
Abstract
This study aimed to investigate white matter microstructural changes in patients with cluster headaches using peak width of skeletonized mean diffusivity (PSMD) derived from diffusion tensor imaging (DTI). A total of 40 participants were recruited, comprising 20 patients with newly diagnosed cluster headaches and 20 healthy controls. DTI was conducted using a 3 Tesla MRI scanner. PSMD was quantified through a standardized multi-step process involving preprocessing, skeletonization, application of a custom mask, and histogram analysis performed with the FSL program. PSMD values were compared between the cluster headache group and the healthy controls, and correlation analyses were performed to examine association between PSMD and clinical factors. Patients with cluster headaches demonstrated significantly higher PSMD values than healthy controls (0.273 × 10⁻3 mm²/s vs. 0.227 × 10⁻3 mm²/s, p = 0.009). PSMD showed a positive correlation with age in the cluster headache group (r = 0.575, p = 0.008). However, there was no significant difference in PSMD between the hemisphere corresponding to the fisymptomatic side of the cluster headache and the contralateral hemisphere (0.270 × 10⁻3 mm²/s vs. 0.272 × 10⁻3 mm²/s, p = 0.909). This study demonstrates that patients with cluster headaches experience compromised white matter microstructural integrity, reflected by elevated PSMD values compared to healthy controls. The observed age-related increase in PSMD across both groups supports the role of aging in white matter microstructure. The lack of hemispheric differences in PSMD suggests that white matter alterations associated with cluster headaches are not confined to the symptomatic side, indicating a diffuse pattern of white matter involvement.
Similar content being viewed by others

Introduction
Cluster headache is a rare neurological disorder characterized by severe unilateral headache attackes accompanied by autonomic symptoms, which often response to oxygen thearpy1,2,3. The prevalence of cluster headache is approximately 0.1% in the general population1,2,3. Diagnosis is primarily clinical, as no definitive biomarker has been established. However, potential candidates include hypothalamic-regulated hormones such as cortisol, inflammatory markers like interleukin-1, and neuropeptides such as calcitonin gene-related peptide4.
Although the exact pathophysiology of cluster headaches remain unclear, advance in neuroimaging have provided valuable insights5,6. Conventional brain magnetic resonance imaging (MRI) typically shows no structural abnormalities; however, volumetric analyses using T1-weighted MRI have identified alterations in hypothalamic gray matter volumes5,6. For instance, increase hypothalamic gray matter volume has been observed bilaterally. Converssely, reductions in the hypothalamic small-worldness index have been reported via volume-based covariance network analysis7,8. Diffuse tensor imaging (DTI) studies have also revealed white matter microstructural abnormalities in multiple brain regions, including the brainstem, frontal, temporal, and occipital lobes, as well as thalamus and cerebellum9. Functional MRI studies have demonstrated activation in the hypothalamus, prefrontal cortex, thalamus, basal ganglia, insula, and cerebellar hemispheres during headache episodes10. These findings collectively suggest that cluster headache involves hypothalamic dysfunction and widespread disruptions in brain network connectivity.
The Peak Width of Skeletonized Mean Diffusivity (PSMD) is an emerging imaging biomarker with high sensitivity for detecting white matter integrity11,12. By quantifying the dispersion of mean diffusivity (MD) values along a white matter skeleton, PSMD captures subtle microstructural changes that may be missed by traditional DTI metrics. PSMD has been shown to correlate with aging, small vessel disease, and neurodegenerative disorders13,14. As a quantitative and objective measure, PSMD reduces subjectivity in analysis and ensures reliability in clinical and research contexts15. The method is highly reproducible, utilizing a standardized skeletonized approach that minimizes variability across studies and imaging centers11. PSMD also demonstrates a strong correlation with cognitive impairment, particularly in conditions related to small vessel disease, making it a valuable tool for monitoring cognitive health16,17. It is non-invasive and can be easily derived from DTI, a technique widely available in clinical MRI settings. The analysis process is also efficient, implying automated processing pipelines that reduce manual intervention and save time. PSMD is a powerful tool for advancing neurological research and care by providing a comprehensive assessment of white matter microstructure11. Despite its significant potential, no studies have yet investigated white matter changes in patients with cluster headaches using PSMD, leaving an important gap in the current literature.
