
Abstract
This assessor-blinded randomized trial was designed to evaluate the effects of aerobic exercise, resistance training, and traditional Chinese gong methods on the quality of life (QoL) of older adults aged 66–96 years living in a nursing facility. Seventy - eight participants, who were over 65 years old, free from severe heart disease, asthma, and other conditions specified in the exclusion criteria, were randomly allocated into three groups to receive 12–24 weeks of different exercise interventions. The SF − 36 Health Survey Scale was employed to assess QoL before the intervention and 12 and 24 weeks after it. The results indicated that all three exercise modalities significantly increased the SF − 36 total score. The aerobic exercise group demonstrated improvements in Physical Component Summary (PCS), Mental Component Summary (MCS), Role Physical(RP), and Role Emotional (RE). The resistance training group showed enhancements in MCS, Physical Functioning (PF), Social Functioning (SF), RE, and Mental Health (MH). The traditional gong group achieved progress in PCS, MCS, PF, RP, Bodily Pain (BP), and Vitality (VT). In summary, all three exercise types effectively enhanced the QoL of older adults. Aerobic and resistance training were beneficial for both physical and psychological aspects, while traditional gong methods mainly had a positive impact on physical functioning. Although the study lacked a non-intervention control group, based on these results, this study not only provides a scientific basis for the development of exercise intervention programs for the elderly but also offers practical suggestions for designing exercise plans, contributing to promoting healthy aging.
Trial registration: The Chinese Clinical Trial Registry on 19/10/2022, (ChiCTR2200064801).
Similar content being viewed by others
Introduction
The aging population has become a prominent feature of today’s society, and with demographic shifts, increasing attention is being paid to the quality of life of older adults1. The World Health Organization defines quality of life as an individual’s perception of their position in life in relation to their goals, expectations, standards, and concerns2. This concept encompasses not only physical health, but also a wide range of psychological, social, economic, and environmental factors. Quality of life (QoL) in older adults is not merely a marker of individual well-being but a critical determinant of healthy aging3. Compared to earlier life stages, the vulnerability of QoL in older populations is amplified by cumulative health burdens (e.g., multimorbidity and functional decline), heightened psychological risks from social isolation, and substantial economic costs to healthcare systems4,5,6,7. The World Health Organization further prioritizes QoL as a central pillar of aging policies, emphasizing that maintaining functional capacity in later life is essential to mitigate societal caregiving pressures and achieve sustainable development goals2.
Several tools have been developed to assess the quality of life in older adults, with the Short Form-36 (SF-36) health survey being one of the most widely used globally due to its reliability and validity8. The SF-36 scale, consisting of eight dimensions, provides a comprehensive reflection of the physical and psychological health of older adults and serves as an important tool for both clinical and research purposes9,10. In this study, we used the Chinese version of the SF-36, which was adapted by Chinese scholar Li Lu et al. to better suit the context of the elderly population in China11. Previous studies in China have validated the use of the Chinese version of the SF-36, demonstrating its applicability and reliability in assessing the QoL of older adults in this region12,13.
Quality of life (QoL) encompasses multidimensional domains, including physical health, psychological well-being, and social functioning. Different exercise modalities may exert heterogeneous effects on these dimensions, necessitating systematic comparisons. Although extensive evidence supports the positive impact of exercise on QoL in older adults, the specific benefits vary substantially across exercise types. For instance, aerobic exercise has been demonstrated to enhance cardiorespiratory fitness, mental health, and overall QoL13,14,15,16. Furthermore, longitudinal studies indicate that sustained aerobic training improves cognitive performance and psychological status in aging populations17.Resistance training not only augments muscle strength (particularly in upper and lower extremities), balance capacity, and grip strength in older adults but also reduces risks of anxiety and depressive symptoms,18,19,20,21,22,23, underscoring its dual benefits in physical and mental health domains. Traditional Chinese exercises, such as Gong (e.g., Tai Chi and Daoyin), have shown efficacy in improving physical function, mitigating stress, and enhancing sleep quality24–26. Emerging evidence further suggests that traditional Chinese exercises may modulate neural activity to improve cognitive performance and potentially delay the onset of neurodegenerative disorders like dementia27.
This study aims to address this research gap by comparing the effects of 12 to 24 weeks of aerobic exercise, resistance training, and traditional Chinese gong methods on SF-36 scores in older adults. The rationale for choosing these three exercise modalities is based on their distinct mechanisms of action and potential benefits. Aerobic exercise is known for its cardiovascular benefits, resistance training for its musculoskeletal advantages. The presence of traditional Chinese gong methods as a study variable is justified by its unique potential benefits that differ from those of aerobic and resistance training. Traditional Chinese exercise, such as Daoyin, emphasize a holistic approach, integrating physical movements, breathing exercises, and mental focus. These exercises are culturally significant, especially in China. Given the aging population’s increasing interest in culturally adapted, comparing Daoyin with more widely studied exercise modalities like aerobic and resistance training provides valuable insight into alternative exercise approaches that may be more accessible and acceptable to older adults.
