
Abstract
To investigate the association between ABCB1 (2677T > G) (rs2032582) polymorphism and lipid-lowering efficacy of atorvastatin with long-term prognosis in patients with cerebral ischemic stroke (CIS). A prospective cohort of 127 CIS patients admitted to Xuchang Central Hospital from January to December 2021 was consecutively enrolled. ABCB1 (2677T > G) genotypes were determined using digital fluorescence molecular hybridization technology, categorizing patients into GG (n = 48), GT (n = 49), and TT (n = 30) groups. All patients received oral atorvastatin 20 mg/day. Lipid profile changes (pre-treatment vs. 2-month post-treatment) were analyzed via analysis of covariance (ANCOVA). Treatment efficacy was defined as achieving serum LDL-C < 1.8 mmol/L, and binary logistic regression analysis was used to explore the impact of ABCB1(2677T > G) gene polymorphism on the lipid-lowering efficacy of atorvastatin. All patients were followed up for 36 months post-discharge to compare differences in long-term prognosis among the three groups. Genotype distribution followed Hardy-Weinberg equilibrium (χ2 = 3.225, P = 0.199). In both the additive and recessive models with age as a covariate, significant differences were observed among the three groups in ΔLDL-C, ΔLDL-C/LDL-C, Δ(LDL-C/HDL-C), and Δ(LDL-C/HDL-C)/(LDL-C/HDL-C) (additive model: FΔLDL−C = 4.198, P = 0.001; FΔLDL−C/LDL−C = 3.042, P = 0.013; FΔ(LDL−C/HDL−C) = 3.870, P = 0.003; FΔ(LDL−C/HDL−C)/(LDL−C/HDL−C) = 2.551, P = 0.031. Recessive model: FΔLDL−C = 5.142, P = 0.002; FΔLDL−C/LDL−C = 3.539, P = 0.017; FΔ(LDL−C/HDL−C) = 5.938, P = 0.001; FΔ(LDL−C/HDL−C)/(LDL−C/HDL−C) = 4.312, P = 0.006). In the dominant model with age as a covariate, ABCB1(2677T > G) gene polymorphism significantly affected Δ(LDL/HDL) (F = 3.571, P = 0.016), but had no significant effect on ΔLDL-C, ΔLDL-C/LDL-C, or Δ(LDL-C/HDL-C)/(LDL-C/HDL-C) (all P > 0.05). Binary logistic regression analysis showed that ABCB1(2677T > G) genotype was an independent risk factor affecting the lipid-lowering efficacy of atorvastatin. In the additive model, GG carriers exhibited 3.181-fold higher efficacy than TT (OR = 3.181, 95%CI:1.159 ~ 8.730, P = 0.025).In the recessive model, GG genotype showed 3.141-fold superiority over T-allele carriers (OR = 3.141, 95%CI:1.397 ~ 7.061, P = 0.006). Nighttime sleep deprivation independently compromised lipid-lowering efficacy (P < 0.001). No statistically significant differences in long-term clinical outcomes were observed among the three groups during the 36-month follow-up period (χ2 = 1.465, P = 0.481). The ABCB1 (2677T > G) polymorphism is significantly associated with interindividual variability in the lipid-lowering efficacy of atorvastatin among patients CIS. Specifically, CIS patients carrying the GG genotype demonstrate superior lipid-lowering responses to atorvastatin therapy compared to wild-type T allele carriers. However, this genetic variation does not appear to influence long-term prognostic outcomes in this patient population.
Similar content being viewed by others


Introduction
Stroke is the second leading cause of death globally and ranks as the primary cause of mortality and the third leading cause of disability in the Chinese population1. Cerebral ischemic stroke (CIS) accounts for 81.9% of all stroke cases, with a recurrence risk of approximately 5–10% within three months following the initial event2,3. Previous studies4,5,6 had demonstrated that elevated levels of low-density lipoprotein cholesterol (LDL-C) serve as an independent risk factor for both the pathogenesis and recurrence of CIS. Reduction of LDL-C levels can mitigate atherosclerosis progression, thereby decreasing the incidence, recurrence, disability, and mortality associated with CIS. Atorvastatin is widely utilized in clinical practice for lipid-lowering therapy in CIS patients. In the context of secondary prevention of CIS, statin therapy that reduces LDL-C by 1 mmol L−1 is associated with a 12% reduction in the risk of CIS recurrence7. However, not all patients derive equal benefit from this treatment, as significant interindividual variability in lipid-lowering efficacy exists. Genetic polymorphisms have been identified as a critical factor contributing to these variations in therapeutic response8.
