
Abstract
Previous studies placed copies of artworks in hospital environments to reduce stress and anxiety of patients. This study aims to investigate the psychological effect of a virtual tour of a museum provided by a virtual reality (VR) system in chronic patients suffering from Chronic Renal Failure (CRF) during the administration of haemodialysis. Twenty-six patients were enrolled at the Hospital where usually underwent for receiving their conventional therapy (CT) for CRF. Their positive and negative affect was measured by PANAS at baseline (before), after CT, and after CT in which a virtual museum visit experience (VR) was added, with a randomized cross-over design. Psychological distress, assessed as the evaluation of positive and negative emotion through PANAS scale, resulted in statistical difference among trait (baseline), CT and VR examination (p = 0.001), with specific difference between positive and negative poles (p < 0.001). Patients reported positive emotions for VR (mean = 28.1 ± 7.5) very close to the baseline (mean = 28.2 ± 8.1), suggesting a potential use of this technology as palliative treatment during CT. Psychological distress associated with CRF was shown to be reduceable by the museal visit fruition through the VR system. This positive effect was reconducted to the so-called cultural wellness potentially induce by the cultural heritage.
Similar content being viewed by others

Introduction
The World Health Organization published a wide extensive review of scientific literature reporting the positive effects of art on promotion of health and on prevention, management and treatment of diseases1. Many studies reported as art can improve mental health and confidence in the future, reducing anxiety and depression symptoms2,3,4. The presence of artworks in hospitals could reduce stress of pathological conditions, providing familiarity, distraction and prompts for social engagement5. It was also shown that art can also have positive effects on emotion regulation and meaning making in individuals with diabetes6,7. As highlighted in a recent review8 recent studies exploited the use of virtual reality systems to foster the positive effects of art in hospitals and ambulatories settings. The participants experience a sense of presence in the immersive virtual environments as if they were not in a clinical environment9. Watching virtual reality movies reduced distress and pain in adults and children during dental examination10,11. A virtual window reduced anxiety and depression symptoms in patients who experienced a transplant12. Recent studies13,14 reported the efficacy of virtual art therapy protocols in neurological rehabilitation, highlighting a reduction of the fatigue perceived by patients, a phenomenon called Michelangelo’s effect. Despite these interesting results, art protocols in patients with chronic renal failure lack in scientific literature. In 201915, it was also proposed an interesting study protocol about the use of virtual reality (but not combined with art) in these patients. Despite the interesting hypothesis about the potential improvement in patients’ quality of life thanks to the VR multisensory experience absorbing patients’ perceptions and thoughts during, the results have not yet published.
Chronic renal failure (CRF) also known as chronic kidney disease (CKD stage 3, 4&5) is a metabolic condition that involves an irreversible loss of the kidney’s ability to expel waste products and regulate electrolyte and water balance16. As a systemic condition, it may involve many organs of the body, thus leading to further dysfunction such as cardiovascular17, anaemia18, malnutrition19, muscle wasting20, glucose intolerance21. As a chronic condition, CRF has emerged as a major public health issue worldwide, representing an important contributor to morbidity and mortality22, significantly compromising the quality of life of people affected23, determining an increased costs for healthcare systems.
Indeed, the World Health Report24 and Global Burden of Disease (GBD) project25 stated that diseases of the kidney and urinary tract contribute to the global burden of diseases causing approximately 850,000 deaths every year and 15.010,167 disability-adjusted life years (DALYs) globally26. From this perspective, it seems clear that the chronicity of the disease can also affect the mental health of patients with renal failure. In particular, the concept of “psycho-nephrology” has been in existence for many years and was firstly used to describe the sense of being completely dependent from the hemodynamic machine27. Following evidence28 has clearly indicated the interaction between psychological factors, such as mood disorders28,29 and medical outcomes of CRF30, as potential psychological distress positively associated with increased health-care utilization31, lower adherence to treatment32 and increased risk of initiation of dialysis29.
Among various psychiatric disorders, depression is the most common psychiatric disorder for patients with CRF, frequently associated with renal function deterioration33. In turn, the chronic debilitating nature of CRF is associated with distressing physiologic, social and psychological responses which might cause or exacerbate depression34.
It follows that managing the psychological distress is a complex process that is not limited to removing the physical symptoms, definitely not enough to guarantee the psychophysical well-being of the person suffering from a chronic pathology like the CRF35. Secondly, it is important to manage psychological distress as it can cause aversive anticipatory responses such as nausea, sleep disturbance, or other symptoms36. Anxiety symptoms experienced by patients during dialysis treatment may also lead to psychological distress, irrational behaviours, conflicts with staff and physicians, reduced compliance to treatment37. Psychological support or distracting interventions may help CRF patients to manage the sequelae of dialysis38.
Over the last two decades, the use of virtual reality systems to support clinical treatments has increased considerably9,39. Among psychological interventions aimed at improving tolerance to therapy in chronic pathologies, distraction could be a promising strategy40,41,42. Distraction is an effective emotion-focused coping strategy as it diverts attention from unpleasant stimuli towards pleasant or interesting stimuli, thus decreasing stress and anxiety43. In this regard, virtual reality has already proven to be a good tool with which conveys distraction during painful38,44 or boring-repetitive treatments such as in the case of physiotherapy13,14.
The potential of using VR relies on the interaction with displayed images, moving and manipulating virtual objects fostering actions allow the users attempts to “immerse” them within the simulated environment, thereby engendering a feeling of “presence” in the virtual world45. As reported by Schubert et al.46, the sense of presence is the distinctive feature that denotes VR as unique technology in its genre and make it different from a simple videogame47. Indeed, VR is considered a suitable candidate to provide positive experiences precisely due to its immersive power and the sense of presence that VR experiences may craft48. Recent research has established that VR is arousing49,50 and is an effective tool for inducing emotions both in laboratory51 and in real settings52. More precisely, VR has proven effective in inducing various positive emotions, such as joy, relaxation53,54 and more complex emotions such as awe (i.e., feeling of wonder when confronted with vast and transcending stimuli55,56), and the sublime (i.e., feeling of “amazement tinged with fear” in response to vast or powerful stimuli57), .
