
Abstract
Most victims of childhood maltreatment have experienced more than one form. Yet, few studies have investigated co-occurrence of multiple childhood maltreatment subtypes (including physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect) using person-centered approaches in Chinese adolescents. Moreover, little is known about associations between different childhood maltreatment subtypes and smartphone addiction. This study aims to examine the specific effects of different childhood maltreatment patterns on smartphone addiction and the potential gender and residence differences. A multistage cluster sampling was adopted for Chinese adolescents aged 12 to 18 years across five representative provinces. The Childhood Trauma Questionnaire-Short Form was used to measure childhood maltreatment subtypes and Mobile phone Addiction Index was used to assess smartphone addiction. Childhood maltreatment patterns were analyzed via latent profile analysis (LPA) in Mplus. Of 23,478 Chinese adolescents, LPA yielded four distinct childhood maltreatment profiles: Low Maltreatment (Profile 1, 86.7%), High Emotional Maltreatment and Low Sexual Abuse (Profile 2, 9.2%), Moderate Multiple Maltreatment (Profile 3, 3.5%), and High Sexual Abuse with Multiple Maltreatment (Profile 4, 0.6%). Logistic regression analysis showed that members of Profile 2, 3, and 4 had higher odds ratio of smartphone addiction than members of Profile 1 (p < .01). Subgroup analysis indicated that members of Profile 4 had a higher odds ratio of smartphone addiction only for boys and rural adolescents (p < .01).. Childhood maltreatment subtypes rarely occur in isolation, and exposure to multiple childhood maltreatment subtypes will increase the risk of smartphone addiction. Particularly, boys and rural adolescents may deserve more attention in preventive strategy.
Similar content being viewed by others

Introduction
Nowadays, smartphone has become an essential tool for people of all ages or even an “intimate partner” in our daily life1,2,3. The amount of smartphone users has reached more than 5 billion around the world and this number will dramatically increase in the coming years4. In China, there were over 1028 million smartphone users in 2021, and 13.3% of them were young population aged from 10 to 19 years old5. Youths are more attracted to the newest electronic technology than the older ones, and smartphones have many functions and features that largely appeal to children and adolescents4,6. Simultaneously, smartphone addiction in adolescents has become an emerging public health issue across the world7,8,9,10,11. Smartphone addiction, commonly termed problematic smartphone use, is characterized by impaired self-regulation of smartphone use, manifesting addictive symptoms analogous to substance use disorders12,13. The prevalence of smartphone addiction among Chinese adolescents has been estimated to be 28–30%14,15,16, and the prevalence rate is still increasing with fast growth8,17. Therefore, it is urgent to explore the precursors and risk factors of smartphone addiction, which has great practical significance for targeted interventions of adolescents’ smartphone addiction.
Association between childhood maltreatment and smartphone addiction
Prior research has revealed that many individual factors (e.g., age and gender) and environmental factors (e.g., family atmosphere and adverse life events) may be the antecedents of smartphone addiction10,18,19,20. Among these factors, an emerging number of studies have supported that childhood maltreatment (CM) is a critical predictive factor of adolescents’ smartphone addiction20,21,22,23. CM is a public health issue worldwide and is typically defined as any action of commission or omission by parents or other caregivers that brings direct or indirect harm, which generally encompasses five core subtypes: physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect24.
According to attachment theory proposed by Bowlby and Ainsworth, stable and enduring emotional bonds between individuals and their caregivers during early life exert profound long-term impacts on subsequent development25. Childhood maltreatment, as a typical adverse family environment, disrupts healthy development through traumatic experiences such as caregiver neglect or abuse, which foster insecure attachment styles. Empirical studies have substantiated that compromised attachment quality predisposes individuals to problematic and addictive behaviors. As a new type of addictive behavior, smartphone addiction has also been found to be associated with childhood maltreatment in studies26,27. Geng et al. found that prior CM experiences significantly predicted adolescents’ subsequent smartphone addiction based on a longitudinal study of 890 students in two senior high schools of Eastern China14. Xiang et al. employed a structural equation model to demonstrate that CM has direct and indirect effects on smartphone addiction with a mediating role of core self-evaluation among 1951 Chinese students in four primary and high schools22. Moreover, Ma et al. recruited 981 students in two junior high schools of Guangdong Province, China, to indicate that CM affects adolescents’ smartphone addiction directly and indirectly via loneliness21. For different subtypes of CM, emotional maltreatment1,28,29 and parental neglect26,30 are risk factors of smartphone addiction in several previous studies. Additionally, General Strain Theory posits that adolescents adopt various delinquent behaviors to cope with or alleviate strains and pressures stemming from family neglect31. Smartphone addiction, as one such problematic behavior, may serve as a mechanism through which adolescents use excessive smartphone engagement to mitigate stress caused by adverse family experiences. This pathway could explain how childhood maltreatment contributes to the development of smartphone addiction among adolescents.
However, existing studies exhibit limitations in comprehensively examining childhood maltreatment subtypes: some have focused on only a limited subset of subtypes (e.g., physical/emotional abuse), while others have treated all five subtypes as a single aggregate score, potentially obscuring their distinct associations. Since different CM subtypes would exert distinct and nonequivalent impact on the physical and psychological development of adolescents21,32,33. Therefore, a key research question should be answered: whether all five core subtypes of CM have a significant association with adolescents’ smartphone addiction? The answers will help a lot for developing targeted prevention programs for smartphone addiction.