The ABCB1 (2677T > G) polymorphism has emerged as one of the most frequently investigated genetic loci influencing statin therapeutic efficacy, though conflicting evidence exists across clinical studies. Investigations by Kadam et al.9 demonstrated that GG genotype carriers exhibited more pronounced LDL-C reduction following atorvastatin administration. However, contradictory findings from Jemaa et al.10 suggested no significant association between ABCB1(2677T > G) polymorphism and lipid-lowering outcomes. While clinical practitioners and patients predominantly focus on serum lipid profile alterations (particularly LDL-C and HDL-C levels) during therapeutic monitoring, emerging evidence suggests the LDL-C/HDL-C ratio demonstrates superior predictive value for atherosclerosis progression compared to isolated lipoprotein measurements11,12. Notably, the potential impact of ABCB1(2677T > G) polymorphism on lipid profile variations (including LDL-C, HDL-C, and their dynamic ratios) and long-term clinical outcomes in ischemic stroke patients remains underexplored.To address this knowledge gap, we systematically evaluated six lipid-related parameters: ΔHDL-C, ΔLDL-C, ΔHDL-C/HDL-C, ΔLDL-C/LDL-C, Δ(LDL-C/HDL-C) and Δ(LDL-C/HDL-C)/(LDL-C/HDL-C). This investigation aimed to elucidate the association between the ABCB1(2677T > G) gene polymorphism and the lipid-lowering efficacy of atorvastatin in patients with CIS under different models, and compared 3-year cerebrovascular event rates across genetic subgroups. Our analytical framework provided a novel biomarker-driven strategy for optimizing precision lipid management in CIS patients.
Materials and methods
Study design and participants
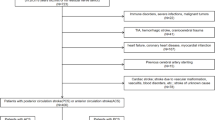
This prospective cohort study consecutively enrolled 152 Han Chinese CIS patients admitted to the Department of Neurology between January 2021 and December 2021. All participants met diagnostic criteria for CIS through clinical evaluation and neuroimaging confirmation (MRI and/or CT). During follow-up, 25 patients were excluded (14 due to protocol non-compliance, 8 withdrew consent, and 3 lost to follow-up), resulting in 127 analyzable cases. Participants were stratified into TT, GT, and GG groups based on ABCB1(2677T > G) genotyping. The study protocol was approved by the Ethics Committee of Xuchang Central Hospital (Approval No.2019-K-12-006), with written informed consent obtained from all participants or legal guardians.Inclusion criteria: (1) First-ever CIS meeting WHO diagnostic criteria; (2) Radiologically confirmed ischemic lesion; (3) Han Chinese ancestry in Henan Province; (4) Age ≥ 18 years; (5) Comorbid hyperlipidemia per 2016 Chinese Guidelines for Dyslipidemia Management13; (6) Stable residency (> 10 years) in the study region.Exclusion criteria: (1) Fatal stroke presentation; (2) Severe systemic comorbidities (cardiac/hepatic/renal failure, malignancies, autoimmune/hematologic disorders); (3) Prior use of statins or lipid-lowering agents within 30 days pre-admission; (4) Atorvastatin intolerance.
Experimental protocols
Genotyping and biochemical profiling
On the morning of the second day of hospitalization, approximately 2 mL of venous blood was collected from patients using EDTA anticoagulant tubes. DNA extraction was performed according to the manufacturer’s protocol of the commercial kit from Sino Era Genotech(China).
employed. Genetic testing for the ABCB1 (2677T > G) polymorphism was conducted using the TL-998 fluorescence detection system(Sino Era Genotech, China) with digital fluorescence molecular hybridization technology, a well-established detection method widely adopted in clinical laboratories across China.Serum lipid profiles (HDL-C, LDL-C) were quantified using commercially available enzymatic assay kits (Roche Diagnostics, Germany) on a cobas 8000 automated analyzer (Roche Diagnostics GmbH, Germany).