By comparing these modalities, we aim to provide a comprehensive understanding of their respective impacts on QoL. The findings will provide a scientific basis for developing effective exercise interventions to improve quality of life and promote healthy aging in older adults.
Metohds and analysis
The study used the CONSORT reporting guidelines28.
Design
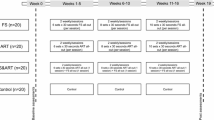
This study was designed as an assessor-blinded randomized controlled trial with a parallel-group design. Participants were then randomly assigned to one of three groups in a 1:1:1 ratio. Each group underwent a 24-week intervention with one of the three exercise modalities. Quality of life assessments were conducted at baseline, as well as after 12 and 24 weeks of intervention. The differences between pre- and post-intervention scores were analyzed. The detailed procedure is outlined in Fig. 1.

Detailed overview of the research program.
Participant recruite
Participant recruitment for the aerobic and resistance training groups was conducted from July 2021 to August 2021, while recruitment for the traditional gong group occurred from May 2023 to June 2023. All participants were enrolled from a community-based nursing facility in Langfang City, Hebei Province, China. Subjects were screened based on questionnaires, outpatient medical records, and hospitalization records. The inclusion criteria were: (1) age 65 years or older; (2) no serious heart disease, asthma, or other underlying conditions; the ability to walk independently and perform exercise and physical fitness tests; (3) clear consciousness, sufficient cognitive ability, and the capacity to respond to questions from the testers. Exclusion criteria included: patients with severe hypertension (SBP > 160 mmHg, DBP > 95 mmHg), serious diabetic complications affecting the heart, brain, kidneys, or eyes, severe lower limb joint diseases or other conditions making exercise unsuitable, and patients with a history of mental illness or a family history of mental disorders.
The delayed recruitment of the traditional gong group was due to logistical constraints and intermittent public health restrictions related to the COVID-19 pandemic, which affected access to the facility and training staff availability. However, the intervention was conducted during a period of relative pandemic stability in China, with minimal restrictions and no reported infections among participants or staff. Recruitment criteria, setting, assessment tools, and intervention procedures were kept consistent across all three groups to minimize the potential impact of temporal heterogeneity.
A total of 78 elderly participants from the senior center were included in the study and randomly assigned to three groups of 26 participants each, according to the 1:1:1 ratio. The basic demographic information of the participants is provided in Table 1.
Sample size
Based on previous research and expected effect sizes, we used G*Power software to calculate the sample size. Assuming an effect size of 0.5, a significance level of α = 0.05, and a statistical power of 80%, we determined that 78 participants were required. Considering a potential dropout rate of 15%, 26 participants were allocated to each group. The basis for the sample size calculation included references to similar studies in the field of exercise interventions for older adults29,30.
Randomization
Sequence Generation: The randomization sequence was generated using a computer-generated random number table created in R software. Participants were assigned to one of the three intervention groups: aerobic exercise, resistance training, or traditional gong.
Allocation concealmen: The random allocation sequence was maintained by a research assistant using a sealed, opaque envelope method. Each envelope was opened only after a participant had provided informed consent and completed the baseline assessment. Although participants and intervention providers were aware of the group assignments, the outcome assessors remained blinded throughout the study to minimize assessment bias. This design aligns with the assessor-blinded randomized controlled trial framework employed in this study.
Implementation: The randomization sequence was generated by an independent statistician who had no involvement in the implementation or data collection. Participant group assignments were carried out by trained research assistants. While participants and intervention staff were aware of the group assignments, the primary investigators responsible for outcome assessment were blinded to group allocation throughout the intervention period, consistent with the assessor-blinded design of this trial.
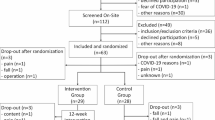
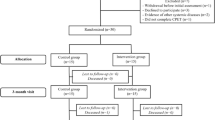
Participant flow diagram
Figure 2 in this manuscript likely presents the participant flow diagram, detailing the recruitment, allocation, and intervention process in the study. It illustrates the stages from screening to randomization, and outlines how participants were assigned to the aerobic exercise, resistance training, and traditional gong groups. The Fig. 2 highlights participant numbers at each phase and indicates any dropouts or exclusions from the study.

CONSORT flow diagram of participant progress through the phases of the trial.
Exercise intervention
In this study, aerobic exercise, resistance exercise, and traditional gong interventions were implemented through walking, chair-based elastic band exercises, and guided health maintenance gong, respectively. Participants continued their usual lifestyle habits while undergoing the exercise interventions. The SF-36 scale was administered at the end of both the 12-week and 24-week interventions. The specific SF-36 scale items and details are provided in Table 2.
Aerobic exercise group
Based on each participant’s heart rate intensity range, a personalized walking exercise program was developed, determining the appropriate walking speed interval. A 24-week walking exercise intervention was conducted, with the experiment staff monitoring the participants’ safety throughout the process. Prior to the start of each exercise, the experimenter distributed sports watches to the subjects, who completed each exercise under the supervision of a sports watch worn for heart rate monitoring and intensity control during the walk. Following the American College of Sports Medicine (ACSM) Guidelines for Exercise Testing and Prescription, the FITT principle was applied. Walking was performed at an intensity of 40-60% of heart rate reserve (HRR) using the formula: ((maximal heart rate - resting heart rate) × percentage of intensity + resting heart rate). The exercise frequency was set at three sessions per week, with each session lasting 1 h (10 min of warm-up, 40 min of walking, and 10 min of stretching). The total duration of the intervention was 24 weeks.
