounced after sustained exposure over multiple days. Second, the synergistic effects of temperature and humidity may prolong biological response times to heat stress and allergen exposure. High temperatures suppress heat shock protein repair capacity, while high humidity promotes dust mite proliferation50, collectively contributing to delayed exacerbation of chronic respiratory diseases. Additionally, distributed lag models, by integrating multi-day exposure weights, more sensitively captured the cumulative effects of environmental stressors, a finding consistent with conclusions from global multi-city studies51,52.
This study revealed significant population heterogeneity in the health effects of environmental factors. The pronounced impact of high temperatures on males and children highlights the interaction between physiological vulnerability and behavioral exposure, with elevated metabolic rates and occupational exposure in males and immature thermoregulatory systems in children constituting critical risk pathways53. The protective effects observed for males and individuals under 34 years old at a humidity above 80% may reflect behavioral adaptations (e.g., surge in air conditioning use) offsetting physiological risks, suggesting that the prevalence of climate-adaptive infrastructure may redefine traditional exposure-response relationships. The heightened sensitivity of elderly males to O3 and NO2 may be linked to chronic respiratory disease burdens and smoking54, while the unique response of female children to low-concentration CO could relate to sex-based differences in hemoglobin levels and prolonged household exposure55,56. The significant effect of SO2 on females aged 15–34 may indicate emerging risk sources such as cosmetic use and occupational exposure. These findings emphasize the need for environmental health policies to transition from ‘one-size-fits-all’ approaches to precision interventions, such as O3 warning systems targeting elderly males and mandatory installation of CO detectors in households with female children.
This study found that although traffic restrictions during the COVID-19 pandemic led to declines in emergency department visits and concentrations of certain pollutants (PM2.5, NO2, and SO2) in early 2020, increased photochemical reactions resulted in elevated O3 levels, potentially partially offsetting the pandemic’s overall environmental effects. On the other hand, segmented sensitivity analysis revealed pandemic-specific modifications in exposure-response relationships. Temperature, humidity, and O3 exhibited similar effect estimates across the entire study period and pre-pandemic phase, suggesting that pandemic control measures significantly altered temperature-related emergency risk pathways, potentially linked to reduced cold exposure due to home confinement and modified physiological responses to heat stress from mask usage57. In contrast, NO2, SO2, and CO showed consistent effect estimates during both the entire period and pandemic phase, reflecting persistent industrial emission impacts3, while lower pre-pandemic effect values may stem from China’s 2019 clean air initiatives. The differential modification of health effects for meteorological factors and specific pollutants by the pandemic does not weaken the conclusions but rather provides new empirical insights into socio-environmental interactions. Further comparative analyses confirmed the reliability of core findings. Sensitivity analyses demonstrated that the directionality and significance levels of effect estimates remained highly consistent across segmented models under varying environmental factor thresholds, with coefficients of variation generally below 15%. Low coefficients of variation suggest spatiotemporal reproducibility in environment-health associations58, necessitating the development of dynamic risk assessment models through multi-regional cohort studies, with particular emphasis on precise identification of the “inflection concentration” in U-shaped dose-response curves. Nevertheless, we recommend validating these findings with longer-term data, particularly from the post-pandemic era.
The strengths of this study lie in being the first systematic investigation in a low-pollution tropical Chinese city to delineate the response mechanisms of all-cause emergency visits to multiple environmental factors, revealing latent risks of SO2 and CO below WHO thresholds and their climate-mediated amplification effects. This provides a template for environmental health risk assessment in other tropical coastal cities globally and informs regional adaptations of WHO guidelines. Through methodological innovation and large-sample empirical validation, the research bridges the paradigm from ‘high-pollution industrial cities’ to ‘low-emission tourist cities’. However, several limitations warrant consideration. As an ecological study employing time-series analysis, this work did not incorporate pathogenicity, socioeconomic status, education level, or personal habits into models, potentially introducing exposure misclassification. COVID-19 restrictions were treated as confounders, and pandemic control policies might have introduced unquantifiable selection bias. Future studies could employ interrupted time-series analysis to disentangle the interference mechanisms of public health emergencies on environment-health associations. The single-city focus (Haikou) limits generalizability; expanding data collection to multiple cities in Hainan Province would enhance representativeness. Additionally, the reliance on emergency department records from three major hospitals in Haikou may not capture all potential cases, and the absence of individual-level exposure data might partially influence the findings.