Therapeutic regimen and outcome measures
All patients received standardized care including anticoagulation, antiplatelet therapy, and neuroprotection. Lipid-lowering therapy comprised atorvastatin calcium tablets (Lipitor®, Pfizer; 20 mg once daily for two consecutive months). The primary outcome measure comprised longitudinal changes in six lipid profile parameters between baseline and post-treatment measurements at 2 months, including ΔHDL-C, ΔLDL-C, ΔHDL-C/HDL-C, ΔLDL-C/LDL-C, Δ(LDL-C/HDL-C), and Δ(LDL-C/HDL-C)/(LDL-C/HDL-C), with the calculation methods shown in Table 1. The secondary outcome measure comprised the cumulative incidence of cerebrovascular events, including radiologically-confirmed ischemic stroke recurrence and transient ischemic attacks (TIAs), which was meticulously assessed through either telephone or outpatient follow-up within 36 months subsequent to the patients’ discharge from the hospital. Therapeutic efficacy was defined as achieving LDL-C < 1.8 mmol L−12. Baseline demographics (age, sex, BMI), clinical parameters (blood pressure, glucose), and adverse health behaviors (tobacco use history, alcohol consumption patterns, nighttime sleep deprivation) were extracted from the Hospital Information System (HIS).
Statistical analysis
All analyses were conducted using SPSS 25.0 (IBM Corp., Armonk, NY). The continuous variables conforming to normal distribution are presented as mean ± standard deviation, and one-way ANOVA was used for comparisons among three groups, with post-hoc testing conducted via the Bonferroni multiple comparison procedure. Non-normally distributed continuous variables are expressed as median (interquartile range), and the Kruskal-Wallis H test was applied. The Hardy-Weinberg equilibrium, categorical data, and prognostic differences between two groups were analyzed using the chi-square test. Analysis of covariance (ANCOVA) was performed to explore the differences in lipid-lowering efficacy of atorvastatin among different groups. Binary logistic regression analysis was employed to assess the association between ABCB1 (2677T > G) and the lipid-lowering efficacy of atorvastatin in CIS patients under additive, recessive, and dominant genetic models. A P-value < 0.05 was considered statistically significant.
Results
Demographic characteristics across genotype groups
The study population comprised 127 analyzable cases stratified by ABCB1(2677T > G) genotypes: GG (n = 48), GT (n = 49), and TT (n = 30). Baseline characteristics revealed comparable demographic profiles across groups (Table 2). The GG cohort included 27 males (56.3%) with mean age 63.17 ± 11.04 years and BMI 24.65 ± 2.99 kg/m2. The GT group contained 32 males (65.3%) aged 61.22 ± 13.53 years (BMI 24.46 ± 3.02 kg/m2), while the TT group consisted of 20 males (66.7%) with mean age 68.73 ± 12.02 years (BMI 23.73 ± 2.88 kg/m2). Intergroup comparisons demonstrated no statistically significant differences in sex distribution, BMI, or other baseline parameters (all P > 0.05), except for age variation (P = 0.031 by ANOVA).
Hardy-Weinberg equilibrium analysis of ABCB1(2677T > G) genotypes
Genetic distribution analysis revealed the following genotype frequencies among 127 participants: GG (homozygous variant, 48 cases, 37.80%), GT (heterozygous variant, 49 cases, 38.58%), and TT (wild-type, 30 cases, 23.62%). Allelic frequencies were 57.09% for G and 42.91% for T. Chi-square test demonstrated concordance between observed and expected genotype frequencies (χ2 = 3.225, P = 0.199), confirming adherence to Hardy-Weinberg equilibrium (HWE). This genetic equilibrium validates the sample population as a representative Mendelian cohort without significant selection bias (Table 3).
ANCOVA analysis of atorvastatin therapeutic efficacy across genotype groups
In both the additive and recessive models with age as a covariate, ABCB1(2677T > G) gene polymorphism significantly affected ΔLDL-C, ΔLDL-C/LDL-C, Δ(LDL-C/HDL-C), and Δ(LDL-C/HDL-C)/(LDL-C/HDL-C). In the additive model: FΔLDL−C = 4.198, P = 0.001; FΔLDL−C/LDL−C = 3.042, P = 0.013; FΔ(LDL−C/HDL−C) = 3.870, P = 0.003; FΔ(LDL−C/HDL−C)/(LDL−C/HDL−C) = 2.551, P = 0.031. In the recessive model: FΔLDL−C = 5.142, P = 0.002; FΔLDL−C/LDL−C = 3.539, P = 0.017; FΔ(LDL−C/HDL−C) = 5.938, P = 0.001; FΔ(LDL−C/HDL−C)/(LDL−C/HDL−C) = 4.312, P = 0.006. In the dominant model with age as a covariate, ABCB1(2677T > G) gene polymorphism significantly affected Δ(LDL-C/HDL-C) (F = 3.571, P = 0.016), but had no significant effect on ΔLDL-C, ΔLDL-C/LDL-C, or Δ(LDL-C/HDL-C)/(LDL-C/HDL-C) (all P > 0.05) (Table 4). Comparative analysis across genetic models consistently indicated superior lipid-lowering efficacy in GG homozygous carriers.