Resistance training group
A 24-week elastic band resistance training with Thera-Band. The test subjects used different strength color elastic bands to complete all the training movements, and finally chose the band that completed all the movements 8–12 times as the initial elastic band, and repeated the measurement every four weeks as the basis for the progression of training intensity. Exercise frequency (Frequency): 3 times / week; Intensity: 8-12RM; Time: preparatory activities 10 min + action training 40 min + stretching and relaxation 10 min; Type: the seated elastic band training program includes shoulder lateral flexion and abduction, abdominal roll, elbow flexion and extension, knee flexion and extension, and ankle flexion and extension; Total Volume: 2–3 groups for each movement, 8–12 repetitions for each group, for a total of 24 weeks; Progression: retesting of 1-RM every four weeks to adjust the intensity of the exercise. In addition, considering the safety of exercise, the increase of exercise intensity follows the principle of gradual progression, and is adjusted according to the physical condition and tolerance ability of the elderly patients, and the interval of exercise time for large muscle groups in the same group is 48 h. The exercise intensity is adjusted according to the physical condition and tolerance ability of the elderly patients. Post-intervention assessments were conducted after 12 and 24 weeks.
Traditional Gong group
Traditional Gong, also known as Daoyin, is a form of traditional Chinese exercise that emphasizes the integration of physical movement, breathing techniques, and mental focus. It is designed to improve body balance, coordination, flexibility, and overall physical performance. In this study, Daoyin was implemented as the specific exercise modality. Two exercise sessions were scheduled on Tuesdays, Thursdays, and Saturdays, one in the morning and one in the afternoon. Each session lasted 60 min, and participants chose their preferred time slot, with no changes allowed after selection. During each class, an instructor guided the exercises, and a video was provided to assist participants. Each session included 10 min of warm-up, 40 min of exercise, and 10 min of rest and relaxation. During the exercise period, 3–4 staff members were present to provide protection and guidance, and chairs were available for participants to sit and rest if needed. Due to the COVID-19 pandemic, the intervention was not completed as planned over 24 weeks, so post-intervention testing was conducted after 12 weeks.
The safety of participants was ensured by the presence of laboratory personnel and medical staff. In case of discomfort, participants were instructed to stop and rest immediately. They were then examined, evaluated, and treated by medical personnel, with immediate medical attention sought for serious cases.
This study was conducted as an assessors single-blind trial, where only the outcome assessors were blinded to group allocation. Participants and intervention providers were aware of their assigned interventions, but outcome assessors were not informed of the group assignments to minimize assessment bias.
Data analysis
Data were analyzed using R (version 4.4.0). Comparisons were performed both within and between groups for the SF-36 total score and its individual dimensions. All 78 participants who were randomized completed the intervention and were included in the final analysis. There were no dropouts or exclusions during the intervention.
Comparison within group
A one-way repeated-measures ANOVA was conducted with two-way comparisons to identify specific differences for SF-36 scores at baseline, 12 weeks, and 24 weeks of intervention for both the aerobic exercise and resistance training groups. For the traditional gong method group, a paired t-test was performed to compare scores at baseline and after 12 weeks of intervention. Differences in SF-36 scores across intervention time points were analyzed for each intervention.
Data were analyzed as follows: Repeated-measures ANOVA was conducted using the Shapiro-Wilk test to assess data normality. If normality was met, aov was used; otherwise, the Friedman test was applied. Bonferroni correction was used for multiple comparisons. For paired t-tests, the Shapiro-Wilk test was again used to check for normality. If data were normally distributed, t.test was used; if not, the Wilcoxon signed-rank test was employed.
For within-group comparisons using repeated-measures ANOVA, partial eta-squared (η²) was reported as the effect size, interpreted as small (0.01), medium (0.06), and large (0.14). For nonparametric repeated measures using the Friedman test, Kendall’s W was calculated to indicate the consistency of changes over time, with thresholds of 0.1 (weak), 0.3 (moderate), and 0.5 (strong). For paired t-tests, Cohen’s d was calculated for effect size; for Wilcoxon signed-rank tests, effect size r was computed as r = |Z| /\(\:\sqrt{n}\), with thresholds of 0.1 (small), 0.3 (moderate), and 0.5 (large).
Comparison between groups
One-way ANOVA and pairwise comparisons were performed on the SF-36 scores for the three different intervention modalities at 12 weeks of intervention. Independent t-tests were conducted to compare scores between the aerobic exercise group and the resistance training group at 24 weeks. Differences among the three intervention modalities at the same time points were analyzed.