Neuroscientific studies such as the pioneering work of Ishizu and Seki’s58,59,60 demonstrated that natural beauty and sublimity is responsible to activate different brain areas and evoke very different experiences in humans58. Specifically, the inferior temporal cortex, hippocampus, inferior/middle frontal gyri, basal ganglia, and cerebellum were suggested as modulators of the intensity of sublimity60. Indeed, fMRI studies such as that of Takano & Nomura61, suggested that awe experiences generally involve the “schema liberation” process since the left middle temporal gyrus (MTG) plays a critical role in matching existing schema to events. In addition, positive awe was associated with increased functional connectivity between the MTG and the anterior/posterior cingulate cortex, which are associated with the aesthetic reward process, and the supramarginal gyrus, which is involved in the self-other representation. As awe and sublime are able to evoke such a strong neural response relying on the need for accommodation and perception of vastness62 which are already found to be potential processes leading to profound and radical changes in people’s self-perception and worldview63. Given these considerations, it is plausible to state that these emotions can foster cumulative psychological benefits, including reduced rumination, improved mood, and enhanced quality of life63. Recent literature64 has traced neural correlates of awe and being able to reproduce with VR, suggesting the potential use of this technology as palliative care when combined with cultural heritage.
The use of artistic stimuli in the virtual environment could be a strategy boosting positive emotions contrasting the psychological distress experienced by patients during dialysis. We aimed at exploiting the beneficial power that art can have in arousing positive emotions. In fact, neuroimaging studies have already proven that observing artistic masterpiece elicit the activation of sensorimotor networks involved in the recognition of emotions of painted subjects, as well as the activation of the mirror neuron networks triggered by the observation of actions performed by painted people65. The wide brain arousal occurring during art fruition even involves motor areas during the observation of panoramas66 and abstract artworks65,67 due to the mirror neuron systems activated by the implicit imagination of the scene explorations66 and of the gestures of the artist needed to generate the artwork65,67.
As fostering the access to positive experiences is an important concern for enhancing well-being and mental health in hospitalized people68, the present study aims at investigating the emotions generated by virtual visit of a museum performed during treatment.
Results
Recruitment process
We collected data from 26 patients (M = 50%, mean = 65.5 ± 13.9 years) who suffered from CRF (median = 4.5 years, IQR = 1.8–9.7 years). All the patients completed the VR session and the questionnaires; therefore, none of participants was excluded from the analysis.
Primary outcome measures
As shown in Fig. 1, positive emotions for VR (mean = 28.1 ± 7.5) are very close to those reported as baseline (PANAS-Trait, mean = 28.2 ± 8.1), while achieve the lowest scores for negative pole (mean = 13.8 ± 5.2). Conversely, patients’ evaluation of Conventional Therapy (CT) reported the lowest scores for positive pole (22.4 ± 7.5) and the highest for negative one (18.0 ± 7.7) compared to the other two evaluations.
We found a significant statistical effect both for the three administrations of the Positive and Negative Affect Schedule (PANAS) (F(2) = 7.483, p = 0.001) but with a small effect size (ES = 0.230), and the poles (F(1) = 32.922, p < 0.001) which contributed mainly to the variance with a medium effect (ES = 0.568). Finally, the interaction between the two factors (conditions*poles) resulted statistically significant (F(2) = 13.142, p < 0.001, ES = 0.345).

Raincloud plots of PANAS assessment. Figure shows the PANAS scores and their frequency distributions on which repeated measure analysis of variance was performed. For each administration (baseline, trait; CT, conventional treatment, VR, Virtual reality session), red distributions refer to positive pole, while the blue ones are for the negative pole. On the x-axis were reported the three testing while y-axis reports the scores obtained in every subscale. Each subject is represented by two dots stand for raw scores: a red dot for positive subscale and in blue for the negative one. The highlighted dots marked with a solid line stand for the mean value of the group for positive and negative subscale.
Post-hoc analyses revealed a significant reduction of negative emotions in Virtual Reality (VR) condition with respect to Trait values (p < 0.001). The data reported in Fig. 1 showed a wide variation of the data; however, it should be kept in mind that the cross-over design of the study allows for a within-subject analysis that is not affected by between subject variability. The positive emotions were not significantly different between VR and Trait, whereas they were significantly lower in conventional therapy (CT) with respect to both Trait values (p = 0.003) and values assessed in VR condition (p < 0.001), where CT was always reported as less positive than the other conditions.
As shown in Fig. 2, positive emotions associated with VR session shows in the left panel consisted of a bigger density of scores in the range between 20 and 35 with respect to the Conventional treatment (CT) session. In the right panel, the VR distribution showed a high concentration in the region scoring between 5 and 15, while conventional therapy showed a distribution of higher scores between 10 and 20, thus resulting in a higher mean.

Positive and negative scores of subscales of PANAS. In each panel, density plots show distribution of PANAS positive and negative subscales administered after the VR o CT session. Y-axis refers to the jittering coefficient needed to create the density plot using the kernel density estimation technique. Every patient is plotted as a dot. Boxplot figure below the raincloud plots shows in detail the distribution of scores for each subscale. Solid lines on the left and right of the box respectively stand for minimum and maximum values of the range; Interquartile range is represented by the box in which a vertical solid line stands for the median value obtained by the group for each subscale.
Analysing the specific positive emotions, we found statistically significant increment in VR with respect to CT for interest (p < 0.001), enthusiasm (p = 0.001), excitement (p = 0.004), inspiration (p = 0.015), and energy (p = 0.032), as shown in Fig. 3 reporting the Effect Size in terms of Cohen’s d.
All the other positive emotions were higher in VR, but not significantly (as strength, p = 0.054), except for alertness, that was higher in CT, but not significantly (p = 0.245). Some negative emotions were significantly lower in VR than in CT: fear (p = 0.019) and jitter (p = 0.039), with some other only approaching the significant threshold (distress: p = 0.054; scare: p = 0.063; nervousness: p = 0.076; hostility: p = 0.078).

