
Abstract
This study aims to evaluate the acid inhibition and clinical improvement of the addition of bedtime lafutidine to esomeprazole in comparison with esomeprazole only in Gastroesophageal reflux disease (GERD) patients with nocturnal symptoms. We conducted a single-center, observer-blinded, randomized, clinical trial. Forty-eight consecutive GERD patients with nocturnal symptoms were randomized to take twice daily esomeprazole, 20 mg (ESO Group, n = 24) or twice daily esomeprazole, 20 mg, with bedtime lafutidine, 10 mg (LAF & ESO Group, n = 24) for one week. The 24-h impedance-pH monitoring, and high-resolution manometry were measured on the seventh day during the treatment. The symptoms and sleep quality were assessed both at baseline and following treatment. Intragastric pH > 4 holding time ratios were significantly higher in the LAF & ESO Group compared to the ESO Group, both overall (85.4% vs. 77.7%, P = 0.003) and specifically during nighttime (92.6% vs. 77.2%, P = 0.006). Furthermore, the incidence of nocturnal acid breakthrough (NAB) was markedly reduced in the LAF & ESO Group (29.2% vs. 75.0%, P = 0.001). Esophageal acid exposure times, however, were comparable between the two groups (P > 0.05). Although both groups experienced symptom improvement, patients in the LAF & ESO Group demonstrated superior enhancement in sleep quality, as measured by the Pittsburgh Sleep Quality Index. Notably, patients without NAB exhibited a more substantial improvement in sleep quality from baseline after treatment. Therefore, adding bedtime lafutidine to esomeprazole effectively inhibits nocturnal gastric acid secretion and reduces the incidence of NAB. GERD patients who received lafutidine in addition to esomeprazole achieved a more significant improvement in sleep quality correlated with NAB reduction.
Similar content being viewed by others
Introduction
Gastroesophageal reflux disease (GERD) is a condition that results from the reflux of gastric contents into the esophagus, often accompanied by symptoms such as heartburn and regurgitation1. It has been estimated that approximately 50–80% of GERD patients experience nighttime symptoms2. Nocturnal symptoms can disturb sleep and daytime function3 and even induce more severe esophageal mucosal damage, such as peptic stricture and adenocarcinoma4,5.
Although proton-pump Inhibitors (PPIs) are commonly recommended as first-line drugs for treating GERD6, 37–76% of GERD patients treated with high-dose PPIs still suffer uncontrolled nocturnal symptoms7,8,9,10. A main reason is that PPIs often fail to suppress acid secretion throughout the nocturnal period, and even up to 70% of patients on PPIs have nocturnal acid-breakthrough (NAB)11,12. Thus, there is a clinical rationale for reducing nocturnal acid secretion.
Histamine is the major stimulator of nocturnal acid secretion. H2 receptor antagonist (H2RA) competitively blocks histamine binding to the H2 receptor and effectively inhibits nocturnal acid secretion13,14. A single nocturnal dose of H2RA could control acid output significantly better than the twice-daily dosage, so bedtime H2RA should be recommended in clinical practice15. Compared to PPIs alone, adding bedtime ranitidine or famotidine could significantly decrease nocturnal gastric acidity and the prevalence of NAB in healthy volunteers or GERD patients16,17. Lafutidine is a new-generation H2RA with a higher endoscopic healing rate and heartburn relief rate in patients with GERD than first-generation H2RA18,19. So, lafutidine may have stronger symptom control and nocturnal acid inhibition potential. However, there is no evidence on the efficacy of lafutidine for GERD patients with nocturnal symptoms.
Therefore, a randomized controlled clinical trial (RCT) was designed to evaluate the intragastric and esophageal acid inhibition, and the clinical improvement of adding bedtime lafutidine to esomeprazole in comparison with esomeprazole only in GERD patients with nocturnal symptoms.
Materials and methods
Study design
We conducted a single-center, observer-blinded RCT in China between March 2022 and April 2023. This study was approved by the medical ethics committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology ([2021] (0940–01)). It has been registered at the Chinese Clinical Trial Registry on January 10, 2022 (ChiCTR2200055479). The study was performed in accordance with declaration of Helinski.