The co-occurring of childhood maltreatment subtypes
Although prior work has examined the relationship between some forms of CM and smartphone addiction, most studies have only examined the independent effects of abuse or neglect28,29,30. Given the extensive overlap between different subtypes of CM experiences, to date, many researchers support that co-occurrence of CM subtypes should be considered when assessing the effect of CM on mental and behavioral problems34,35,36. In general, most victims of CM suffer from more than one subtype in reality. In other words, it can be concluded that different subtypes of CM co-occur frequently35,37. Some empirical studies have compiled the number of subtypes of CM in an additive risk score and found that a higher number of subtypes of CM are associated with adverse health outcomes38,39. However, this approach assume that different subtypes are equally important for a specific health problem and does not consider possible interactional effects of various CM subtypes33. Apparently, this assumption is inconsistent with reality and has been opposed by more and more scholars recently32,40. Considering that CM subtypes are complicated and overlapped41,42revealing the disclosing patterns of CM experiences is promising and profound to understand resources of adolescents’ mental and behavioral problems, which can also benefit decision-makers for taking targeted and specific interventions34.
A promising methodological approaches for investigating co-occurrence and underlying interaction of different CM subtypes is person-centered approaches, such as latent profile analysis (LPA) and latent class analysis (LCA)35. There are several merits of person-centered approaches to address the issue. First, person-centered approaches enable identifying different classes of CM profiles rather than driving a predefined classification pattern that may not appropriate for a given sample43. Contrary to variable-centered modeling approaches, person-centered approaches can recognize and categorize “hidden” subgroups of people with a certain pattern of CM subtypes35. Second, person-centered approaches allow for different patterns at all CM subtype, thus could provide new perspectives about how different CM subtypes interact with each other36. Third, person-centered approaches can greatly benefit clinical practices for prioritizing treatments and interventions for individuals who report the most CM experiences since it can reveal the proportion and impact of different CM combinations44. Therefore, more and more scholars support adopting people-centered statistical techniques to deal with co-occurring CM subtypes and its potential detrimental influence34,36,37.
If indeed the co-occurrence of different CM subtypes is the rule rather than an exception, more research and clinical assessment should therefore consider all five subtypes of CM, including physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect. Several recent studies have used LPA or LCA (LPA is generally for multiple continuous variables while LCA is for multiple categorical variables) to empirically identify distinct groups of individuals who share similar experiences of abuse and neglect via the most wide-utilized scale globally: The Childhood Trauma Questionnaire—Short Form (CTQ-SF). For example, Zhang et al. uncovered two patterns of CM, “No Maltreatment” (89.3%) and “Multiple Maltreatment” (10.7%), via LPA among 9071 high school students in Chongqing City, China36. Niu et al. revealed four unique CM profiles: “Low Maltreatment” (76%), “Moderate Emotional Neglect Only” (15%), “Severe Physical and Emotional Abuse” (3%), and “Severe Sexual Abuse” (6%) among 882 sexually active girls in the United States34. Similarly, Zhang et al. revealed four distinct profiles of CM: “Minimal Maltreatment” (61.5%), “Low Abuse and High Neglect” (26.6%), “High Sexual Abuse with Multiple Maltreatment” (4%), and “High Physical and Emotional Maltreatment” (7.8%) among 1011 incarcerated Chinese male45. However, there is still few studies explored maltreatment profiles based on all five major subtypes of CM in a large-size sample of Chinese adolescents36. Furthermore, to date, none of previous studies has estimated the association between co-occurrence of CM subtypes and smartphone addiction.
The potential moderating roles of gender and residence
In addition to CM, existing literature also suggests that gender may be an influencing factor of smartphone addiction9,16,18. For example, some previous studies have demonstrated that girls are more likely to have smartphone addiction while boys have more tendency to Internet addiction11,46. For function of smartphone use, girls are more likely to overuse their smartphones for communication applications, while male commonly overuse smartphones for entertainment purposes, such as online games and videos47. However, Okasha et al. found that the prevalence of smartphone addiction has no significant difference between male and female in Egyptian youths10. Therefore, it is still necessary to compare the risk odds of smartphone addiction across different gender in different populations. Meanwhile, there is no prior work to explore whether there is gender difference in association between CM and smartphone addiction. Similarly, another important covariate, such as residence, has also scarcely been concerned. To date, little is known about the incidence of smartphone addiction and its risk factors between urban and rural areas of China. This detailed information will help decision-makers to find high-risk population and take targeted and efficient intervention of smartphone addiction. Thus, the underlying moderating roles of gender and residence are supposed to be considered when we examining the relationship between CM and smartphone addiction.
The present study
Taken together, some limitations in prior studies could be addressed. First, there is a dearth of studies on co-occurrence of five CM subtypes, including physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect. Second, there is a small-size or non-random sample in the previous studies and the findings might be hard to generalize for population across the whole country14,28,36. Third, gender difference and residence difference in the relationship between CM and smartphone addiction are still unknown. Therefore, the cross-sectional study was conducted in a large-size sample from five representative provinces across China. There are three aims in the current study: First, to identify CM patterns among Chinese adolescents using LPA based on five CM subtypes; Second, to examine how different CM profiles predict adolescents’ smartphone addiction; Third, to explore whether association between CM and smartphone addiction differs between boys and girls or between urban and rural adolescents.
Method
Procedure and participant
A multi-stage cluster sampling method was conducted in the cross-sectional study. Five stages of sampling were conducted from April to December 2021 in mainland of China. In Stage 1, China was divided into five main geographic locations (eastern, southern, western, northern, and central regions). Five representative provinces (Jiangsu, Guangdong, Yunnan, Gansu, and Hubei) were randomly selected from each region. In Stage 2, two cities were chosen randomly in each selected province. In Stage 3, we selected one district in an urban area and one county in a rural area from each selected city. In Stage 4, one junior high school and one senior high school were selected randomly in each sample district or county. In Stage 5, we used random digits to choose four or six classes from every grade (7th to 12th) in each selected school based on enrollment size. Finally, we invited all students in the selected class to participate in this survey voluntarily48. The study procedures were carried out in accordance with the Declaration of Helsinki. The personally identifiable information of all participating students was anonymized using de-identification techniques, with student names and ID numbers replaced by unique random codes. All investigators involved in the survey are legally and ethically bound to maintain strict confidentiality of collected personal information, explicitly pledging non-disclosure of any participant-related data to third parties. Access to raw data is exclusively granted to the principal investigator and authorized statistical analysis team members. This study obtained informed consent from schools, teachers, students, and their guardians, and was approved by the Medical Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (2021-A216).