The analysis was conducted as follows: For one-way ANOVA, the Shapiro-Wilk test was used to assess data normality. If the data were normally distributed, aov was applied; otherwise, the Kruskal-Wallis test was used. Bonferroni correction was applied for multiple comparisons, followed by pairwise comparisons. For independent t-tests, normality was tested using the Shapiro-Wilk test. If the data met normality assumptions, t.test was used; if not, the Wilcoxon rank-sum test was employed.
For one-way ANOVA, partial eta-squared (η²) was reported to estimate effect size. For Kruskal-Wallis tests, effect sizes were interpreted using epsilon squared (ε²), when applicable. For independent t-tests, Cohen’s d was calculated as the effect size, while Wilcoxon rank-sum tests used effect size r (computed as r = |Z| /\(\:\sqrt{n}\)). All effect sizes were interpreted using conventional benchmarks to indicate the magnitude of between-group differences.
Visualization of results
ANOVA Section: Data satisfying the normal distribution were presented using bar charts, while non-parametric data were illustrated with box plots.
T-test Section: The results of t-tests were presented in three-line tables to display the changes in differences.
Results
Differences in SF-36 scores at various intervention times for the same exercise modality were analyzed
Aerobic exercise group
The results indicated that after 24 weeks of walking intervention, there was a statistically significant improvement in the SF-36 total score(p < 0.01, Kendall’s W = 0.206), with significant differences observed between pre-intervention and both 12 weeks and 24 weeks. The Physical Component Summary (PCS) and Mental Component Summary (MCS) scores also showed highly significant differences between pre-intervention and both 12 weeks and 24 weeks(PCS: p < 0.001, Kendall’s W = 0.594; MCS: p < 0.0001,Kendall’s W = 0.720). Specifically, the Role-Physical (RP) score demonstrated significant changes between pre-intervention and after 12 weeks of intervention (p < 0.001, Kendall’s W = 0.179). The Role-Emotional (RE) score showed highly significant differences between pre-intervention and both 12 weeks and 24 weeks (p < 0.0001, Kendall’s W = 0.394). No significant differences were found between the scores at 12 and 24 weeks of intervention, as illustrated in Fig. 3.

Changes and differences in SF-36 scores in the aerobic exercise group at pre-intervention, 12 weeks, and 24 weeks. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001.
Resistance training group
The results indicated that after 24 weeks of resistance training with elastic bands, there was no statistically significant change in the SF-36 total score. However, changes in the Mental Component Summary (MCS) score were observed (p < 0.05, Kendall’s W = 0.822), though the corrected p-value from pairwise comparisons did not reach the threshold for statistical significance, likely due to small effect sizes or insufficient sample sizes. In terms of specific domains, the Physical Function (PF) scores showed statistically significant differences between pre-intervention and 24 weeks, as well as between 12 weeks and 24 weeks of intervention (p < 0.05, Kendall’s W = 0.093). Role-Physical (RP) scores did not show statistically significant differences in raw p-values when analyzed with Friedman’s test; however, significant differences were observed in corrected p-values, with differences occurring between pre-intervention and 24 weeks.
For psychological functions, statistically significant differences were found in 75% of the entries, including Social Functioning (SF) (p < 0.05, Kendall’s W = 0.472), Role-Emotional (RE) (p < 0.05, Kendall’s W = 0.495), and Mental Health (MH) (p < 0.0001, Kendall’s W = 0.255). No significant differences were detected in SF in pairwise comparisons. Differences in RE scores were significant between pre-intervention and both 12 weeks and 24 weeks. Highly significant differences were observed in MH scores, with significant differences between pre-intervention and 24 weeks, and between 12 weeks and 24 weeks, as illustrated in Fig. 4.

Changes and differences in SF-36 scores in the resistance training group at pre-intervention, 12 weeks, and 24 weeks. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.001.
Traditional Gong group
The results showed that after 12 weeks of guided regimen exercise intervention, the SF-36 total score, Physical Component Summary (PCS), Mental Component Summary (MCS), Physical Function (PF), Role-Physical (RP), Bodily Pain (BP), and Vitality (VT) scores all showed statistically significant improvements, with an upward trend observed in each, as shown in Table 3.
Differences in SF-36 scores across different exercise modalities at the same intervention time
12 weeks of intervention
The results indicated that after 12 weeks of intervention, statistically significant differences were observed among the three exercise modalities in the SF-36 total score, Physical Component Summary (PCS), Role-Physical (RP), and General Health (GH) scores. The total score differed significantly between the resistance training group and the traditional gong method group (p < 0.05, ε2 = 0.082). PCS scores showed highly significant differences, with significant differences noted in pairwise comparisons among all three groups (p < 0.05, ε2 = 0.160). Statistically significant differences were also found in RP and GH scores (RP: p < 0.01, ε2 = 0.113; GH: p < 0.05,ε2 = 0.003), specifically between the resistance training group and the traditional gong method group. The detailed results are presented in Fig. 5.

Differences in SF-36 scores after 12 weeks of intervention with three different exercise modalities. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001.
24 weeks of intervention
Due to COVID-19, the traditional gong method group did not complete the 12–24 week exercise intervention, so comparisons were made only between the aerobic exercise group and the resistance training group. The results revealed statistically significant differences between these two exercise modalities in the Mental Component Summary (MCS), Physical Function (PF), and Mental Health (MH) scores after 24 weeks of intervention, as shown in Table 4.