Participants
We hypothesized that the incidence of NAB would be 20% in the ESO & LAF group and 60% in the ESO group. A difference of 10% between the two groups is considered clinically significant. Assuming a dropout rate of 10%, for 80% power at an alpha level of 0.05 with a two-side test, the required number of two groups were both 30. An interim analysis was conducted when enrollment reached 80% of the calculated sample size. The clinical trial was terminated early due to the demonstration of significant efficacy of primary outcomes.
Written informed consent was obtained from all eligible participants. Patients had to meet all of the inclusion criteria for enrollment: 1) aged between 18 and 65 years old; 2) GERD-Q score ≥ 8 with nocturnal symptoms (regurgitation or heartburn); 3) completed upper endoscopy within the past year; 4) willingness to take part in this study.
Patients with any of the following conditions were excluded:1) There are contraindications to esophageal high-resolution esophageal manometry (HREM) and 24-h pH monitoring such as cardiopulmonary dysfunction, esophageal stenosis or varices; 2) pregnant or lactating women; 3) participating in other clinical studies; 4) Taking gastric acid inhibit drugs within one week; 5) Communication or coordination disorders.
Study methods
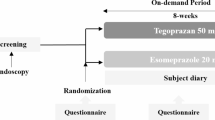
The duration of treatment was one week. Patients were randomly assigned to either the treatment group (LAF& ESO: lafutidine 10 mg at bedtime, esomeprazole 20 mg twice daily) or the control group (ESO: esomeprazole 20 mg twice daily). Baseline information, symptom evaluation, and sleep quality were assessed when patients were enrolled and completed the treatment. HREM and 24-h pH monitoring were performed on the last day of the treatment.
Randomization and blinding
For patient randomization, we generated a block of random numbers using Microsoft Excel 2019. Patients were not blinded to their treatment assignments. Additionally, the physicians involved in our study were divided into two categories: Physician A (blinded) was responsible for enrollment, data collection, and outcome evaluation. Physician B (unblinded) was specialized in prescribing the assigned medications according to the randomization protocol.
Drugs and safety assessments
The study medications used were Lafutidine 5 mg (Grand Pharmaceutical Group Co., Ltd.) and Esomeprazole 20 mg (AstraZeneca, Ltd.). During the study, participants were prohibited from using other gastric acid inhibitors, gastric mucosal protectants, prokinetic agents, antacids, or antispasmodic agents. No new medications were permitted to be initiated during the study period. The number of remaining prescribed drugs tables was checked when the treatment duration was over. Compliance was considered good if patients took 85% or more of their assigned medications.
Adverse events were actively monitored daily throughout the study via telephone calls. In the event that patients reported any adverse events, physical examinations and laboratory analyses were promptly conducted.
Outcome measures
The primary outcome was the intragastric pH metrics assessed after one week of treatment, including occurrence rate of NAB and gastric pH > 4 holding time ratio (pH 4 HTR). The secondary outcomes are esophageal pH metrics, changes in symptom scores, and sleep quality scores.
High-resolution esophageal manometry
Before pH monitoring, all patients underwent HREM using a water perfusion catheter (Medkinetic, Ltd). Two experienced investigators performed the data analysis. We collected parameters such as low esophageal sphincter (LES) pressure and esophagogastric junction (EGJ) morphology (EGJ I, II, or III) based on Chicago Classification v3.020. Hypotensive EGJ was defined when LES pressure was < 10 mm Hg. If the frequency of the ineffective swallow reached 50% out of water swallows, ineffective esophageal motility (IEM) was diagnosed20.
24-h pH monitoring
The 24-h pH monitoring was performed after an overnight fast using a catheter (VersaFlex, Given Imaging) with two pH sensors placed 15 cm apart. The proximal pH probe recorded esophageal pH was placed 5 cm above LES, while the distal probe recorded the gastric pH was placed in the stomach. Patients were instructed to record the time of the positions (upright or supine), meals, and symptoms occurring in the diary. Two experienced investigators analyzed the data by using the Accuview pH-Z V5.2 software.
The pH 4 HTR was defined as the % time of intragastric pH > 4. A fall of pH below 4 at 5 cm above LES was taken to indicate esophageal acid reflux. The esophageal acid reflux numbers and durations were recorded. The nighttime period was defined as between 11 PM and 7 AM, while the rest of the day before 11 PM was considered daytime. NAB was defined as a drop in intra-gastric pH of less than 4 continuously for more than one hour during the nighttime period. Patients were given 20 mg of esomeprazole on the day of pH monitoring on an empty stomach in the morning.
