
Abstract
The Thoracic Training Course of the Royal College of Surgeons of Edinburgh in China is dedicated to training skilled thoracic surgeons to an elite level. Almost all the learners at the Nanjing training station showed great interest in a novel stapler tractor designed for dissociating segmental vessels during lung segmentectomy. This study aimed to unveil the beneficial of the novel stapler tractor. Three hundred twenty-three patients who underwent lung segmentectomy at the Nanjing training station were retrospectively analyzed. First, surgical outcomes were compared between those who used a stapler tractor for dissociating segmental vessels and those who did not. Secondly, the results of dissociating segmental vessels were compared between the group that used the stapler tractor and the other three techniques. Lastly, the same variable comparisons were made among the learners. Compared with the outcomes of the non-used stapler tractor patient group during the teaching period, the patients in the used stapler tractor group had shorter operation times (143.15 ± 28.05 min vs. 152.83 ± 37.92 min, P = 0.019), less intraoperative bleeding (51.41 ± 42.60 mL vs. 70.70 ± 63.19 mL, P = 0.017), shorter postoperative hospital stays (3.39 ± 0.81 days vs. 3.70 ± 1.07 days, P = 0.008), and a lower incidence of postoperative pulmonary embolism (0.3% vs. 4.2%, P = 0.035). Compared with the results of other techniques for dissociating segmental vessels, the stapler tractor group had a lower occurrence of intraoperative bleeding (P = 0.002), a reduced time for dissociating the vessel (P < 0.05), a greater successful traction ratio (P = 0.022), and a shorter vascular stump length (P = 0.000). The learners reproduced similar outcomes and results in 58 patients across different affiliations. The benefits of using stapler techniques for dissociating vascular structures in lung segmentectomy include, but are not limited to, shortened operation time, reduced intraoperative blood loss, shorter postoperative hospital stays, reduced postoperative air leakage rates, and a lower incidence of postoperative pulmonary embolism, whether during the teaching or learning period.
Similar content being viewed by others


Introduction
Due to the shortage of medical resources, past operations have mainly emphasized whether surgeons could carry them out successfully1. With the application of new surgical instruments and technical training in surgery, the field is pursuing precision and minimally invasive techniques2,3,4. Especially, the intensive specialized technical training of the Royal College of Surgeons of Edinburgh has been widely carried out at the Nanjing training station. The Nanjing training station is one of the earliest centers for precision thoracic surgery training established by the Royal College of Surgeons of Edinburgh. As one of the first institutions to perform precision resections of lung segments, we have trained at least 50 institutions around the world to carry out precision resections of lung segments5,6,7.
In this training, the most discussed topic is the dissociation of vascular structures in lung segmentectomy8. Improper dissection of vessels is one of the most important factors leading to intraoperative and postoperative complications during lung segmentectomy. In many surgical institutions, silk traction, staplers without assistance, and silk ligation are used by surgeons for vascular dissociation in lung segmentectomy.
In order to reduce the occurrence of adverse events during vascular dissociation in lung segmentectomy, we designed a novel tool, the stapler tractor (Fig. 1), more than ten years ago. We have since gained extensive clinical experience with the stapler tractor for dissociating segmental vessels (Fig. 2). The use of a stapler tractor in lung segmentectomy has emerged as a promising technique, particularly when combined with the tunneling method. This innovative approach addresses some of the challenges traditionally associated with lung segment resections, such as the difficulty in maneuvering staples through anatomical obstacles. The stapler tractor, a self-designed tool, facilitates the precise resection of lung segments by enhancing the surgeon’s ability to navigate complex anatomical structures9. However, the learners had not used it prior to entering this course of study at their institutions. Consequently, they have some doubts about this novel tool, which they perceive as adding complexity to the surgical process and potentially challenging surgical outcomes. In this context, we designed a parametric comparison study focusing on specific skill details related to the stapler tractor for dissociating segmental vessels during lung segmentectomy, akin to the analysis of competitive ball game videos.