Effect sizes (Cohen’s d) of emotional responses measured by the PANAS scale. The Figure displays the effect size for each of the 20 emotions from the Positive and Negative Affect Schedule (PANAS) following the VR condition. Effect sizes were calculated using Cohen’s d, where values around 0.2, 0.5, and 0.8 represent small, medium, and large effects, respectively (shaded regions for reference). Positive emotions (orange dots) are shown on the left and negative emotions (blue dots) on the right, sorted by descending effect size. Colours indicate direction of the effect (yellow = increase; blue = decrease). Asterisks (*) denote statistically significant changes (p < 0.05).
Quality of life and of experience associated with dialysis
Finally, quality of life for CRF patients was assessed with Italian version of the Edmonton Symptom Assessment System (ESAS). This scale has already proven to be an effective tool to assess QoL in patients with end-stage renal disease69. Although symptoms reported for VR conditions were always lower than CT, we found a difference only for depression (p = 0.018) and tiredness (p = 0.048). We also investigate the sense of presence of being in the hospital and the stress associated to doing the dialysis in the two conditions using the Visual Analogical Scale (VAS) on 10 points. Patients reported low scores in the evaluation of stress associated with VR and CT (17% and 22% respectively).
VR quality assessment and usability
Indeed, patients rated very highly the quality of the VR experience as the feature to let them forget being in the hospital (80%) and by giving them a sense of being in a museum (75%). Conversely, few patients (27%) during CT reported to have forgotten to be in hospital because they are engaged in other activities as usual (such as reading a newspaper or watching their smartphone).
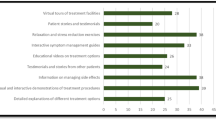
We tested the usability of the system during dialysis using the System Usability Scale. SUS is a tool mainly helpful for comparing competitive alternatives, according to a relative approach rather than an absolute interpretation of the score70, hence caution is needed when interpreting the SUS score for a single technology. However, a curved grading scale71 and an adjective rating70 have both been developed for the SUS score. According to these ratings, our average score of 62 ± 16% corresponds to a grade C+, which indicates a good level of usability.as shown in Fig. 4.

System usability scale scoring (SUS). Items of SUS have been normalized on the maximum score of the scale and reported as percentage. Descriptive error bars were added as standard deviation. Beneath a table was added to specify each item of the scale.
Discussion
This study was focused on validating the use of art as alternative palliative intervention for the negative emotions conveyed by being subjected to long-term haemodialisys procedure. We examined the effects of a cultural heritage artistic protocol delivered in VR technology on emotional responses in patients suffering from chronic renal failure (CRF). Our findings indicate that art therapy, particularly in its immersive VR form, plays a significant role in enhancing positive emotions and reducing negative emotions associated with conventional treatment. Although the overall effect size of PANAS ranged from small to medium, it was large for certain emotions that our intervention primarily target. Our results revealed a notable increment in interest, excitement, enthusiasm, inspiration and energy during haemodialisys immediately after the virtual tour of the museum, for which these emotions reported a large to medium effect size as shown in Fig. 3. Particularly interesting was also the decrease of negative emotions such as fear and jitter. Scare, distress, hostility and nervousness were also reduced, but not significantly. Some other emotions were not targeted by our intervention and, in fact, did not show significant changes, such as attention, pride and determination among positive emotions, and guilt, disappointment and shame among negative emotions. These findings support the idea that art protocols can serve as effective adjuncts in clinical settings, particularly for patients facing the challenges of CRF. The ESAS scale confirmed this trend, showing a reduction in depression and tiredness after the virtual visit to the museum.
Potential contribution of art protocol on emotional distress
Recent literature has underscored the therapeutic benefits of art interventions in healthcare72. For instance, a study by Bell et al.73 found that art therapy significantly improved emotional well-being and reduced anxiety levels among patients receiving chemotherapy. This aligns with our findings, which demonstrated that VR, as an art-based intervention, can promote a more pleasant emotional experience compared to conventional therapy. Additionally, a 2021 review by Zubala, Kennell & Hackett74 highlights the potential of digital art therapy, including VR experiences, to engage patients emotionally with the aim to help them transcend their immediate healthcare environment, thus providing a sense of relief during medical procedures.
The VR was probably also a booster of these positive effects for its capacity to make the patients feel as in another place and not in the hospital, as reported by the 80% of the participants. Furthermore, the VR system was also judged as easy to use.
The use of VR technology to reduce stress associated with medical procedures has already proven to be very effective, for example to relieve pain and distress during medical procedures such as patients with burn injuries undergoing wound care, and physical therapy40. However, our study aimed at using an artistic protocol based on cultural heritage to promote positive emotions in contrast to the negative ones that can be aroused by prolonged exposure to haemodialisys.
Immersive VR experiences that incorporate culturally significant artworks, historical sites, and traditional artistic expressions have the potential to deepen patients’ emotional engagement by fostering a sense of connection with their personal and collective histories. A study by Grossi et al.75 found that exposure to cultural heritage is positively associated with stress reduction, (lowering cortisol levels) and subjective wellbeing increase.
The cultural heritage as a booster for wellness
Similarly, work by Yim76 emphasized that integrating culturally meaningful content into therapeutic interventions enhances emotional resonance and reduces feelings of isolation among patients undergoing long-term treatment. The incorporation of cultural heritage elements in VR art therapy allows patients to reconnect with familiar symbols and narratives, evoking feelings of nostalgia and identity reinforcement which may be challenged in case of prolonged treatment due to a chronic disease. The reduction in symptoms of depression and tiredness reported in our study following participation in the VR sessions emphasizes the broader psychological benefits of integrating art therapy into patient care. Further, in line with the study of Bennington et al.,77 our study showed the potential of cultural heritage to be used in therapeutic context to enhance cognitive engagement and provide psychological relief by invoking positive memories and personal associations77.
By embracing art therapy in the form of immersive VR, enriched with cultural heritage elements, healthcare providers can not only improve emotional well-being but also contribute to a more holistic approach to patient care that recognizes the importance of psychological health alongside medical treatment in line with the concept of health supported by World Health Organization78.