Symptom assessment
Reflux symptoms were comprehensively assessed using validated scales, including the GERD questionnaire (GERD-Q), Reflux disease questionnaire (RDQ), and Reflux symptom index (RSI). Additionally, heartburn and regurgitation symptoms were specifically assessed before and after treatment: The frequency of these symptoms was categorized as follows: 0 days (score = 0), 1 day (score = 1), 2–3 days (score = 2), 4–5 days (score = 3), and 6–7 days per week (score = 4). The severity of symptoms was assessed by the Visual Analogue Scale (VAS) score from 0 to 10. The total symptom score was calculated by multiplying the frequency score by the severity score, yielding a minimum score of 0 and a maximum score of 40. PPI responders were the patients whose symptoms improved for more than 50% compared with the baseline.
Sleep quality evaluation
Sleep quality was evaluated by the Pittsburgh Sleep Quality Index (PSQI). The PSQI had seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, used sleep medication, and daytime dysfunction.
Statistical analysis
The primary outcome analysis was conducted based on the intention-to-treat (ITT) population, comprising all patients who received at least one dose of study medication. Multiple imputations were performed to address missing data for primary outcomes. All outcome analyses were further evaluated in the per-protocol (PP) population, which included patients who adhered to their assigned treatment regimen and completed the 1-week follow-up questionnaire and esophageal measurements. The continuous data were described by median and interquartile ranges. The difference in scale scores before and after treatment were compared using the Wilcoxon test. Other continuous data were compared using the Mann–Whitney U test. The distribution of the categorical data was expressed as a percentage (%). Categoric data were compared using the chi-squared test. Interim analysis used O’Brien-Fleming boundaries. The significance level (p-value) with 2-tails was set at 0.05. All statistical analysis was performed using SPSS statistics 25.0 (IBM, Armonk, NY, USA).
Results
Baseline characteristics
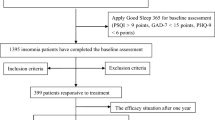
Forty-eight patients were included from fifty-nine enrolled participants. Thirty-nine completed the 1-week follow-up questionnaire, HRM and 24 h-pH monitoring (Fig. 1). The observed effect (Z score:3.681) exceeded the boundary (bound: 3.471), triggering predefined stopping criteria at 48 patients (80% planned sample).The demographic and clinical characteristics were comparable between the two groups (Table 1). No severe adverse events occurred during the study period.

Flow chart of the study. Fifty-nine participants were screened, and Forty-eight patients (Intention to treat set) were included. Thirty-nine patients (Pre-protocol set) completed the follow-up esophageal examination.
Inhibition of gastric and esophageal pH
By both ITT and PP analysis, the gastric pH 4 HTRs were significantly higher in the LAF& ESO Group compared to the ESO Group during the 24-h period (ITT: 85.4% vs. 77.7%, P = 0.006; PP: 87.9% vs. 77.7%, P = 0.012) and the nighttime (ITT: 92.6% vs. 77.2%, P = 0.003; PP: 96.9% vs 68.4%, P < 0.001). In contrast, the daytime pH 4 HTRs were similar between two groups (ITT: 84.4% vs 82.4%, P = 0.370; PP: 84.4% vs 84.6%, P = 0.728) (Fig. 2a–f). Additionally, the incidence of NAB was significantly lower in the LAF & ESO group than in the ESO group (ITT: 29.2% vs. 75.0%, P = 0.001; PP: 21.1% vs. 80.0%, P < 0.001).

The intragastric 24-h pH parameters of participants of two groups. (a) All-day intragastric pH 4 HTR by ITT analysis; (b) Daytime intragastric pH 4 HTR by ITT analysis; (c) Nighttime intragastric pH 4 HTR by ITT analysis; (d) All-day intragastric pH 4 HTR by PP analysis; (e) Daytime intragastric pH 4 HTR by PP analysis; (f) Nighttime intragastric pH 4 HTR by PP analysis; (g) The median intragastric pH value curves in 24 h period. ITT: Intention to treat set; PP: Pre-protocol set; pH 4 HTR: pH > 4 holding time ratio; Solid black line: lafutidine and esomeprazole group; Dashed gray line: esomeprazole group.
