
Abstract
TNFα-induced protein 2 (TNFAIP2) reportedly plays a significant role in the initiation and progression of malignancy. However, its function in skin cutaneous melanoma (SKCM) is largely unknown and urgently needs to be explored. Analysis of a publicly available database revealed that TNFAIP2 was significantly downregulated in SKCM tissues vs. normal controls (P < 0.001) and that its expression was a significant indicator for SKCM diagnosis (AUC = 0.742). Patients with low TNFAIP2 expression tended to have tumors in advanced clinical stages with a poor prognosis (P < 0.01), which was validated in our cohort. Subsequent enrichment analysis revealed that genes differentially expressed between SKCM tissues with high and low TNFAIP2 expression were highly enriched in with multiple tumor immune signatures, especially immune checkpoint signalling. Immune infiltration estimation indicated that TNFAIP2 upregulation predicated increased infiltration of CD8+ T cells, B cells, NK cells, and M1 macrophages and predicted a favourable response to immune checkpoint blockade (ICB) treatment in SKCM. In the SKCM mouse model, TNFAIP2 overexpression suppressed tumor growth and lung metastasis, and this effect was even more pronounced in immunocompetent mice; notably, these mice presented increased infiltration of CD8+ T cells and M1 macrophages into the tumor microenvironment. Moreover, TNFAIP2 overexpression clearly increased the sensitivity of SKCM to anti-PD-1 immunotherapy. The above results indicate the tumor-suppressive role of TNFAIP2, which may be a promising target for improving the efficacy of ICB treatment in SKCM.
Similar content being viewed by others


Introduction
Skin cutaneous melanoma (SKCM), which originates from highly malignant melanocytes, accounts for approximately 6.8-20% of all skin malignancies. Globally, approximately 160,000 new cases of SKCM and 48,000 related deaths occur each year, and the incidence rate is still increasing by 3–7% per year1. Many factors, including race, genetics, carcinogen exposure and ultraviolet radiation, have been proven to be related to SKCM initiation2. Compared with patients with other solid tumor types, SKCM patients die younger and have a much higher risk of distant metastasis3. Despite surgery, chemotherapy and targeted therapy utilization, the overall survival rate of SKCM patients has not fundamentally improved. Dissecting the complex tumor constitution and its precise interactions are urgently needed to overcome the current SKCM treatment dilemma.
The tumor microenvironment (TME) is a dynamic and modifiable network. Tumor cells, the dominant cell type in the TME, promote an immunosuppressive state to avoid immune elimination and ultimately accomplish immune escape4,5. Therefore, targeting the abnormal TME, rather than merely targeting tumor cells, may be a better approach for treating malignancies. In this context, immunotherapy has greatly revolutionized cancer treatment. Multiple immunotherapies, including cancer vaccines, adoptive cell transfer, oncolytic virus therapy and immune checkpoint blockade, have achieved remarkable therapeutic effects6,7. Among these immunotherapies, anti-PD-1/PD-L1-based immunotherapy is the most widely used in SKCM. However, its effects are mild and temporary because of primary or acquired resistance in most patients. According to previous research, CD8+ T cells exclusion and alternative M2 macrophage activation are significantly associated with low efficacy of ICB treatment8,9. A high level of CD8+ T cells and M1 macrophages infiltrating the TME at baseline and/or during treatment can predict a favourable clinical response. Therefore, it is critical to elucidate the mechanism underlying the immunosuppressive TME to increase the efficacy of ICB treatment.
TNFα-induced protein 2 (TNFAIP2) was initially identified in umbilical vein endothelial cells stimulated with TNFα and has been comprehensively investigated in several cancer types, including acute promyelocytic leukaemia, breast cancer, and nasopharyngeal carcinoma10,11,12. Our previous research revealed that TNFAIP2 confers intrinsic cisplatin resistance and lymphatic metastasis in oral squamous cell carcinoma via the KEAP1/NRF2 and NF-κB signalling pathways, respectively13,14. In recent years, its function in regulating the tumor immune microenvironment has been gradually revealed15,16. However, its specific role in SKCM, especially with respect to immunoregulation, is largely unknown.
In this study, the differential expression, prognostic value and function of TNFAIP2 in SKCM were systematically assessed by integrating the Cancer Genome Atlas (TCGA) and Gene Expression Omnibus (GEO) databases. In particular, TNFAIP2 expression was strongly correlated with the enrichment of many immune-associated gene sets and infiltrating immune cell types. Furthermore, TNFAIP2 upregulation was identified as an indicator of a favourable response of SKCM to ICB treatment. The above results were validated in an SKCM mouse model in vivo. Taken together, our study preliminarily revealed the potential role of TNFAIP2 in immune activation in the TME and suggested that TNFAIP2 might be a prospective target for improving SKCM immunotherapy efficacy.
Results
TNFAIP2 is a protective factor in SKCM progression
According to the GENT2 database, TNFAIP2 is downregulated in skin cancer vs. controls at both the tissue and cell line levels (Fig. S1A–B). To further determine its expression characteristics, we referred to the TCGA-SKCM dataset. The results indicated that TNFAIP2 mRNA expression was lower in SKCM tissues than in normal skin tissues (Fig. 1A). Moreover, the area under the receiver operating characteristic curve (AUC) value was 0.742 (Fig. 1B), indicating the high diagnostic efficacy of TNFAIP2 in SKCM. Further analyses of SKCM subgroups revealed that the TNFAIP2 mRNA level was lower in tumors with advanced T stage, a high Clark level and a Breslow depth greater than 3 mm (Fig. 1C–E). In SKCM with ulceration, TNFAIP2 was also significantly downregulated (Fig. 1F). Moreover, the Kaplan‒Meier (KM) curves indicated that SKCM patients with high TNFAIP2 expression always had better overall survival (OS) (P = 0.003) (Fig. 1G) and disease-specific survival (DSS) rates (P < 0.001) (Fig. 1H). In addition, a meta-analysis verified the protective role of TNFAIP2 in SKCM (Fig. S1C). We subsequently constructed a nomogram incorporating the TNFAIP2 level to predict 5-year and 10-year OS and DSS in SKCM patients, and the calibration curve revealed favourable prediction effects (Fig. 1I–N). Taken together, the above results suggest that TNFAIP2 is a protective factor in SKCM patients.