This study aimed to investigate white matter microstructural changes in patients with cluster headaches using PSMD derived from DTI, compared to healthy controls. Additionally, we compared conventional DTI metrics, including fractional anisotropy (FA), MD, axial diffusivity (AD), and radial diffusivity (RD), differed between the two groups, to determine whether PSDM offers greater sensitivity or complementary information. By addressing this gap, the findings are expected to advance understanding the mechanisms underlying cluster headache pathophysiology and contribute to the broader field of neuroimaging biomarkers.
Results
Demographic and clinical characteristics of participants
Table 1 presents the demographic and clinical characteristics of patients with cluster headaches and healthy controls. There were no significant differences between the groups in terms of age (41.4 ± 16.3 years vs. 41.5 ± 16.5 years, p = 0.984) and sex distribution (85.0% male in both groups, p = 1.000).
Difference in PSMD between the groups
A significant difference in PSMD was observed between patients with cluster headaches and healthy controls. Patients with cluster headaches had significantly elevated PSMD values compared to healthy controls (0.273 × 10⁻ 3 mm²/s vs. 0.227 × 10⁻ 3 mm²/s, p = 0.009) (Fig. 1). However, there was no significant difference in PSMD values between the hemisphere corresponding to the side of symptomatic side and the contralateral hemisphere (0.270 × 10⁻ 3 mm²/s vs. 0.272 × 10⁻ 3 mm²/s, p = 0.909).

Comparison of PSMD between patients with cluster headache and healthy controls. The figure illustrates that patients with cluster headaches have significantly higher PSMD values compared to healthy controls (0.273 × 10⁻ 3 mm²/s vs. 0.227 × 10⁻ 3 mm²/s, p = 0.009). The unit of PSMD in the figure is x 10⁻ 3 mm²/s. PSMD peak width of skeletonized mean diffusivity.
Correlation between PSMD and clinical characteristics
PSMD was positively correlated with age in both patients with cluster headache (r = 0.575, p = 0.008) (Fig. 2A) and healthy controls (r = 0.449, p = 0.046) (Fig. 2B). However, after applying Bonferroni correction for multiple comparisons, the correlation in the healthy control group was no longer statistically significant.

Correlation between age and PSMD among participants. The figures demonstrate a positive correlation between PSMD and age in both groups: (A) patients with cluster headache (r = 0.575, p = 0.008) and (B) healthy controls (r = 0.449, p = 0.046).The unit of PSMD in the figure is x10⁻ 3 mm²/s. PSMD peak width of skeletonized mean diffusivity.
No significant associations were identified between PSMD and other clinical factors, including disease duration (r = -0.028, p = 0.905) and headache intensity (r = 0.166, p = 0.484).
Comparison of conventional DTI metrics
There were no significant differences of the conventional DTI metrics between patients with cluster headaches and healthy controls. This included FA (0.465 ± 0.017 vs. 0.460 ± 0.018, p = 0.316), MD (0.859 ± 0.041 vs. 0.865 ± 0.022, p = 0.592), AD (1.321 ± 0.045 vs. 1.322 ± 0.023, p = 0.916), and RD (0.628 ± 0.042 vs. 0.636 ± 0.027, p = 0.478).
ROC curve analysis
To evaluate the discriminatory performance of each diffusion metric in distinguishing patients with cluster headache from healthy controls, receiver operating characteristic (ROC) analyses were conducted (Fig. 3). PSMD showed the highest diagnostic accuracy, with an area under the curve (AUC) of 0.743 (p = 0.002), indicating statistically significant discriminatory power. In contrast, conventional DTI metrics demonstrated lower and non-significant AUC values: FA (AUC = 0.560, p = 0.522), MD (AUC = 0.640, p = 0.129), AD (AUC = 0.608, p = 0.262), and RD (AUC = 0.623, p = 0.186).

ROC curve analysis PSMD shows the highest diagnostic accuracy, with an area under the curve (AUC) of 0.743 (p = 0.002), indicating statistically significant discriminatory power. In contrast, conventional DTI metrics demonstrated lower and non-significant AUC values: FA (AUC = 0.560, p = 0.522), MD (AUC = 0.640, p = 0.129), AD (AUC = 0.608, p = 0.262), and RD (AUC = 0.623, p = 0.186). PSMD peak width of skeletonized mean diffusivity, FA fractional anisotropy, MD mean diffusivity, AD axial diffusivity, RD radial diffusivity.