In the PP set, patients with LAF & ESO exhibited higher intragastric pH values from 23:00 to 7:00 than patients with ESO, as illustrated by the intragastric pH curves (Fig. 2g). Besides, the onset of NAB in the ESO group demonstrated a time-delayed trend, even extending into the early morning. In contrast, all NAB events in the LAF & ESO group occurred between 23:00 and 1:00 (Supplement Table 1). Esophageal acid exposure time and acid reflux events were comparable between the two groups, both during nighttime and daytime(P > 0.05) (Table 2).
Symptom and Sleep quality improvement
By PP analysis, both the scores of symptom scales (GERD-Q, RDQ, and RSI) and reflux symptoms (daytime or nighttime heartburn, and regurgitation) decreased after treatment in both groups (P < 0.05) (Table 3). The PSQI scores also decreased significantly after treatment in both groups (P < 0.05) by PP analysis (Supplementary Table 2). Among the multiple sleep dimensions, patients in the LAF & ESO group exhibited more remarkable improvements in subjective sleep quality, sleep disturbance, and used sleep medication, though these differences did not reach statistical significance (Supplementary Table 2).
The relationship between NAB and Sleep quality, symptom improvement
The improvement of night sleep quality is related to the occurrence of NAB and the duration of nocturnal gastric acid suppression time. Specifically, there was no significant difference in PSQI scores before and after treatment among patients with NAB (13.5 vs. 11.0, p = 0.582). However, the PSQI scores decreased significantly among patients without NAB (10.0 vs. 6.0, p = 0.019). In terms of the PSQI dimensions, the differences were more pronounced in patients with NAB compared to those without NAB (Table 4). Besides, the 24-h (r = 0.361, p = 0.024) and nocturnal (r = 0.307, p = 0.057) gastric acid suppression time were correlated with the changes in PSQI scores. Within the PSQI dimensions, only subjective sleep quality was significantly correlated with both 24-h (r = 0.352, p = 0.028) and nocturnal (r = 0.392, p = 0.014) acid suppression time.
The response rates to treatment for daytime and nighttime heartburn and regurgitation symptoms showed no statistically significant differences between patients with and without NAB (p > 0.05). However, the treatment response rates for nighttime heartburn and regurgitation were numerically higher in patients without NAB (nighttime heartburn: 80.0% vs. 64.3%; nighttime reflux: 73.3% vs. 64.3%) (Fig. 3).

The response rate of heartburn and regurgitation of patients with or without NAB. The response rates to treatment for daytime and nighttime heartburn and regurgitation symptoms showed no statistically significant differences between patients with and without NAB (p > 0.05). However, the treatment response rates for nighttime heartburn and regurgitation were numerically higher in patients without NAB. NAB: nocturnal acid-breakthrough
Discussion
In summary, patients receiving LAF & ESO exhibited a significant increase in intragastric pH from 23:00 to 07:00 compared to those receiving ESO alone. The gastric pH 4 HTRs were higher in the LAF & ESO group than in the ESO group, with a more pronounced difference observed during nighttime. The occurrence rate of NAB in patients with LAF & ESO significantly decreased. Esophageal acid exposure times were comparable between the two groups (P > 0.05). While both groups experienced symptom improvement, patients in the LAF & ESO group demonstrated superior enhancement in sleep quality dimensions, as measured by PSQI. Moreover, patients without NAB exhibited a more substantial improvement in sleep quality from baseline after treatment.
Adding bedtime lafutidine to twice-daily PPIs emerged as a highly effective strategy for potent nocturnal acid inhibition. Although 29.2% of patients with LAF & ESO still suffered NAB, none occurred in the early morning. This may be attributed to lafutidine’s rapid achievement of effective plasma concentrations within three hours of administration. The Seoul Consensus 2020 explicitly noted that adding a bedtime H2RA can improve nocturnal pH control and symptoms21. Moreover, bedtime lafutidine demonstrated superior nocturnal acid suppression compared to conventional H₂RAs. For instance, the administration of omeprazole twice daily with bedtime ranitidine significantly increased gastric pH 4 HTRs to 84.0% for the supine period, but the NAB rate remained at 59.0%16. Similarly, adding bedtime ranitidine, famotidine, or nizatidine to twice-daily PPIs increased the median overnight pH 4 HTRs to 96.5%, yet NAB still occurred in 40.0% of GERD patients17. Although Lyon Consensus 2.0 recommended that clinicians should first confirm adequate esophageal acid suppression via on-PPI pH monitoring before escalating therapy22, for patients with persistent nocturnal symptoms despite standard PPI therapy, adjunctive lafutidine offered a mechanistically rational strategy to address gastric acid suppression, even reduce NAB.