Conclusion
This study systematically elucidates the distinct mechanisms underlying environmental health effects in a tropical city through four-year emergency department big data coupled with DLNM models, yielding the following key findings. Significant emergency visit risks persist even at low concentrations of SO2 and CO, challenging traditional linear risk models. The low toxicity of sea salt aerosols and their climate-driven rapid dispersion collectively obscure the health signals of PM2.5 and PM10. The pandemic induced differential modification in the health effects of specific environmental factors, providing novel empirical dimensions for understanding socio-environmental interactions. Tailored to tropical climatic features, we recommend lowering SO₂ health alert thresholds and establishing a ‘high temperature-O3 compound alert’ mechanism. The study identifies females aged 15–34 and elderly males as high-risk populations, necessitating prioritized deployment of mobile monitoring stations at their activity hotspots (schools, senior communities).
Data availability
Meteorological data were obtained from the Hainan Meteorological Bureau, and air pollution data were collected from the China Air Quality Online Monitoring Platform (https://www.aqistudy.cn/historydata/). Because of the confidentiality requirements of this study, the emergency department dataset was not made publicly available but could be obtained from the corresponding author on reasonable request.
References
Murray, C. J. L. et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396 (10258), 1223–1249 (2020).
Chen, C. et al. Ambient air pollution and daily hospital admissions for mental disorders in Shanghai, China. Sci. Total Environ. 613–614, 324–330 (2018).
Lakra, A. R., Gautam, S., Samuel, C. & Blaga, R. College bus commuter exposures to air pollutants in Indian City: the urban-rural transportation exposure study. Geosyst. Geoenvironment. 4 (1), 100346 (2025).
Blaga, R. & Gautam, S. Improving PM10 sensor accuracy in urban areas through calibration in Timișoara. Npj Clim. Atmospheric Sci. 7 (1), 268 (2024).
Patella, V. et al. Atopic dermatitis severity during exposure to air pollutants and weather changes with an artificial neural network (ANN) analysis. Pediatr. Allergy Immunol. 31, 938–945 (2020).
Song, X. P. et al. The impact of heat waves and cold spells on respiratory emergency department visits in Beijing, China. Sci. Total Environ. 615, 1499–1505 (2018).
Tobías, A. et al. Geographical variations of the minimum mortality temperature at a global scale. Environmental Epidemiology, 5(5) (2021).
Gasparrini, A. et al. Mortality risks attributable to high and low ambient temperature: a multicountry observational study. Lancet 386, 369–375 (2015).
Park, J., Kim, H. J., Lee, C. H., Lee, C. H. & Lee, H. W. Impact of long-term exposure to ambient air pollution on the incidence of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Environ. Res. 194, 110703 (2021).
Tsai, S. S., Chang, C. C. & Yang, C. Y. Fine particulate air pollution and hospital admissions for chronic obstructive pulmonary disease: a case-crossover study in Taipei. Int. J. Environ. Res. Public Health. 10 (11), 6015–6026 (2013).
Liu, Y. et al. Association between air pollution and emergency department visits for upper respiratory tract infection in Lanzhou, China. Environ. Sci. Pollut. Res. 29 (19), 28816–28828 (2022).
Corcuera, H. I. & Hajat, S. The effects of temperature on accident and emergency department attendances in London: A Time-Series regression analysis. Int. J. Environ. Res. Public Health. 17 (6), 1957 (2020).
Ma, Y. et al. Effects of extreme temperatures on hospital emergency room visits for respiratory diseases in Beijing, China. Environ. Sci. Pollut. Res. 26 (3), 3055–3064 (2019).
Wang, Y. et al. High temperatures and emergency department visits in 18 sites with different Climatic characteristics in China: risk assessment and attributable fraction identification. Environ. In. 136, 105486 (2020).
Peng, J. et al. Short-term effects of low-level PM2.5, PM10, O3, and tropical meteorological conditions on emergency department visits for respiratory diseases in Haikou, China. Asian Pac. J. Trop. Med. 17 (7), 317–328 (2024).
Wu, S., Xing, C. & Zhu, J. Climatic characteristic analysis of Hainan Island. J. Trop. Biology. 13 (4), 315–323 (2022).
Ulpiani, G., Ranzi, G. & Santamouris, M. Local synergies and antagonisms between meteorological factors and air pollution: A 15-year comprehensive study in the Sydney region. Sci. Total Environ. 788, 147783 (2021).
Mukaka, M. Statistics corner: a guide to the appropriate use of correlation coefficient in medical research. Malawi Med. J. 24 (3), 69–71 (2012).