Discussion
The primary findings of this study indicate that patients with cluster headaches exhibit significantly elevated PSMD values compared to healthy controls, suggesting microstructural white matter alterations associated with the disorder. Notably, there were no lateralized differences in PSMD between the symptomatic and contralateral hemispheres, supporting the notion that white matter changes in cluster headache are diffuse rather than confined to the side of headache symptoms. PSMD was also positively correlated with age in patients, consistent with prior evidence that white matter integrity declines with aging. Furthermore, no significant associations were observed between PSMD and clinical factors such as disease duration or headache intensity, implying that white matter alterations may occur independently of these variables. There were no significant differences of the conventional DTI measures, including FA, MD, AD, and RD, between the patients with cluster headache and healthy controls.
Previous DTI-based studies have also reported white matter abnormalities in patients with cluster headaches9. Szabo et al. reported increased mean, axial, and perpendicular diffusivity in widespread white matter regions, including the frontal, parietal, temporal, and occipital lobes, along with reduced FA in the corpus callosum and certain frontal and parietal white matter tracts, primarily on the contralateral side of pain9,18,19. Another study found bilateral microstructural changes in the brainstem, thalamus, internal capsule, and cerebellum, with additional lesions detected in the basal frontal lobe, implicating the olfactory system and trigeminal-sympathetic pathways18. Chou et al. investigated white matter changes in patients with cluster headaches using post-hoc probabilistic tractography to better understand the disease’s pathophysiology19. Their results showed that during the “in-bout” period, patients exhibited higher absolute radial diffusivities and MD in the left medial frontal gyrus and frontal sub-gyrus and lower diffusivities in the right parahippocampal gyrus of the limbic lobe, compared to healthy controls. These changes generally persisted into the “out-of-bout” period, except in the left cerebellar tonsil. Post-hoc tractography revealed consistent anatomical connections between these altered regions and the hypothalamus across participants. These findings suggest that disruptions in white matter connections between pain-modulation areas and the hypothalamus may play a significant role in the pathophysiology of cluster headaches19. These results, along with the present study, suggest widespread white matter abnormalities in cluster headaches, involving multiple neural systems, including those related to pain processing, the sympathetic nervous system, and potentially the olfactory system. Furthermore, our findings, alongside earlier studies, support the notion that these changes are not confined to the symptomatic side, highlighting a more widespread and non-lateralized white matter disruptions in patients with cluster headaches.
This study also highlights that PSMD increases with age in patients with cluster headaches, consistent with prior research findings13,20,21,22,23. As we age, white matter undergoes degeneration driven by various factors, including reduced myelin integrity, the protective sheath surrounding nerve fibers24,25,26. This deterioration impairs the efficiency of neural communication, as myelin damage slows the transmission of electrical signals between brain regions. Age-related vascular changes, oxidative stress, and inflammation further exacerbate white matter breakdown. These cumulative alterations contribute to cognitive decline and increased susceptibility to neurological disorders by impairing the brain’s capacity to process and integrate information24,25,26.
Although PSMD has been reported to reflect white matter changes associated with small vessel disease11,12,27, the relationship between cluster headache and small vessel disease remains poorly understood. Small vessel disease, characterized by changes in the brain’s small blood vessels, has been linked to white matter abnormalities and microstructural changes28. Similarly, cluster headaches have been linked to disruptions in brain regions and pathways involved in pain processing, including the hypothalamus and white matter microstructure. However, although PSMD has been widely used as a marker of small vessel disease, its elevation in patients with cluster headaches should be interpreted with caution. While both cluster headache and small vessel disease are associated with white matter microstructural changes, the underlying mechanisms may differ. It is currently unknown whether the observed PSMD changes in cluster headache reflect microvascular pathology, neuroinflammation, or other disease-specific processes. The overlap in imaging findings is intriguing and raises the hypothesis that vascular dysregulation or subtle microvascular involvement could exacerbate hypothalamic dysfunction and neuronal hyperexcitability, key features of cluster headaches pathophysiology28,29. However, this remains speculative and should be further investigated in future studies incorporating direct markers of vascular health and inflammatory processes.