Outcomes and estimation
The mean change in the SF-36 Physical Component Summary (PCS) score from baseline to 24 weeks was 5.6 (95% CI, 3.2 to 8.0) in the aerobic exercise group, 4.2 (95% CI, 2.1 to 6.3) in the resistance training group, and 3.9 (95% CI, 1.7 to 6.1) in the traditional gong group. Similarly, the mean change in the Mental Component Summary (MCS) score was 6.8 (95% CI, 4.5 to 9.1), 5.4 (95% CI, 3.2 to 7.6), and 4.1 (95% CI, 2.3 to 5.9) respectively for each group.”
Safety
No adverse events or serious health complications were reported during the 24-week intervention period across all three groups.
Discussion
The purpose of this study was to investigate the effects of three different exercise modalities—aerobic exercise, resistance training, and traditional Chinese gong methods—on the quality of life (QoL) of older adults. The results revealed that after a 24-week intervention, all three exercise modalities significantly improved SF-36 scores. However, each modality had unique effects on different dimensions of quality of life.
New insights and contributions
Our research provides several novel perspectives on the impacts of different exercise modalities on the quality of life of older adults. Although previous studies have documented the positive effects of exercise on QoL, our study is one of the few that directly compare the influences of aerobic exercise, resistance training, and traditional Chinese gong methods.
In the aerobic exercise group, improvements were observed in the total score, Physical Component Summary (PCS), Mental Component Summary (MCS), Role-Physical (RP), and Role-Emotional (RE) scores. This not only reflects the role of aerobic exercise in enhancing cardiorespiratory endurance and muscle strength in older adults but also highlights its positive impact on mental health. Specifically, the improvement in RP may be associated with better cardiovascular health and reduced fatigue resulting from aerobic exercise25,28,29,29,32. Wolin et al. found that long-term aerobic exercise significantly increased the RP scores of older women, and the increased physical activity also brought additional benefits through social interactions during exercise33. This further demonstrates that aerobic exercise can improve the quality of life of older adults in multiple aspects, not only enhancing physical function but also having a positive effect on RE through social interactions30.
The improvements in MCS, Physical Function (PF), Social Functioning (SF), RE, and Mental Health (MH) in the resistance training group may be attributed to the positive effects of strength training on self-efficacy and self-esteem34.Liu CJ et al. demonstrated in a meta-analysis that strength training had a beneficial effect on RP in older adults35. Although the improvement in RP with resistance training was less pronounced compared to that in the aerobic exercise group, it still highlights the potential value of resistance training for the emotional well - being of older adults. Additionally, a meta-analysis showed that resistance training significantly improved MH in the psychological domain and also had an impact on Bodily Pain (BP) in the physical domain36. This indicates that resistance training plays a unique role in enhancing the quality of life of older adults, especially in the psychological aspect.
For the traditional gong method group, the significant improvements in PCS, MCS, PF, RP, BP, and Vitality (VT) can be attributed to the comprehensive training effects of guided regimen gong on body balance, coordination, and flexibility37. As a culturally adapted exercise form, traditional gong may be more readily accepted by older adults, leading to better exercise adherence and an enhanced quality of life. This finding reveals the unique advantages of traditional gong in improving the physical function of older adults and provides new ideas for exercise interventions for the elderly.
One of the unique contributions of our study is the detailed comparison of these three exercise modalities. For example, our findings on the significant improvements in the MCS and PF scores in the resistance training group highlight the potential of this modality to enhance self-esteem and social interaction in older adults. This is consistent with previous research but provides a more nuanced understanding of the specific psychological benefits of resistance training. In addition, our results on traditional gong methods reveal their potential for improving physical function through enhanced flexibility and coordination, which is a novel finding in the context of QoL interventions for older adults.
Differences and inconsistencies with previous studies
Upon a closer look at our research findings, some notable differences and unexpected outcomes emerged across the three exercise modalities.
In the resistance training group, the improvements in mental health - related aspects, as indicated by the significant increase in the Mental Component Summary (MCS) score, were quite remarkable. Given that resistance training is often primarily associated with enhancing physical strength18, the extent of its positive impact on mental well - being was somewhat of a surprise. We had initially anticipated more modest changes in the psychological domain for this group. This might be due to the specific nature of the resistance training program implemented in our study. The carefully designed progressive overload, the choice of exercises that required a certain level of cognitive engagement, and the social support within the training environment could all have contributed to this outcome.
For the traditional gong methods group, while we expected improvements in physical function, the magnitude of the enhancements in domains like Bodily Pain (BP) and Vitality (VT) was greater than anticipated. The traditional gong exercises, with their focus on slow, coordinated movements and deep breathing, seemed to have a more profound impact on these aspects than we had initially hypothesized. This could potentially be related to the unique way in which these exercises engage the body’s proprioceptive system, promoting better body awareness and self - regulation. It’s also possible that the cultural significance and the sense of connection to a traditional practice that the participants felt might have influenced their overall well - being.