Picture of the novel stapler tractor. Appearance and dimensions of the tractor (A); Hand drawing depict the method of the tractor of wearing on the stapler (B); Picture of the stapler worn the tractor(C). Jian Zhu drew this hand- drawing picture (B), Email: zhujian0718@163.com.

Hand drawing of using the novel stapler tractor during the operation. pull-on tractor the guide end passes through the target vessels (A); the surgeon pushes the stapler, and passes the target vessel with the assistant dragging and guiding by the tractor (B); the tractor is removed, and the stapler is cut and sutured to the target vessels (C). Jian Zhu drew these hand- drawing pictures, Email: zhujian0718@163.com.
Methods
Participants
The participants of this study are divided into two periods: the teaching period and the learning period. In the teaching period, patients who underwent precision resection of lung segments by instructors at the Nanjing training station between October 8, 2019, and May 19, 2023, were retrospectively analyzed. In the learning period, patients who underwent lung segmentectomy by learners at three institutions between June 7, 2021, and December 8, 2023, were retrospectively analyzed. These two periods represent the groupings of the study, and we compared surgical outcomes and procedural results independently.
Firstly, surgical outcomes were compared between the use and non-use of the stapler tractor for dissociating segmental vessels. Secondly, the specific role of surgical details was included in this study. These details were divided into four groups according to different techniques for treating segmental vascular issues during the teaching and learning periods: by stapler tractor (Group A, Fig. 3), by stapler with silk (Group B, Fig. 3), by stapler without assistance (Group C, Fig. 4), and by silk ligation (Group D, Fig. 4). Finally, we observed whether similar results from the learning period could be achieved during the teaching period.

Real scenes and effects of segmental vessel dissection via the stapler tractor, before dissection (A); during dissection(B); after dissection measuring vessel stump(C). Real scenes and effects of segmental vessel dissection via the stapler with silk, before dissection (D); during dissection(E); after dissection measuring vessel stump(F).

Real scenes and effects of segmental vessel dissection via the stapler without assisted, before dissection (A); during dissection(B); after dissection measuring vessel stump(C). Real scenes and effects of segmental vessel dissection via the silk ligation, before dissection (D); during dissection(E); after dissection measuring vessel stump(F).
Lung segmentectomy, as defined by the teacher, involves (1) having a safe surgical margin distance that is greater than the maximum diameter of the tumor or at least 2 cm; (2) dividing and severing the arterial, bronchial, and main venous structures (all three are indispensable); and (3) using the unit for lung subsegments to reduce the number of resected subsegments as much as possible. Lung segmentectomy by a learner was defined as (1) having a safe surgical margin distance that is greater than the maximum diameter of the tumor or 2 cm; and (2) dividing and severing the arterial, bronchial, or main venous structures.
Inclusion criteria: (1) The operation of lung segmentectomy was performed. (2) The collected data must include intact surgical videos. (3) The method of approach was multi-port.
Exclusion criteria: (1) dealing with unplanned events for more than 30 min during the operation; (2) having two or more lesions that need to be treated in different anatomical fields; (3) cases with incomplete data, such as a lack of key surgical details; (4) cases converted to lobectomy during the operation.
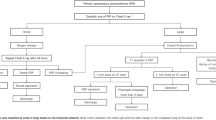
The detailed experimental design and data grouping comparison are shown in Fig. 5.

Flowchart of patients on teaching period and learning period.
Procedures
The stapler tractor comprises a flat tube with a cavity (approximately 5–10 cm), a round tube (approximately 30–50 cm) with a diameter smaller than the width of the flat tube, and a shifter for connecting the flat tube and the round tube; the hollow part of the flat tube is aligned with the anvil of the stapler (Fig. 1). During operation, the anvil of the stapler is firmly inserted into the cavity of the flat tube, and the round tube is gently pulled. At the same time, the stapler is moved toward the target vessel, allowing the round tube, shifter, flat tube, and anvil to pass successively through the safe passage. The stapler is then stabilized, the flat tube is removed, the anvil is exposed, and the stapler tractor is withdrawn from the incisions (Fig. 2, Supplemental Video 1).