While traditional DTI metrics such as FA, MD, AD, and RD have been extensively used to assess white matter integrity, PSMD offers distinct advantages. Notably, PSMD has demonstrated higher sensitivity in detecting subtle white matter changes, as evidenced in studies where it identified alterations not captured by conventional metrics. In the present study, conventional DTI metrics such as FA, MD, AD, and RD did not show statistically significant differences between patients with cluster headaches and healthy controls. However, PSMD values were significantly elevated in the cluster headache group, indicating its greater sensitivity in detecting white matter microstructural alterations. In a study involving first-episode schizophrenia patients, PSMD was the only DTI-derived metric that showed significant differences compared to healthy controls. Conventional metrics like FA, MD, AD, and RD did not exhibit significant changes30. In addition, PSMD has demonstrated high reproducibility and reliability across different MRI scanners and imaging protocols. This robustness makes it a valuable tool for multi-center studies and clinical applications where consistency across varying equipment and procedures is crucial11. Furthermore, PSMD has been found to correlate strongly with cognitive performance, particularly processing speed. In contrast, conventional DTI metrics have shown weaker or inconsistent associations with cognitive measures. This indicates that PSMD may provide more relevant insights into the functional implications of white matter integrity31,32.
In line with our primary findings, ROC curve analysis demonstrated that PSMD outperformed conventional DTI metrics in distinguishing patients with cluster headache from healthy controls. PSMD achieved a statistically significant area under the curve, whereas FA, MD, AD, and RD yielded lower and non-significant AUC values. These results reinforce the superior sensitivity of PSMD in capturing subtle white matter alterations that may be missed by traditional diffusivity measures. The higher discriminatory power of PSMD may be attributed to its design, which captures the variability in MD across the white matter skeleton, rather than relying on regional or directional diffusion properties alone. This makes PSMD particularly valuable in detecting diffuse microstructural changes, as may be present in cluster headache.
This study is the first to investigate white matter microstructural changes in patients with cluster headaches using PSMD. However, several limitations should be noted. First, a key limitation of this study was the relatively small sample size, with 20 participants in each group. This limited sample may reduce the generalizability of our findings and constrain the statistical power to detect subtle effects. In particular, the possibility of Type II errors should be considered when interpreting non-significant results, such as the absence of differences in PSMD between the symptomatic and contralateral hemispheres. With a larger cohort, such comparisons may have yielded significant findings, particularly if the effects are modest in magnitude. Additionally, the small sample size may limit the robustness of correlation analyses and restrict the exploration of more complex interactions between clinical variables and imaging biomarkers. Second, the cross-sectional design precludes conclusions about causality or the progression of white matter changes over time. Third, our study had the lack of data on lifestyle-related factors that may influence white matter integrity. Although participants with overt vascular risk factors such as hypertension, diabetes, and dyslipidemia were excluded, other potential confounding variables, such as smoking status, alcohol consumption, physical activity, and sleep patterns, were not systematically assessed or controlled for in the current study. These factors are known to impact white matter microstructure and could have contributed to inter-individual variability in PSMD values. Lastly, another limitation of this study was the lack of cognitive function assessment in participants. Previous research has demonstrated that PSMD is strongly associated with cognitive performance, particularly processing speed, and may provide important insights into the functional consequences of white matter microstructural changes. However, in the current study, we did not collect or analyze cognitive data, which limits our ability to explore the clinical significance of elevated PSMD values in terms of neuropsychological outcomes.
In conclusion, this study demonstrates that patients with cluster headache exhibit diffuse white matter microstructural abnormalities as reflected by elevated PSMD values, even in the absence of changes in conventional DTI measures. These findings highlight the potential utility of PSMD as a sensitive imaging biomarker in neurological disorders. Further studies with larger cohorts, longitudinal designs, and detailed clinical and cognitive profiling are needed to validate and expand on these results.