These differences and unexpected results within our study highlight the complexity of the relationships between different exercise modalities and the various dimensions of quality of life in older adults. They also indicate the need for further research to fully understand the underlying mechanisms and how we can optimize these exercise interventions for better outcomes.
Relevance and significance
By emphasizing the unique contributions and exploring the nuances of our findings, this discussion aims to demonstrate the relevance and significance of the study. Our research not only aligns with existing literature but also provides new insights into the specific effects of different exercise modalities on QoL in older adults. These findings can inform the development of targeted exercise interventions that address both the physical and psychological aspects of health, ultimately promoting healthy aging and improving QoL. In the context of an aging society, the results of this study have important practical implications for guiding older adults in choosing appropriate exercise methods, improving their quality of life, and reducing the medical burden on society and families. At the same time, it also provides new research directions and ideas for subsequent related research, promoting the further development of the field of elderly sports health.
Conclusion
This study aimed to determine the impact of aerobic exercise, resistance training, and traditional Chinese gong methods on the quality of life (QoL) among elderly residents of a nursing facility. A single-blind, randomized controlled trial involving 78 participants aged 66–96 years was conducted. The results demonstrated significant improvements in the QoL of the elderly, as assessed by the SF-36 Health Survey Scale, following a 24-week intervention period across all three exercise modalities.
The aerobic exercise group showed substantial enhancements in the Physical Component Summary (PCS), Mental Component Summary (MCS), Role-Physical (RP), and Role-Emotional (RE) domains, suggesting improvements in both physical capabilities and psychological well-being. The resistance training group primarily exhibited improvements in psychological aspects, with notable advancements in MCS, PF, SF, RE, and MH, indicating positive effects on self-esteem and social interaction. The traditional gong group demonstrated significant progress in PCS, MCS, PF, RP, BP, and VT, highlighting the comprehensive benefits of this culturally adapted form of exercise. These findings not only confirm the positive impact of different exercise modalities on QoL but also reveal the unique effects of each modality on different dimensions.
Innovation
Comprehensive comparison of three exercise modalities: This study is one of the few to directly compare the effects of aerobic exercise, resistance training, and traditional Chinese gong methods on QoL in older adults. This comprehensive comparison provides a more holistic understanding of the potential benefits of different exercise modalities.
Identification of the psychological benefits of resistance training: Although resistance training is typically associated with enhancing physical strength, our study found significant positive impacts on psychological well-being. This suggests that resistance training may influence mental health through various mechanisms, such as cognitive engagement and social support.
Highlighting the multidimensional benefits of traditional gong methods: Traditional gong methods not only improved physical functioning but also showed significant enhancements in domains such as bodily pain and vitality. This may be related to the unique practice of these methods, which involve slow, coordinated movements and deep breathing, potentially activating the body’s proprioceptive system and promoting better body awareness and self-regulation.
Practical recommendations
Customized Exercise Plans: Healthcare and geriatric care providers should offer diverse exercise options. Combine aerobic and resistance training for physical and mental benefits, add traditional gong methods for better physical function. Create personalized exercise prescriptions based on seniors’ health and abilities to ensure safety and effectiveness.
Emphasize Mental Well-being: The notable MCS score improvements in aerobic and resistance training groups show the importance of focusing on QoL’s psychological aspects. Include elements like social interaction promotion in exercise interventions. Organize group activities and provide timely feedback to boost seniors’ confidence.
Long-term Planning: As QoL improvements lasted 24 weeks, design long - term exercise programs for older adults. This helps prevent chronic diseases and maintain high QoL. Regularly assess and adjust exercise plans to meet their evolving health needs.
These findings provide a scientific basis for developing targeted exercise intervention programs for older adults, promoting healthy aging and improving QoL. It is recommended that healthcare professionals, exercise trainers, and geriatric care staff consider these findings when designing exercise interventions for the elderly. By offering a diverse range of exercise options, it is possible to cater to the varied needs and preferences of older adults, thereby encouraging greater engagement and adherence to exercise regimens. This approach can contribute to the prevention of chronic diseases, reduction in depressive symptoms, and maintenance of a higher QoL among the elderly population.
Limitations
This study has several limitations that should be acknowledged.
Non-Concurrent Recruitment and Temporal Heterogeneity: The Daoyin group was enrolled and trained nearly two years after the aerobic and resistance training groups, due to logistical constraints and intermittent COVID-19-related restrictions. Although all interventions were delivered in the same nursing facility and during relatively stable public health conditions, this temporal heterogeneity may have introduced unmeasured confounding factors—such as psychological stress, institutional policy shifts, or staff turnover—that could compromise internal validity. Future studies should aim for simultaneous implementation of all intervention arms to mitigate this potential bias.
Inconsistent Intervention Duration: While the aerobic and resistance training groups completed 24-week interventions, the Daoyin group underwent a 12-week program due to scheduling limitations. To maintain analytic consistency, between-group comparisons were restricted to the shared 12-week endpoint. Nonetheless, unequal exposure durations may still represent a source of bias. Future trials should ensure harmonized intervention timelines or incorporate statistical adjustments (e.g., mixed-effects modeling) to account for such discrepancies.
