
Abstract
The leadless pacemaker represents a significant advancement in cardiac pacing technology. This retrospective, single-center cohort study aims to evaluate whether acute impedance and pacing thresholds can predict long-term pacing capture threshold (PCT) in Chinese patients implanted with leadless pacemakers. A total of 409 Chinese patients who underwent Micra leadless pacemaker implantation between January 2019, and November 2023, were included in the study.Among them, 19 patients were classified as having very high PCT levels due to elevated levels persisting from implantation to the final follow-up. Receiver operating characteristic (ROC) curve analysis revealed that acute PCT is a significant predictor of long-term PCT elevation, with an area under the curve (AUC) of 0.733, a sensitivity of 77.8%, and a specificity of 61.1%.Similarly, acute pacing impedance was found to significantly predict long-term PCT elevation, with an AUC of 0.689, a sensitivity of 83.3%, and a specificity of 50.9%. Furthermore, multivariate Cox proportional hazards regression analysis identified acute PCT ≥ 1.0 V (HR = 3.62, 95% CI = 1.19–11.00, p < 0.05) as an independent predictor of long-term PCT elevation. Additionally, acute pacing impedance < 800 Ω (HR = 3.76, 95% CI = 1.17–12.10, p < 0.05) was found to independently predict long-term PCT elevation. These findings underscore the importance of monitoring acute parameters during implantation to ensure optimal long-term device performance and reliability.
Similar content being viewed by others

Leadless pacemakers represent a significant advancement in cardiac pacing technology, offering several advantages over traditional transvenous pacemakers. These advantages include a lower risk of infection, a reduced incidence of lead-related complications, and a decreased occurrence of pocket hematomas1.The Micra™ leadless pacemaker (Medtronic, USA) has seen increasing adoption among patients requiring single-chamber ventricular pacing, particularly those with contraindications to transvenous systems or those at high risk of infection2.
Despite these advantages, optimizing implantation parameters to ensure long-term device performance remains a critical concern. The pacing capture threshold (PCT) is a key parameter that reflects the energy required for effective cardiac stimulation. An elevated PCT can necessitate increased pacing output, which reduces battery longevity and may lead to early device replacement3. Previous studies have suggested that acute parameters measured during implantation, such as impedance and PCT, can predict long-term pacing outcomes4,5. However, data on the predictive value of these acute parameters for long-term outcomes in the Chinese population are still limited. A thorough understanding of the relationship between acute electrical parameters and long-term pacing performance is essential for improving patient outcomes, optimizing device programming, and enhancing the cost-effectiveness of leadless pacemaker therapy. Therefore, this study aims to evaluate the predictive value of acute impedance and pacing thresholds in determining long-term PCT outcomes in Chinese patients with leadless pacemakers.
Methods
Study population
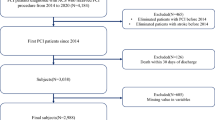
This single-center, retrospective cohort study involved 409 patients who underwent implantation of the Micra Transcatheter Leadless Pacing System (Medtronic, Minneapolis, USA) at the Department of Cardiology, West China Hospital, Sichuan University, from January 2019 to November 2023. All patients provided written informed consent prior to the procedure.
Baseline clinical data, encompassing demographic information, indications for pacemaker implantation, echocardiographic parameters, and comorbid conditions, were collected for each patient. Information on patient follow-up was carefully documented. Patients who were lost to follow-up or had incomplete clinical data were excluded from the final analysis. The reasons for missing data included inability to contact the patient after discharge or incomplete medical records.The experimental protocol was approved by the Ethics Committee of West China Hospital, Sichuan University (Approval No.: 2019(1079)). The study was conducted in accordance with the Declaration of Helsinki and received approval from the institutional review board.
Leadless pacemaker implantation procedure
Temporary pacemaker placement
In this study, all patients scheduled for the Micra leadless pacemaker implantation underwent comprehensive preoperative evaluations. For those identified as pacemaker-dependent, we conducted an assessment of their electrocardiographic characteristics to determine the necessity for temporary pacing before the procedure. Temporary pacemaker insertion was performed via the right femoral vein, using standard techniques with local anesthesia. Post-insertion, we meticulously monitored the patients’ hemodynamic status and verified appropriate pacing function. After the successful implantation of the leadless pacemaker, the temporary pacemaker was promptly removed, prioritizing patient safety and comfort throughout the procedure.
Leadless pacemaker implantation
The procedure began with flushing all devices using heparinized saline. Local anesthesia was administered with lidocaine, followed by a puncture of the right femoral vein. The access site was sequentially dilated with 8 F, 12 F, and 18 F dilator sheaths. A 27 F puncture sheath was then introduced after a standard intravenous heparin bolus (50 U/kg) was administered.