Univariate analysis of factors influencing atorvastatin treatment efficacy
Patients were stratified into responders (serum LDL-C level < 1.8 mmol L−1) and non-responders based on therapeutic efficacy criteria. Univariate analysis revealed significant differences (P < 0.1) between the two groups in nighttime sleep deprivation, and genetic inheritance models (additive and recessive models). These findings suggested potential confounding effects of lifestyle factors and genetic polymorphisms on lipid-lowering outcomes (Table 5).
Binary logistic regression analysis of factors influencing atorvastatin therapeutic efficacy
Using lipid-lowering efficacy (responder vs. non-responder) as the dependent variable, covariates with P < 0.1 from the univariate analysis including nighttime sleep deprivation, and genetic models (additive and recessive models for ABCB1(2677T > G) were incorporated into separate binary logistic regression analyses. The analysis identified nighttime sleep deprivation and ABCB1 (2677T > G) genotype as significant predictors of atorvastatin efficacy. After adjusting for nighttime sleep deprivation, the association between ABCB1 genotype and therapeutic response remained statistically robust. In the additive model, patients with the GG genotype exhibited a 3.181-fold higher likelihood of achieving lipid-lowering targets compared to wild-type TT carriers (OR = 3.181, 95%CI:1.159 ~ 8.730, P = 0.025). Similarly, in the recessive model, GG genotype patients demonstrated a 3.141-fold increased efficacy relative to T-allele carriers (OR = 3.141, 95%CI:1.397 ~ 7.061, P = 0.006). Nighttime sleep deprivation independently predicted reduced treatment efficacy across both genetic models, with comparable effect magnitudes in the additive (OR = 0.237, 95%CI:0.108 ~ 0.522, P < 0.001) and recessive models (OR = 0.238, 95%CI:0.108 ~ 0.522, P < 0.001) (Table 6).
Long-term outcomes assessment based on cerebral infarction recurrence
Cerebral infarction recurrence was evaluated as the primary endpoint to assess long-term therapeutic efficacy. Over a 36-month follow-up period, no statistically significant differences in the cumulative incidence of cerebrovascular events were observed among patients stratified by ABCB1 G2677T genotypes(χ2 = 1.465, P = 0.481) (Table 7).
Discussion
This study investigated the association between ABCB1 (2677T > G) genetic polymorphism and lipid-lowering efficacy of atorvastatin in cerebral ischemic stroke (CIS). Our findings demonstrate superior therapeutic responses in GG genotype carriers compared to wild-type T allele carriers under both additive and recessive genetic models. It should be noted that the consistency of these results across distinct inheritance patterns strengthens the pharmacogenetic relevance of ABCB1 2677T > G in statin metabolism. Our findings carry direct implications for precision medicine approaches in stroke secondary prevention. Incorporating ABCB1 genotyping into clinical decision-making may enable stratified therapeutic strategies, particularly for patients exhibiting inadequate statin responses. Based on our findings, we propose the following clinical recommendations: For patients with the ABCB1 (2677T > G) GG genotype, standard-dose atorvastatin is recommended, along with regular lipid profile monitoring. For those with TT/GT genotypes (particularly TT), strategies such as dose escalation, combination therapy with ezetimibe, therapeutic drug monitoring of plasma concentrations, or switching to rosuvastatin are suggested to optimize lipid control.
Lipid-lowering therapy, endorsed by international guidelines as a cornerstone of secondary prevention in cerebral infarction survivors (CIS)14, mitigates atherosclerotic progression through LDL-C reduction, thereby improving long-term clinical outcomes. Atorvastatin, widely utilized in CIS management due to its favorable efficacy-safety profile15, demonstrates dose-dependent protective effects. Amarenco et al.16 reported a 16% reduction in stroke recurrence risk (median follow-up: 4.9 years) with high-dose atorvastatin (80 mg nightly). However, substantial interindividual variability in therapeutic response persists, with a proportion of patients exhibiting suboptimal lipid control17, underscoring the need to elucidate mechanisms underlying statin resistance.Our study identifies ABCB1 (2677T > G) polymorphism as a novel pharmacogenetic determinant of atorvastatin efficacy.