All surgical videos were recorded using XIRecorder software. All the vessels were either segmental or subsegmental vessels. Because the height of the footplate of the high-frequency electrocoagulation hook is equal to half the width of the stapler, we measured the length of the vascular stump based on whether it exceeds the height of the footplate of the high-frequency electrocoagulation hook (Supplemental 1a), treating this as count data.
Procedure of the four techniques for vascular dissection
To evaluate the advantages of procedural outcomes using the stapler tractor, four techniques were assessed based on all techniques employed for segmental vessel dissection during the teaching period. The techniques were defined as follows: dissociating segmental vessels using the stapler tractor was classified as Group A, using a stapler with silk was classified as Group B, using a stapler without assistance was classified as Group C, and using silk ligation was classified as Group D.
Statistical analysis
The continuous data are presented as the mean ± standard deviation for continuous variables and as absolute numbers and percentages for categorical variables. Categorical variables were assessed using χ2 tests or Fisher’s exact tests as appropriate, and t-test or one-way ANOVA was used to compare the mean values of continuous variables. The non-normally distributed data were compared between groups using the Mann-Whitney U test. A p-value ≤ 0.05 indicated statistical significance. All statistical analyses were performed using SPSS version 26.0 software.
Ethics approval
This study was approved by the institutional review board (IRB) of the First Affiliated Hospital of Nanjing Medical University (No. 2021-SR-164); the IRB of Nanjing Pukou People’s Hospital (No. 2023-NT-011); the IRB of Taizhou Hospital of Traditional Chinese Medicine (No. 2023-010-03). Data from the surgical options cohort do not involve any personally identifiable information. All methods were carried out in accordance with relevant guidelines and regulations. Written informed consent was waived by the IRB of the First Affiliated Hospital of Nanjing Medical University (No. 2021-SR-164), the IRB of Nanjing Pukou People’s Hospital (No. 2023-NT-011), the IRB of Taizhou Hospital of Traditional Chinese Medicine (No. 2023-010-03) due to retrospective nature of study and was obtained from all participants.
Transparency statement
The manuscripts guarantors (all authors) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and any discrepancies from the study as planned have been explained. This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited.
Results
Patient characteristics
During the teaching period, this study included 323 patients; 185 (57.3%) were female, and 79 (24.5%) were smokers. These patients were divided into two groups: vascular dissection without a stapler tractor (non-used group, n = 71) and vascular dissection with a stapler tractor (used group, n = 252). The baseline characteristics are shown in Table 1. There was no significant difference between the two groups. The mean age of the patients was 57.39 ± 11.78 years. The mean tumor size was 1.45 ± 0.61 cm. Preoperative comorbidities included heart disease (22.0%), COPD (22.0%), diabetes (13.6%), hypertension (25.1%), and cerebrovascular disease (13.3%). In total, 11 types of segmentectomy were performed. Similar characteristics were observed during the learning period (Table 1).
Surgical outcomes between the non-used group and used group
To evaluate the advantages of surgical outcomes using the stapler tractor, we collected and analyzed the surgical outcome data of the patients during the teaching period. The operation time was significantly shorter in the used group than in the non-used group (143.15 ± 28.05 min vs. 152.83 ± 37.92 min, P = 0.019). Intraoperative bleeding in the used group was significantly lower than that in the non-used group (51.41 ± 42.60 mL vs. 70.70 ± 63.19 mL, P = 0.017). The postoperative hospital stay was significantly decreased in the used group (3.39 ± 0.81 days vs. 3.70 ± 1.07 days, P = 0.008). The duration of chest tube placement in the used group was shorter than that in the non-used group (2.48 ± 0.75 days vs. 2.77 ± 0.91 days, P = 0.005). No significant difference in postoperative drainage volume was observed between the two groups. The occurrence of air leakage was lower in the used group compared to the non-used group (17.1% vs. 28.2%, P = 0.037), as was the incidence of postoperative pulmonary embolism (0.3% vs. 4.2%, P = 0.035). Then, these surgical outcomes were compared between used and non-used the stapler tractor for dissociating segmental vessels by learners, which reproduced the similar outcome (Table 2).