The delivery system was advanced into the right atrium and navigated across the tricuspid valve into the right ventricle. Using fluoroscopic guidance in the right anterior oblique (RAO) 30°and left anterior oblique (LAO) 45°views, the pacemaker was positioned in the mid-septal region of the right ventricle. Once the position and stability were confirmed, the pacemaker was deployed, and a pull-and-hold test was performed to ensure adequate fixation with at least two tines. Pacing threshold, sensing, and impedance were then measured and verified.
Afterward, the tether was cut, and the delivery system was then withdrawn.The puncture site of the procedure was sutured and covered with a pressure dressing. Patients were instructed to maintain bed rest for 24 h, and sutures were removed 10 days post-procedure.
Follow-up
Acute parameters, including R-wave sensing amplitude, PCT, and pacing impedance, were measured and recorded intraoperatively during device implantation. Subsequent PCT measurements were conducted at 3, 6, and 12 months post-implantation during routine follow-up visits.
Throughout the follow-up period, patients were categorized into the Very high PCT group if their PCT exceeded 2.0 V/0.24 ms or increased by more than 0.5 V/0.24 ms from implantation to the final follow-up. Patients who did not meet these criteria were classified as part of the normal PCT group. At each visit, the programmed pacing parameters were reviewed, and any adverse events related to the Micra leadless pacemaker were carefully evaluated.
Statistical analysis
Data are presented as means ± standard deviations (SD) for continuous variables and as frequencies (%) for categorical variables. To investigate the relationship between acute electrical parameters and the risk of elevated PCT, a multivariate Cox proportional hazards regression model was employed to estimate odds ratios (ORs) and 95% confidence intervals. Variables included in the multivariate Cox regression model were selected based on prior clinical evidence and statistical significance in univariate analysis (P < 0.05). No stepwise variable selection was performed. All clinically relevant factors and those significant in univariate analysis were entered into the model.
The diagnostic performance of acute electrical parameters in predicting elevated PCT was evaluated using receiver operating characteristic (ROC) curves. Pairwise comparisons of the area under the curve (AUC) values for the two parameters were performed. A two-tailed p-value of < 0.05 was deemed statistically significant. All analyses were conducted using Empower (R) (X&Y Solutions, Inc., Boston, MA) and R software (http://www.R-project.org).
Results
Baseline characteristics
Among 409 patients undergoing leadless pacemaker implantation (Table 1), 249 (60.9%) received devices for atrioventricular block (AVB), and 177 (43.3%) for sinus node dysfunction (SND), with 17 patients (4.2%) having overlapping indications. The selection of leadless pacing for SND was individualized and primarily indicated in patients with an increased risk of infection or challenging vascular anatomy.
There were no significant differences between the normal and very high PCT groups in terms of age, sex, body mass index (BMI), or left ventricular ejection fraction (LVEF). However, comorbidities such as Alzheimer’s disease (10.53% vs. 1.80%, p = 0.011) and chronic obstructive pulmonary disease (COPD) (31.58% vs. 13.08%, p = 0.023) were significantly more prevalent in the very high PCT group.
Electrical performance during acute procedure and followup
Table 2 summarizes the acute electrical parameters recorded immediately after implantation and at the final follow-up. Immediately after implantation, the normal PCT group demonstrated significantly lower PCT values and higher pacing impedance compared to the very high PCT group (PCT: 0.59 ± 0.32 V/0.24 ms vs. 0.90 ± 0.45 V/0.24 ms, p < 0.001; impedance: 858.7 ± 270.4 Ω vs. 714.4 ± 199.2 Ω, p = 0.026).
At the final follow-up, the normal PCT group continued to display significantly lower PCT values and higher pacing impedance compared to the very high PCT group (PCT: 0.51 ± 0.16 V/0.24 ms vs. 1.82 ± 0.64 V/0.24 ms, p < 0.001; impedance: 613.87 ± 141.54 Ω vs. 480.53 ± 67.37 Ω, p < 0.001). Additionally, the R-wave amplitude was significantly lower in the very high PCT group compared to the normal PCT group at follow-up (9.85 ± 3.85 mV vs. 11.94 ± 4.08 mV, p = 0.035).
The ROC curve analysis for predicting the very high PCT group
The ROC curve analysis shown in Fig. 1 illustrates the ability to predict membership in the very high PCT group at the final follow-up. The area under the curve (AUC) for PCT was 0.733, indicating moderate predictive accuracy, while the AUC for pacing impedance was 0.689. The sensitivity values were 77.8% for PCT and 83.3% for pacing impedance, with corresponding specificities of 61.1% and 50.9%. These results demonstrate both metrics in identifying patients at risk of very high PCT outcomes.

ROC curves of predictors of categorization into the Very high PCT group. Model 1: Pacing threshold–AUC, 0.733.Model 2: Pacing impedance–AUC, 0.689.Compare 2 models: Comparison of the ROC Model 1 and ROC Model 2. ROC indicates receiver operating characteristic; PCT indicates pacing capture threshold; and AUC indicates area under the curve.