Methods
Participants
The study protocol was approved by the Institutional Review Board of Haeundae Paik Hospital. Informed consent was obtained from all subjects, and all medical procedures followed the tenets of the Declaration of Helsinki. Twenty patients with newly diagnosed episodic cluster headaches were prospectively recruited from a single hospital between September 2019 and December 2023. The diagnosis was based on clinical criteria outlined in the International Classification of Headache Disorders, 3rd edition33. All included patients experienced strictly unilateral cluster headache attacks, consistently occurring on the same side. Participants with alternating or bilateral headache presentations were excluded to ensure consistency in the lateralized analysis. All participants underwent DTI imaging at the time of diagnosis, prior to receiving pharmacological treatment. Participants with any history of neurological disorders other than cluster headaches, structural brain abnormalities on brain MRI, or risk factors for small vessel disease (e.g., diabetes, hypertension, or dyslipidemia) were excluded. The study also included 20 age- and sex-matched healthy controls with no medical or neurological conditions. All control participants underwent the same imaging protocols and were confirmed to have no visible abnormalities on brain MRI or known risk factors for small vessel disease.
DTI scanning protocol
DTI scans were performed using a 3.0 T MRI scanner with a 32-channel head coil (AchievaTx; Philips Healthcare, Best, Netherlands). The scanning protocol employed spin-echo single-shot echo-planar pulse sequences with 32 diffusion directions, a repetition time of 8620 ms, an echo time of 85 ms, a flip angle of 90°, and a slice thickness of 2.25 mm. The acquisition matrix was 120 × 120, with a field of view of 240 × 240 mm² and a b-value of 1,000 s/mm².
PSMD acquisition
PSMD values were derived from DTI data using the FMRIB Software Library (FSL) on a Linux platform, following a standardized four-step process11,12:
-
1.
Preprocessing included motion and eddy current correction, brain extraction, and tensor fitting on the raw DTI data.
-
2.
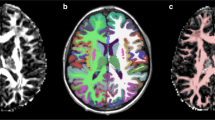
Skeletonization aligned FA maps to a standardized space and projected them onto a white matter framework using tract-based spatial statistics (TBSS). The same transformation matrices were then applied to MD maps to generate skeletonized MD maps.
-
3.
A custom mask with a threshold FA value of 0.3 was applied to the skeletonized MD maps to focus analyses on relevant white matter tracts.
-
4.
Histogram analysis was performed by generating histograms of MD values from all voxels within the skeleton. PSMD was calculated as the difference between the 95th and 5th percentiles of the histogram distribution.
PSMD values were calculated separately for the whole brain and the right and left hemispheres.
FA, MD, AD, and RD analysis
Conventional DTI metrics, including FA, MD, AD, and RD, were computed using the DSI Studio software package. DTI data were imported in DICOM format, and we set the brain mask with thresholding, smoothing, and defragment steps. Then, we did reconstruction and fiber tracking. Whole-brain seeding was conducted with a total of 10,000 seeds, and the angular threshold was 60 degrees. Tracks with length less than 30 mm were discarded. The Automated Anatomical Labeling template was used for brain parcellation, and every white matter fiber was evaluated for extreme points. After a whole brain seeding, we calculated the conventional DTI measures, including FA, MD, AD, and RD values.
Statistical analysis
Statistical analyses were conducted using MedCalc® Statistical Software version 22.009 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2023). Group differences in age, PSMD, FA, MD, AD, and RD values were assessed using independent sample t-tests, while sex differences were evaluated with the chi-square test. Pearson’s correlation analysis was performed to examine associations between PSMD and clinical factors. Statistical significance was defined as a p-value of < 0.05. To account for the risk of Type I error due to multiple comparisons, we applied the Bonferroni correction when performing correlation analyses and comparing conventional DTI metrics (FA, MD, AD, and RD) between groups. Given that four comparisons were made, a Bonferroni-adjusted significance threshold of p < 0.0125 (i.e., 0.05/4) was used to determine statistical significance.
To evaluate the discriminatory ability of PSMD and conventional DTI metrics (FA, MD, AD, RD) in differentiating patients with cluster headache from healthy controls, we performed ROC curve analyses for each parameter. The area under the curve (AUC) was calculated to quantify diagnostic performance, with higher AUC values indicating better discriminatory power. Sensitivity and specificity values were also derived at optimal cutoff points based on Youden’s index.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
15 September 2025
The original online version of this Article was revised: In the original version of this Article, Kang Min Park was incorrectly affiliated with ‘Department of Thoracic and Cardiovascular Surgery, Busan Paik Hospital, Inje University College of Medicine, Busan, Republic of Korea’. The correct affiliation is ‘Department of Neurology, Haeundae Paik Hospital, Inje University College of Medicine, Haeundae-ro 875, Haeundae-gu, Busan 48108, Republic of Korea’.