Group administration was conducted by class unit, with each class supervised by one teacher and a uniformly trained research team member who consistently followed the same procedures to ensure students independently completed the questionnaires. Prior to the survey, all instructors and investigators received uniform training. During implementation, investigators strictly avoided using any leading language. Upon completion, the questionnaires were collected by investigators and checked for completeness.
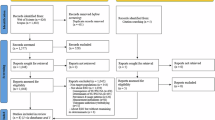
Of 25,779 respondents who sent back the questionnaire and provided the consent form, 2092 were excluded due to the age was more than 18 or less than 12 years old. During data cleaning, 209 participants were excluded because questionnaires with > 15% missing data were deemed insufficient for reliable analysis. For the remaining datasets with incomplete responses (i.e., ≤ 15% missing items within the full questionnaire), missing values were addressed through a simple imputation approach: median imputation was applied to skewed continuous variables (e.g., age), and mode imputation was used for categorical variables (e.g., household income, parental education level). Finally, 23,478 participants’ questionnaires were qualified in the data analysis, and the actual valid response rate of the current study was 91.07% (23,478/25,779).
Measurement
A custom-designed questionnaire was designed to collect demographic characteristics, childhood maltreatment experiences, smartphone addiction, and other related information. Previous studies have demonstrated that the following demographic factors are associated with smartphone addiction and thus were included as confounding variables in the study: gender (boys or girls), residence (urban or rural areas), age (in years), school type (junior or senior), family construction (living in a family with two biological parents, one biological parent, or others), father and mother’s education level (primary school or less, junior high school, senior high school, and college or more), family income (average family income per month in RMB, more than 8000, 6000–8000, 4000–5999, 2000–3999, and less than 2000). Screen duration (average duration per day in using an electronic screen, less than 30 min, 30–60 min, 61–120 min, and more than 120 min). Physical activity duration (average duration per day in physical activity, less than 30 min, 30–60 min, and more than 60 min)23,49,50,51,52.
The Childhood Trauma Questionnaire—Short Form (CTQ-SF) was administered to measure participants’ experiences of childhood maltreatment subtypes24. The CTQ-SF consists of 25 clinical items for five subscales: physical abuse, physical neglect, emotional abuse, emotional neglect, and sexual abuse. Each item was rated on a 5-point Likert scale from 1 = never true to 5 = very often. Therefore, the score of each subscale ranged from 5 to 25, and higher scores indicate more severe experiences of each CM subtype. The Cronbach’s alpha coefficient of the CTQ-SF in the current study was 0.851.
The Mobile phone Addiction Index (MPAI) was used to assess smartphone addiction29,53. The MPAI consists of 17 items and each item is scored on a 5-point Likert scale from 1 = never to 5 = always. The total score of MPAI ranged from 17 to 85. A higher score reveals a greater severity of smartphone addiction. In addition, according to Young’s recommendation, Items 3, 4, 5, 6, 8, 9, 14, and 15 could be used to screen smartphone addiction, which are equivalent to the 8-item Young’s Internet addiction diagnostic scale53. If the participants responded to 5 or more items with a score of 3 to 5, they were considered to have smartphone addiction (1 = yes)54. The others were treated as having no smartphone addiction (0 = no). The Cronbach’s α coefficient of MPAI was 0.888 in this study.
Statistical analysis
First, demographic characteristics of participants and the prevalence of smartphone addiction were described by descriptive statistics [n (%)]. The scores of CM subtypes and age were depicted by mean (SD). Second, the chi-square test was used to compare the prevalence of smartphone addiction across different categories. ANOVA was used to compare the means between participants with and without smartphone addiction.
Second, we used Latent profile analysis in Mplus 8.3 to characterize co-occurrence of five CM subtypes and to classify groups of participants with similar patterns. A set of models was fitted sequentially estimating 2 to 5 profiles. The best-fitting model was selected based on the criteria including Log-likelihood test, Akaike’s Information Criteria (AIC), Bayesian Information Criteria (BIC) and adjusted Bayesian Information Criteria (a-BIC), Entropy, Lo-Mendell-Rubin Likelihood Ratio Test (LMRT), and Bootstrap Likelihood Ratio Test (BLRT)55. Specifically, smaller absolute values of Log-likelihood, AIC, BIC, and a-BIC indicate better model fit. Significant p values of LMRT and BLRT indicate that the k class model fits better than k-1 class model. An Entropy value closer to 1 (more than 0.8 was accepted in common) indicates clearer classification between LPA56. After identifying the most optimal model, participants were classified into profile groups of a categorical variable36.
Third, to assess association between co-occurrence of childhood maltreatment subtypes and smartphone addiction, several models of Binary logistic regression analysis for smartphone addiction (0 = No, 1 = Yes) were conducted in SPSS 26.0 to estimate odds ratios (ORs) and 95% confidence intervals (95% CIs). The independent variable was profiles of the best model from LPA. Besides, to further examine the moderating role of gender and residence in the association, we conducted subgroup analyses between boys and girls, urban and rural participants, separately. In all models, we included age, high school type, family construction, father and mother’s education level, family income, screen duration, and physical activity duration as covariates. The significance level was set at p < .05 and all tests were two-sided.