Previous studies have demonstrated that tachyphylaxis to oral H2RAs primarily manifested one week after initial dosing, whereas intravenous administration has been documented to induce tolerance within 2–3 days23. Notably, our investigation revealed no observable tachyphylaxis phenomena in patient-reported symptom relief metrics during one week of continuous oral lafutidine therapy. Lafutidine’s unique dual mechanism—combining H2RA with transient receptor potential vanilloid 1 (TRPV1)-mediated sensory neuromodulation—may delay tolerance onset. Based on these findings, we proposed the incorporation of one-week bedtime lafutidine administration as a viable one-week therapeutic strategy for GERD patients with nocturnal symptoms. However, the absence of tachyphylaxis signals at Day 7 did not guarantee durability beyond this window. Future investigations are warranted to characterize tachyphylaxis patterns associated with prolonged lafutidine use by incorporate serial pH monitoring and symptom recording.
Although Potassium-Competitive Acid Blockers (PCABs) has been widely used and achieves near-complete acid suppression, PCABs were not recommended as initial therapy for nocturnal acid suppression conditions in which clinical superiority has not been vilidated. PCABs demonstrated superior nocturnal acid suppression duration. Vonoprazan 20 mg once daily achieved nocturnal acid suppression duration of approximately 75%-100%24,25,26 , while ESO combined with LAF exhibited 92.6% nocturnal acid suppression. Notably, the incidence of NAB was 0% with PCABs, in contrast to 29.2% observed with ESO & LAF therapy. However, as American Gastroenterological Association (AGA) Institute Clinical Practice Update recommended, clinicians should generally not use PCABs as initial therapy for acid-related conditions. Factors such as more medication costs and greater obstacles to obtaining PCABs may outweigh potential advantages related to acid inhibition. So PCABs may play a role in patients with acid-related disorders who fail PPI therapy. In terms of the safety data, recent studies have showned that the use of PCABs was associated with a higher gastric cancer risk (HR 1.92; 95% CI, 1.13–3.25; P = 0.016) compared with H2RA during the follow-up period (mean, 3.65 years)27. Furthermore, PCABs elevated serum gastrin levels to a greater extent compared to PPIs28. A study proposing a novel therapeutic regimen demonstrated that the addition of lafutidine 10 mg to vonoprazan 10 mg achieved sufficient acid inhibition, particularly during nocturnal periods, without inducing further increases in serum gastrin levels25. Considering the widespread availability of PCABs, combination therapy utilizing low-dose PCABs with lafutidine may represent a promising therapeutic alternative. Therefore, lafutidine’s clinical benefits and safety profile ensure ongoing relevance in personalized GERD care, particularly as global disparities in PCAB access persist.
Though the addition of lafutidine to esomeprazole showed outstanding gastric acid inhibition, we did not observe a beneficial effect on esophageal pH parameters. The lack of intergroup differences in esophageal acid metrics challenged a direct reflux-mediated mechanism. This aligns with prior evidence that NAB often represented an isolated gastric phenomenon without proportional esophageal acidification29,30,31,32. Our study also supported the opinion that no esophageal acid reflux episodes happened during the NAB period among GERD patients. Therefore, the comparable esophageal acid exposure between the two groups was reasonable.
The addition of lafutidine to PPI effectively alleviated the symptoms of gastroesophageal reflux disease (GERD) overall. Interestingly, the suppression of NAB did not enhance the efficacy of treatment for nighttime heartburn or regurgitation symptoms (p > 0.05). The comparable symptom outcomes of patients with and without NAB were consistent with previous research findings. For instance, an Indian study involving 58 GERD patients treated with oral PPIs reported no statistically significant difference in the incidence of nighttime symptoms between patients with and without NAB (31% vs. 37.5%, p = 0.756)32. However, in our study, treatment response rates were numerically higher among patients without NAB, suggesting that NAB might have a certain impact on treatment efficacy, although this effect did not reach statistical significance. Further studies with larger sample sizes are warranted to explore this potential influence.