Liao, J. et al. Short-term effects of climatic variables of hand, foot, and mouth disease in mainland China, 2008–2013: A Multilevel Spatial Poisson Regression Model Accounting for Overdispersion. PLOS ONE, 11 (1) e0147054 20.
Pan A, Sarnat SE, Chang HH. Time-series analysis of air pollution and health accounting for covariate-dependent overdispersion. Am. J. Epidemiol.,187(12):2698–2704 (2018).
Hu, Y. et al. The relative impact of meteorological factors and air pollutants on childhood allergic diseases in Shanghai, China. Sci. Total Environ. 706, 135975 (2020).
Wang, J. et al. Short-term effect of meteorological factors on the risk of rheumatoid arthritis hospital admissions: A distributed lag non-linear analysis in Hefei, China. Environ. Res. 207, 112168 (2022).
Wang, W. et al. Epidemiological characteristics of tuberculosis and effects of meteorological factors and air pollutants on tuberculosis in Shijiazhuang, China: A distribution lag non-linear analysis. Environ. Res. 195, 110310 (2021).
Luo, C. et al. Long-term air pollution levels modify the relationships between short-term exposure to meteorological factors, air pollution, and the incidence of hand, foot and mouth disease in children: a DLNM-based multicity time series study in Sichuan Province, China. BMC Public. Health. 22 (1), 1484 (2022).
Pan, H. et al. Comparison of survival outcomes among patients with breast Cancer with distant vs ipsilateral supraclavicular lymph node metastases. JAMA Netw. Open. 4 (3), e211809 (2020).
Portet, S. A primer on model selection using the Akaike information criterion. Infect. Dis. Model. 5, 111–128 (2020).
Lin, Q. et al. The effects of excess degree-hours on mortality in Guangzhou, China. Environ. Res. 176, 108510 (2019).
Bont, J. et al. Associations between ambient temperature and risk of preterm birth in Sweden: A comparison of analytical approaches. Environ. Res. 213, 113586 (2022).
Song, X. et al. The impact of main air pollutants on respiratory emergency department visits and the modification effects of temperature in Beijing, China. Environ. Sci. Pollut. Res. 28 (6), 6990–7000 (2021).
Ahbil, K., Sellami, F., Baati, H., Gautam, S. & Azri, C. Influence of localized sources and meteorological conditions on dry-deposited particles: A case study of Gabès, Tunisia. Sci. Total Environ. 954, 176726 (2024).
Szyszkowicz, M. & Angelis, N. D. Urban air pollution and emergency department visits for cardiac and respiratory diseases. Adv. Environ. Eng. Res. 03 (01), 005 (2022).
Stowell, J. D. et al. Warm season ambient Ozone and children’s health in the USA. Int. J. Epidemiol. 53 (2), dyae035 (2024).
Zhang, Z. et al. Association of long-term exposure to Ozone with cardiovascular mortality and its metabolic mediators: evidence from a nationwide, population-based, prospective cohort study. The Lancet Reg. Health – Western Pacific, 52 (2024).
Święczkowski, M. et al. Association between exposure to air pollution and increased ischaemic stroke incidence: a retrospective population-based cohort study (EP-PARTICLES study). Eur. J. Prev. Cardiol. 32 (4), 276–287 (2025).
Chen, R. et al. Association between ambient temperature and mortality risk and burden: time series study in 272 main Chinese cities. BMJ 363, k4306 (2018).
De Souza, A. et al. Analyzing maximum temperature trends and extremes in Brazil: A study of climate variability and anthropogenic influences from 1960 to 2020. Aerosol Sci. Engineering, (2025).
Haas, M. et al. Meteorological extremes and their impact on tinnitus-related emergency room visits: a time-series analysis. Eur. Arch. Otorhinolaryngol. 280 (9), 3997–4007 (2023).
Périard, J. D., Eijsvogels, T. M. H. & Daanen, H. A. M. Exercise under heat stress: thermoregulation, hydration, performance implications, and mitigation strategies. Physiol. Rev. 101 (4), 1873–1979 (2021).
Rising, J., Tedesco, M., Piontek, F. & Stainforth, D. A. The missing risks of climate change. Nature 610 (7933), 643–651 (2022).
Szyszkowicz, M., Schoen, S. & Angelis, N. D. Air pollution and emergency department visits for disease of the genitourinary system. Environ. Health Insights. 15, 11786302211025360 (2021).
Arjomandi, M. et al. Respiratory responses to Ozone exposure. Moses (the multicenter Ozone study in older subjects). Am. J. Respir. Crit Care Med. 197 (10), 1319–1327 (2018).