Results
Characteristics of participants
Among 23,478 participants, the proportion of boys and girls were almost equal (50.4% vs. 49.6%), urban adolescents were slightly more than rural adolescents (55.1% vs. 44.9%). The mean (SD) of age was 15.00 (1.63). More than one third (37.1%) of participants spent an average of over 60 min per day using electronic screens. Only 17.4% of adolescents spent more than one hour/day on physical activity. The prevalence of smartphone addiction was 25.9% (6077/23,478). The prevalence in girls was higher than boys (27.9% vs. 23.9%, p < .001), and rural adolescents was higher than urban adolescents (28.9% vs. 23.4%, p < .001). Participants with smartphone addiction had higher scores of five childhood maltreatment (CM) subtypes than participants without smartphone addiction (p < .001). More information was presented in Table 1.
Latent profile analysis of five childhood maltreatment subtypes
A series of 2- to 5-latent profile models were estimated based on all five CM subtypes (Table 2). The LMRT statistic suggested that the 4- profile model was significantly better than the 3- profile model (p = .043), but the 5- profile model was not significantly better than the 4- profile model (p = .305). The p values of the BLRT were all less than 0.001. The entropy values were high and more than 0.90 in all the solutions. After considered fit indices and practical interpretation, the 4-profile solution was chosen as the optimal solution.
The latent indicator means for the 4-profile solution are depicted in Fig. 1. Profile 1 (n = 20,365, 86.7%) was defined by none or low level of CM subtypes, which was labeled as the “Low Maltreatment” group. Profile 2 (n = 2155, 9.2%) was characterized by high level of emotional abuse and neglect, moderate level of physical abuse and neglect, and low level of sexual abuse, which was labeled as the “High Emotional Maltreatment and Low Sexual Abuse” group. Profile 3 (n = 823, 3.5%) was defined by moderate level of all five CM subtypes, which was labeled as the “Moderate Multiple Maltreatment” group. Profile 4 (n = 135, 0.6%) was characterized by high level of all CM subtypes, especially for sexual abuse, which was labeled as the “High Sexual Abuse with Multiple Maltreatment” group. An ANOVA was conducted to assess intergroup differences among the four conditions, revealing statistically significant variation (F = 11.844, p < .001).

Profiles of five childhood maltreatment subtypes for the four-class solution.
In addition, girls had higher proportion in Profile 2 than boys (57.6% vs. 42.4%), while boys had higher proportion in Profile 3 (63.3% vs. 36.7%) and Profile 4 (77.0% vs. 23.0%) than girls. Urban adolescents had higher proportion in Profile 2 than rural adolescents (54.3% vs. 45.7%), while rural adolescents had higher proportion in Profile 3 than urban adolescents (56.4% vs. 43.6%) (Table 3).
Association between profiles of childhood maltreatment and smartphone addiction
The prevalence of smartphone addiction differed between four groups of CM profiles (p < .001) (Table 3). In pairwise comparison, participants of Profile 2 had the highest prevalence of smartphone addiction (41.9%) and participants of Profile 1 had the lowest (23.6%). The difference of prevalence between Profile 3 (37.3%) and Profile 4 (37.8%) was not significant (p > .05).
Subgroup analysis by gender and urban-rural disparities
Results of the binary logistic regression analysis for smartphone addiction presents in Table 4. Compared to participants in Low Maltreatment, participants in High Emotional Maltreatment and Low Sexual Abuse (OR = 2.191, 95% CI 1.988–2.415, p < .001), Moderate Multiple Maltreatment (OR = 1.783, 95% CI 1.530–2.078, p < .001), and High Sexual Abuse with Multiple Maltreatment (OR = 1.902, 95% CI 1.316–2.748, p < .01) had higher odds ratio of smartphone addiction. girls had higher odds ratio (OR = 1.175, 95% CI 1.102–1.253, p < .001) than boys. Rural participants had higher odds ratio (OR = 1.202, 95% CI 1.125–1.284, p < .001) than urban counterparts. Besides, screen duration, physical activity duration, age, high school type, family construction, father’s and mother’s education were significantly associated with smartphone addiction. In subgroup analysis, boys in High Sexual Abuse with Multiple Maltreatment had higher odds ratio (OR = 1.910, 95% CI 1.257–2.902, p < .01) than boys in Low Maltreatment. The association was not significant for girls (p > .05). Similarly, rural adolescents in High Sexual Abuse with Multiple Maltreatment had higher odds ratio (OR = 2.286, 95% CI 1.382–3.782, p < .01) than rural adolescents in Low Maltreatment. The association was not significant for urban adolescents (p > .05).
Discussion
This study is the first to examine the association between smartphone addiction and the co-occurrence of five core childhood maltreatment subtypes in a large sample of Chinese adolescents. There are several major and new findings. First, four distinct CM profiles are identified based on LPA, and victims of maltreatment almost experience multiple subtypes concurrently rather than a single form. Second, compared to adolescents in profile of Low Maltreatment, adolescents in profile of High Emotional Maltreatment and Low Sexual Abuse, Moderate Multiple Maltreatment, and High Sexual Abuse with Multiple Maltreatment have greater risks of smartphone addiction. Third, associations between CM profiles and smartphone addiction differ by gender and residence. Specifically, only boys and rural adolescents in profile of High Sexual Abuse with Multiple Maltreatment are more likely to report smartphone addiction. These findings advance the literature in this field and provide an innovative perspective in development of adolescents’ addictive behaviors. More importantly, it will benefit medical personnel for screening risk population of smartphone addiction and help policy-makers making targeted preventive strategy for smartphone addiction.
Profiles of childhood maltreatment
Similar to some previous studies34,57we identified four maltreatment profiles based on five CM subtypes. The largest proportion of the sample was classified into the Low Maltreatment profile (86.7%), followed by High Emotional Maltreatment and Low Sexual Abuse (9.2%), Moderate Multiple Maltreatment (3.5%), and High Sexual Abuse with Multiple Maltreatment (0.6%). Although the proportion of High Sexual Abuse with Multiple Maltreatment is less than 1%, we still include this profile in subsequent analysis because the sample size is very large and the number of the profile is 135 in the study. On the other hand, according to the fit indices of LPA, four-profile is the optimal solution and better than three- or two-profile solution. Consistent with prior research37,42,43,58different subtypes of CM often co-occur. In other words, victims of maltreatment almost experience a combination of multiple abuse and neglect in reality. In our sample, except for members of Low Maltreatment, the remaining participants almost all report more than one subtype of CM.