Lafutidine significantly improved sleep quality, with the degree of improvement in sleep scores being associated with NAB and nocturnal acid suppression. A previous cross-sectional survey of 56 GERD patients demonstrated that the addition of nighttime H2RA to PPI therapy improved GERD-associated sleep disturbances in 67% (18/27) of patients33. NAB reduction alleviated gastric mucosal irritation, indirectly improving sleep through somatic comfort. As previously reported, H2RAs significantly reduced acid secretion not only via histamine but also through vagal pathways34.Unlike other H2RAs, lafutidine can induce TRPV1 activation leading to sensory nerve desensitization and analgesia, which may contribute to symptom improvement and better sleep35,36. Additionally, TRPV1 is expressed in the hippocampus and hypothalamus, which are key brain regions regulating sleep and wakefulness. So the sleep benefit was a true improvement in sleep quality, not simply medication-induced sleepiness. An animal study in rats has shown that activation of TRPV1 receptors leaded to increased delta waves and decreased alpha and beta waves in sleep-stage electroencephalograms, indicating deeper sleep states and reduced sleep disturbances37. As such, this study represented the first prospective RCT to suggest that lafutidine may have a potential role in improving sleep quality in patients with GERD. Future investigations should incorporate objective evidence (such as polysomnography) to quantify sleep architecture and explore lafutidine’s neuromodulatory mechanisms in GERD-related sleep dysfunction.
There are some limitations in our study. First, the observation period was limited to one week, but the long-term efficacy, particularly the H2RA tachyphylaxis remained unknown. Second, our study was conducted in a single center in China without investigating the CYP2C19 genotype. This study design limited direct extrapolation to diverse populations. Future multi-center validation with genetic polymorphism profiling is essential to delineate population-specific efficacy. Third, The lack of baseline pH monitoring data precluded direct quantification of pretreatment nocturnal acid exposure patterns of participants. The open-label design and and lack of placebo control introduced expectancy bias in patient-reported outcomes like PSQI, though objective metrics (such as, NAB incidence) were the primary outcomes. At last, stopping early could overestimate primary benefits, along with the fact that some secondary endpoints (nocturnal symptom relief differences, etc.) may have been underpowered due to the smaller sample. These limited the external validity of our results. Future multicenter studies with larger and more diverse sample sizes are needed to address these limitations and further validate our findings.
Conclusion
The addition of bedtime lafutidine to esomeprazole significantly increased nocturnal intragastric pH > 4 holding time ratios and decrease the occurrence of NAB. GERD patients with the addition of lafutidine experienced a more pronounced improvement in sleep quality correlated with NAB reduction.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Maret-Ouda, J., Markar, S. R. & Lagergren, J. Gastroesophageal Reflux Disease: A Review. JAMA 324(24), 2536–2547 (2020).
Gerson, L. B. & Fass, R. A systematic review of the definitions, prevalence, and response to treatment of nocturnal gastroesophageal reflux disease. Clin. Gastroenterol. Hepatol. 7(4), 372–367 (2009).
Shaker, R., Castell, D. O., Schoenfeld, P. S. & Spechler, S. J. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am. J. Gastroenterol. 98(7), 1487–1493 (2003).
Orr, W. C., Allen, M. L. & Robinson, M. The pattern of nocturnal and diurnal esophageal acid exposure in the pathogenesis of erosive mucosal damage. Am. J. Gastroenterol. 89(4), 509–512 (1994).
Lagergren, J., Bergström, R., Lindgren, A. & Nyrén, O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N. Engl. J. Med. 340(11), 825–831 (1999).
Yadlapati R, Gyawali CP, Pandolfino JE; CGIT GERD Consensus Conference Participants. AGA Clinical Practice Update on the Personalized Approach to the Evaluation and Management of GERD: Expert Review [published correction appears in Clin Gastroenterol Hepatol. 2022 Sep;20(9):2156]. Clin. Gastroenterol Hepatol.. (2022).
Peura, D. A., Riff, D. S., Snoddy, A. M. & Fennerty, M. B. Clinical trial: lansoprazole 15 or 30 mg once daily vs. placebo for treatment of frequent nighttime heartburn in self-treating subjects. Aliment Pharmacol. Ther. 30(5), 459–468 (2009).
