
Abstract
Menopausal women in suburban regions often face challenges in accessing healthcare resources, leading to lower health literacy and reduced quality of life. The aim of this study was to determine the effect of an education intervention based on self-efficacy theory on the quality of life, self-efficacy and health literacy of menopausal women living in suburban areas. This Quasi- experimental study was conducted on 214 suburban menopausal women in Mashhad-Iran from 2021 to 2022. At first, women were divided into intervention and control groups by a simple random method. Intervention group received training in four sessions based on the self-efficacy theory. The questionnaires used in this study were TOFLA (Test of Functional Health Literacy in Adults), Scherer’s self-efficacy and MENQOL (Menopausal Quality of Life). Questionnaires were completed before intervention, immediately, and 3 months later. The mean score of quality of life in the experimental group before intervention was 80 ± 27.33, immediately after intervention was 62.66 ± 22.45, and after 3 months was 51.12 ± 23.57 and this improvement was significant (p < 0.001). However, in the control group, there was no significant difference in mean score of quality of life before, immediately and 3 months after the intervention(p > 0.05). The mean score of health literacy in the experimental group before the intervention was 9.36 ± 11.36, immediately after the intervention was 20.65 ± 11.41, and three months after the intervention was 21.09 ± 11.78 (p < 0.001). Results from the study indicated that educational interventions based on the self-efficacy model is an appropriate strategy to promote quality of life and health literacy in menopausal women.
Similar content being viewed by others
Introduction
Menopause one of the important periods in women’s life. Women expend one- third of their life past menopause. women’s knowledge of the changes that occur during middle age and understanding of the reasons for these changes can make it easier to for them to navigate this stage of life. Having Knowledge about health and healthcare can have a positive impact on individuals’ health and well-being. The World Health Organization(WHO) defines quality of life as an individual’s perception of their position in life in the context of the culture and value system in which they live, and obtain about their goals, expectations, communications, and needs. Therefore, all women must live that healthy, and be active in the social and economic the future1.
During menopause, women experience physical and psychological changes that can impact their quality of life and interpersonal relationships. one of the problems that women may experience during menopause is Sexual dysfunction which can affect mental health, quality of life, and interpersonal relationship2. One of the complications of menopause is depression, which can double the problems of this period and can affected quality of life of women3. Anxiety is a condition that can affect quality of life and health of postmenopausal women4. The quality of life of postmenopausal women can also be affected by Genitourinary syndrome5. Genitourinary syndrome of menopause is a persistent and gradually worsening condition that affects the genital and urinary tissues, largely resulting from reduced estrogen during and post-menopause6.
Confidence in one’s abilities is an important and influential factor in the quality of life and controlling middle age symptoms. People with strong self-efficacy believe that they can do any difficult task which can lead to success and hopefulness in work and life. They see difficult tasks as challenges and struggles to become proficient rather than threats that they must avoid. Efficient people in the failure continue to strive that succeed7.
Deficiency of health literacy can be a factor that affects the quality of life of individuals, and it is considered a global threat today. Health education aims to raise the level of health literacy which helps individuals make informed decisions about their health and the health of their community8. In the study of Rachel Yolizmatores, a clear correlation was seen between health literacy, self-efficacy, knowledge. Quality of life improves with proper and timely education accordance with the needs9. This study aimed to determine the effect of educational intervention based on self-efficacy model on promoting quality of life, self-efficacy, and health literacy in menopausal women living in the suburbs of Mashhad, Iran.
Methods
Sampling and design
This study was a quasi-experimental with a control group that was conducted in menopausal women aged 40–60 years living in the suburbs of Mashhad (Iran). The study period was from 2020 to 2021. In this study, the elderly was eligible to participate in the study if (a) they had informed consent to participate in the study; (b) Menopausal women with no documented medication use in their health records; (c) they living in the suburbs of the city and speaking Persian. Exclusion criteria were unwillingness to participate in training sessions during the intervention, the absence of more than two sessions in education classes and presence of incurable diseases.
The sample size was estimated based on the information about mean and standard deviation change of behavior scores between two groups, from a similar study10, Thus, we calculated the sample size equals to 107 participations in each group, using following formula with consideration α = 0.05, β = 0.2, S1 = 9.12, S2 = 10.07, \(\overline{X}\)1 = 55.85 and \(\overline{X}\)2 = 59.45.
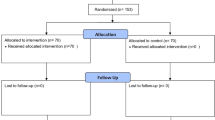
For sampling we used a cluster randomization design, two comparable streets (3 and 6) in Mashhad’s southern marginal zone were selected. Through coin toss randomization, Street 3 became the intervention group while Street 6 served as control. All eligible female residents meeting was enrolled (Fig. 1).

Flow of participants through each stage of the study.