It is interesting to notice that sexual abuse can hardly occur in isolation. According to the four profiles of maltreatment in the study, some subtypes (e.g. emotional abuse) can occur without sexual abuse, but sexual abuse may not occur without other forms of maltreatment. According to psychosocial theories59sexual abuse is featured by negative emotions, which stem from physical exploitation, cognitive stigmatization, and social isolation60. Besides, according to biological theories61sexual abuse may cause dysregulation of the Hypothalamic-Pituitary-Adrenocortical axis (HPA), which will constrain the development of cognitive, emotional, and relational skills. For example, victims of sexual abuse may have difficulty to construct intimate relationships and be prone to have a lower self-concept and self-esteem in social exploration and development. Eventually, they are more likely to be victims of other forms of abuse and neglect34.
However, another recent study conducted in Chinese adolescents did not discover unique co-occurrences of CM subtypes beyond the two profiles labeled “No Maltreatment” and “Multiple Maltreatment”36. Particularly, this study did not discover a profile dominated by sexual abuse. The possible reason of the inconsistent findings could be distinct measurement methods and cut-off values of the CTQ-SF in different studies. For example, Zhang et al. categorized each subtype of CM into four levels based on cut-off scores recommended by Bernstein24which including none, low, moderate, and severe. Then, LPA was used for the four categories of five subtypes36. First, whether LPA is suitable and valid for multiple categorical variables is debatable and deserves further discussion. Second, more and more scholars support that the cut-off values recommended by Bernstein are not universal for different population across the world, such as Chinese adolescents48. Therefore, to avoid potential risk of misclassification of severity of five CM subtypes, we included raw scores of the CTQ-SF in LPA in the current study. Another possible explanation may be different sample representativeness. Zhang et al. recruited 9027 participants from three high schools in Chongqing City36while we included 23,478 students from 40 schools across five representative provinces of China. In a word, the disagreement of CM patterns in different studies also suggests that sexual abuse is a unique subtype of CM and should be included as an important indicator when investigating or evaluating specific forms of maltreatment experiences33,42,45.
Associations between childhood maltreatment and smartphone addiction
Our findings highlight the critical role of CM profiles in smartphone addiction among adolescents, which will benefit for targeted interventions to effectively address smartphone addiction in different groups of early maltreatment experiences. Overall, profile reflecting high levels of emotional maltreatment might be more strongly associated with smartphone addiction than other profiles of CM. Emotional maltreatment refers to the harmful and inappropriate parenting behaviors of caregivers, which does not involve physical and sexual contact62. Emotional maltreatment has long-term impacts on individual’s psychological health and social development63. According to interpersonal theory, positive parent-child relationships are linked to individuals’ good interpersonal relationships with others. In contrast, negative and poor parent-child relationships, such as emotional abuse and neglect, can be inferred to weaken one’s social ability face to face and increase the risk odds of smartphone addiction since the major function and purpose of smartphone use is interpersonal communication in virtual world29,64. From this perspective, smartphone addiction could serve as a compensatory response for those victims to handle undesirable interpersonal relationships in reality. Therefore, individuals with high levels of emotional maltreatment may use their smartphones excessively to maintain affective identification online and obtain support from friends, which can further lead to smartphone addiction1,30.
According to existing literature, it is still unknown about the relationship between sexual abuse and smartphone addiction. The possible reason may due to statistical problems related to unidirectional redundancy, which stem from a small sample size and lower incidence of sexual abuse compared to other subtypes of abuse and neglect65. In the current study, we are able to estimate the risk odd of smartphone addiction in distinct CM profiles based on a large-size sample of adolescents, particularly in profiles for presence or absence of sexual abuse. Our results revealed that profiles with and without sexual abuse are all associated with elevated odds of smartphone addiction. This finding may demonstrate that sexual abuse is not a sensitive and reasonable predictor of smartphone addiction. Given few previous studies concerning this issue, more future research is supposed to reveal the association between sexual abuse and smartphone addiction and explore the potential mechanism.
The moderating roles of gender and residence
In line with most previous studies9,11,46our results indicate that girls have greater risk of smartphone addiction than boys. Besides, we also find a significant gender difference in CM patterns. In general, girls report more emotional abuse and neglect while boys experience more sexual abuse and multiple maltreatment. This finding is incongruent with many existing studies conducted in Western countries42,66which believe girls are more likely to be victims of sexual abuse. Then, the results further reveal gender differences in association between CM and smartphone addiction. In specific, boys in High Sexual Abuse with Multiple Maltreatment are more likely to be smartphone addicts, but not for girls. Cultural values in China might prohibit victims from reporting their sexual abuse experiences, especially for Chinese girls. If girls disclose sexual abuse experience, their personal reputation and family grace can be damaged fatally. Under this cultural background, Chinese girls and their family members are prone to hide experiences of sexual abuse67. Therefore, the association between high level of sexual abuse and smartphone addiction may be weakened or concealed in Chinese girls.
To extend the existing literature in the field, our study first considers residence as an influencing factor of smartphone addiction. First, we find that rural teenagers have more tendency to smartphone addiction than urban teenagers. Second, we further find a moderating role of residence in the relationship between CM and smartphone addiction. Notably, rural adolescents in High Sexual Abuse with Multiple Maltreatment have increased risk of smartphone addiction, but not for urban adolescents. On the one hand, urban students generally have more academic pressure and admission competition than rural students in China. Therefore, urban students may have less chance and time to excessive smartphone use. On the other hand, although urban youths may have more access to smartphone use, their parents will supervise their use of smartphones more strictly. However, in rural China, many parents have to migrate to towns or other cities to work, and most left-behind children lack appropriate regulation and discipline68. In this slack circumstance, rural adolescents are more likely to rely on smartphone use.