In our research, patients expressed a high degree of presence and immersion during the VR sessions, which allowed them to temporarily escape the clinical context and experience feelings akin to being in a museum. On the contrary, patients reported a low sense of presence associated with being in hospital doing haemodialisys which aligns with research reporting a sense of disembodiment or transcendence associated with medical treatment for this chronic disease79,80. This is consistent with findings by Godley et al.81, where art therapy was associated with shortened hospital stays, improved recovery time, and reduced need for pain management. The significant effect of the VR art protocol on reducing negative emotions and enhancing the sense of presence indicates that art therapy can create a safe emotional space for patients, fostering resilience and improving overall treatment experiences. The good usability ratings reported by our participants also amplify the applicability of art therapy in routine clinical practice, as patients expressed a willingness to frequently engage with VR art experiences. This finding corroborates recent research by Clarke et al.82, which demonstrated that using art in therapeutic settings could nurture feelings of joy and satisfaction, ultimately improving patients’ quality of life.
Implications for clinical practice and future directions
Such acceptance of innovative art therapies highlights the need for healthcare providers to incorporate creative modalities to alleviate distress and improve coping mechanisms among patients undergoing intensive treatment regimens. By integrating cultural heritage into VR-based art therapy, we can offer patients a more profound and emotionally enriching experience, helping them navigate the complexities of chronic illness treatment with a stronger sense of identity and emotional well-being. Given the low stress scores reported during the conventional treatment in combination with the VR art protocol, it suggests a promising avenue for future research to explore immersive technologies as a standard adjunct in dialysis treatment protocols. Collectively, these findings emphasize the applicability of VR not solely as a diversion but as a viable palliative tool that can enhance patient experience, alleviate negative emotions, and ultimately improve quality of life not limited to hospital settings. Indeed, VR enables virtual experiences that would be difficult to achieve in practice, considering that patients are forced to remain attached to dialysis equipment for a long time. And this technology will be particularly beneficial not only for ambulatory patients but also for those forced to do dialysis every day at home.
The findings of our study highlighted the potential emotional and experiential benefits together with a good assessment of usability of the VR system used to deliver the ART-base protocol. However, several important challenges must be considered for broader implementation. One key limitation is that not all patients tolerate VR equally well; side effects such as dizziness, nausea, or eye strain, commonly referred to as cybersickness, can affect a subset of users, particularly those with vestibular sensitivities or neurological conditions83. Additionally, individual differences in familiarity with technology, cognitive capacity, and visual or motor impairments may limit the feasibility of VR use in certain patient populations. From a logistical standpoint, implementing VR across diverse clinical settings requires considerations related to equipment costs, staff training, hygiene protocols, and physical space requirements84. These factors may pose barriers in resource-limited environments. Therefore, while VR holds promise as a scalable tool to support emotional well-being, future research and implementation efforts must carefully address these practical and patient-centered concerns to ensure accessibility, safety, and equity in use.
Although our study focused on single-session VR intervention, we acknowledge that multi-session approaches, involving aesthetic or art-based experiences, may yield enhanced and more enduring effects for individuals with chronic conditions. Previous studies have explored the therapeutic potential of immersive VR environments that incorporate art, music, or contemplative visual experiences across multiple sessions85. For example, Godley et al.81 created an exhibition of various dynamic light art installations that investigated the potential impact of this experience on viewers’ sense of well-being in a mock healthcare setting. Similarly, Tymoszuk et al. (2020) conducted a longitudinal study using art museum experience, reporting that long-term and frequent exposition with certain arts activities is associated with higher levels of happiness, life satisfaction, self-realization, and control/autonomy in older adults86. These findings underscore the value of designing future interventions that leverage the immersive and aesthetic qualities of VR in a multi-session format with extended follow-up to assess long-term impact on emotional and cognitive outcomes in chronic care populations.
As we collected all the data through self-reported measures, further research will be needed to collect physiological and behavioral measures of stress, positive or negative emotions and cognitive load associated with CT and VR. Furtherly, the study involves a short-term assessment, and it is limited, for each condition, to one session only. As our study was intended to explore acceptability and usability by CRF patients, it should be read as a first look to possible palliative treatment that needs to be further developed to be used in prolonged treatments.
Moreover, the virtual tour consists of a unique museal visit which may not correspond necessary to the individual preferences for art styles. Future research should therefore consider all these limitations and involve different scenarios for the creation of a prolonged treatment in which heart rate variability; cortisol levels or electroencephalography may overcome the limitations of this study.
Finally, given the need to continue exploring innovative methodologies and technology, integrating artistic protocols into patient care could revolutionize how healthcare is delivered by fostering clinical environments that promote emotional healing alongside physical health.
Methods
Patients and study design
To be included in the study, participants must meet the following requirements: established diagnosis of chronic renal failure (CRF) for more than six months were enrolled; patients undergoing treatment; age between 18 and 90 years; absence of clinically proven serious visual, cognitive, or linguistic deficits that would make patients incapable of carrying out the virtual visit and answering the questionnaires; absence of further comorbid pathologies; absence of risks of visual epilepsy for which virtual reality could be a trigger.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Independent Etical Institutional Review Board of Santa Lucia Foundation (CE/2023_031). All participants signed a written informed consent.
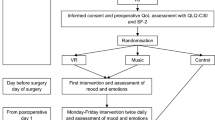
The study had a cross-over design in which, after the enrolment of patients, they were randomly allocated in two groups for the psychological assessment of their emotional trait as detailed below. As shown in Fig. 5, the first group received conventional therapy in the session immediately after the enrolment (session N), and after 30 min underwent a psychological evaluation with the Positive and Negative Affect Schedule (PANAS) as the main outcome for state assessment. In the successive session (N + 1), in the first 30 min of they also wore the VR headset and virtually visited the National Etruscan Museum of Rome. At the end of the virtual tour, they compiled PANAS for state assessment and other psychological scales as detailed below. According to the cross-over design, the other group of subjects had the VR protocol in the session N and CT in N + 1. During CT, patients were left free to do the same things they usually did during such as reading a newspaper or a book or interacting with their smartphones or listening to music.
The psychological scales were administered to each patient during the therapy by an experienced researcher that was also available for any doubt regarding the questionnaires.

Flow-chart of the study. PANAS is Positive and Negative Affect Schedule; CT stands for conventional treatment; VR is the administration of the virtual tour during a CT session.