Johnson, D., Crawley, J. A., Hwang, C. & Brown, K. Clinical trial: esomeprazole for moderate-to-severe nighttime heartburn and gastro-oesophageal reflux disease-related sleep disturbances. Aliment Pharmacol. Ther. 32(2), 182–190 (2010).
Fass, R. et al. Clinical trial: the effects of the proton pump inhibitor dexlansoprazole MR on daytime and nighttime heartburn in patients with non-erosive reflux disease. Aliment Pharmacol. Ther. 29(12), 1261–1272 (2009).
Fass, R. et al. The effect of dexlansoprazole MR on nocturnal heartburn and GERD-related sleep disturbances in patients with symptomatic GERD. Am. J. Gastroenterol. 106(3), 421–431 (2011).
Nzeako, U. C. & Murray, J. A. An evaluation of the clinical implications of acid breakthrough in patients on proton pump inhibitor therapy. Aliment Pharmacol. Ther. 16(7), 1309–1316 (2002).
Katz, P. O., Anderson, C., Khoury, R. & Castell, D. O. Gastro-oesophageal reflux associated with nocturnal gastric acid breakthrough on proton pump inhibitors. Aliment Pharmacol. Ther. 12(12), 1231–1234 (1998).
Shirai, N. et al. Comparison of lansoprazole and famotidine for gastric acid inhibition during the daytime and night-time in different CYP2C19 genotype groups. Aliment Pharmacol. Ther. 16(4), 837–846 (2002).
Engevik, A. C., Kaji, I. & Goldenring, J. R. The Physiology of the Gastric Parietal Cell. Physiol. Rev. 100(2), 573–602 (2020).
Gledhill, T., Howard, O. M., Buck, M., Paul, A. & Hunt, R. H. Single nocturnal dose of an H2 receptor antagonist for the treatment of duodenal ulcer. Gut 24(10), 904–908 (1983).
Fackler, W. K., Ours, T. M., Vaezi, M. F. & Richter, J. E. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology 122(3), 625–632 (2002).
Xue, S., Katz, P. O., Banerjee, P., Tutuian, R. & Castell, D. O. Bedtime H2 blockers improve nocturnal gastric acid control in GERD patients on proton pump inhibitors. Aliment Pharmacol. Ther. 15(9), 1351–1356 (2001).
Kim, E. H. et al. Efficacy of Lafutidine Versus Famotidine in Patients with Reflux Esophagitis: A Multi-Center, Randomized, Double-Blind, Non-inferiority Phase III Trial. Dig. Dis. Sci. 60(6), 1724–1732 (2015).
Ohara, S., Haruma, K., Kinoshita, Y. & Kusano, M. A double-blind, controlled study comparing lafutidine with placebo and famotidine in Japanese patients with mild reflux esophagitis. J. Gastroenterol. 45(12), 1219–1227 (2010).
Kahrilas PJ, Bredenoord AJ, Fox M, et al. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil. 27(2):160–174. (2015).
Jung, H. K. et al. 2020 Seoul Consensus on the Diagnosis and Management of Gastroesophageal Reflux Disease. J. Neurogastroenterol Motil. 27(4), 453–481 (2021).
Gyawali CP, Yadlapati R, Fass R, et al. Updates to the modern diagnosis of GERD: Lyon consensus 2.0. Gut. 73(2):361–371. (2024).
McRorie, J. W., Kirby, J. A. & Miner, P. B. Histamine2-receptor antagonists: Rapid development of tachyphylaxis with repeat dosing. World J. Gastrointest Pharmacol. Ther. 5(2), 57–62 (2014).
Sakurai, Y. et al. Acid-inhibitory effects of vonoprazan 20 mg compared with esomeprazole 20 mg or rabeprazole 10 mg in healthy adult male subjects–a randomised open-label cross-over study. Aliment Pharmacol. Ther. 42(6), 719–730 (2015).
Suzuki, T. et al. Comparison of effect of an increased dosage of vonoprazan versus vonoprazan plus lafutidine on gastric acid inhibition and serum gastrin. Eur. J. Clin. Pharmacol. 74(1), 45–52 (2018).
Takeuchi, T. et al. Randomised trial of acid inhibition by vonoprazan 10/20 mg once daily vs rabeprazole 10/20 mg twice daily in healthy Japanese volunteers (SAMURAI pH study). Aliment Pharmacol. Ther. 51(5), 534–543 (2020).