Implications
Our findings could provide several valuable implications, both theoretically and clinically. First, this study suggests that adolescents with co-occurrence of multiple CM subtypes have greater risk of smartphone addiction, especially for emotional abuse and neglect. From a clinical perspective, for smartphone addicts, it is appropriate for mental health workers to investigate their history of multiple CM forms. For policy-makers, it is urgent to formulate prioritized interventions for victims of multiple CM forms, such as emotional abuse and emotional neglect, to reduce risk odds of addictive behaviors. Meanwhile, developing positive parenting skills and promoting parent-child attachment may be significantly effective in the treatment for adolescents addicted to smartphones36. Second, girls and rural adolescents are more likely to overuse smartphones and gender and residence play a moderating role in relationship between CM and smartphone addiction. On the one hand, targeted intervention for smartphone addiction should give priority to girls and adolescents in rural China. On the other hand, to prevent smartphone addiction for victims of maltreatment experiences, one-size-fits-all approach may be not promising for all high-risk population and strategies are supposed to be tailored by sex and residence. At the same time, scholars are encouraged to explore the potential mechanism about the effects of specific combinations of CM subtypes on smartphone addiction, and why the effects are distinct among population with different characteristics.
Limitations
Some limitations in the current study should be noted. First, the cross-sectional design of the current study does not allow us to draw a causal relationship between childhood maltreatment profiles and smartphone addiction, although smartphone addiction can hardly increase the risk odds of childhood maltreatment in reality. Future studies could benefit from a longitudinal design. Second, the self-report and retrospective character of the CTQ-SF may magnify reporting bias and recall bias. Although the CTQ-SF demonstrates good reliability and validity in many previous studies, participants may also under- or over-report their history of abuse and neglect as there is no ‘‘gold standard’’ to validate childhood maltreatment yet69. Future research could take multi-informant measurements (e.g., peer reports or official reports) to obtain some sensitive information, such as sexual abuse experiences. Third, although the fit indices of LPA in the study suggest that four-profile solution is the best pattern of five CM subtypes, the proportion of High Sexual Abuse with Multiple Maltreatment is less than 1%, which may weaken statistical power or increase the odds of statistical error. Therefore, our findings should be further verified based on other sample with different cultural backgrounds.
Conclusion
The current study provides a better understanding of the co-occurrence of five CM subtypes and their specific associations with smartphone addiction in a large-size sample of Chinese adolescents. Different forms of CM experiences tend to co-occur and almost no subtype happens in isolation. Four CM profiles have distinct effects on smartphone addiction and profiles with high levels of emotional abuse and neglect may be more detrimental. Moreover, these associations differ between boys and girls, as well as between urban and rural adolescents. Our findings suggest that specific combinations of abuse and neglect experiences should be included in psychiatric evaluations, especially for smartphone addicts. Meanwhile, intervention programs tailored by gender and residence may be more promising than adopting a generic one-size-fits-all strategy to prevent smartphone addiction. Particularly, more attention should be paid to girls and rural adolescents.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to the privacy of respondents but are available from the corresponding author on reasonable request.
References
Chen, Y. et al. Childhood emotional neglect and problematic mobile phone use among Chinese adolescents: A longitudinal moderated mediation model involving school engagement and sensation seeking. Child. Abuse Negl. 115, 104991 (2021).
Demirci, K., Akgönül, M. & Akpinar, A. Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J. Behav. Addict. 4, 85–92 (2015).
Huang, Q. et al. Suicidal ideation is associated with excessive smartphone use among Chinese college students. Front. Public. Health. 9, 809463 (2022).
Islam, M. Link between excessive smartphone use and sleeping disorders and depression among South Korean university students. Health Care (Don Mills). 9, 1213 (2021).
Gao, Q. et al. How different levels of mobile phone addiction relate to adolescent depressive symptoms: the mediating role of parent-adolescent relationships. J. Psychopathol. Behav. 44, 1099–1109 (2022).
Parasuraman, S., Sam, A. T., Yee, S. W. K., Chuon, B. L. C. & Ren, L. Y. Smartphone usage and increased risk of mobile phone addiction: A concurrent study. Int. J. Pharm. Investig. 7, 125 (2017).
Lee, J., Ahn, J. S., Min, S. & Kim, M. H. Psychological characteristics and addiction propensity according to content type of smartphone use. Int. J. Environ. Res. Public. Health. 17, 2292 (2020).
Liu, Q. Q. et al. Perceived stress and mobile phone addiction in Chinese adolescents: A moderated mediation model. Comput. Hum. Behav. 87, 247–253 (2018).
Nayak, J. K. Relationship among smartphone usage, addiction, academic performance and the moderating role of gender: A study of higher education students in India. Comput. Educ. 123, 164–173 (2018).
Okasha, T. et al. Prevalence of smartphone addiction and its correlates in a sample of Egyptian university students. Int. J. Soc. Psychiatr. 68, 1580–1588 (2021).
Smartphone addiction - ScienceDirect. https://www.sciencedirect.com/science/article/pii/B9780128186268000086.
Panova, T. & Carbonell, X. Is smartphone addiction really an addiction? J. Behav. Addict. 7, 252–259 (2018).
Yang, J., Fu, X., Liao, X. & Li, Y. Association of problematic smartphone use with poor sleep quality, depression, and anxiety: A systematic review and meta-analysis. Psychiat Res. 284, 112686 (2020).
Geng, J. et al. Does childhood maltreatment increase the subsequent risk of problematic smartphone use among adolescents? A two-wave longitudinal study. Addict. Behav. 129, 107250 (2022).
Tao, S. et al. Association of alcohol use with problematic mobile phone use and depressive symptoms among college students in anhui, China. J. Public. Health-uk. 25, 103–112 (2016).