In this study, we assessed the magnitude of LDL-C reduction (ΔLDL-C/LDL-C) across the three genotype groups before and after treatment. Notably, the GG group exhibited a significantly greater LDL-C reduction rate compared to the GT and TT groups (Table 4).To further evaluate the absolute therapeutic efficacy, we defined treatment success as achieving an LDL-C level below 1.8 mmol/L. Strikingly, the proportion of responders was significantly higher in the GG group than in the GT and TT groups (Table 5). To the best of our knowledge, this was the first study to integrate both relative LDL-C reduction and absolute treatment success rate in assessing the impact of ABCB1 G2677T polymorphism on statin response. This dual-metric approach provided a more comprehensive evaluation of genotype-dependent lipid-lowering effects across patients with varying baseline LDL-C levels, thereby better reflecting real-world clinical outcomes.Our findings demonstrate a significant association between ABCB1 (2677T > G) polymorphism and the magnitude of LDL-C reduction in CIS receiving atorvastatin therapy, with GG allele carriers exhibiting enhanced therapeutic sensitivity. This genotype-dependent efficacy variation may stem from two interrelated pharmacokinetic mechanisms: (1) P-glycoprotein-Mediated Drug Disposition: The ABCB1-encoded P-glycoprotein functions as a critical efflux transporter, displaying interindividual expression variations associated with the ABCB1 2677T > G polymorphism. GG genotype carriers exhibit enhanced P-glycoprotein activity, which reduces first-pass hepatic clearance through elevated transporter functionality. This mechanistic cascade increases systemic drug exposure, evidenced by elevated area under the curve (AUC) values and prolonged elimination half-life. This had been confirmed in the study by Qu et al.18 (2) Structural Determinants of Transporter Affinity: The T → G substitution at position 2677 induces a serine-to-alanine amino acid transition (hydrophilic → hydrophobic) in transmembrane domain 11 of P-glycoprotein. This structural modification reduces transporter affinity for atorvastatin’s open-ring conformation, impeding its efflux from hepatocytes and intestinal epithelia. Consequently, GG genotype carriers retain higher intracellular drug concentrations, potentiating HMG-CoA reductase inhibition and LDL-C catabolism19,20.These mechanistic insights align with our clinical observations of genotype-stratified responses. The dual pharmacokinetic advantages prolonged circulation time and enhanced cellular retention collectively explain the superior efficacy in GG carriers. These findings underscore the importance of ABCB1 pharmacogenetics in optimizing statin therapy, particularly for CIS patients with suboptimal lipid control.
Previous studies had established that genetic polymorphisms in SLCO1B1 521T > C (rs4149056)21, ABCB1 C1236T (rs1128503), ABCB1 C3435T (rs1045642)9,19, UGT1A3(rs3821242), and CYP3A4 (rs55785340, rs35599367)22 influenced atorvastatin plasma concentrations, thereby modulating both drug efficacy and adverse effects.Specifically, Bosco et al.21 demonstrated that the SLCO1B1 521T > C (rs4149056) variant increased systemic statin exposure, contributing to a higher risk of adverse drug reactions. Kadam et al.9 showed in a study on Indian populations that patients with ABCB1 C3435T mutation genotypes had better lipid-lowering efficacy with atorvastatin than wild-type patients. A study by Wang et al.17 on the Chinese Uyghur population demonstrated that coronary heart disease patients with the ABCB1 C3435T TT genotype showed more significant triglyceride (TG) reduction after atorvastatin treatment. However, a study by Qu et al.18 on hyperlipidemic patients in southeastern China showed that the ABCB1 C3435T gene polymorphism was not associated with the lipid-lowering efficacy of atorvastatin.Nevertheless, due to limitations in detection conditions, this study did not examine the impact of the above-mentioned genetic loci on lipid-lowering therapy with atorvastatin in cerebral infarction patients. This represents a limitation of our research, which warrants further investigation in future studies.Our genetic models revealed substantial efficacy differences in atorvastatin response stratified by ABCB1 (2677T > G) genotypes. In the additive model, GG homozygotes demonstrated a 3.181-fold increased probability of achieving lipid targets compared to wild-type TT carriers. Similarly, under the recessive model, GG genotype patients exhibited a 3.141-fold higher therapeutic efficacy relative to T-allele carriers. These findings align with Jiang et al.23, who reported a 3% greater LDL-C reduction in GG versus TT genotype patients, .However, contradictory evidence exists. Prado et al.24 observed no ABCB1-statin association in Chilean populations, while a meta-analysis of 3, 088 participants across 10 studies25 found no global pharmacogenetic correlation. We hypothesize that ethnic-specific allele frequency variations may underlie these discrepancies. Supporting this, Wang et al.26 demonstrated divergent ABCB1 (2677T > G) genotype distributions between Han and Uyghur ethnic groups in China.Notably, our lipid profile analyses revealed genotype-dependent bidirectional effects: LDL-C reductions and HDL-C elevations were significantly amplified in GG carriers across both genetic models. This dual lipid-modifying advantage suggests preferential atorvastatin utilization for cerebral infarction survivors (CIS) harboring the GG genotype. Importantly, these findings underscore the necessity for clinicians to consider pharmacogenomic profiles when implementing statin-based secondary prevention strategies, extending beyond conventional lipid monitoring.