A comparison of the two ROC models revealed no statistically significant difference in their predictive performance (p = 0.471).
A multivariate Cox regression analysis for predicting the very high PCT group
Table 3 summarizes the variables evaluated for inclusion in the multivariable Cox model.In Model I, multivariate Cox regression analysis identified pacing impedance values of < 800 Ω (OR = 4.09, 95% CI: 1.34–12.52, p = 0.014), < 650 Ω (OR = 2.88, 95% CI: 1.13–7.38, p = 0.027), and < 600 Ω (OR = 4.77, 95% CI: 1.73–13.16, p = 0.003) as significant independent predictors of very high PCT classification. Additionally, pacing thresholds of ≥ 1.0 V (OR = 3.96, 95% CI: 1.48–10.61, p = 0.006) and ≥ 1.5 V (OR = 6.04, 95% CI: 1.71–21.35, p = 0.005) were also identified as significant predictors.
In Model II, which adjusted for additional comorbidities such as coronary artery disease, hypertension, atrial fibrillation, diabetes, dyslipidemia, dialysis, chronic kidney disease, stroke, chronic obstructive pulmonary disease (COPD), infection, cancer, and Alzheimer’s disease, most associations remained significant. Specifically, pacing impedances of < 800 Ω (OR = 3.76, 95% CI: 1.17–12.10, p = 0.027) and < 600 Ω (OR = 4.00, 95% CI: 1.27–12.58, p = 0.018), together with pacing thresholds of ≥ 1.0 V (OR = 3.62, 95% CI: 1.19–11.00, p = 0.024) and ≥ 1.5 V (OR = 8.51, 95% CI: 1.96–36.94, p = 0.004), remained significantly associated with very high PCT classification. However, pacing impedance of < 650 Ω (OR = 2.47, 95% CI: 0.91–6.71, p = 0.077) did not retain statistical significance following adjustment.
The proportion of patients in the normal PCT group differed significantly from that in the very high PCT group at threshold values of ≥ 1.0 V (p = 0.002) and ≥ 1.5 V (p < 0.001), but not at ≥ 2.0 V (p = 0.705). (Fig. 2)

The graph illustrates the distribution of patients by PCT in two groups: the Normal PCT group and the Very high PCT group. The pacing threshold is categorized into three ranges: ≥1.0 V, ≥ 1.5 V, and ≥ 2.0 V, each presented with the corresponding percentage of patients. PCT: pacing capture threshold.
Significant differences were also observed between groups at all impedance cutoff levels: <800 Ω (p = 0.014), < 650 Ω (p = 0.018), and < 600 Ω (p = 0.001). (Fig. 3)

The graph shows the distribution of patients by pacing impedance levels in two groups: the Normal PCT group and the Very high PCT group. The pacing impedance is categorized into three ranges: <800 Ω, < 650 Ω, and < 600 Ω, with the corresponding percentages of patients represented for each group. PCT: pacing capture threshold.
Discussion
In this retrospective study of a Chinese cohort, we demonstrate that elevated acute-phase pacing thresholds (≥ 1.0 V) and reduced impedance (< 800 Ω) are significant predictors of subsequent pacing threshold instability. These findings underscore the practical importance of monitoring electrical parameters immediately after leadless pacemaker implantation to better assess long-term device performance and patient prognosis.
As suggested by Mitacchione et al., intraoperative R-wave monitoring is useful, but our findings suggest that pacing threshold and impedance are even more reliable indicators in the acute Chinese patient setting6.Prior research has established the predictive value of acute impedance cutoffs (600–800 Ω) for long-term pacing outcomes5,7,8. Our data support these thresholds in the Chinese context and further suggest that 1.0 V is an important acute-phase cutoff for pacing threshold, possibly due to anatomical or procedural factors unique to this population.
Intraoperative clinical decision-making
Our findings have direct relevance to intraoperative management strategies. The Micra™ LP manufacturer recommends a pacing threshold ≤ 1.0 V to optimize battery longevity and avoid unnecessary device repositioning9,10. Elevated thresholds during implantation may prompt additional device manipulation, which increases the risk of serious complications (e.g., cardiac perforation)4. Evidence linking thresholds ≥ 1.5 V and 2.0 V to the need for repositioning and suboptimal long-term thresholds emphasizes the value of real-time monitoring and timely intervention4,5. Our results suggest that when an acute-phase threshold meets or exceeds 1.0 V, clinicians should carefully weigh the risks and benefits of repositioning, especially in patients with multiple comorbidities.