TNFAIP2 is a protective factor in SKCM progression. (A) TNFAIP2 mRNA expression in normal and SKCM based on the TCGA database. (B) AUC evaluated the diagnosis value of TNFAIP2 in SKCM. (C–F) TNFAIP2 mRNA expression in different T stages (C), Clark levels (D), Breslow depths (E) and ulceration subtype of SKCM (F). (G–H) Prognosis values of TNFAIP2 in OS and DSS of SKCM. (I–K) Construction and assessment of TNFAIP2 associated nomogram to predict 5-, and 10-year OS of SKCM. (L–N) Construction and assessment of TNFAIP2 associated nomogram to predict 5-, and 10-year DSS of SKCM. AUC, area under receiver operating characteristic curve. OS, overall survival. DSS, disease special survival. *P < 0.05. **P < 0.01. ***P < 0.001.
The protective role of TNFAIP2 was validated in the SKCM cohort
To verify the aforementioned results, we conducted immunohistochemistry (IHC) on a group of 20 normal skin tissues and 86 SKCM tissues. The results revealed that TNFAIP2 was downregulated in tumors and was expressed mainly in the cytoplasm in both normal and cancerous cells (Fig. 2A–B). Further immunofluorescence staining revealed that TNFAIP2 was expressed in the nucleus of keratinocytes (HaCaT) and melanoma cells (A375), whereas it was almost completely concentrated in the cytoplasm in normal melanocytes (PIG1) (Fig. S2). Among the 86 included SKCM patients {age mean [standard deviation (SD)], 65.53 (11.57) years; 54.7% (47) males}, approximately 60.5% (52) had low TNFAIP2 expression. Further analyses revealed that TNFAIP2 staining intensity was lower in larger tumors and tumors with Breslow depths greater than 3 mm, suggesting its ability to suppress tumor growth and invasion (Fig. 2C–D). Although the difference in TNFAIP2 expression wasnot significant between SKCM patients with or without local/distant metastasis (Fig. 2E–F), survival analysis revealed that TNFAIP2 downregulation predicted poor OS (Fig. 2G). Furthermore, univariate and multivariate Cox proportional hazard regression confirmed that TNFAIP2 is an independent protective factor in SKCM (Fig. 2H). Therefore, the above results validate the protective role of TNFAIP2 in SKCM.

The protecting role of TNFAIP2 is validated in SKCM cohort. (A) Representative IHC images of TNFAIP2 in normal skin and SKCM tissues. Scale bars, 100 μm. (B–F) Quantitative analyses of TNFAIP2 in different clinical subgroups. (G) Prognosis values of TNFAIP2 in OS of SKCM. (H) Univariate and multivariate COX proportional hazard regression evaluated prognosis values of TNFAIP2 in SKCM. IHC, immunohistochemistry. OS, overall survival. N.S., no significance. **P < 0.01. ***P < 0.001.
TNFAIP2 inhibits the proliferation and migration of SKCM cells in vitro
To verify the tumor-suppressive role of TNFAIP2 in SKCM, we overexpressed or knocked down TNFAIP2 in the A375 and B16 cell lines, respectively (Fig. 3A–B). A CCK-8 assay revealed that cell viability was significantly decreased when TNFAIP2 was overexpressed but increased after TNFAIP2 was knocked down (Fig. 3C). In addition, we conducted a 5-ethynyl-2′-deoxyuridine (EdU) staining assay, and the results revealed that TNFAIP2 obviously inhibited cell proliferation (Fig. 3D, F). To determine whether TNFAIP2 affects cell motility, wound healing assays were performed. Our results revealed that TNFAIP2 overexpression significantly inhibited cell migration and that TNFAIP2 knockdown promoted cell migration (Fig. 3E, G). These results indicate that TNFAIP2 suppresses SKCM cell viability and motility.

TNFAIP2 inhibits the proliferation and migration of SKCM in vitro. (A–B) The overexpression/ knockdown efficiency of TNFAIP2 in A375 and B16 cells were confirmed by RT‒qPCR and western blot. (C) CCK-8 assay monitored the cell viability of A375 and B16. (D) EDU staining assay evaluated the cell proliferation of A375 and B16. (E) Wound healing assay detected the cell migration of A375 and B16. (F–G) Quantitative analyses of cell proliferation and migration of A375 and B16. *P < 0.05. **P < 0.01. ***P < 0.001.