Chen, B. et al. Gender differences in factors associated with smartphone addiction: a cross-sectional study among medical college students. BMC Psychiatry. 17, 341 (2017).
Li, D. et al. Interaction of health literacy and problematic mobile phone use and their impact on Non-Suicidal Self-Injury among Chinese adolescents. Int. J. Environ. Res. Public. Health. 16, 2366 (2019).
Busch, P. A. & McCarthy, S. Antecedents and consequences of problematic smartphone use: A systematic literature review of an emerging research area. Comput. Hum. Behav. 114, 106414 (2021).
Tymofiyeva, O. et al. Neural correlates of smartphone dependence in adolescents. Front. Hum. Neurosci. 14, 564629 (2020).
Zhao, C. et al. Longitudinal effects of stressful life events on problematic smartphone use and the mediating roles of mental health problems in Chinese undergraduate students. Front. Public. Health. 9, 752210 (2021).
Ma, S., Huang, Y. & Ma, Y. Childhood maltreatment and mobile phone addiction among Chinese adolescents: loneliness as a mediator and Self-Control as a moderator. Front. Psychol. 11, 813 (2020).
Xiang, Y., He, Q. & Yuan, R. Childhood maltreatment affects mobile phone addiction from the perspective of attachment theory. Int. J. Mental Health Addict. 21, 3536–3548 (2022).
Peng, J. et al. Physical and emotional abuse with internet addiction and anxiety as a mediator and physical activity as a moderator. Sci. Rep. 15, 2305 (2025).
Bernstein, D. P. et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child. Abuse Negl. 27, 169–190 (2003).
Slade, A. & Holmes, J. Attachment and psychotherapy. Curr. Opin. Psychol. 25, 152–156 (2019).
Kwak, J. Y., Kim, J. Y. & Yoon, Y. W. Effect of parental neglect on smartphone addiction in adolescents in South Korea. Child. Abuse Negl. 77, 75–84 (2018).
Hagborg, J. M., Tidefors, I. & Fahlke, C. Gender differences in the association between emotional maltreatment with mental, emotional, and behavioral problems in Swedish adolescents. Child. Abuse Negl. 67, 249–259 (2017).
Emirtekin, E. et al. The role of childhood emotional maltreatment and body image dissatisfaction in problematic smartphone use among adolescents. Psychiat Res. 271, 634–639 (2019).
Liu, F., Zhang, Z. & Chen, L. Mediating effect of neuroticism and negative coping style in relation to childhood psychological maltreatment and smartphone addiction among college students in China. Child. Abuse Negl. 106, 104531 (2020).
Sun, J., Liu, Q. & Yu, S. Child neglect, psychological abuse and smartphone addiction among Chinese adolescents: the roles of emotional intelligence and coping style. Comput. Hum. Behav. 90, 74–83 (2019).
Agnew, R. Foundation for a generalism strain theory of crime and delinquency. Criminology 30, 47 (1992).
Angelakis, I., Austin, J. L. & Gooding, P. Association of childhood maltreatment with suicide behaviors among young people: A systematic review and Meta-analysis. JAMA Netw. Open. 3, e2012563 (2020).
Vachon, D. D., Krueger, R. F., Rogosch, F. A. & Cicchetti, D. Assessment of the harmful psychiatric and behavioral effects of different forms of child maltreatment. JAMA Psychiatry. 72, 1135 (2015).
Niu, L. et al. Profiles of childhood maltreatment: associations with sexual risk behavior during adolescence in a sample of racial/ethnic minority girls. Child. Dev. 92, 1421–1438 (2021).
O’Donnell, M. L. et al. A systematic review of person-centered approaches to investigating patterns of trauma exposure. Clin. Psychol. Rev. 57, 208–225 (2017).
Zhang, Y., Liao, H., Gu, J. & Wang, J. Anxiety and depression related to childhood maltreatment in teenagers: comparing multiple individual risk model, cumulative risk model and latent profile analysis. Child. Abuse Negl. 128, 105630 (2022).
Debowska, A., Willmott, D., Boduszek, D. & Jones, A. D. What do we know about child abuse and neglect patterns of co-occurrence? A systematic review of profiling studies and recommendations for future research. Child. Abuse Negl. 70, 100–111 (2017).
Wan, Y. et al. Associations of adverse childhood experiences and social support with self-injurious behaviour and suicidality in adolescents. Brit J. Psychiat. 214, 146–152 (2018).
Xiao, D. et al. Gender differences in the associations between types of childhood maltreatment and sleep disturbance among Chinese adolescents. J. Affect. Disorders. 265, 595–602 (2020).
Kang, C. et al. Specific effects of neglect and physical abuse on adolescent aggressive behaviors by gender: A multicenter study in rural China. J. Affect. Disorders. 281, 271–278 (2021).
Angelakis, I., Gillespie, E. L. & Panagioti, M. Childhood maltreatment and adult suicidality: a comprehensive systematic review with meta-analysis. Psychol. Med. 49, 1057–1078 (2019).
Witt, A. et al. Experience by children and adolescents of more than one type of maltreatment: association of different classes of maltreatment profiles with clinical outcome variables. Child. Abuse Negl. 57, 1–11 (2016).
Warmingham, J. M., Handley, E. D., Rogosch, F. A., Manly, J. T. & Cicchetti, D. Identifying maltreatment subgroups with patterns of maltreatment subtype and chronicity: A latent class analysis approach. Child. Abuse Negl. 87, 28–39 (2019).
Lacey, R. E. & Minnis, H. Practitioner Review: Twenty years of research with adverse childhood experience scores - Advantages, disadvantages and applications to practice. J. Child. Psychol. Psyc. 61, 116–130 (2019).
Zhang, J. & Zheng, Y. Childhood maltreatment profiles among incarcerated Chinese males and their associations with personality disorder symptoms and criminal behaviors. Psychiat Res. 268, 272–278 (2018).