References
Lindemann, C. R. Cluster headache: A review of clinical presentation, evaluation, and management. JAAPA 35, 15–19, (2022). https://doi.org/10.1097/01.JAA.0000840484.33065.21
Fischera, M., Marziniak, M., Gralow, I. & Evers, S. The incidence and prevalence of cluster headache: a meta-analysis of population-based studies. Cephalalgia 28, 614–618. https://doi.org/10.1111/j.1468-2982.2008.01592.x (2008).
Cho, S. et al. Efficacy of oxygen treatment using home oxygen concentrators for the treatment of cluster headaches: A randomized, crossover, multicenter study. J. Clin. Neurol. 20, 78–85. https://doi.org/10.3988/jcn.2023.0103 (2024).
Soborg, M. K., Jensen, R. H., Barloese, M. & Petersen, A. S. Biomarkers in cluster headache: A systematic review. Headache 64, 98–116. https://doi.org/10.1111/head.14641 (2024).
Silvestro, M. et al. Cluster headache pathophysiology: what we have learned from advanced neuroimaging. Headache 62, 436–452. https://doi.org/10.1111/head.14279 (2022).
Iacovelli, E., Coppola, G., Tinelli, E., Pierelli, F. & Bianco, F. Neuroimaging in cluster headache and other trigeminal autonomic cephalalgias. J. Headache Pain. 13, 11–20. https://doi.org/10.1007/s10194-011-0403-8 (2012).
Lee, D. A., Lee, H. J., Kim, H. C. & Park, K. M. Alterations of the structural covariance network in the hypothalamus of patients with cluster headache. J. Neurol. 269, 316–322. https://doi.org/10.1007/s00415-021-10629-z (2022).
Arkink, E. B. et al. The anterior hypothalamus in cluster headache. Cephalalgia 37, 1039–1050. https://doi.org/10.1177/0333102416660550 (2017).
Szabo, N. et al. White matter disintegration in cluster headache. J. Headache Pain. 14, 64. https://doi.org/10.1186/1129-2377-14-64 (2013).
Morelli, N. et al. Functional magnetic resonance imaging in episodic cluster headache. J. Headache Pain. 10, 11–14. https://doi.org/10.1007/s10194-008-0085-z (2009).
Zanon Zotin, M. C. et al. Peak width of skeletonized mean diffusivity: A neuroimaging marker for white matter injury. Radiology 306, e212780. https://doi.org/10.1148/radiol.212780 (2023).
Baykara, E. et al. A novel imaging marker for small vessel disease based on skeletonization of white matter tracts and diffusion histograms. Ann. Neurol. 80, 581–592. https://doi.org/10.1002/ana.24758 (2016).
Beaudet, G. et al. Age-related changes of peak width skeletonized mean diffusivity (PSMD) across the adult lifespan: A Multi-Cohort study. Front. Psychiatry. 11, 342. https://doi.org/10.3389/fpsyt.2020.00342 (2020).
Lam, B. Y. K. et al. Peak width of skeletonized mean diffusivity and its association with age-related cognitive alterations and vascular risk factors. Alzheimers Dement. (Amst). 11, 721–729. https://doi.org/10.1016/j.dadm.2019.09.003 (2019).
Maillard, P. et al. Instrumental validation of free water, peak-width of skeletonized mean diffusivity, and white matter hyperintensities: MarkVCID neuroimaging kits. Alzheimers Dement. (Amst). 14, e12261. https://doi.org/10.1002/dad2.12261 (2022).
Horn, M. J. et al. Peak width of skeletonized mean diffusivity and cognitive performance in cerebral amyloid angiopathy. Front. Neurosci. 17, 1141007. https://doi.org/10.3389/fnins.2023.1141007 (2023).
Jochems, A. C. C. et al. Associations of Peak-Width skeletonized mean diffusivity and Post-Stroke cognition. Life (Basel). 12 https://doi.org/10.3390/life12091362 (2022).
Teepker, M. et al. Diffusion tensor imaging in episodic cluster headache. Headache 52, 274–282. https://doi.org/10.1111/j.1526-4610.2011.02000.x (2012).
Chou, K. H. et al. Altered white matter microstructural connectivity in cluster headaches: a longitudinal diffusion tensor imaging study. Cephalalgia 34, 1040–1052. https://doi.org/10.1177/0333102414527649 (2014).