TNFAIP2 is significantly associated with immune regulation in SKCM
To further determine the biological function of TNFAIP2, enrichment analyses were performed via the GeneMANIA17 database. The results revealed that a series of proteins, such as exocyst complex component 3-like 1 (EXOC3L1), EXOC3L4, EXOC3L2, and DNA topoisomerase II binding protein 1 (TOPBP1), may interact with TNFAIP2. Moreover, several biological functions, including cellular protein-containing complex localization, vesicle tethering complexes, and the cell cortex, were enriched in TNFAIP2-related genes (Fig. 4A). We subsequently conducted Gene Ontology (GO) and Kyoto Encyclopaedia of Genes and Genomes (KEGG) analyses, and the results revealed that TNFAIP2-related genes widely participated in adaptive immune responses, lymphocyte-mediated immunity, Th1-type immune responses, etc. (Fig. 4B). They were also enriched in the NOD-like receptor signalling pathway, the TNF signalling pathway, and immune response-associated pathways (Fig. 4C). Moreover, considering the GO and KEGG results, TNFAIP2 likely plays a nonnegligible role in the tumor-associated immune microenvironment (Fig. 4D). In addition, we explored TNFAIP2-associated signalling pathways via the TCGA-SKCM and GEO (GSE65904) datasets. Gene set enrichment analysis (GSEA) revealed that PD-1 signalling, the CTLA4 pathway, the IFNG pathway, etc., were significantly enriched in TNFAIP2-related genes (Fig. 4E-F), which indicated that TNFAIP2 is closely involved in immunoregulation of the TME in SKCM. Furthermore, other tumor biological pathways, such as “PI3K/AKT signalling”, “VEGF signalling”, and “Wnt signalling”, were also enriched in TNFAIP2-related genes, suggesting that TNFAIP2 might influence tumor progression in addition to immune regulation.

TNFAIP2 is significantly associated with immune regulation in SKCM. (A) Potential TNFAIP2 interacted proteins. (B–C) GO and KEGG analyses based on TNFAIP2 interacted proteins. (D) Construction of GO and KEGG interaction networks. (E–F) GSEA of TNFAIP2 associated immunoregulation signalling pathways. GO, Gene Ontology. KEGG, Kyoto Encyclopaedia of Genes and Genomes. GSEA, gene set enrichment analysis.
TNFAIP2 promotes the antitumor immune response to SKCM
According to the above results, we further conducted immune infiltration estimation via the TCGA-SKCM. The ESTIMATE algorithm strongly positively correlated the TNFAIP2 score with the immune score (R = 0.713, P < 0.001) and the stromal score (R = 0.602, P < 0.001) (Fig. 5A). In addition, the ssGSEA algorithm revealed that TNFAIP2 expression was positively correlated with the proportions of CD8+ T cells (R = 0.517, P < 0.001), cytotoxic cells (R = 0.652, P < 0.001), B cells (R = 0.504, P < 0.001), NK cells (R = 0.175, P < 0.001), and M1 macrophages (R = 0.149, P = 0.001) and negatively correlated with the proportions of M2 macrophages (R=-0.157, P < 0.001), which indicates that TNFAIP2 can promote antitumor immune cell infiltration into the TME (Fig. 5B). Additionally, immune checkpoint genes, which participate in regulating T cells receptor recognition, play significant roles in the immune response. Our results revealed that TNFAIP2 expression was positively correlated with the expression of most immune checkpoints (CD274, CTLA4, and LAG3 but not IGSF8) (Fig. 5C). The recognition of tumor cells by the immune system relies largely on major histocompatibility complexes (MHCs). Increasing evidence indicates that tumor-specific MHC-II is associated with immune exclusion in cancer patients, especially those treated with immunotherapy. As shown in Fig. 5D, TNFAIP2 was positively correlated with most MHC genes, which suggested that it is involved in the antigen presentation process. Chemokines and chemokine receptors extensively mediate intercellular signal transduction. Correlation analyses revealed thatTNFAIP2 was commonly positively associated with these genes in SKCM, indicating that TNFAIP2 facilitates the immune response (Fig. 5E–G). These results indicate that TNFAIP2 plays a significant role in remodelling the TME and might be a potential therapeutic target in SKCM.

TNFAIP2 could active the antitumor immunity in SKCM. (A) Correlations of TNFAIP2 with immune score and stromal score. (B) Correlations of TNFAIP2 with six immune cell subtypes estimated using ssGSEA algorithm. (C) Correlations of TNFAIP2 with immune checkpoint genes. (D) Correlations of TNFAIP2 with MHC genes. (E–G) Correlations of TNFAIP2 with chemokines and chemokine receptors. MHC, major histocompatibility complex. *P < 0.05. **P < 0.01. ***P < 0.001.
TNFAIP2 upregulation predicts a favourable immunotherapy response in SKCM patients
Following the immune infiltration analysis, we investigated the impact of TNFAIP2 on the response to ICB treatment. The Tumor immune dysfunction and exclusion (TIDE) database was used to predict the immunotherapy response on the basis of existing biomarkers, including microsatellite instability (MSI), CD274 (PD-L1), and CD8, and on TNFAIP2 expression. In five melanoma samples, one glioblastoma sample and one non-small cell lung cancer sample, the predictive performance of TNFAIP2 was comparable to that of CD8, with AUC values greater than 0.7, which indicated favourable immunotherapy response prediction accuracy (Fig. 6A). In particular, its high expression implied a favourable ICB treatment response in melanoma. Survival analyses revealed that high TNFAIP2 expression was associated with superior OS in patients with melanoma treated with anti-CTLA-4 blockade in the Nathanson and VanAllen cohorts (Fig. 6B). In melanoma cohorts treated with anti-PD-1 inhibitors, including the Riaz, Gide, and Liu cohorts, TNFAIP2 upregulation improved patient OS (Fig. 6C). Moreover, on the basis of the transcriptome data from TCGA and GEO (GSE59455, GSE54467, and GSE8401) datasets, patients with high TNFAIP2 expression also had a favourable ICB response (Fig. 6D). Therefore, these results indicate that TNFAIP2 upregulation might promote the immunotherapy response to SKCM.

TNFAIP2 upregulation predicts favourable ICB treatment response in SKCM. (A) The immunotherapy response predictive effect of TNFAIP2 compared to other existing markers. (B–D) Survival curves based on different cohorts underwent ICB treatment as indicated. ICB, immune checkpoint blockade. AUC, area under receiver operating characteristic curve. MSI, microsatellite instability.