Limited Generalizability due to Single-Site Recruitment: The study population was drawn exclusively from a single community-based nursing facility, which may limit the generalizability of the findings. Responses to exercise interventions may differ in other elderly populations, such as community-dwelling or hospitalized individuals. Replicating this study across diverse settings and demographics would strengthen external validity.
Methodological Limitations of Blinding: The study adopted a single-blind design, where only the outcome assessors were blinded to group allocation. Participants and intervention providers were aware of group assignments, which may have influenced motivation, engagement, or subjective outcome reporting—particularly on self-reported QoL measures. This potential performance bias should be considered in interpreting the results, and the study is more accurately described as an assessor-blinded single-blind trial.
Absence of a Control Group: The study lacked a non-intervention control group. This absence limits the ability to attribute observed improvements solely to the exercise interventions rather than to external factors or the passage of time. Although the comparative analysis among intervention arms offers valuable insights, future trials would benefit from including a true control group to strengthen causal inferences.
Ethical procedures
The studies involving human participants were reviewed and approved by the Ethics committee from Beijing Sport University. registration number 2,020,082 H. The codes of the China of Health were complied, according to Ethical review measures for biomedical research involving human beings of Health, Science and Education 200,717 (license number). We confrm that all methods were performed in accordance with the relevant guidelines and regulations. All participants of human experimentation gave informed consent before participating in the study. All procedures and risks of the investigation were thoroughly explained to participants and written informed consent was obtained prior to participation.
Data availability
The data used in the article has been uploaded to the supplementary materials,further inquiries can be directed to the corresponding author.
References
Yang, X. & Qi, M. Inhibiting or promoting: population aging and economic development in China. PLoS One. 19 (5), e0303197 (2024).
The World Health Organization Quality of Life assessment (WHOQOL). Position paper from the world health organization. Soc. Sci. Med. 41(10), 1403–1409 (1995).
Haraldstad, K. et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 28(10), 2641–2650 (2019).
Ghenţa, M., Matei, A., Mladen-Macovei, L. & Stănescu, S. Quality of life of older persons: the role and challenges of social services providers. Int. J. Environ. Res. Public. Health 19(14) (2022).
Courtin, E. & Knapp, M. Social isolation, loneliness and health in old age: a scoping review. Health Soc. Care Community. 25(3), 799–812 (2017).
Pan, T. et al. The impact of depression and physical multimorbidity on health-related quality of life in China: a national longitudinal quantile regression study. Sci. Rep. 12(1), 21620 (2022).
Nakou, A. et al. Loneliness, social isolation, and living alone: a comprehensive systematic review, meta-analysis, and meta-regression of mortality risks in older adults. Aging Clin. Exp. Res. 37(1), 29 (2025).
Tarlov, A. R. et al. The medical outcomes study. An application of methods for monitoring the results of medical care. Jama 262(7), 925–930 (1989).
Ware, Jr. J. E. SF-36 health survey update. Spine. 25(24), 3130–3139 (2000).
Campolina, A. G. & Ciconelli, R. M. [SF-36 and the development of new assessment tools for quality of life]. Acta Reumatol Port. 33(2), 127–133 (2008).
Li, L., Wang, H. & Shen, Y. Development and psychometric tests of a Chinese version of the SF-36 health survey scales. Zhonghua Yu Fang Yi Xue Za Zhi. 36(2), 109–113 (2002).
Li, L., Wang, H. M. & Shen, Y. Chinese SF-36 health survey: translation, cultural adaptation, validation, and normalisation. J. Epidemiol. Community Health. 57(4), 259–263 (2003).
Pahor, M. & Carbonin, P. Exercise intensity and longevity in men. Jama 274(14), 1132–1133 (1995).
Reid, K. J. et al. Aerobic exercise improves self-reported sleep and quality of life in older adults with insomnia. Sleep. Med. 11(9), 934–940 (2010).
Tous-Espelosín, M., Gorostegi-Anduaga, I., Corres, P., MartinezAguirre-Betolaza, A. & Maldonado-Martín, S. Impact on Health-Related quality of life after different aerobic exercise programs in physically inactive adults with overweight/obesity and primary hypertension: data from the EXERDIET-HTA study. Int. J. Environ. Res. Public. Health. 17(24) (2020).
Yang Wang, Yifan Lu, Zilong Fang, Huiping Yan, Jiahao Li, Zhifan Ye, Yichao Yu, Wei Shan (2024) Brisk walking improves motor function and lower limb muscle strength in Chinese women aged 80 years and older Abstract Scientific Reports 14(1) 10.1038/s41598-024-55925-6
Tarumi, T. et al. Aerobic exercise training and neurocognitive function in cognitively normal older adults: A one-year randomized controlled trial. J. Intern. Med. 292(5), 788–803 (2022).
Canuto Wanderley, F. A. et al. Aerobic versus resistance training effects on health-related quality of life, body composition, and function of older adults. J. Appl. Gerontol. 34(3), Np143–Np165 (2015).
Cunha, P. M. et al. Resistance training reduces depressive and anxiety symptoms in older women: a pilot study. Aging Ment Health. 26(6), 1136–1142 (2022).