Park, K. M., Kim, K. T., Lee, D. A. & Cho, Y. W. Small vessel disease in patients with restless legs syndrome evidenced by elevated peak width of skeletonized mean diffusivity. J. Neurol. Sci. 467, 123310. https://doi.org/10.1016/j.jns.2024.123310 (2024).
Lee, D. A., Lee, H. J., Kim, S. E. & Park, K. M. Peak width of skeletonized mean diffusivity as a marker of small vessel disease in patients with Temporal lobe epilepsy with hippocampal sclerosis. Epilepsia https://doi.org/10.1111/epi.18205 (2024).
Lee, D. A., Lee, H. J. & Park, K. M. Evidence of small vessel disease in patients with juvenile myoclonic epilepsy based on the peak width of skeletonized mean diffusivity. Seizure 124, 75–79. https://doi.org/10.1016/j.seizure.2024.12.003 (2024).
Lee, D. A., Lee, H. J. & Park, K. M. Evidence of small vessel disease in patients with transient global amnesia based on the peak width of skeletonized mean diffusivity. AJNR Am. J. Neuroradiol. https://doi.org/10.3174/ajnr.A8530 (2024).
Caligiuri, M. E. et al. Automatic detection of white matter hyperintensities in healthy aging and pathology using magnetic resonance imaging: A review. Neuroinformatics 13, 261–276. https://doi.org/10.1007/s12021-015-9260-y (2015).
Gunning-Dixon, F. M., Brickman, A. M., Cheng, J. C. & Alexopoulos, G. S. Aging of cerebral white matter: a review of MRI findings. Int. J. Geriatr. Psychiatry. 24, 109–117. https://doi.org/10.1002/gps.2087 (2009).
Gunning-Dixon, F. M. & Raz, N. The cognitive correlates of white matter abnormalities in normal aging: a quantitative review. Neuropsychology 14, 224–232. (2000).
Low, A. et al. Peak width of skeletonized mean diffusivity as a marker of diffuse cerebrovascular damage. Front. Neurosci. 14, 238. https://doi.org/10.3389/fnins.2020.00238 (2020).
Hannawi, Y. Cerebral small vessel disease: a review of the pathophysiological mechanisms. Transl Stroke Res. 15, 1050–1069. https://doi.org/10.1007/s12975-023-01195-9 (2024).
Low, A., Mak, E., Rowe, J. B., Markus, H. S. & O’Brien, J. T. Inflammation and cerebral small vessel disease: A systematic review. Ageing Res. Rev. 53, 100916. https://doi.org/10.1016/j.arr.2019.100916 (2019).
Xu, M. et al. Peak width of skeletonized mean diffusivity as a neuroimaging biomarker in first-episode schizophrenia. Front. Neurosci. 18, 1427947. https://doi.org/10.3389/fnins.2024.1427947 (2024).
Deary, I. J. et al. Brain peak width of skeletonized mean diffusivity (PSMD) and cognitive function in later life. Front. Psychiatry. 10, 524. https://doi.org/10.3389/fpsyt.2019.00524 (2019).
Raposo, N. et al. Peak width of skeletonized mean diffusivity as neuroimaging biomarker in cerebral amyloid angiopathy. AJNR Am. J. Neuroradiol. 42, 875–881. https://doi.org/10.3174/ajnr.A7042 (2021).
Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38, 1-211. https://doi:10.1177/0333102417738202 (2018).
Acknowledgements
This research was supported by a grant of the Korea Health Technology R&D Project throughthe Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health &Welfare, Republic of Korea (grant number : HR21C1003).
Author information
Authors and Affiliations
Contributions
JK and DAL, these two authors equally contributed to paper writing and data analysis as the first author. HJL and KMP participated in recruiting patients and controls and organizing data.KMP supervised the paper writing. JK and DAL wrote the manuscript. JHW participated in additional data analysis and visualization. All the authors participated in the analysis and interpretation of data. All the authors revised the manuscript critically and approved the manuscript in its final form.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kim, J., Lee, D.A., Lee, HJ. et al. White matter alterations in cluster headache identified using PSMD analysis. Sci Rep 15, 24220 (2025). https://doi.org/10.1038/s41598-025-09291-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-09291-6