Tools of assessment
The measurement tools were Short Test of Functional Health Literacy in Adults (S-TOFLA), Menopausal Quality of Life (MENQOL) questionnaire, and sharer self-efficacy questionnaires which previously, its validity and reliability have been confirmed in the study of Nowruzi et al.11. The Short Test of Functional Health Literacy in Adults (S-TOFHLA) is a widely recognized instrument for assessing functional health literacy, focusing on reading comprehension and numeracy related to health tasks. This questionnaire contains 36 questions, with each individual’s total score ranging from 0 to 36. In Iran, the full-length Persian version of TOFHLA (which includes the S-TOFHLA components) has been validated and extensively used in health literacy studies among adults. Studies report Cronbach’s alpha coefficients and intraclass correlation coefficients (ICC) for TOFHLA and similar instruments in Iran consistently above 0.7, indicating good reliability12.
Scherer’s general self-efficacy questionnaire consists of 17 standard questions, which are graded on a Likert scale from Strongly Disagree (1) to Strongly Agree (5). The maximum score is 85 and the minimum is 17. This questionnaire has been translated and validated by Asgharnejad in Iran13. In various Iranian studies, the Cronbach’s alpha coefficient of this questionnaire has been reported to be between 0.75 and 0.89, indicating favorable reliability14.
The Menopausal Quality of Life Questionnaire was developed and standardized by John Hildage et al. and consists of 29 questions with psychosocial (7 questions), physical (16 questions), sexual (3 questions), cardiovascular dimension (3 questions), which are graded by Three-option Likert scale. The maximum score is 203 and the minimum is 29. Golrokh Moridi12 approved validity and reliability of this questionnaire in Iran. The lower scores obtained in this questionnaire, indicate a better the quality of life.
The questionnaires were completed before intervention, instantly after the intervention, and at 3-months follow-up by participants in both groups. A demographic form was only full filled at baseline.
Educational intervention
In this study, the intervention was conducted based on self-efficacy model. The intervention was delivered through four 90-minute educational sessions. According to the self-efficacy model, training sessions were conducted based on the progress and success of the participants’ performance in activities to prevent menopausal complications and improve the quality of life during this period. The intervention aimed to realistically design goals and programs and allocate specific rewards for success small goals achieved. The details of the intervention are shown in Table 1. Educational intervention was performed by a specialist health educator at the health care center. Also, review action planning, educational pamphlets, and focus group discussion are used. During the intervention time, participants on the control side had not received any education. They accessed a training package 6 months after the educational intervention.
Statistical analysis
Statistical analysis was performed using SPSS software (version 21). First, the data were checked for normality by Kolmogorov-Smirnov. The characteristics of the participants were described using descriptive statistics. The data were analyzed using independent t-test and Repeated measures. The significance level chosen for this study was p < 0.05.
Results
The Participants were 214 people with a mean age of 53.4 7 ± 7.72. In the control group 53.3%(57) had primary education, 15%(16) middle school, 23.4%(25) had a diploma, and 8.4%(9) had university education. There was no significant difference in education level between the experimental and control groups (P > 0.05). In the control group 92.5%(99) were housewives, 5.6%(6) self-employed. 1.9%(2) had government jobs. Occupational status did not differ significantly between the experimental and control groups (P > 0.05). In the control group, income status was favorable for 58.9%(63), unfavorable for 27.1%(29), while 14%(15) could not meet basic daily needs. We found no significant between-group differences in income status (P > 0.05). Details of the demographic characteristics and matching status of the control and experimental groups were shown in Table 2.
The mean score of quality of life in the experimental group before intervention was 80 ± 27.33, immediately after intervention was 62.66 ± 22.45, (p < 0.001), and after 3 months was 51.12 ± 23.57, (p < 0.001). This improvement was significant (p-value < 0.001). However, in the control group, there was no significant difference in mean score of quality of life before, immediately and 3 months after the intervention (Table 3).
The mean score of health literacy in the experimental group before the intervention was 9.36 ± 11.36, immediately after the intervention was 20.65 ± 11.41, and three months after the intervention was 21.09 ± 11.78, and this improvement was also significant (p-value < 0.001). However, in the control group, there was no significant difference in mean score of quality of life before, immediately and 3 months after the intervention (Table 3).
The self-efficacy scores in the experimental group were 44.73 ± 13.72, before the intervention, 54.76 ± 14.36, immediately after the intervention, and 55.96 ± 14.80, three months after the intervention. This improvement was also significant (p-value < 0.001). However, in the control group, there was no significant difference in mean score of quality of life before, immediately and 3 months after the intervention (Table 3).