TNFAIP2 inhibits the proliferation and lung metastasis of SKCM cells in vivo
To validate the ability of TNFAIP2 to inhibit cell proliferation and migration in vivo, we constructed a xenograft model by inoculating A375 cells transduced with TNFAIP2-overexpressing lentivirus or vector into BALB/c nude mice (Fig. 7A). Consistent with the in vitro findings, TNFAIP2 overexpression decreased the tumor burden (Fig. 7B–D), which was verified by Ki67 staining (Fig. 7E–F). To investigate the ability of TNFAIP2 to inhibit cell migration in vivo, we used a tail vein injection mouse model (Fig. 7G). TNFAIP2 overexpression alleviated A375 cell lung metastasis (Fig. 7H–J). Taken together, these data demonstrate that TNFAIP2 inhibits the proliferation and lung metastasis of SKCM cells in vivo.

TNFAIP2 inhibits the proliferation and lung metastasis of SKCM in vivo. (A) BALB/c nude mice (n = 5) were subcutaneously inoculated with A375 cells. (B) Xenograft tumor images in BABL/c nude mice. (C–D) Tumor volume curves and tumor weights in BABL/c nude mice. (E–F) Representative images and qualification of Ki67 staining in xenografts with or without TNFAIP2 overexpression. Scale bars, 100 μm. (G) BALB/c nude mice (n = 5) were subjected to tail vein injection of A375 cells. (H–I) Representative images of lung tissues (red arrows) and H&E staining (black arrows). Scale bars, 100 μm. (J) Qualification of lung metastasis nodules. s.c., subcutaneous injections. H&E, haematoxylin and eosin. *P < 0.05. **P < 0.01. ***P < 0.001.
TNFAIP2 improves immunocompetence and anti-PD-1 therapy response in SKCM
To verify the immunoregulatory potential of TNFAIP2, we constructed a xenograft model by inoculating B16 cells transduced with Tnfaip2-overexpressing lentivirus or vector into C57BL/6 mice (Fig. 8A). The results revealed greater tumor suppression in this model than in the BALB/c nude mouse model, which suggested that T cells might participate in the antitumor effects of TNFAIP2 (Fig. 8B–D). We subsequently conducted flow cytometry to profile alterations in the TME. Our results revealed significantly increased infiltration of CD8+ T cells and M1 macrophages (Fig. 8E and Fig. S3A) but decreased infiltration of Treg cells and M2 macrophages in Tnfaip2-overexpressing tumors (Fig. 8F and Fig. S3B). Considering that CD8+ T cells are the primary antineoplastic cell type, we systematically depleted CD8+ T cells, and the antitumor effect of TNFAIP2 was significantly abolished (Fig. 8G-J). TNFAIP2 expression was correlated with macrophage infiltration (Fig. 5B), and M1 macrophages were the primary source of TNFα in the TME. Moreover, TNFAIP2 is a direct downstream target of TNFα, and we hypothesized that macrophages are involved in the antitumor effect of TNFAIP2. As expected, the clearance of macrophages by clodronate liposomes also partially abolished the antitumor effect (Fig. S3C-F).
According to the bioinformatics analyses and experimental results, we speculated that TNFAIP2 can improve the response of SKCM to ICB treatment. In the anti-PD-1 Ab treatment xenograft model (Fig. 8K), Tnfaip2 overexpression resulted in a more significant tumor inhibition effect than monotherapy (Fig. 8L), and this effect was quantified according to the tumor volume and weight (Fig. 8M-N). Collectively, the above results provide solid evidence of the role of TNFAIP2 in promoting SKCM suppression and the response to ICB therapy.

TNFAIP2 improves the immunocompetence and anti-PD-1 therapy response in SKCM. (A) C57BL/6 mice (n = 5) were subcutaneously inoculated with B16 cells. (B) Xenograft tumor images in C57BL/6 mice. (C-D) Tumor volume curves and tumor weights in C57BL/6 mice. (E–F) Flow cytometry detected CD8+ T cells and Treg cells in respective groups. (G) C57BL/6 mice (n = 5) with CD8+ T cells depletion were subcutaneously inoculated with B16 cells (CD8α antibody, 250 µg/mouse, i.p. every 5 days). (H) Xenograft tumor images in C57BL/6 mice with CD8+ T cells depletion. (I–J) Tumor volume curves and tumor weights in C57BL/6 mice with CD8+ T cells depletion. (K) C57BL/6 mice (n = 5) were subcutaneously inoculated with B16 cells and treated with anti-PD-1 mAb (120 µg/mouse, i.p. every 3 days). (L) Xenograft tumor images in C57BL/6 mice treated with anti-PD-1 mAb. (M–N) Tumor volume curves and tumor weights in C57BL/6 mice treated with anti-PD-1 mAb. s.c., subcutaneous injections. i.p., intraperitoneal injections. mAb, monoclonal antibody. *P < 0.05. ***P < 0.001.
Discussion
Malignant tumors are difficult to treat due to the presence of a complex TME, in which immune cells play elusive roles ranging from antitumorigenic to tumorigenic18,19. Tumor cells can evade or hijack immune cells to coordinate with the immunosuppressive TME, but the exact mechanism is still undetermined. Our previous study demonstrated the function of TNFAIP2 in cisplatin resistance and metastasis13,14. However, its immunoregulatory function is largely unknown. In this study, the immune signature of TNFAIP2 was explored in SKCM. TNFAIP2 expression was closely correlated with the proportions of many immunoregulatory cells, including CD8+ T cells, regulatory T (Treg) cells and macrophages, according to bioinformatics predictions and in vivo validation experiments. Moreover, Tnfaip2 overexpression significantly increased the efficacy of anti-PD-1 Ab treatment. The above results highlight the role of TNFAIP2 in promoting SKCM suppression and the response to ICB therapy.