The dominant model analysis in this study revealed no significant differences in lipid-lowering efficacy across covariates or regression models, with the exception of Δ(LDL-C/HDL-C). Three potential mechanisms could underlie this observation: First, the relatively small cohort size inherently restricted statistical power for identifying subtle genotype-phenotype associations. Second, our exclusive focus on ABCB1 (2677T > G) polymorphism overlooks the pharmacokinetic complexity of atorvastatin metabolism, which likely involves polygenic interactions across multiple transporters and metabolic enzymes27,28. Additionally, prior pharmacogenomic investigations have implicated other ABCB1 variants (e.g., C3435T) in statin response heterogeneity29. Furthermore, the observed 2677T > G effects may reflect linkage disequilibrium with functional SNPs in regulatory regions rather than direct causality. Haplotype analyses demonstrate that ABCB1 polymorphisms frequently co-segregate, with the 2677T > G locus potentially serving as a proxy marker for clinically relevant variants affecting P-glycoprotein expression18.
Interestingly, our findings revealed that the efficacy rate of lipid-lowering therapy in CIS patients with nighttime sleep deprivation was approximately 24% of that observed in patients maintaining regular sleep patterns. This discovery highlights two critical implications. First, it underscores the clinical importance of prioritizing healthy sleep hygiene when administering atorvastatin-based lipid management to ischemic stroke patients. Second, the results suggest that the ABCB1 (2677T > G) gene polymorphism does not singularly account for the observed variability in therapeutic outcomes among CIS patients. Instead, modifiable lifestyle factors—including environmental influences, dietary habits, and physical activity levels—may synergistically modulate lipid metabolism and treatment responsiveness30.
In this study, no statistically significant differences in clinical outcomes were observed among the three patient groups, suggesting that the ABCB1 (2677T > G) polymorphism may not serve as an independent prognostic predictor for cerebral infarction patients. A plausible explanation lied in the multifactorial nature of stroke recurrence, which involves a complex interplay of platelet hyperreactivity following antiplatelet therapy31, adverse lifestyle habits32, hypertension33, diabetes mellitus34, and other contributing factors.To the best of our knowledge, this study was the first systematic investigation of the association between ABCB1 (2677T > G) (rs2032582) polymorphism and long-term stroke outcomes. Although the results were negative, our findings aligned with the previously reported observations by Liang et al.35 regarding the ABCB1 rs1045642 genetic variant.
This study demonstrated that the lipid-lowering efficacy of atorvastatin in CIS patients was significantly influenced by the ABCB1 (2677T > G) gene polymorphism, providing critical evidence for precision statin therapy in this population. However, several limitations warranted consideration. First, the single-center design with a limited sample size could introduce selection bias. Second, this study was conducted in a Han Chinese population from central China. Due to ethnic variations, the findings may not be generalizable to other racial or ethnic groups. Third, this study only monitored the lipid profile changes for two months in the enrolled patients. Fourth, this study did not experimentally validate the impact of ABCB1 (2677T > G) gene polymorphism on atorvastatin drug concentration, which warrants further investigation in our future research.Therefore, the results may not fully represent the long-term outcomes of lipid-lowering therapy. In light of the above, these conclusions warrant further validation through rigorously designed multicenter studies that should incorporate larger sample sizes, cohorts with broader ethnic representation, extended observation periods, and deeper investigations into the mechanistic impacts of genetic polymorphisms on drug actions.