Virtual reality equipment and content
Each subject sat wearing an Oculus Rift Head Mounted Display. The virtual environment, designed by using 3ds MAX 2018 and implemented in Unity 2018 game engine software consisted of a tour of the 3D reproduction of the National Etruscan Museum of Villa Giulia located in Rome, Italy. The virtual tour reproduced a visit such as the subject was walking into the museum. Among the artworks that can be viewed by patients there will be the sarcophagus of the spouses, the pediment of the temple of Pyrgi, the Apollo of Veii. To increase the engagement, a music accompanied the virtual visit: the music chosen was that of the so-called Mozart effect, the sonata for two pianos in D major K44887.
Psychological assessments
As described in Fig. 5, the experiment was performed during 2 consecutive sessions of conventional treatment- PANAS scale was administered to patients to measure the level of emotions considered as Trait at baseline, referring to their emotional state in the week before the inclusion in this research.
This evaluation, together with the collection of demographical information, was underwent before the first condition. The design of the study was a randomized cross-over. Hence, a group of patients received as first condition a conventional treatment or the experimental one in which dialysis is performed while wearing the headset for VR.
In the session of Conventional Treatment (CT), after 30 min of dialysis, the researcher administered to the patients the PANAS-State88, Edmonton Symptom Assessment System (ESAS)89, and Questionnaire referring to his/her emotional state in the last 30 min of therapy.
In the session with Virtual Reality (VR), the patient wore the headset mounted display and virtually visited a museum for 30 min during the dialysis. At the end of the visit, the researcher administered to the patients the same scales of CT session with the adjunction of the System Usability Scale (SUS90), .
The main outcome measure of this study was the Positive and Negative Affect Schedule (PANAS88), . PANAS is a 20-item self-report measure assessing positive affect (PA, related to 10 items) and negative affect (NA, related to the other 10 items). PA is associated with pleasurable engagement with the environment, whereas NA reflects a dimension of general distress summarising a variety of negative states such as anxiety and distress. Each item is rated on a five-point Likert Scale, ranging from 1 = Very Slightly or Not at all to 5 = Extremely, to measure the extent to which the effect has been experienced in a specified time frame. The PANAS was designed to measure affect in two main contexts: Trait, that refers to a previous period (in our study the week before therapy), or State, that refers to the present moment (in our study the last 30 min before the scale administration).
We also administered the Italian version of the Edmonton Symptom Assessment System (ESAS89), since a similar version was already used with patients undergoing dialysis69, to assess symptoms and discomfort associated to CT and VR. ESAS is a valid and reliable tool to assess on a visual analogue scale (ranging from 0 to 10) nine common symptoms experienced in palliative care settings.
A brief questionnaire with scores based on a Visual Analogue Scale (VAS, ranging from 0 to 10) were also administered to patients, with some questions specific for the sessions in which the VR was used (as detailed below).
Usability assessment
Since the usage of VR systems in healthcare protocols is continuously spreading, it is a good practise to assess patients’ comfort of new technological devices used as addons to their conventional treatment. For the evaluation of the usability of this VR protocol, we used the System Usability Scale (SUS, Italian version validated by Borsci et al.90. It consists of 10 items on a 5-point Likert scale, in which patient evaluates the VR features and property from a technical point of view.
Finally, like a previous study91, we recorded the level of stress, sense of agency and sense of presence associated with the VR session, and the stress associated to CT, using a numeric rating scale on 10 points.
Statistical analysis
The statistical analyses were performed using version 23 of IBM SPSS statistical software. Customized code was implemented for data visualization in MATLAB environment (MathWorks, 2020b version). Sample Size was estimated on the basis of a previous study using a 3D virtual tourism protocol for psychological after stressing events92. In that study, the effect sizes on PANAS scores ranged between 0.72 up to 0.920, depending on different scenarios. Setting an average effect size of 0.82, an alpha level of 5% and a power of 97% (software: GPower 3.1.97, Kiel University, Germany) we obtained a needed sample size of 26 subjects for having statistically significant results also using non-parametric tests. This number was also in line with that planned in another study about the use of virtual reality for palliative purposes [Perna et al.85. Data are reported in terms of means and standard deviations (SD) for continuous measures, as medians and interquartile ranges for ordinal measures, and as percentage for patient’s self-rating of stress associated with experimental conditions. The normal distribution of each variable was verified using the Kolgomorov-Smirnov test which revealed an assumption of normality for most of the variables considered with the exception for the visual scales. A 3 × 2 repeated measures analysis of variance (ANOVA) with a three-level “within subjects” factor, namely conditions (“State”, “CT”, “VR”), and a two-level between-subjects factor, that is poles (“positive” and “negative” emotions) was conducted. We used Wilcoxon for dependent sample to verify statistical difference between VR and CT conditions in terms of single emotions reported as single items of PANAS. Effect size (ES) for analysis of variance was computed through the partial-eta squared (pes) with the assumption of low, medium and large effect according to Cohen’s guidelines93. For pairwise comparisons, the Effect size was computed in terms of Cohen’s d, id est the ratio between the difference of the means computed in VR and CT conditions and divided by the standard deviation in CT condition. The chosen level of significance for all analysis was set at 5%, with the exception of post-hoc tests following Anova for which it was set at 2.5%.
Data availability
The data that supports the findings of this study are available from the corresponding author, upon reasonable request.
Abbreviations
- CRF:
-
Chronic renal failure
- CKD:
-
Chronic kidney disease
- GBD:
-
Global burden disease
- DALYs:
-
Disability-adjusted life years
- VR:
-
Virtual reality
- CT:
-
Conventional therapy
- PANAS:
-
Positive and negative affect schedule
- EDAS:
-
Edmonton Symptom Assessment System
- VAS:
-
Visual Analogue Scale
- SUS:
-
System Usability Scale
- SD:
-
Standard deviation
- ANOVA:
-
Analysis of variance
- ES:
-
Effect size
- pes:
-
Partial-eta squared
References
Fancourt, D. & Finn, S. What is the evidence on the role of the arts in improving health and well-being? A scoping review. (2020).
Rice, G., Ingram, J. & Mizan, J. Enhancing a primary care environment: a case study of effects on patients and staff in a single general practice. Br. J. Gen. Pract. 58(552), e1 (2008).