Procedure results of the four techniques for vascular dissection
The sample sizes for each group are as follows, Group A (n = 263), Group B (n = 52), Group C (n = 95), and Group D (n = 169). The occurrence of intraoperative bleeding in Group A was lower than that in Groups B, C, and D (P = 0.002). Additionally, the successful traction ratio in Group A was significantly greater than that in Group B and C (P = 0.022, Fig. 6). Compared to Group B/C/D, the time taken to dissociate the segmental vessel in Group A was shorter (314.33 ± 98.02 s vs. 356.48 ± 106.60 s, P = 0.006; 314.33 ± 98.02 s vs. 346.72 ± 90.40 s, P = 0.007; 314.33 ± 98.02 s vs. 344.75 ± 108.01 s, P = 0.002). In addition, 57 vessels were successfully converted to staple tractors using the other three techniques. At least two vessels were dissected simultaneously with one stapler, resulting in a total of 81 vessels (Supplemental 1b). However, the vascular stump length in Group A was markedly shorter than that in Groups B, C, and D (P = 0.000). The results of these procedures were then compared among the four techniques for dissociating segmental vessels by learners, which produced similar outcomes (Table 3).

Procedure results about time of dissociating the segmental vessel by four techniques.
Discussion
With the popularization of computed tomography, an increasing number of early NSCLCs have been detected10,11. The main treatment for early NSCLC is surgery12,13, and lung segmentectomy has been regarded as a common type of surgery9,14. The Nanjing training station, as one of the earliest stations of the Royal College of Surgeons of Edinburgh for precision thoracic surgery training, is dedicated to training in the precision resection of lung segments. During this training, we demonstrated the novel stapler tractor, which provides a safer and more efficient way to dissect segmental vessels and offers a new approach for improving the development of lung segmentectomy. Compared with other operational processes and auxiliary tools, the benefits of using a stapler tractor for dissociating vascular structures in lung segmentectomy include, but are not limited to, shortened operation time, reduced intraoperative blood loss, shorter postoperative hospital stays, lower postoperative air leakage rates, and reduced rates of postoperative pulmonary embolism during the teaching period. These benefits were also observed in the learners at the Royal College of Surgeons of Edinburgh. Furthermore, the study methods and surgical evaluation techniques obtained through the analysis of surgical details from video playback in this study are helpful for evaluating and improving the quality of lung segmentectomy.
In total, 323 patients who underwent lung segmentectomy were enrolled at the Nanjing training station. The benefits of using a stapler for vascular dissociation in lung segmentectomy were analyzed by examining specific quantitative parameters from video replays of the surgical detail analysis. Although several published studies have reported that video-based surgical coaching is a reliable approach for improving performance15,16,17, the parameterization of data regarding the same surgical procedure criteria using different techniques or habits in surgical videos has not been addressed in the existing literature. Emerging studies reveal that surgical videos clearly document the entire surgical process, including the movements of the surgeon, the use of surgical instruments, and the details of each step. Assessing surgical skill by replaying these videos can provide objective and efficient tools for surgeons and can improve not only surgical techniques but also surgical procedures15,17.
However, these surgical techniques require comparative analysis based on concrete real data parameters18, distinct from the literature that analyzes surgical procedures in surgical videos19. Therefore, there are no standardized assessment criteria for evaluating the differences in the efficiency of these various techniques. The evaluation index (data parameters) adopted in this study is based on the improvement of action details in the evaluation of ball games. For example, when the surgeon finds it difficult to pass the stapler after freeing the segmental vessels, we consider this a technical foul. This difficulty is categorized as a failure to pass through the target vessel in this study, which corresponds to a low-quality parameter of the surgical procedure. Additionally, when the surgeon plans to dissociate segmental vessels, the total time also requires quality control; longer times are included in the assessment of lower surgical quality.