Arai, J. et al. Association Between Vonoprazan and the Risk of Gastric Cancer After Helicobacter pylori Eradication. Clin. Gastroenterol. Hepatol. 22(6), 1217-1225.e6 (2024).
Patel, A. et al. AGA Clinical Practice Update on Integrating Potassium-Competitive Acid Blockers Into Clinical Practice: Expert Review. Gastroenterology 167(6), 1228–1238 (2024).
Ours, T. M., Fackler, W. K., Richter, J. E. & Vaezi, M. F. Nocturnal acid breakthrough: clinical significance and correlation with esophageal acid exposure. Am. J. Gastroenterol. 98(3), 545–550 (2003).
Ghoshal, U. C., Chourasia, D., Tripathi, S., Misra, A. & Singh, K. Relationship of severity of gastroesophageal reflux disease with gastric acid secretory profile and esophageal acid exposure during nocturnal acid breakthrough: a study using 24-h dual-channel pH-metry. Scand J. Gastroenterol. 43(6), 654–661 (2008).
Weigt, J., Kandulski, A., Büsch, F. & Malfertheiner, P. Nocturnal gastric acid breakthrough is not associated with night-time gastroesophageal reflux in GERD patients. Dig. Dis. 27(1), 68–73 (2009).
Karyampudi, A. et al. Esophageal Acidification During Nocturnal Acid-breakthrough with Ilaprazole Versus Omeprazole in Gastroesophageal Reflux Disease. J. Neurogastroenterol. Motil. 23(2), 208–217 (2017).
Rackoff, A. et al. Histamine-2 receptor antagonists at night improve gastroesophageal reflux disease symptoms for patients on proton pump inhibitor therapy. Dis. Esophagus. 18(6), 370–373 (2005).
Schuitenmaker, J. M., Kuipers, T., Smout, A. J. P. M., Fockens, P. & Bredenoord, A. J. Systematic review: Clinical effectiveness of interventions for the treatment of nocturnal gastroesophageal reflux. Neurogastroenterol. Motil. 34(12), e14385 (2022).
Cho, K. et al. A randomized trial to evaluate the preventive effect of lafutidine on chemotherapy-induced peripheral neuropathy in patients treated with carboplatin and paclitaxel for lung cancer. Ann. Palliat Med. 12(6), 1136–1145 (2023).
Numazaki, M. et al. Structural determinant of TRPV1 desensitization interacts with calmodulin. Proc. Natl. Acad. Sci. U S A. 100(13), 8002–8006 (2003).
Liu, L. & Tian, Y. Capsaicin Changes the Pattern of Brain Rhythms in Sleeping Rats. Molecules 28(12), 4736 (2023).
Funding
This study was funded by National Natural Science Foundation of China (No. 92268108) and the Natural Science Foundation of Hubei Province (No. 2023AFB807).
Author information
Authors and Affiliations
Contributions
Dongke Wang: Conceptualized and designed the study, supervised the overall project, and contributed to manuscript writing. Ruohang He: Co-designed the study, coordinated participant recruitment and data collection, and contributed to the manuscript writing. Chaofan Duan: Conducted statistical analyses, interpreted the data, and drafted the methods and results sections of the manuscript. Xiaohao Zhang: Assisted with participant recruitment and data collection, and contributed to the discussion section of the manuscript. Tao Bai: Provided clinical expertise, oversaw the medical aspects of the study, and reviewed the manuscript for clinical accuracy. Junying Xu: Coordinated the logistics of the study, managed the database, and contributed to the final editing of the manuscript. Xuelian Xiang: Conducted literature reviews, assisted with data analysis, and contributed to the final approval of the manuscript. Xiaohua Hou: Supervised the overall project, managed study materials, and contributed to the final proofreading of the manuscript. All authors contributed to the interpretation of the results, reviewed the manuscript for intellectual content, and approved the final version for submission.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, D., He, R., Zhang, X. et al. Addition of bedtime lafutidine inhibits nocturnal acid-breakthrough and improves sleep quality in gastroesophageal reflux disease patients on esomeprazole: a randomized controlled trial. Sci Rep 15, 23286 (2025). https://doi.org/10.1038/s41598-025-06767-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-06767-3