Cain, M., Lakhani, A. & Istvandity, L. Short and long term outcomes for culturally and linguistically diverse (cald) and at-risk communities in participatory music programs: a systematic review. Arts Health. 8(2), 105–124 (2016).
Kim, J. Effects of community-based group music therapy for children exposed to ongoing child maltreatment & poverty in South korea: A block randomized controlled trial. Arts Psychother. 54, 69–77 (2017).
Rollins, J. & Wallace, K. E. The vintage photograph project. Arts Health. 9(2), 167–185 (2017).
Stuckey, H. L. & Tisdell, E. J. The role of creative expression in diabetes: an exploration into the meaning-making process. Qual. Health Res. 20(1), 42–56 (2010).
Basso, R. V. & Pelech, W. J. A creative arts intervention for children with diabetes: part 1: development. J. PsychoSoc. Nurs. Ment. Health Serv. 46(10), 25–29 (2008).
Patil, V., Narayan, J., Sandhu, K. & Dwivedy, S. K. Integration of virtual reality and augmented reality in physical rehabilitation: a state-of-the-art review. Revol. Prod. Des. Healthc. Adv. Prod. Des. Des. Methods Healthc. 177–205 (2022).
Tieri, G., Morone, G., Paolucci, S. & Iosa, M. Virtual reality in cognitive and motor rehabilitation: facts, fiction and fallacies. Expert Rev. Med. Dev. 15(2), 107–117 (2018).
Hoffman, H. G. et al. The effectiveness of virtual reality for dental pain control: a case study. CyberPsychology Behav. 4(4), 527–535 (2001).
Ram, D. et al. Audiovisual video eyeglass distraction during dental treatment in children. Quintessence Int., 41(8). (2010).
McCabe, C., Roche, D., Hegarty, F. & McCann, S. Open window’: a randomized trial of the effect of new media Art using a virtual window on quality of life in patients’ experiencing stem cell transplantation. Psycho-Oncology 22(2), 330–337 (2013).
Iosa, M. et al. The Michelangelo effect: Art improves the performance in a virtual reality task developed for upper limb neurorehabilitation. Front. Psychol. 11, 611956 (2021).
De Giorgi, R. et al. Virtual Art therapy: application of Michelangelo effect to neurorehabilitation of patients with stroke. J. Clin. Med. 12(7), 2590 (2023).
Burrai, F. et al. Effects of virtual reality in patients undergoing dialysis: study protocol. Holist. Nurs. Pract. 33(6), 327–337 (2019).
Catto, G. R. (ed) Chronic Renal Failure, Vol. 3 (Springer Science & Business Media, 2012).
Fort, J. Chronic renal failure: a cardiovascular risk factor. Kidney Int. 68, S25–S29 (2005).
Palaka, E., Grandy, S., van Haalen, H., McEwan, P. & Darlington, O. The impact of CKD anaemia on patients: incidence, risk factors, and clinical outcomes—a systematic literature review. Int. J. Nephrol. 2020 (2020).
Racha, A. et al. Assessment of malnutrition in patients with chronic kidney disease undergoing Hemodialysis. J. Egypt. Soc. Nephrol. Transplantation. 20(3), 179 (2020).
Wang, X. H. & Price, S. R. March). Organ crosstalk contributes to muscle wasting in chronic kidney disease. In Seminars in Nephrology, Vol. 43, No. 2, 151409 (WB Saunders, 2023).
Adamczak, M., Ritz, E. & Wiecek, A. Carbohydrate metabolism in chronic renal disease. In Nutritional Management of Renal Disease, 29–41 (Academic Press, 2022).
Bikbov, B. et al. Global, regional, and national burden of chronic kidney disease, 1990–2017:a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 395(10225), 709–733 (2020).
van Haalen, H., Jackson, J., Spinowitz, B., Milligan, G. & Moon, R. Impact of chronic kidney disease and anemia on health-related quality of life and work productivity: analysis of multinational real-world data. BMC Nephrol. 21(1), 1–15 (2020).
World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life (World Health Organization, 2002).
Liu, Y. et al. Global incidence and death estimates of chronic kidney disease due to hypertension from 1990 to 2019, an ecological analysis of the global burden of diseases 2019 study. BMC Nephrol. 24(1), 352 (2023).
Senanayake, S. et al. Depression and psychological distress in patients with chronic renal failure: prevalence and associated factors in a rural district in Sri Lanka. J. Psychosom. Res. 112, 25–31 (2018).
Levy, N. B. Psychological reactions to machine dependency: Hemodialysis. Psychiatr. Clin. North Am. 4(2), 351–363 (1981).
Simoes e Silva, A. C., Miranda, A. S., Rocha, N. P. & Teixeira, A. L. Neuropsychiatric disorders in chronic kidney disease. Front. Pharmacol. 10, 932 (2019).
Hedayati, S. S. et al. Association between major depressive episodes in patients with chronic kidney disease and initiation of dialysis, hospitalization, or death. Jama 303(19), 1946–1953 (2010).
Kimmel, P. L. et al. Psychiatric illness and mortality in hospitalized ESKD dialysis patients. Clin. J. Am. Soc. Nephrology: CJASN. 14(9), 1363 (2019).
Tavallaii, S. A., Ebrahimnia, M., Shamspour, N. & Assari, S. Effect of depression on health care utilization in patients with end-stage renal disease treated with Hemodialysis. Eur. J. Intern. Med. 20(4), 411–414 (2009).
Gebrie, M. H. & Ford, J. Depressive symptoms and dietary non-adherence among end stage renal disease patients undergoing hemodialysis therapy: systematic review. BMC Nephrol. 20(1), 1–7 (2019).
Zhang, Z. et al. Association of depressive symptoms with rapid kidney function decline in adults with normal kidney function. Clin. J. Am. Soc. Nephrol. 16(6), 889 (2021).
Keskin, G. Resilience in patients with dialysis-dependent renal failure: evaluation in terms of depression, anxiety, traumatic growths. Appl. Nurs. Res. 65, 151575 (2022).
Ridner, S. H. Psychological distress: concept analysis. J. Adv. Nurs. 45(5), 536–545 (2004).