The parameter data in this study, which showed a significant reduction in total operative time in the used group compared with the non-used group, seems to exaggerate the effect of these tools, but it does not. The investigators believe that the reasons for these effects are: (1) the specific parametric data indicate that the time for segmental vessel dissection is significantly reduced, and the successful traction rate for passing through the segmental vessel is significantly increased, which is the main reason for the reduction in total operative time; (2) segmental vessel dissection using silk ligation or a stapler with silk requires space to be ligated at both ends and to be dissected in the middle to prevent the ligature from slipping. Here, our technique can reduce the time needed to dissociate the target vessel because the required dissociation length of the vessel is short. Additionally, the segmental vessels being dissociated do not bleed, allowing the surgical procedures to proceed smoothly, which also increases the confidence and morale of the operators. This ultimately facilitates the surgical procedure and reduces the total operative time. Although it takes time to put on and remove the stapler, the overall operation time is saved.
Intraoperative bleeding is one of the most common and serious complications in thoracoscopic surgery and frequently necessitates conversion to thoracotomy20. Previous studies have suggested that thoracoscopic lung vascular bleeding is related to surgeon skill and surgical instruments, and it can prolong hospital stays and increase hospitalization costs21.
A few patients may be forced to undergo total pneumonectomy due to intraoperative bleeding and may even die during or after surgery8. Thus, the safe handling of vessels is very important. Because segmental vessels need to be dissociated for a longer time, traditional techniques (such as silk ligation and stapling, unassisted or with target vessel traction using silk) often damage surrounding tissues, especially in patients with COPD. Our technique significantly reduced the occurrence of intraoperative bleeding during segmentectomy for three reasons: (1) the stapler tractor is made of soft silicone material, which gently passes through the target vessel and forms a closed loop from the entrance to the exit, protecting surrounding tissues from damage; (2) the stapler tractor requires only a small space and short length to traverse the target vessel, which saves operative time in freeing segmental vessels; (3) it exerts minimal tension on the segmental vessel, reducing the risk of tearing, making it more appropriate for use.
The vascular stump is an important factor affecting the safety of surgery. On one hand, if the stump is too short or if intraoperative bleeding occurs, it can be difficult to apply a vascular clamp or ligation; if the stump is sutured, vein or artery stem formation may occur. On the other hand, if the stump is too long, the patient may be prone to thrombosis. The length of the vessel stump is often reduced by using a stapler, which may need improvements in the future.
The occurrence of air leakage was lower in the used group compared to the non-used group, two experiences are worthy of attention: (1) the stapler tractor is made of soft silicone material, which gently passes through the target vessel and forms a closed loop from the entrance to the exit, protecting surrounding lung tissues from damage; (2) the stapler tractor requires only a small space and short length to traverse the target vessel, protecting surrounding lung tissues from damage.
Additionally, there are two other advantages to using the stapler tractor. (1) Sometimes, there are two or more vessels traveling at disparate angles that cannot be addressed using silk ligation or staplers (whether unassisted or with target vessel traction using silk). However, these vessels can be dissected simultaneously using a stapler tractor. To a certain extent, this approach may also reduce surgical costs. (2) The use of a stapler tractor serves as a reliable marker for accurately identifying the target vessel or bronchus22. For example, during LS1 + 2 + S3 resection, B1 + 2c or B3a is often difficult to confirm, and we can place the stapler tractor on the initial resection path as a marker and then determine it from the anterior mediastinum or posterior mediastinum view, respectively, to avoid incorrect resection.
Limitations
The study was not designed as a prospective randomized controlled study because of the need to review the details of the surgical video replay.