Discussion
This study aimed to investigate the effect of an educational intervention based on self-efficacy theory on the quality of life, self-efficacy, and health literacy of postmenopausal women who living in the suburban areas. The results generally showed that Self-efficacy training has been found to be effective in improving the health literacy and quality of life of postmenopausal women living in suburban areas. In line with this finding, Hossein Mirzaee Beni in their study conducted on menopausal women showed that self-care education on the health literacy index significantly improves the quality of life of menopausal women and self-care15. Another study conducted on 60 menopausal women in Iran also showed that educational intervention based on health literacy is effective in improving the quality of life of menopausal women.
Quality of life refers to an individual’s perception of physical, mental, social, and environmental health state. Various variables such as personal characteristics can have an impact on the quality of life. These variables may include: age, gender, personality and education. organizational factors such as stress experienced in the workplace and the nature of work and tasks can have an impact on the quality of life. Nazarpour’s et al. found that individual and social factors can exacerbate menopausal complications and thus diminished the quality of life16. Golyan et al. presented that one of the main factors to improve quality of life is the improvement of lifestyle17.
The results of the study suggest that education can significantly increase the average health literacy of women. This finding is consistent with the results of previous studies that attributed a significant improvement in health literacy to health education. A study investigated the effect of educational intervention on health literacy, self-efficacy, and quality of life in women and found that training based on health literacy can improve quality of life18. By improving health literacy, women can make informed decisions about their health, engage in self-care practices, and ultimately enhance their overall well-being19. In a study conducted by Khanderoo et al. on postmenopausal women, it was shown that education improves women’s health literacy, and increasing health literacy is significantly effective in improving the quality of life20. Additionally, a study found that self-care education based on the health literacy index has the potential to improve self-care and quality of life among menopausal women15.
The results of the study on self-efficacy showed that after the educational intervention, the mean of self-efficacy in the intervention group increased significantly, while no significant increase was observed in the control group. This suggests that the educational intervention had a positive impact on the self-efficacy of postmenopausal women in intervention group compared to the control group. the results of other studies are similar to the study in question because they also trained the participants about menopause-related self-care1. For example, a randomized controlled trial found that a group-based educational program improved the self-efficacy and self-acceptance of Iranian menopausal women21. One study found that self-care education based on self-efficacy theory, individual empowerment model, and their integration improved the quality of life of menopausal women22.
Limitation
In this study, we faced some limitations. First, the self-report questionnaire was used, possibly leading to biases in final outcomes. Second, the presence of Covid-19 and its impact on communication and education of participants, as well as the fear of Covid-19 if they participated in training classes.
Conclusion
Based on these findings, it can be concluded that education plays a crucial role in increasing the health literacy of women, leading to improved quality of life. These interventions can be particularly beneficial for postmenopausal women living in suburban areas who may face unique challenges in accessing healthcare and health information. Using the results of such studies in the community can have several positive impacts, particularly in promoting women’s health and well-being, making them healthier and more productive throughout their lives, and taking more effective steps toward sustainable development. In addition to providing the necessary knowledge about menopausal symptoms, complications, how to deal with and adapt to them to maintain health and improve the menopausal quality of life, it is important to Create support groups, induce a positive attitude, and promote healthier behaviors among in postmenopausal women.
Educational interventions can also help managers of health services in controlling and reducing the complications of menopause and reducing the resulting burden on the health care system. Authorities can use the results of this study to inform their policies in disease and health services management.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Tugut, N., Yesildag Celik, B. & Yılmaz, A. Health literacy and its association with health perception in pregnant women. J. Health Lit. 6 (2), 9–20 (2021).
Hosseinabadi, M. et al. Sexual function and marital satisfaction of migrant women during menopause: an application of the theory of planned behavior. Iran. J. Health Educ. Health Promotion. 11 (1), 69–80 (2023).
Karimi, F. Z. et al. Sexual dysfunction in postmenopausal women. Acta Med. Iran. 2021, 720–725 .
Bakhshi, F. et al. Applying the social cognitive theory for predicting the related factors to mental health of middle-age women referring to comprehensive health services centers. Iran. J. Health Educ. Health Promotion. 11 (2), 127–140 (2023).
Salarfard, M., Yazdimoghaddam, H., Abdollahi, M. & Karimi, F. The effect of herbal medicines on vaginal atrophy in postmenopausal women: a systematic review and meta-analysis. Iran. J. Obstet. Gynecol. Infertility. 24 (13), 100–118 (2022).
Angelou, K., Grigoriadis, T., Diakosavvas, M., Zacharakis, D. & Athanasiou, S. The genitourinary syndrome of menopause: an overview of the recent data. Cureus 12 (4), e7586 (2020).
Gheshlagh, R. G. et al. Psychometric features of the Persian version of self-efficacy tool for patients with hypertension. Int. Cardiovasc. Res. J. 12 (2), 50–56 (2018).