Data availability
All the data are included in the article. For further inquiries, please contact the corresponding author.
References
GBD Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 20(10), 795–820 (2021).
Chinese Society of Neurology, Chinese Stroke Society. Chinese guideline for the secondary prevention of ischemic stroke and transient ischemic attack 2022. Chin. J. Neurol. 55(10), 1071–1110 (2022).
Wang, Y. et al. CHANCE-2 investigators. Ticagrelor versus clopidogrel in CYP2C19 Loss-of-Function carriers with stroke or TIA. N. Engl. J. Med. 385(27), 2520–2530 (2021).
Giugliano, R. P. et al. Long-term safety and efficacy of achieving very low levels of low-density lipoprotein cholesterol: A prespecified analysis of the IMPROVE-IT trial. JAMA Cardiol. 2(5), 547–555 (2017).
Balling, M. et al. Small dense Low-Density lipoprotein cholesterol and ischemic Stroke. Ann. Neurol. 93(5), 952–964 (2023).
Fan, J. et al. Global burden, risk factor analysis, and prediction study of ischemic stroke, 1990–2030. Neurology 101(2), e137–e150 (2023).
Kleindorfer, D. O. et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline from the American heart association/american stroke association. Stroke 52(7), e483–e484 (2021).
Maslub, M. G. et al. Association between CYP3A4/CYP3A5 genetic polymorphisms and treatment outcomes of Atorvastatin worldwide: Is there enough research on the Egyptian population?. Eur. J. Med. Res. 28(1), 381 (2023).
Kadam, P. et al. Genetic determinants of lipid-lowering response to Atorvastatin therapy in an Indian population. J. Clin. Pharm. Ther. 41, 329–333 (2016).
Jemaa, R. et al. Lack of association between theABCB1 G2677T polymorphism and the lipid-lowering effects of Atorvastatin in Tunisian patients. Arch. Cardiovas Dis. 10(1), 117 (2018).
Yue, Y. H. et al. Gene polymorphisms affect the effectiveness of Atorvastatin in treating ischemic stroke patients. Cell. Physiol. Biochem. 39, 630–638 (2016).
Peng, C. et al. Polymorphisms in CYP450 genes and the therapeutic effect of Atorvastatin on ischemic stroke: A retrospective cohort study in Chinese population. Clin. Ther. 40(3), 469–477 (2018).
Joint Committee Issued Chinese Guideline for the Management of Dyslipidemia in Adults. 2016 Chinese guideline for the management of dyslipidemia in adults. Chin. J. Health Manag. 11(1), 7–28 (2017).
Xu, J. et al. Effect of Lipoprotein(a) on stroke recurrence attenuates at low LDL-C (Low-Density Lipoprotein) and inflammation Levels. Stroke 53(8), 2504–2511 (2022).
Tramacere, I. et al. Comparison of Statins for secondary prevention in patients with ischemic stroke or transient ischemic attack: A systematic review and network meta-analysis. BMC Med. 17(1), 67 (2019).
Amarenco, P. et al. High-dose Atorvastatin after stroke or transient ischemic attack. N. Engl. J. Med. 378(25), 2450 (2018).
Wang, T. et al. The ABCB1 C3435T polymorphism is associated with triglyceride reduction in Atorvastatin-treated Uygur patients with coronary heart disease and dyslipidemia: An observational study. Endocr. Metab. Immune Disord. Drug Targets 23(9), 1215–1228 (2023).
Qu, K. K. et al. Association of ABCB1 polymorphisms with lipid homeostasis and liver injury response to Atorvastatin in the Chinese population. Can. J. Physiol. Pharmacol. 98(1), 15–22 (2020).
Keskitalo, J. E. et al. ABCB1 haplotypes differentially affect the pharmacokinetics of the acid and lactone forms of Simvastatin and Atorvastatin. Clin. Pharmacol. Ther. 84(4), 457–461 (2008).
Huang, L. et al. Significance and mechanisms of P-glycoprotein in central nervous system diseases. Curr. Drug Targets 20(11), 1141–1155 (2019).