Conclusions
In summary, the use of a stapler tractor, which better protects the lung vessels, is a safer and more efficient method for dissecting segmental vessels and enhances the success of lung segmentectomy. The benefits of using a stapler tractor for vascular dissociation in lung segmentectomy include, but are not limited to, shortened operation time, reduced intraoperative blood loss, shorter postoperative hospital stays, and decreased rates of postoperative air leakage and pulmonary embolism. Furthermore, the evaluation indices (data parameters) obtained through the analysis of surgical details from video playback in this study are helpful for assessing and improving the quality of segmentectomy. In particular, this approach provides insights for scoring detailed parameters in surgical video competitions. Therefore, detailed analysis based on surgical video replays should focus not only on the procedures themselves but, more importantly, on the quality parameters of the surgical techniques.
Data availability
Data are available through the institutional medical charts database with relevant approvals. The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
References
Yao, F. et al. Thoracoscopic pulmonary segmentectomy with collateral ventilation method. Ann. Thorac. Surg. 112 (6), 1814–1823. https://doi.org/10.1016/j.athoracsur.2020.12.020 (2021).
Zhu, J. et al. Case report: Recombinant human endostatin plus chemotherapy for epidermal growth factor Receptor-Negative miliary lung adenocarcinoma. Front. Oncol. 12, 922076. https://doi.org/10.3389/fonc.2022.922076 (2022).
Xi, E. P. et al. Surgical treatment of aortoesophageal fistula induced by a foreign body in the esophagus: 40 years of experience at a single hospital. Surg. Endosc. 27 (9), 3412–3416. https://doi.org/10.1007/s00464-013-2926-3 (2013).
He, Z., Wu, W. & Chen, L. A ‘true segmentectomy’ cannot be overemphasized especially in the complex setting. Interdiscip Cardiovasc. Thorac. Surg. 36 (5), ivad075. https://doi.org/10.1093/icvts/ivad075 (2023).
Xu, X. F., Chen, L., Wu, W. B. & Zhu, Q. Thoracoscopic right posterior segmentectomy of a patient with anomalous bronchus and pulmonary vein. Ann. Thorac. Surg. 98 (6), e127–e129. https://doi.org/10.1016/j.athoracsur.2014.09.059 (2014).
Chen, L. & Wu, W. The main technical points of thoracoscopic anatomical lung segment resection. Zhongguo Fei Ai Za Zhi. 19 (6), 377–381. https://doi.org/10.3779/j.issn.1009-3419.2016.06.16 (2016). Chinese.
Wang, J. et al. Modified method for distinguishing the intersegmental border for lung segmentectomy. Thorac. Cancer. 9 (2), 330–333. https://doi.org/10.1111/1759-7714.12540 (2018).
Decaluwe, H. et al. Major intraoperative complications during video-assisted thoracoscopic anatomical lung resections: an intention-to-treat analysis. Eur. J. Cardiothorac. Surg. 48 (4), 588–598. https://doi.org/10.1093/ejcts/ezv287 (2015). discussion 599.
Zhu, J., Zhang, Y., Gao, X. H. & Xi, E. P. Coronavirus disease 2019 or lung cancer: A differential diagnostic experience and management model from Wuhan. J. Thorac. Oncol. 15 (8), e141–e142. https://doi.org/10.1016/j.jtho.2020.04.030 (2020).
Zhu, J. et al. Unveiling the synergetic benefits of the tunneling technique using stapler tractor in precise resection of lung segments: a retrospective cohort study. Front. Oncol. 14, 1417871. https://doi.org/10.3389/fonc.2024.1417871 (2024).
Cao, K. et al. Safety and efficacy of anatomical tunneling technique for precise lung segment resection in complex anatomical settings. BMC Surg. 24 (1), 409. https://doi.org/10.1186/s12893-024-02719-2 (2024).
Huang, K. et al. Rhinitis May be a clinical symptom of primary pulmonary lymphoepithelioma-like carcinoma, an incidental finding during the COVID-19 pandemic. Chin. Med. J. (Engl). 134 (15), 1883–1884. https://doi.org/10.1097/CM9.0000000000001541 (2021).