TNFAIP2 is expressed in human umbilical vein endothelial cells stimulated with TNFα and belongs to the Sec6 family10,20. Previous studies have shown that it tends to promote tumor progression. In nasopharyngeal carcinoma, TNFAIP2 is transcriptionally induced by latent membrane protein 1 and promotes cell migration12. In breast cancer, TNFAIP2 affects the integrin β4-mediated IQGAP1/RAC1 axis and promotes DNA damage-related drug resistance21. However, the present results revealed its tumor-suppressive role in SKCM. According to the in vitro and in vivo results in BALB/c nude mice, TNFAIP2 overexpression decreased tumor size. However, this inhibitory effect was even more pronounced in immunocompetent mice, and CD8+ T cells depletion partly abolished the tumor-suppressive effect of TNFAIP2. Therefore, we concluded that the function of TNFAIP2 is highly dependent on T cells infiltration. Notably, our IHC and immunofluorescence results revealed partial nuclear translocation of TNFAIP2 in tumor cells but not melanocytes. We hypothesized that this localization may lead to activation of several tumor suppressor signalling pathways or suppression of tumor immunogenicity, which impacts its tumor-suppressive role. More experiments are needed to clarify this speculation.
Macrophages account for most myeloid cells and exhibit diverse functional states22. In mice, perivascular CD163+ macrophages express alternative activation markers, whereas some CD163lo macrophages activate inflammatory pathways in necrotic tumor regions23. In colorectal cancer, Zhang et al.24 found that the colorectal adenoma and metastatic liver cancer pathways were specifically enriched in the SPP1+ macrophage subgroup, implying that these pathways have protumorigenic and prometastatic characteristics. In this study, our results revealed a close correlation between TNFAIP2 expression and M1 macrophage polarization; thus, TNFAIP2 may promote antigen delivery and the production of a series of molecules, such as nitric oxide, reactive oxygen species and inflammatory factors, including TNFα and IL-12, that directly or indirectly kill tumor cells. Notably, M1 macrophages are the main source of TNFα, the secretion of which can increase TNFAIP2 synthesis and form a positive feedback loop to inhibit tumor progression. Further experiments are needed to elucidate the exact mechanism by which TNFAIP2 exerts antitumor effects via M1 macrophages.
Anti-PD-1/PD-L1 immunotherapy has shown remarkable clinical efficacy, especially in advanced or unresectable SKCM. However, the response rate of less than 30% indicates that this approach does not meet the treatment demand, and most patients inevitably develop acquired resistance over time. Therefore, it is necessary to further dissect the immunological characteristics related to the response and drug resistance of the TME to improve the response to anti-PD-1 monotherapy. Previous studies have demonstrated that sufficient CD8+ T cells infiltration and activation are preconditions for a durable therapeutic response25,26,27. Klement et al. demonstrated that tumor cell PD-L1 can engage myeloid cell PD-1 to activate SHP2 to suppress T cells recruitment28. Moreover, mitochondrial dysfunction-induced glycolytic reprogramming could facilitate terminal exhausted T cells transition. Therefore, metabolic engineering of T cells might be a promising strategy to increase the stemness and functionality of precursor T cells for cancer immunotherapy29. The present study preliminarily revealed a positive relationship between TNFAIP2 and CD8+ T cells abundance, but the exact mechanism remains unclear. We hypothesized that the expression of multiple chemokines and receptors might contribute to the infiltration and activity of CD8+ T cells. This specific mechanism will be explored in our future studies.
In conclusion, the expression pattern, prognostic value, and molecular function of TNFAIP2 in SKCM were determined via multiomics and experimental analyses. The close relationship of TNFAIP2 with different infiltrating immune cells and ICB treatment outcomes indicate that TNFAIP2 might be an indicator of a favourable immunotherapy response or a potential treatment target. In-depth mechanistic research is worth conducting in the future.
Materials and methods
Data extraction and analysis
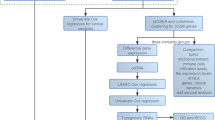
Transcriptome data were derived from GENT2 (http://gent2.appex.kr/gent2/), TCGA (https://www.portal.gdc.cancer.gov/) and GEO (https://www.ncbi.nlm.nih.gov/gds/) database. The potential interacted proteins with TNFAIP2 were determined by GeneMANIA (http://genemania.org/). Bioinformatics analyses were conducted using R Studio and R packages including limma, pheatmap, ggpubr, clusterProfiler, org.Hs.eg.db, ggplot2, survival, survminer, and forestploter to determine the differential expressed genes, associated signalling pathways, and prognosis characteristics in SKCM. The Immune infiltration estimation was conducted using “ESTIMATE” and “ssGSEA” algorithm.
Immunotherapy response prediction
The immunotherapy response was evaluated by TIDE (http://tide.dfci.harvard.edu/)30, which comprehensively analysed the tumor immune escape and exclusion mechanism, so as to effectively predict the treatment effect of ICB.
Clinical specimen collection
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and informed consent was taken from all the patients. A total of 20 normal skin and 86 SKCM tissues were incorporated in this study. The demographic and clinical characteristics were displayed in Table S1. Our research was approved by the Ethic Committee of the Second Hospital of Shandong University (No. KYLL2023016).
IHC
The paraffin-embedded sections underwent deparaffinization, dehydration and antigen retrieval. After natural cooling to room temperature, primary antibodies (TNFAIP2, Santa Cruz, sc-28318) were incubated overnight. After flush, secondary antibodies (MXB Biotechnologies, Kit-5010) incubation, slides developed colour using 3,3-N-diaminobenzidine tetrahydrochloride (DAB, YEASEN, 36201ES03) for the indicated times. Finally, counterstaining, differentiation and mounting were performed.