Bosco, G. et al. The impact of SLCO1B1 rs4149056 on LDL-C target achievement after lipid Lowering therapy optimization in men and women with Familial hypercholesterolemia. Front. Endocrinol. 15, 1346152 (2024).
Mykkänen, A. J. H. et al. Genome-Wide association study of Atorvastatin pharmacokinetics: Associations with SLCO1B1, UGT1A3, and LPP. Clin. Pharmacol. Ther. 115(6), 1428–1440 (2024).
Jiang, Z. et al. Effect of polymorphisms in drug metabolism and transportation on plasma concentration of Atorvastatin and its metabolites in patients with chronic kidney disease. Front. Pharmacol. 14, 1102810 (2023).
Prado, Y., Zambrano, T. & Salazar, L. A. Transporter genes ABCG2 rs2231142 and ABCB1 rs1128503 polymorphisms and Atorvastatin response in Chilean subjects. J. Clin. Pharm. Ther. 43(1), 87–91 (2018).
Yao, C., Xing, H. & Xu, J. The role of ABCB1 G2677T/A polymorphisms in serum lipid levels and lipid-lowering response to statin treatment: A meta-analysis. Anhui Med. Pharm. J. 24(3), 551–556 .
Xu, T. W. L. et al. Research of ABCB1 C3435T and ABCB1 T2677G gene polymorphism in patients with dyslipidemia of Xinjiang. Acta Univ. Med. Anhui 56(3), 454–457 (2021).
Zhang, L. et al. Association of SLCO1B1 and ABCB1 genetic variants with Atorvastatin-induced myopathy in patients with acute ischemic stroke. Curr. Pharm. Des. 25(14), 1663–1670 (2019).
Bharath, G. et al. SLCO1B1 and ABCB1 variants synergistically influence the Atorvastatin treatment response in South Indian coronary artery disease patients. Pharmacogenomics 23(12), 683–694 (2022).
Karaźniewicz-Łada, M. et al. Impact of genetic variants of selected cytochrome P450 isoenzymes on pharmacokinetics and pharmacodynamics of clopidogrel in patients co-treated with Atorvastatin or rosuvastatin. Eur. J. Clin. Pharmacol. 76(3), 419–430 (2020).
Hsu, H. Y. et al. Efficacy of more intensive lipid-lowering therapy on cardiovascular diseases: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 20(1), 334 (2020).
Mao, Y. et al. Impact of platelet hyperreactivity and diabetes mellitus on ischemic stroke recurrence: A single-center cohort clinical study. Int. J. Gen. Med. 17, 1127–1138 (2024).
Cao, Y. et al. Analysis of prognostic risk factors for ischemic stroke in china: A multicentre retrospective clinical study; A National survey in China. Curr. Neurovasc. Res. 19(1), 117–126 (2022).
Tu, W. J. & Wang, L. D. China stroke surveillance report 2021. Mil. Med. Res. 10(1), 33 (2023).
Kolmos, M., Christoffersen, L. & Kruuse, C. Recurrent ischemic stroke—A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 30(8), 105935 (2021).
Liang, C. et al. Correlation between ABCB1 and OLIG2 polymorphisms and the severity and prognosis of patients with cerebral infarction. Open Med. 19(1), 20230841 (2024).
Acknowledgements
We would like to extend our heartfelt gratitude to each and every participant for their tireless efforts that were instrumental in bringing this project to its successful completion.
Funding
This work was supported by Henan Province Science and Technology Research and Development Program Project (grant no. 232102311112).
Author information
Authors and Affiliations
Contributions
Y.T.: Research design, funding acquisition, writing-original draft. B.X.: data analysis and interpretation. S.G. and W.L.: Research design. Q.L., H.Z. and P.G.: Patient enrollment, informed consent, and dosing protocol design, clinical Follow-up. Y.Z.: ABCB1(2677T> G) genetic testing. W.L. and H.W.: Research data collection, methodology. X.Z.: Conception and design, writing (review and editing), supervision.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by Ethics Committee of the xuchang central hospital (No.2019-K-12-006). All aspects of the study complied with the Declaration of Helsinki.
Consent to participate
Written informed consent was secured from all participants or their legal guardians.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tian, Y., Xu, B., Guo, S. et al. Association of ABCB1 G2677T polymorphism with atorvastatin lipid efficacy and extended prognosis in patients with cerebral ischemic stroke. Sci Rep 15, 30132 (2025). https://doi.org/10.1038/s41598-025-15434-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-15434-6