Heiden, B. T. et al. Association between surgical quality metric adherence and overall survival among US veterans with Early-Stage Non-Small cell lung cancer. JAMA Surg. 158 (3), 293–301. https://doi.org/10.1001/jamasurg.2022.6826 (2023).
Zhu, S. S. et al. The safety and efficacy of the fissure-first approach in lung segmentectomy for patients with incomplete fissures. Front. Oncol. 14, 1391835. https://doi.org/10.3389/fonc.2024.1391835 (2024).
Greenberg, C. C., Dombrowski, J. & Dimick, J. B. Video-Based surgical coaching: an emerging approach to performance improvement. JAMA Surg. 151 (3), 282–283. https://doi.org/10.1001/jamasurg.2015.4442 (2016).
Igaki, T. et al. Automatic surgical skill assessment system based on concordance of standardized surgical field development using artificial intelligence. JAMA Surg. 158 (8), e231131. https://doi.org/10.1001/jamasurg.2023.1131 (2023).
Chhabra, K. R., Thumma, J. R., Varban, O. A. & Dimick, J. B. Associations between video evaluations of surgical technique and outcomes of laparoscopic sleeve gastrectomy. JAMA Surg. 156 (2), e205532. https://doi.org/10.1001/jamasurg.2020.5532 (2021).
Bowyer, M. W. et al. A novel paradigm for surgical skills training and assessment of competency. JAMA Surg. 156 (12), 1103–1109. https://doi.org/10.1001/jamasurg.2021.4412 (2021).
Schlick, C. J. R., Bilimoria, K. Y. & Stulberg, J. J. Video-Based feedback for the improvement of surgical technique: A platform for remote review and improvement of surgical technique. JAMA Surg. 155 (11), 1078–1079. https://doi.org/10.1001/jamasurg.2020.3286 (2020).
Gonzalez-Rivas, D. et al. Intraoperative bleeding control by uniportal video-assisted thoracoscopic surgery†. Eur. J. Cardiothorac. Surg. 49 (Suppl 1), i17–24. https://doi.org/10.1093/ejcts/ezv333 (2016).
Liu, L. et al. International expert consensus on the management of bleeding during VATS lung surgery. Ann. Transl Med. 7 (23), 712. https://doi.org/10.21037/atm.2019.11.142 (2019).
Wu, W. B. et al. Three-dimensional navigation-guided thoracoscopic combined subsegmentectomy for intersegmental pulmonary nodules. Thorac. Cancer. 10 (1), 41–46. https://doi.org/10.1111/1759-7714.12897 (2019).
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Scientific Foundation of People’s Republic of China’s General Program [No.82372639, No.82401412 and No. 61971118], and the “Three Heroes and One Team” Talent Project of the Central Theater Command General Hospital of the People’s Liberation Army [No.2023 − 1692].
Author information
Authors and Affiliations
Contributions
Yang Xia: provided clinical data; assisted the conduction and analysis data of the present study; Jian Zhu: provided imaging data, wrote the manuscript, supervised study design; Quan Zhu, Jun Wang, Wei Wen, Shu-Sheng Zhu, Tan Tan, Zhibin Lu, Hu Tian: provided clinical data; assisted the conduction and analysis data of the present study; Weibing Wu, Liang Chen: conceptualization of this study, critical revision of the manuscript. All the authors revised the manuscript, read and finally approved the published manuscript and are responsible for ensuring the accuracy and completeness of the work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
All authors declare that they have no conflicts of interest or financial ties to disclose.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 2
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xia, Y., Zhu, J., Zhu, Q. et al. Unveiling the beneficial techniques in lung segmentectomy by using a stapler tractor for vascular dissection based on surgical video replay. Sci Rep 15, 34379 (2025). https://doi.org/10.1038/s41598-025-17168-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-17168-x