Williams, M. L., Atkinson, R. W., Anderson, H. R. & Kelly, F. J. Associations between daily mortality in London and combined oxidant capacity, Ozone, and nitrogen dioxide. Air Qual. Atmos. Health. 7 (4), 407–414 (2014).
Tian, Y. et al. Short-term effect of ambient Ozone on daily emergency room visits in Beijing, China. Sci. Rep. 8 (1), 2775 (2018).
He, C. et al. Synergistic PM2.5 and O3 control to address the emerging global PM2.5-O3 compound pollution challenges. Eco-Environment Health. 3 (3), 325–337 (2024).
Gao, H. Y. et al. Short-term effects of gaseous air pollutants on outpatient visits for respiratory diseases: a case-crossover study in Baotou, China. Environ. Sci. Pollut. Res. 29 (33), 49937–49946 (2022).
Ding, P. H., Wang, G. S., Guo, Y. L., Chang, S. C. & Wan, G. H. Urban air pollution and meteorological factors affect emergency department visits of elderly patients with chronic obstructive pulmonary disease in Taiwan. Environ. Pollut. 224, 751–758 (2017).
Zhu, Y. et al. Joint effect of multiple air pollutants on daily emergency department visits in Chengdu, China. Environ. Pollut. 257, 113548 (2020).
Patel, D. et al. Joint effect of heatwaves and air quality on emergency department attendances for vulnerable population in Perth, Western Australia, 2006 to 2015. Environ. Res. 174, 80–87 (2019).
Scimeca, M. et al. Impact of the environmental pollution on cardiovascular diseases: from epidemiological to molecular evidence. Heliyon, 10(18) (2024).
Bergmann, K. C. et al. Impact of climate change on allergic diseases in Germany. J. Health Monit. 8 (4), 76–102 (2023).
Lin, H. et al. Hourly peak concentration measuring the PM2.5-mortality association: results from six cities in the Pearl river Delta study. Atmos. Environ. 161, 27–33 (2017).
Mokoena, K. K., Ethan, C. J., Yu, Y., Shale, K. & Liu, F. Ambient air pollution and respiratory mortality in Xi’an, China: a time-series analysis. Respir. Res. 20 (1), 139 (2019).
Mo, Z. et al. Acute effects of air pollution on respiratory disease mortalities and outpatients in southeastern China. Sci. Rep. 8 (1), 3461 (2018).
He, M., Zhong, Y., Chen, Y., Zhong, N. & Lai, K. Association of short-term exposure to air pollution with emergency visits for respiratory diseases in children. iScience 25 (9), 104879 (2022).
Cheng, C. Y. et al. Association between ambient air pollution and emergency room visits for pediatric respiratory diseases: the impact of COVID-19 pandemic. Toxics 10 (5), 247 (2022).
Tseng, H. W., Lu, L. Y. & Shiue, Y. L. Short-term impact of ambient air pollution exposure on daily clinic visits for patients with urticaria in Kaohsiung, Taiwan. Air Qual. Atmos. Health. 14 (7), 1063–1070 (2021).
Figi, C. E. et al. Literature review of physiological strain of personal protective equipment on personnel in the high-consequence infectious disease isolation environment. Am. J. Infect. Control. 51 (12), 1384–1391 (2023).
Kumar, R. P., Perumpully, S. J., Samuel, C. & Gautam, S. Exposure and health: A progress update by evaluation and scientometric analysis. Stoch. Env. Res. Risk Assess. 37 (2), 453–465 (2023).
Funding
This research was funded by the National Key R&D Program of China (NO. 2023YFC3011805), National Natural Science Foundation of China (No: 81960351), Research Foundation for Advanced Talents of Hainan (No: 822RC835), and Province Natural Science Key Foundation of Hainan (No: ZDYF 2019125).
Author information
Authors and Affiliations
Contributions
J.C.P. was responsible for the conception and design of the study, J.Q., J.C.L., W.X.Z., Z.Y.L., and Z.L. were responsible for data gathering, X.X.W., J.C., Y.Y., N.L., Y.H., and M.L. were responsible for data analysis, J.C.P. drafted the manuscript, X.R.L. responsible for the critical review of the paper. All authors participated in the interpretation of the data.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peng, J., Wu, X., Chen, J. et al. Short-term effects of ambient air pollutants and meteorological factors on emergency department visits in tropical Haikou, China. Sci Rep 15, 20849 (2025). https://doi.org/10.1038/s41598-025-03517-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-03517-3