Cox, K. J., Parshall, M. B., Hernandez, S. H., Parvez, S. Z. & Unruh, M. L. Symptoms among patients receiving in-center hemodialysis: A qualitative study. Hemodial. Int. 21(4), 524–533 (2017).
Cohen, S. D., Cukor, D. & Kimmel, P. L. Anxiety in patients treated with Hemodialysis. Clin. J. Am. Soc. Nephrol. 11(12), 2250–2255 (2016).
Gaina, A. M. et al. A systematic review of virtual reality’s impact on anxiety during palliative care. In Healthcare, Vol. 12, No. 24, 2517 (MDPI, 2024).
Maggio, M. G. et al. The growing use of virtual reality in cognitive rehabilitation: fact, fake or vision? A scoping review. J. Natl. Med. Assoc. 111(4), 457–463 (2019).
Indovina, P. et al. Virtual reality as a distraction intervention to relieve pain and distress during medical procedures. Clin. J. Pain. 34(9), 858–877 (2018).
De Bartolo, D. et al. Effect of different music genres on gait patterns in Parkinson’s disease. Neurol. Sci. 41, 575–582 (2020).
Chirico, A. et al. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J. Cell. Physiol. 235(6), 5353–5362 (2020).
Ahmadpour, N. et al. Virtual reality interventions for acute and chronic pain management. Int. J. Biochem. Cell Biol. 114, 105568 (2019).
Nunna, M., Dasaraju, R. K., Kamatham, R., Mallineni, S. K. & Nuvvula, S. Comparative evaluation of virtual reality distraction and counter-stimulation on dental anxiety and pain perception in children. J. Dent. Anesth. Pain Med. 19(5), 277 (2019).
Weiss, P. L., Kizony, R., Feintuch, U. & Katz, N. Virtual reality in neurorehabilitation. Textbook Neural Repair. Rehabilitation. 51(8), 182–197 (2006).
Schubert, T., Friedmann, F. & Regenbrecht, H. The experience of presence: factor analytic insights. Teleoperators Virtual Environ. 10(3), 266–281 (2001).
Pallavicini, F., Pepe, A. & Minissi, M. E. Gaming in virtual reality: what changes in terms of usability, emotional response and sense of presence compared to non-immersive video games? Simul. Gaming. 50(2), 136–159 (2019).
Pavic, K., Vergilino-Perez, D., Gricourt, T. & Chaby, L. Because i’m happy—an overview on fostering positive emotions through virtual reality. Front. Virtual Real. 3, 788820 (2022).
Felnhofer, A. et al. Is virtual reality emotionally arousing? Investigating five emotion inducing virtual park scenarios. Int. J. Hum. Comput. Stud. 82, 48–56 (2015).
Marín-Morales, J. et al. Affective computing in virtual reality: emotion recognition from brain and heartbeat dynamics using wearable sensors. Sci. Rep. 8(1),13657 (2018).
Diniz Bernardo, P., Bains, A., Westwood, S. & Mograbi, D. C. Mood induction using virtual reality: A systematic review of recent findings. J. Technol. Behav. Sci. 6, 3–24 (2021).
Di Pompeo, I., D’Aurizio, G., Burattini, C., Bisegna, F. & Curcio, G. Positive mood induction to promote well-being and health: A systematic review from real settings to virtual reality. J. Environ. Psychol. 102095 (2023).
Serrano, B., Baños, R. M. & Botella, C. Virtual reality and stimulation of touch and smell for inducing relaxation: A randomized controlled trial. Comput. Hum. Behav. 55, 1–8 (2016).
Anderson, A. P. et al. Relaxation with immersive natural scenes presented using virtual reality. Aerosp. Med. Hum. Perform. 88(6), 520–526 (2017).
Chirico, A. et al. Effectiveness of immersive videos in inducing awe: an experimental study. Sci. Rep. 7(1), 1218 (2017).
Chirico, A., Ferrise, F., Cordella, L. & Gaggioli, A. Designing Awe in virtual reality: an experimental study. Front. Psychol. 8, 293522 (2018).
Chirico, A., Clewis, R. R., Yaden, D. B. & Gaggioli, A. Nature versus Art as elicitors of the sublime: A virtual reality study. PLoS ONE. 16(3), e0233628 (2021).
Ishizu, T. & Zeki, S. Toward a brain-based theory of beauty. PLoS ONE. 6(7), e21852 (2011).
Ishizu, T. & Zeki, S. The brain’s specialized systems for aesthetic and perceptual judgment. Eur. J. Neurosci. 37(9), 1413–1420 (2013).
Ishizu, T. & Zeki, S. A Neurobiological enquiry into the origins of our experience of the sublime and beautiful. Front. Hum. Neurosci. 8, 891 (2014).
Takano, R. & Nomura, M. Neural representations of awe: distinguishing common and distinct neural mechanisms. Emotion 22(4), 669 (2022).
Jiang, T. et al. The unique nature and psychosocial implications of Awe. Nat. Reviews Psychol. 3(7), 475–488 (2024).
Chirico, A. & Yaden, D. B. The Function of Emotions (ed. Lench, H. C.) 221–233 (Springer,2018).
Bondi, E. et al. Integrating virtual reality, electroencephalography, and transcranial magnetic stimulation to study the neural correlates of awe experiences: The SUBRAIN protocol. PLoS ONE. 20(4), e0302762 (2025).
Freedberg, D. & Gallese, V. Motion, emotion and empathy in esthetic experience. Trends Cogn. Sci. 11(5), 197–203 (2007).
Di Dio, C. et al. Human, nature, dynamism: the effects of content and movement perception on brain activations during the aesthetic judgment of representational paintings. Front. Hum. Neurosci. 9, 705 (2016).
Knoblich, G. Self-recognition: body and action. Trends Cogn. Sci. 6(11), 447–449 (2002).
Weber, C., Flores, M., Wheele, V., Miedema, T. P., White, E. V. & E., & Patients’ health & well-being in inpatient mental health-care facilities: a systematic review. Front. Psychiatry. 12, 758039 (2022).