Choi, S. W. et al. Comparison of risk and protective factors associated with smartphone addiction and internet addiction. J. Behav. Addict. 4, 308–314 (2015).
Lee, E. J. & Kim, H. S. Gender differences in smartphone addiction behaviors associated with Parent-Child bonding, Parent-Child communication, and parental mediation among Korean elementary school students. J. Addict. Nurs. 29, 244–254 (2018).
Peng, C., Cheng, J., Rong, F., Wang, Y. & Yu, Y. Psychometric properties and normative data of the childhood trauma questionnaire-short form in Chinese adolescents. Front. Psychol. 14, 1130683 (2023).
Long, J. et al. Prevalence and correlates of problematic smartphone use in a large random sample of Chinese undergraduates. BMC Psychiatry. 16, 408 (2016).
Beison, A. & Rademacher, D. J. Relationship between family history of alcohol addiction, parents’ education level, and smartphone problem use scale scores. J. Behav. Addict. 6, 84–91 (2016).
Bianchi, A. & Phillips, J. G. Psychological predictors of problem mobile phone use. Cyberpsychol Behav. 8, 39–51 (2005).
Lee, C. & Lee, S. J. Prevalence and predictors of smartphone addiction proneness among Korean adolescents. Child. Youth Serv. Rev. 77, 10–17 (2017).
Leung, L. Linking psychological attributes to addiction and improper use of & the mobile phone among adolescents in Hong Kong. J. Child. Media 2, 93–113 (2008).
Shi, M., Zhai, X., Li, S., Shi, Y. & Fan, X. The relationship between physical activity, mobile phone addiction, and irrational procrastination in Chinese college students. Int. J. Environ. Res. Public. Health. 18, 5325 (2021).
Nylund, K. L., Asparouhov, T. & Muthen, B. O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study Struct. Equ. Model. 14, 535–569 (2007).
Tein, J. Y., Coxe, S. & Cham, H. Statistical power to detect the correct number of classes in latent profile analysis. Struct. Equ Model. 20, 640–657 (2013).
Guyon-Harris, K. L., Madigan, S., Bronfman, E., Romero, G. & Huth-Bocks, A. C. Prenatal identification of risk for later disrupted parenting behavior using latent profiles of childhood maltreatment. J. Interpers. Violence. 36, NP13517–NP13540 (2020).
Luk, J. W. et al. A latent class analysis of physical, emotional, and sexual abuse history among suicidal inpatients. J. Psychiatr Res. 142, 9–16 (2021).
Shaw, J. A., Lewis, J. E., Loeb, A., Rosado, J. & Rodriguez, R. A. Child on child sexual abuse: psychological perspectives. Child. Abuse Negl. 24, 1591–1600 (2000).
Ji, K., Finkelhor, D. & Dunne, M. Child sexual abuse in china: a meta-analysis of 27 studies. Child. Abuse Negl. 37, 613–622 (2013).
Koss, K. J. & Gunnar, M. R. Annual research review: early adversity, the hypothalamic-pituitary-adrenocortical axis, and child psychopathology. J. Child. Psychol. Psyc. 59, 327–346 (2017).
Glaser, D. Emotional abuse and neglect (psychological maltreatment): a conceptual framework. Child. Abuse Negl. 26, 697–714 (2002).
Arslan, G. Psychological maltreatment, forgiveness, mindfulness, and internet addiction among young adults: A study of mediation effect. Comput. Hum. Behav. 72, 57–66 (2017).
Arslan, G. Psychological maltreatment, emotional and behavioral problems in adolescents: the mediating role of resilience and self-esteem. Child. Abuse Negl. 52, 200–209 (2016).
Stein, M. B. et al. Childhood maltreatment and lifetime suicidal behaviors among new soldiers in the US army: results from the army study to assess risk and resilience in servicemembers (Army STARRS). J. Clin. Psychiat. 79, 70–77 (2018).
Radford, L., Corral, S., Bradley, C. & Fisher, H. L. The prevalence and impact of child maltreatment and other types of victimization in the UK: findings from a population survey of caregivers, children and young people and young adults. Child. Abuse Negl. 37, 801–813 (2013).
Stoltenborgh, M., van Ijzendoorn, M. H., Euser, E. M. & Bakermans-Kranenburg, M. J. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat. 16, 79–101 (2011).
Peng, C. et al. Association between internet addiction and suicidal ideation, suicide plans, and suicide attempts among Chinese adolescents with and without parental migration. Comput. Hum. Behav. 125, 106949 (2021).
Jiang, Y., Perry, D. K. & Hesser, J. E. Suicide patterns and association with predictors among Rhode Island public high school students: a latent class analysis. Am. J. Public. Health. 100, 1701–1707 (2010).
Acknowledgements
The authors thank students who took part in the survey, parents who supported the work, teachers who assisted with the field investigation, and all investigators.
Funding
This work was supported by the National Natural Science Foundation of China (Grant Number is 82173541, 82373599, and 82404288) and the Postdoctoral Fellowship Program of CPSF (Grant Number is GZC20242134). The funding body had no role in the design of the study and collection, analysis and interpretation of data or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
CP: Conceptualization, Formal analysis and Methodology, Funding acquisition, Investigation, Writing original draft. NZ: Formal analysis and Methodology, Investigation, Writing original draft, Writing - review & editing. JH: Investigation. FR: Investigation. JC: Writing - review & editing. MG: Visualization. ZX: Visualization. YY: Conceptualization, Funding acquisition, Supervision, Writing - review & editing. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peng, C., Zhang, N., Cheng, J. et al. Latent profile analysis of five childhood maltreatment subtypes and its associations with smartphone addiction among Chinese adolescents. Sci Rep 15, 21579 (2025). https://doi.org/10.1038/s41598-025-08139-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-08139-3