Post-implantation follow-up implications
Proactive follow-up of patients with borderline acute-phase device parameters is warranted. Identifying those at higher risk of threshold instability enables early, targeted interventions and helps prevent late device failures. Our study supports the adoption of intensive post-discharge monitoring protocols for this high-risk group within Chinese populations. This approach also allows for technological interventions—such as retrieval systems—only when truly needed, optimizing resource use and minimizing procedural risk11,12.
Population-specific risk stratification
Our study also identified Alzheimer’s disease and COPD as independent risk factors for pacing instability, underscoring the importance of population-tailored risk models. These findings align with the i-LEAPER registry13.
The main limitation of this study is its retrospective design, which poses a risk for selection bias. Patients who were lost to follow-up or had incomplete clinical data were excluded from the final analysis, which may introduce further selection bias and affect the generalizability of our results. Additionally, all patients were recruited from a single geographic area, potentially limiting external validity. Although every effort was made to perform complete data collection, missing data or loss to follow-up may still introduce bias. In this study, chronic threshold evaluation was conducted around 12 months post-implantation; thus, prospective studies with more frequent, longitudinal follow-up are needed. Despite these limitations, our findings are consistent with prior mechanistic studies4,5. Further multicenter research involving broader populations is recommended to extend our results.
Conclusion
Acute pacing parameters, including impedance and PCT, play a crucial role in predicting long-term outcomes in Chinese patients with leadless pacemakers. Our study reveals that long-term pacing stability is reliably forecasted by an acute-phase impedance below 800 Ω or an acute-phase PCT of 1.0 V or greater. These findings emphasize the critical importance of monitoring acute parameters during the implantation process to achieve optimal long-term device performance and reliability.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due privacy/ethical restrictions but are available from the corresponding author on reasonable request.
References
Reddy, V. Y. et al. Percutaneous implantation of an entirely intracardiac leadless pacemaker. N Engl. J. Med. 373, 1125–1135 (2015).
Jelisejevas, J. et al. Leadless pacemaker implantation in patients with a prior conventional pacing system. CJC Open. 6, 649–655 (2024).
Vouliotis, A. I. et al. Leadless pacemakers: current achievements and future perspectives. Eur. Cardiol. 18, e49 (2023).
Piccini, J. P. et al. Long-Term outcomes in leadless Micra transcatheter pacemakers with elevated thresholds at implantation: results from the Micra transcatheter pacing system global clinical trial. Heart Rhythm. 14, 685–691 (2017).
Kiani, S. et al. A predictive model for the Long-Term electrical performance of a leadless transcatheter pacemaker. JACC Clin. Electrophysiol. 7, 502–512 (2021).
Mitacchione, G. et al. Intraoperative sensing increase predicts Long-Term pacing threshold in leadless pacemakers. J. Interv Card Electrophysiol. 63, 679–686 (2022).
Tolosana, J. M. et al. Very high pacing thresholds during Long-Term Follow-Up predicted by a combination of implant pacing threshold and impedance in leadless transcatheter pacemakers. J. Cardiovasc. Electrophysiol. 31, 868–874 (2020).
Morita, J. et al. Predictors of pacing capture threshold exacerbation after leadless pacemaker implantation. Int. Heart J. 64, 602–605 (2023).
Ritter, P. et al. The rationale and design of the Micra transcatheter pacing study: safety and efficacy of a novel miniaturized pacemaker. Europace 17, 807–813 (2015).
Coates, S. & Thwaites, B. The Strength-Duration curve and its importance in pacing efficiency: A study of 325 pacing leads in 229 patients. Pacing Clin. Electrophysiol. 23, 1273–1277 (2000).
Li, J. et al. Safety and efficacy of leadless pacemaker retrieval. J. Cardiovasc. Electrophysiol. 30, 1671–1678 (2019).
Afzal, M. R. et al. Techniques for successful early retrieval of the Micra transcatheter pacing system: A worldwide experience. Heart Rhythm. 15, 841–846 (2018).
Mitacchione, G. et al. Leadless pacemakers in patients with different stages of chronic kidney disease: Real-World data from the updated I-Leaper registry. Heart Rhythm. 22, 325–331 (2025).
Funding
The study was supported by Natural Science Foundation of Sichuan Province (Grant No. 22NSFSC0801).
Author information
Authors and Affiliations
Contributions
Xin Zhang: data acquisition, data analysis, data interpretation, and manuscript drafting and review;.Lingyun Jiang, Yuanning Xu and Xuehui Liu : data acquisition, data interpretation, and manuscript review; Xingbin liu: study concept and design, data analysis, data interpretation, manuscript review, and study supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, X., Jiang, L., Xu, Y. et al. Retrospective evaluation of the predictive value of acute pacing capture threshold for long-term outcomes in Chinese patients with leadless pacemakers. Sci Rep 15, 29206 (2025). https://doi.org/10.1038/s41598-025-15213-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-15213-3