Davison, S. N., Jhangri, G. S. & Johnson, J. A. Cross-sectional validity of a modified Edmonton symptom assessment system in dialysis patients: a simple assessment of symptom burden. Kidney Int. 69(9), 1621–1625 (2006).
Bangor, A., Kortum, P. T. & Miller, J. T. An empirical evaluation of the system usability scale. Intl J. Human–Computer Interact. 24(6), 574–594 (2008).
Lewis, J. R. & Sauro, J. Item benchmarks for the system usability scale. J. Usability Stud., 13(3) (2018).
Oliva, A., Iosa, M., Antonucci, G. & De Bartolo, D. Are neuroaesthetic principles applied in Art therapy protocols for neurorehabilitation? A systematic mini-review. Front. Psychol. 14, 1158304 (2023).
Bell, J. G., McHale, J., Elliott, J. O. & Heaton, W. The impact of art therapy on anxiety and hope in patients with gynecologic cancer undergoing chemotherapy. Arts Psychother. 80, 101947 (2022).
Zubala, A., Kennell, N. & Hackett, S. Art therapy in the digital world: an integrative review of current practice and future directions. Front. Psychol. 12, 595536 (2021).
Grossi, E., Tavano Blessi, G. & Sacco, P. L. Magic moments: determinants of stress relief and subjective wellbeing from visiting a cultural heritage site. Cult. Med. Psychiatry. 43(1), 4–24 (2019).
Yim, S. H. Cultural heritage through the lens of community psychology and narrative therapy: a community project on Chinese and Vietnamese diaspora in London. Int. J. Herit. Stud. 28(8), 970–983 (2022).
Bennington, R., Backos, A., Harrison, J., Reader, A. E. & Carolan, R. Art therapy in art museums: promoting social connectedness and psychological well-being of older adults. Arts Psychother. 49, 34–43 (2016).
World Health Organization. Integrating Mental Health into Primary Care: a Global Perspective (World Organization of National Colleges, Academies, & Academic Associations of General Practitioners/Family Physicians, 2008).
Shaw, R. Being-in-dialysis: the experience of the machine–body for home dialysis users. Health 19(3), 229–244 (2015).
King, R. A. The spontaneous transcendental out-of-body experience: A beneficial absorption response to threat. J. Mind Behav. 45(1), 49–65 (2024).
Godley, L., Frasso, R., Igoe, T., Erel, Y. & LeNoir, J. The use of immersive light-based art for well-being. In IOP Conference Series: Earth and Environmental Science, Vol. 1320, No. 1, 012008 (IOP Publishing, 2024).
Clarke, J., Crosbie, A. & Green, K. Safety in a person-centred, garden-based Art therapy group for people with dementia. Int. J. Art Ther. 1–10. (2024).
Biswas, N., Mukherjee, A. & Bhattacharya, S. Are you feeling sick?–A systematic literature review of cybersickness in virtual reality. ACM Comput. Surveys. 56(11), 1–38 (2024).
Kouijzer, M. M., Kip, H., Bouman, Y. H. & Kelders, S. M. Implementation of virtual reality in healthcare: a scoping review on the implementation process of virtual reality in various healthcare settings. Implement. Sci. Commun. 4(1), 67 (2023).
Perna, M. S., Lund, M. S. W. L., White, S., Minton, O. & N., & The potential of personalized virtual reality in palliative care: a feasibility trial. Am. J. Hospice Palliat. Medicine®. 38(12), 1488–1494 (2021).
Tymoszuk, U., Perkins, R., Spiro, N., Williamon, A. & Fancourt, D. Longitudinal associations between short-term, repeated, and sustained arts engagement and well-being outcomes in older adults. J. Gerontol. Ser. B. 75(7), 1609–1619 (2020).
Rauscher, F. H. Music and spatial task performance. Nature 365, 611 (1993).
Terraciano, A., McCrae, R. R. & Costa, P. T. Jr Factorial and construct validity of the Italian positive and negative affect schedule (PANAS). Eur. J. Psychol. Assess. 19(2), 131 (2003).
Ripamonti, C. et al. Italian version of the Edmonton Symptom Assessment System (ESAS)–Total Care (TC): development and psychometric validation in patients undergoing cancer treatment or follow-up. Support. Care Cancer. 1–11 (2022).
Borsci, S., Federici, S. & Lauriola, M. On the dimensionality of the system usability scale: a test of alternative measurement models. Cogn. Process. 10, 193–197 (2009).
Frisanco, A., Schepisi, M., Tieri, G. & Aglioti, S. M. Embodying the avatar of an omnipotent agent modulates the perception of one’s own abilities and enhances feelings of invulnerability. Sci. Rep. 12(1), 21585 (2022).
Zhang, S., Tan, Y., Zhong, Y., Yuan, J. & Ding, Y. Psychological recovery effects of 3D virtual tourism with real scenes–a comparative study. Inform. Technol. Tourism. 25(1), 71–103 (2023).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences (Academic Press, 2013).
Acknowledgements
The study has been conducted with financial support from the European Commission within the HORIZON Action Grant Budget Based (Topic: HORIZON-CL2-2023-HERITAGE-01-04), Project 101132488, META-MUSEUM: Moving Emotions towards confidence in the Transformative Appropriation for a Meaningful Understanding of cultural heritage: a neuroScientific approach to EUropean Museums.
Author information
Authors and Affiliations
Contributions
Conceptualization M.I., Methodology D.D.B., G.T., M.I., Software G.T., Validation D.D.B., R.D.G., M.I., Formal Analysis D.D.B., Investigation R.D.G., F.G., F.A., C.R., A.C., M.S., Resources D.D.B., R.D.G., G.T., M.S., , M.I., Data Curation D.D.B., R.D.G., F.G., F.A., C.R., A.C., Writing original draft D.D.B., Writing – Reviewing and Editing All authors, Visualization D.D.B., Supervision R.D.G., M.S., G.A., M.I., Project administration R.D.G., Funding acquisition G.A., M.I.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
De Bartolo, D., De Giorgi, R., Tieri, G. et al. Bringing the museum into the hospital to promote cultural wellness in patients undergoing haemodialysis through a virtual reality tour. Sci Rep 15, 28168 (2025). https://doi.org/10.1038/s41598-025-11859-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-11859-1