Staining score evaluation
Two pathologists evaluated the staining score independently. The positive staining scope score was divided into 4 grades: 0 to 1 (0-25%), 1 to 2 (26-50%), 2 to 3 (51-75%), and 3 to 4 (76-100%). The staining intensity score was evaluated based on following criteria: 0, no appreciable staining; 1, weak intensity (light yellow); 2, moderate intensity (yellow‒brown); 3, strong intensity (brown). The staining score was calculated as the score positive staining scope × the staining intensity score.
Cell culture and transfection
The keratinocytes, HaCat, and normal melanocytes, PIG1 (American Type Culture Collection, ATCC, Manassas, VA, USA), were cultured in Dulbecco’s modified Eagle’s medium (DMEM, Gibco) containing 10% fetal bovine serum (FBS, Cellmax). The melanoma cell lines, A375 and B16 (ATCC, Manassas, VA, USA), were cultured in high glucose (4.5 g/L) DMEM (Gibco) or RPMI 1640 (Gibco) medium containing 10% FBS (Cellmax) under 5% CO2 atmosphere. The overexpression and short hairpin RNA (shRNA) lentivirus were synthesized by Cas9X™ and transfected according to the manufacturer instructions. The shRNA sequences were 5′-GGATGTCCATGGAGCAGAATT-3′ for TNFAIP2 (human species), 5′-GGACACCACGGGCTCTGTAAG-3′ for Tnfaip2 (mouse).
Western blot (WB) and Real-time quantitative polymerase chain reaction (RT-qPCR)
The WB and RT-qPCR were conducted as our previous study description. The antibody and primer sequences were displayed in Table S2 and S3.
Cell viability assays
Approximately 2000 cells with indicated treatment were seed into 96-well plates in quintuplicate. The CCK-8 kit (Dojindo, Japan) was compounded with DMEM in 1:9 ratio. Each group was then incubated in the mixed solution for 2 h. The absorbance was measured by using a spectrophotometer microplate reader (Multiskan MK3, Thermo) at 450 nm wavelength.
Cell proliferation
Cell proliferation was evaluated using the Cell-Light™ EdU Apollo In Vitro Kit (RiboBio) according to the manufacturer’s instructions. In brief, approximately 1 × 105 cells with indicated treatment were seeded in 96-well plates. After adherence, cells were incubated with EdU medium for 2 h and fixed with 4% paraformaldehyde (Biosharp) for 30 min. Then, cells were permeabilized with 0.5% Triton X-100 (Beyotime) for 10 min. Subsequently, 1×Apollo® staining solution was added and incubated for 30 min avoid light at room temperature. Finally, 1×Hoechst 33,342 reaction solution was added to incubate for 30 min and photographed using a microscope (Leica Microsystems) avoid light at room temperature.
Wound healing
Cells were cultured in 6-well plates and straight wounds were generated by 200 µl pipette tips. After removed exfoliated cells, complete medium was added followed by photographed immediately and at 24 h. The formula for calculating mobility was as follows: migration ratio = [(gap width at 0 h) − (gap width at 24 h)]/ (gap width at 0 h) ×100.
SKCM mouse model construction and management
The BALB/c nude and C57BL/6 mice (Beijing Vital River Laboratory) were housed in standard specific-pathogen-free (SPF) conditions. All treatments were designed to minimize mice suffering. To construct SKCM mouse model, 1 × 106 A375 or 5 × 105 B16 tumor cells (100 µl) were subcutaneously flank inoculated per mouse (N = 5 in each group). For CD8+ T cells or macrophages depletion, 250 µg anti-CD8 Abs (Bio X Cell, West Lebanon, NH, USA) or 200 µl clodronate liposomes (FormuMax, F70101C-AC) were administered intraperitoneally once every 5 days per mouse. For the ICB therapy in SKCM mouse model, an anti-mouse PD-1 Ab (Bio X Cell, West Lebanon, NH, USA) was intraperitoneally injected 5 days after the tumor cells inoculation at a dose of 120 µg/mouse once every 3 days. The diameters were measured every 3 days using vernier caliper after tumors were palpable. The tumor volumes were calculated as 0.54×length×width2 and confirmed the maximal tumor burden were not exceeded 2000mm3 according to the ethics committee. For the lung metastasis model construction, 1 × 106 A375 cells (100 µl) were injected via BALB/c nude mice tail vein. After 4 weeks, lung tissues were harvested for haematoxylin and eosin (H&E) staining. The mice were euthanized by excessive isoflurane anaesthesia. Our animal experiments were approved by the Ethic Committee of the Second Hospital of Shandong University (No. KYLL2023016) and conducted in accordance with the institutional guidelines and regulations. The study was carried out in compliance with the ARRIVE guidelines.
Flow cytometry
The tumors were resected at the end of the in vivo experimental period. Single-cell suspensions were obtained from fresh tumor tissues by incubation with a mixture of RPMI 1640 medium containing 2% FBS, 3mM CaCl2, 200U/ml collagenase (17104019, Thermo Fisher Scientific), and 10 µg/ml DNase (D5025, Sigma‒Aldrich) with shaking at 200 rpm and 37 °C for 1 h. Invitrogen LIVE/DEAD Fixable Dead Cell Stain was used to distinguish dead cells, and live cells were further incubated with an anti-CD16/CD32 Ab for 30 min to block Fc-mediated reactions. To analyse immune cell infiltration, CD45, CD3, CD4, CD8, Foxp3, F4/80, CD86 and CD206 proteins on the cell surface were stained. The antibodies were displayed in Table S2. All samples were analysed using a Fortessa cell analyser (BD Biosciences), and the data were analysed using FlowJo software (v10.4).