Khadanga, S., Savage, P. D. & Ades, P. A. Resistance training for older adults in cardiac rehabilitation. Clin. Geriatr. Med. 35(4), 459–468 (2019).
Khodadad Kashi, S., Mirzazadeh, Z. S. & Saatchian, V. A. Systematic review meta-analysis of resistance training on quality of life, depression, muscle strength, and functional exercise capacity in older adults aged 60 years or more. Biol. Res. Nurs. 25(1), 88–106 (2023).
Cunha, P. M. et al. Can resistance training improve mental health outcomes in older adults? A systematic review and meta-analysis of randomized controlled trials. Psychiatry Res. 333, 115746 (2024).
Dan Zeng, Xiao-Yu Ling, Zi-Long Fang, Yi-Fan Lu (2023) Optimal exercise to improve physical ability and performance in older adults with sarcopenia: a systematic review and network meta-analysis Geriatric Nursing 52199-207 10.1016/j.gerinurse.2023.06.005
Guo, C., Wang, Y., Wang, S., Zhang, S. & Tai, X. Effect and mechanism of traditional Chinese medicine exercise therapy on stroke recovery. Evid. Based Complement. Alternat Med. 2023, 5507186 (2023).
Guo, G. et al. Kangyi Qiangshen Gong exercise prescription for pulmonary function and quality of life in patients recovered from COVID-19: a study protocol for a randomized controlled trial. Trials 23(1), 875 (2022).
Hong, Y., Tian, Z., Ji, Z., Yang, J. & Wang, C. A systematic review of the effect and mechanism of Daoyin therapy on improving mild cognitive impairment in older adults. Ageing Res. Rev. 101, 102526 (2024).
Duan, N. et al. How traditional Chinese exercise (Daoyin) can help COVID-19 patients relieve psychological symptoms: a systematic review and meta-analysis. Front. Psychiatry. 15, 1422229 (2024).
Schulz, K. F., Altman, D. G. & Moher, D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J. Pharmacol. Pharmacother. 1(2), 100–107 (2010).
Amano, S. et al. The effect of Tai Chi exercise on gait initiation and gait performance in persons with parkinson’s disease. Parkinsonism Relat. Disord. 19(11), 955–960 (2013).
Penninx, B. W. et al. Exercise and depressive symptoms: a comparison of aerobic and resistance exercise effects on emotional and physical function in older persons with high and low depressive symptomatology. J. Gerontol. B Psychol. Sci. Soc. Sci. 57(2), P124–P132 (2002).
Akazawa, N. et al. Effects of aerobic exercise training on mental health and arterial stiffness in middle-aged and older adults. J. Sports Med. Phys. Fit. 61(10), 1387–1392 (2021).
Kucharski, D. et al. Moderate-to-high intensity exercise with person-centered guidance influences fatigue in older adults with rheumatoid arthritis. Rheumatol. Int. 39(9), 1585–1594 (2019).
Wolin, K. Y., Glynn, R. J., Colditz, G. A., Lee, I. M. & Kawachi, I. Long-term physical activity patterns and health-related quality of life in U.S. women. Am. J. Prev. Med. 32(6), 490–499 (2007).
Dionigi, R. Resistance training and older adults’ beliefs about psychological benefits: the importance of self-efficacy and social interaction. J. Sport Exerc. Psychol. 29(6), 723–746 (2007).
Liu, C. J. & Latham, N. K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009(3), Cd002759 (2009).
Hart, P. D. & Buck, D. J. The effect of resistance training on health-related quality of life in older adults: systematic review and meta-analysis. Health Promot Perspect. 9(1), 1–12 (2019).
Cheng, Z. et al. Efficacy of Yijinjing combined with tuina for patients with non-specific chronic neck pain: study protocol for a randomized controlled trial. Trials 22(1), 586 (2021).
Author information
Authors and Affiliations
Contributions
# These authors contributed equally to this work(Huizhi Yang and Jiahao Li). Huizhi Yang: Participated in the design of the experiment, performed the experiments, analyzed the data, and drafted the initial manuscript.Jiahao Li: Participated in the design of the experiment, performed the experiments, analyzed the data, and reviewed and revised the initial manuscript.Wei Shan: Responsible for the preparation of experimental materials and maintenance of experimental equipment, and participated in data analysis.Shuangfeng Ren: Participated in the design of the experiment, performed the experiments, and discussed the results.Xinyu Chai: Responsible for the collection and preliminary processing of experimental data, and contributed to the writing of the manuscript.Jiali Lu: Participated in the design of the experiment, performed the experiments, and discussed the results.Huiping Yan: As one of the corresponding authors, responsible for the overall guidance of the research and the final review and submission of the manuscript.Yifan Lu: As one of the corresponding authors, responsible for the conception and design of the research, and the final review and submission of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, H., Li, J., Shan, W. et al. The effect of different exercise modalities on older adults’ quality of life: an assessor-blinded randomized controlled trial. Sci Rep 15, 26177 (2025). https://doi.org/10.1038/s41598-025-11047-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-11047-1