Kharazi Ss, Peyman, N. & Esmaily, H. The effect of health literacy and Self-Efficacy intervention on nutrition of pregnant mothers and infant weight. J. Health Lit. 7 (2), 24–36 (2022).
Torres, R. Y. & Marks, R. Relationships among health literacy, knowledge about hormone therapy, self-efficacy, and decision-making among postmenopausal health. J. Health Communication. 14 (1), 43–55 (2009).
mohammadi, N. Takarli f, khodaveisi m, Soltanian a: the effect of peer educational program on the Self-Efficacy of multiple sclerosis patients: A Randomized-Controlled trial. Avicenna J. Nurs. Midwifery Care. 25 (2), 36–44 (2017).
Norozi, E., Mostafavi, F., Hassanzadeh, A., Moodi, M. & Sharifirad, G. Factors related with quality of life among postmenopausal women inisfahan, iran, based on behavioral analysis phase of PRECEDE model. Health Syst. Res. 7 (3), 0–0 (2011).
Tavousi, M. et al. Health literacy instrument for Adults-Short form (HELIA-SF): development and psychometric properties. Payesh (Health Monitor) J. 21 (3), 309–319 (2022).
Asgharnejad, T., Ahmadi, D. M., Farzad, V. E. & Khodapanahi, M. K. Psychometric Properties of Sherer’s General Self-Efficacy Scale (2006).
Sharif-Nia, H., She, L., Rahmatpour, P., Sharifi, M. & Goudarzian, A. H. Self-Efficacy scale among Iranian cardiovascular patients: Persian translation, validity, and reliability assessment. J. Nurs. Meas. 32 (3), 404–414 (2024).
Hossein Mirzaee Beni, Z., Maasoumi, R., Pashaeypoor, S. & Haghani, S. The effects of self-care education based on the health literacy index on self-care and quality of life among menopausal women: a randomized clinical trial. BMC Women’s Health. 22 (1), 1–10 (2022).
Nazarpour, S., Simbar, M. & Tehrani, F. R. Factors affecting sexual function in menopause: A review Article. Taiwan. J. Obstet. Gynecol. 55 (4), 480–487 (2016).
Golyan Tehrani, S., Ghobadzadeh, M. & Arastou, M. Promoting health status of menopausal women by educating self care strategies. Hayat 13 (3), 67–75 (2007).
Khaleghi, M., Shokravi, F. A., Peyman, N. & Moridi, M. Evaluating the effect of educational interventions on health literacy through social networking services to promote students’ quality of life. Korean J. Family Med. 40 (3), 188 (2019).
Samerski, S. Health literacy as a social practice: social and empirical dimensions of knowledge on health and healthcare. Soc. Sci. Med. 226, 1–8 (2019).
Khandehroo, M., Tavakoly Sany, S. B., Oakley, D. & Peyman, N. Health literacy intervention and quality of life in menopausal women: a randomized controlled trial. Int. J. Health Promotion Educ. 60 (2), 114–126 (2022).
Moshki, M., Mohammadzadeh, F. & Dehnoalian, A. The effectiveness of a group-based educational program on the self-efficacy and self-acceptance of menopausal women: A randomized controlled trial. J. Women Aging. 30 (4), 310–325 (2018).
Tajurahim, N. N. S., Abu Bakar, E., Md Jusoh, Z., Ahmad So, M. & Arif, A. M. The effect of intensity of consumer education, self-efficacy, personality traits and social media on consumer empowerment. Int. J. Consumer Stud. 44 (6), 511–520 (2020).
Acknowledgements
We are particularly grateful to the researchers who have provided us with a wealth of knowledge and experience of menopause. As well, we thank professors of the Faculty of Health and Research Committee of Mashhad University of Medical Sciences.
Funding
This study was sponsored by Mashhad University of Medical Sciences. There was no funding agency’s role in the design of the study, data collection, and analysis, or presentation of the results.
Author information
Authors and Affiliations
Contributions
Conceived and designed the review, writing & editing: H T. Data collection: M Kh. Preformed analysis and validation: N P and M Gh-A. Supervision and conceptualization: H T.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This article is a part of research in the field of Health Education and Health Promotion at Mashhad University of Medical Sciences. All procedures performed in studies were in accordance with the ethical standards of the institutional research committee with the 1964 Helsinki declaration. This study was conducted after the approval and permission of Mashhad University of Medical Sciences Research Committee (IR.MUMS.FHMPM.REC.1400.035).
Informed consent
Written informed consent was obtained from the participants. Moreover, they were assured that all the information would be kept confidential and would not be revealed unless for research purposes and in an anonymous form.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Khandehroo, M., Peyman, N., Gholian-Aval, M. et al. Self-efficacy intervention on health literacy and quality of life in menopausal women of suburban areas. Sci Rep 15, 23813 (2025). https://doi.org/10.1038/s41598-025-09347-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-09347-7