Statistical analysis
All experiments were performed at least three times and data were represented as the means ± SEM. Comparisons were performed using Student’s t-test between two groups and ANOVA in multi-groups. Survival analyses were conducted using the KM method and Cox proportional hazard model. The genes correlations were evaluated using Pearson correlation coefficient with the normal distribution test. Statistical analyses were conducted using GraphPad Prism 8 and R studio software. A two-sided P value < 0.05 was considered to be statistical significance. Levels of significance were denoted as N.S., no significance, *P < 0.05, ** P < 0.01, and *** P < 0.001.
Data availability
The datasets used during the current study are available from the corresponding author on reasonable request. Public datasets analyzed in this study are available in TCGA database (https://www.portal.gdc.cancer.gov/), GEO database (https://www.ncbi.nlm.nih.gov/gds/, GSE25099, GSE39366,GSE103512, GSE196723, GSE103512, GSE164760, GSE73731, GSE103512, GSE121931, GSE32507, GSE82208, GSE188256, GSE100935, GSE53462, GSE87437, GSE29695, GSE32507), TIMER 2.0 (http://timer.cistrome.org), SangerBox 3.0 (http://www.sangerbox.com/tool), UALCAN (http://ualcan.path.uab.edu), TISIDB (http://cis.hku.hk/TISIDB), TIDE (http://tide.dfci.harvard.edu/), and GeneMANIA (http://genemania.org/). The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
16 November 2025
A Correction to this paper has been published: https://doi.org/10.1038/s41598-025-26656-z
Abbreviations
- SKCM:
-
Skin cutaneous melanoma
- TME:
-
Tumor microenvironment
- TNFα:
-
Tumor necrosis factor α
- TNFAIP2:
-
TNFα-induced protein 2
- TCGA:
-
The cancer genome atlas
- GEO:
-
Gene expression omnibus
- ICB:
-
Immune checkpoint blockade
- KEAP1:
-
Kelch-like ECH-associated protein 1
- NRF2:
-
Nuclear factor, erythroid 2-like 2
- AUC:
-
Area under receiver operating characteristic curve
- OS:
-
Overall survival
- DSS:
-
Disease special survival
- IHC:
-
Immunohistochemistry
- EDU:
-
5-Ethynyl-2′-deoxyuridine
- GO:
-
Gene ontology
- KEGG:
-
Kyoto encyclopaedia of genes and genomes
- GSEA:
-
Gene set enrichment analysis
- MHC:
-
Major histocompatibility complex
- SPF:
-
Specific-pathogen-free
- MSI:
-
Microsatellite instability
- H&E:
-
Haematoxylin and eosin
References
Arnold, M. et al. Global burden of cutaneous melanoma in 2020 and projections to 2040. JAMA Dermatol. 158, 495–503. https://doi.org/10.1001/jamadermatol.2022.0160 (2022).
Long, G. V., Swetter, S. M., Menzies, A. M., Gershenwald, J. E. & Scolyer, R. A. Cutaneous melanoma. Lancet (London England) 402, 485–502. https://doi.org/10.1016/s0140-6736(23)00821-8 (2023).
Lee, T. L., Liao, Y. H., Liau, J. Y. & Sheen, Y. S. Risk factors of recurrence and distant metastasis in primary cutaneous melanoma in Taiwan. Sci. Rep. 11, 21012. https://doi.org/10.1038/s41598-021-00386-4 (2021).
Xiao, Y. & Yu, D. Tumor microenvironment as a therapeutic target in cancer. Pharmacol. Ther. 221 https://doi.org/10.1016/j.pharmthera.2020.107753 (2021).
Xiao, Z., Dai, Z. & Locasale, J. W. Metabolic landscape of the tumor microenvironment at single cell resolution. Nat. Commun. 10, 3763. https://doi.org/10.1038/s41467-019-11738-0 (2019).
Rui, R., Zhou, L. & He, S. Cancer immunotherapies: Advances and bottlenecks. Front. Immunol. 14, 1212476. https://doi.org/10.3389/fimmu.2023.1212476 (2023).
Szeto, G. L. & Finley, S. D. Integrative approaches to cancer immunotherapy. Trends Cancer 5, 400–410. https://doi.org/10.1016/j.trecan.2019.05.010 (2019).
Liao, W. et al. KRAS-IRF2 axis drives immune suppression and immune therapy resistance in colorectal cancer. Cancer Cell 35, 559–572e557. https://doi.org/10.1016/j.ccell.2019.02.008(2019).
Pozniak, J. et al. A TCF4-dependent gene regulatory network confers resistance to immunotherapy in melanoma. Cell 187, 166–183e125. https://doi.org/10.1016/j.cell.2023.11.037 (2024).
Rusiniak, M. E., Yu, M., Ross, D. T., Tolhurst, E. C. & Slack, J. L. Identification of B94 (TNFAIP2) as a potential retinoic acid target gene in acute promyelocytic leukemia. Cancer Res. 60, 1824–1829 (2000).
Jia, L. et al. KLF5 promotes breast cancer proliferation, migration and invasion in part by upregulating the transcription of TNFAIP2. Oncogene 35, 2040–2051. https://doi.org/10.1038/onc.2015.263 (2016).
Chen, C. C. et al. NF-κB-mediated transcriptional upregulation of TNFAIP2 by the Epstein-Barr virus oncoprotein, LMP1, promotes cell motility in nasopharyngeal carcinoma. Oncogene 33, 3648–3659. https://doi.org/10.1038/onc.2013.345 (2014).
Xu, T. et al. TNFAIP2 confers cisplatin resistance in head and neck squamous cell carcinoma via KEAP1/NRF2 signaling. J. Experimental Clin. cancer Research: CR. 42, 190. https://doi.org/10.1186/s13046-023-02775-1 (2023).
Xu, T. et al. TNFAIP2 promotes NF-κB signaling mediate lymph node metastasis of oral squamous cell carcinoma by protecting IKKβ from ubiquitin proteasome degradation. Cell. Communication Signaling: CCS. 23, 83. https://doi.org/10.1186/s12964-025-02077-3 (2025).
Wang, Y., Chen, Y., Zhu, B., Ma, L. & Xing, Q. A. Novel nine apoptosis-related genes signature predicting overall survival for kidney renal clear cell carcinoma and its associations with immune infiltration. Front. Mol. Biosci. 8, 567730. https://doi.org/10.3389/fmolb.2021.567730 (2021).
Hou, C. et al. Targeting TNFAIP2 induces immunogenic cell death and sensitizes glioblastoma multiforme to anti-PD-1 therapy. J. Neuro-Oncol. 165, 79–90. https://doi.org/10.1007/s11060-023-04449-6 (2023).
Warde-Farley, D. et al. The genemania prediction server: Biological network integration for gene prioritization and predicting gene function. Nucleic Acids Res. 38, W214–W220. https://doi.org/10.1093/nar/gkq537 (2010).
Gou, Q. et al. PPARγ inhibited tumor immune escape by inducing PD-L1 autophagic degradation. Cancer Sci. 114, 2871–2881. https://doi.org/10.1111/cas.15818 (2023).
Jiang, X. et al. Role of the tumor microenvironment in PD-L1/PD-1-mediated tumor immune escape. Mol. Cancer 18 https://doi.org/10.1186/s12943-018-0928-4 (2019).
Wolf, F. W. et al. B94, a primary response gene inducible by tumor necrosis factor-alpha, is expressed in developing hematopoietic tissues and the sperm acrosome. J. Biol. Chem. 269, 3633–3640 (1994).
Fang, H. et al. Integrin β4 promotes DNA damage-related drug resistance in triple-negative breast cancer via TNFAIP2/IQGAP1/RAC1. eLife 12. https://doi.org/10.7554/eLife.88483 (2023).
Engblom, C., Pfirschke, C. & Pittet, M. J. The role of myeloid cells in cancer therapies. Nat. Rev. Cancer 16, 447–462. https://doi.org/10.1038/nrc.2016.54 (2016).
Etzerodt, A. et al. Specific targeting of CD163(+) TAMs mobilizes inflammatory monocytes and promotes T cell-mediated tumor regression. J. Exp. Med. 216, 2394–2411. https://doi.org/10.1084/jem.20182124 (2019).
Zhang, L. et al. Single-cell analyses inform mechanisms of myeloid-targeted therapies in colon cancer. Cell 181, 442–459e429. https://doi.org/10.1016/j.cell.2020.03.048 (2020).
Meng, Y. et al. Immunosuppressive CD10(+)ALPL(+) neutrophils promote resistance to anti-PD-1 therapy in HCC by mediating irreversible exhaustion of T cells. J. Hepatol. 79, 1435–1449. https://doi.org/10.1016/j.jhep.2023.08.024 (2023).
de Ruiz, M. et al. β-catenin activation promotes immune escape and resistance to Anti-PD-1 therapy in hepatocellular carcinoma. Cancer Discov. 9, 1124–1141. https://doi.org/10.1158/2159-8290.Cd-19-0074 (2019).
Verma, V. et al. PD-1 blockade in subprimed CD8 cells induces dysfunctional PD-1(+)CD38(hi) cells and anti-PD-1 resistance. Nat. Immunol. 20, 1231–1243. https://doi.org/10.1038/s41590-019-0441-y (2019).
Klement, J. D. et al. Tumor PD-L1 engages myeloid PD-1 to suppress type I interferon to impair cytotoxic T lymphocyte recruitment. Cancer Cell. 41, 620–636e629. https://doi.org/10.1016/j.ccell.2023.02.005 (2023).
Wu, H. et al. Mitochondrial dysfunction promotes the transition of precursor to terminally exhausted T cells through HIF-1α-mediated glycolytic reprogramming. Nat. Commun. 14, 6858. https://doi.org/10.1038/s41467-023-42634-3 (2023).
Fu, J. et al. Large-scale public data reuse to model immunotherapy response and resistance. Genome Med. 12 https://doi.org/10.1186/s13073-020-0721-z (2020).
Acknowledgements
We thank W.Z. and Y.L. for reagents and helpful discussions.
Funding
This study was supported by China Postdoctoral Science Foundation (2024M751825).
Author information
Authors and Affiliations
Contributions
T.X. conceived the project. T.X., Y.W., J.W. and Z.C. performed experiments. T.X. and C.Z. performed bioinformatics analysis. T.X. and H.L. interpreted and analysed data. T.X. and Y.W. wrote the manuscript with comments from all authors. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
Our research was conducted in accordance with the Declaration of Helsinki (as revised in 2013) with informed consent signed by all incorporated patients. Our animal experiments were approved by the Ethic Committee of the Second Hospital of Shandong University (No. KYLL2023016) and conducted in accordance with the institutional guidelines and regulations. The study was carried out in compliance with the ARRIVE guidelines.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in Figure 3. Full information regarding the corrections made can be found in the correction for this Article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Y., Wang, J., Chen, Z. et al. TNFAIP2 deficiency drives formation of an immunosuppressive tumor microenvironment and confers resistance to anti-PD-1 therapy in skin cutaneous melanoma. Sci Rep 15, 25569 (2025). https://doi.org/10.1038/s41598-025-10952-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-10952-9
