
Abstract
Postpartum Depression (PPD) is a significant public health issue in China. Despite the launch of a universal PPD screening and intervention programme in Shenzhen, there remains a substantial gap between the number of women who screened positive and were referred for psychological interventions and those who actually presented at mental health institutions for further evaluation and treatment. This study sought to understand the factors influencing adherence to intervention referrals among women with positive PPD screening results. Using a retrospective study design, data from the programme management information system was analysed. The sample comprised 35,390 women who gave births in Shenzhen and screened positive for PPD between January 2016 and December 2020. Chi-square test and stepwise logistic regression were employed to determine factors affecting intervention uptake, with a p-value of less than 0.05 indicating statistical significance. The study found that although referral messages were given to 30,408 (85.9%) of women with positive PPD screening results, only 5,712 (16.1%) of them received psychological interventions. High school education (OR = 1.266, 95% CI: 1.1602 ~ 1.38), anxiety during pregnancy (OR = 1.126, 95% CI: 1.048 ~ 1.210), as well as bottle (OR = 1.368, 95% CI: 1.218 ~ 1.535) and mixed feeding (OR = 1.110, 95% CI: 1.043 ~ 1.181) were positively associated with treatment engagement. Conversely, women with EPDS scores of > 13 (OR = 0.892, 95% CI: 0.836 ~ 0.953), and temporary (OR = 0.860, 95% CI: 0.800 ~ 0.924) or floating residence (OR = 0.628, 95% CI: 0.550 ~ 0.713) were less likely to seek mental health support. This study contributes to a better understanding of the factors influencing intervention-seeking behaviours among women who screened positive for PPD in China. The main findings underline the necessity for tailored interventions that cater to the specific needs and circumstances of different groups of women. It is crucial to encourage treatment engagement through strategies such as psychoeducation, addressing stigma, and providing supportive resources.
Similar content being viewed by others

Introduction
Postpartum depression (PPD) is one of the most common complications of childbearing, affecting approximately one in six (17.2%) women after childbirth worldwide1. This disorder encompasses a range of mental, emotional and behavioural symptoms, often beginning within the first a few weeks after delivery and lasting up to one year2. If left untreated, PPD can lead to negative health consequences in both the women and their offspring3, ranging from mild symptoms such as low mood and anxiety to more severe outcomes such as recurrent or chronic depression, postpartum psychosis4, and cognitive and behavioural disorders in the children5,6. Moreover, women with severe PPD are at higher risk of committing suicide and infanticide7. It has been reported that PPD-related suicides account for up to 20% of all postpartum deaths8. As such, PPD has emerged as a critical public health problem warranting research and resource attention.
Studies have shown that screening for PPD, followed by diagnosis and appropriate management for those who detected positive, can effectively reduce the burden of this disorder9,10. Over the past decade, there has been a growing movement to integrate depression screening into routine postnatal care11,12,13,14. In 2020, the National Health Commission of China issued the first guideline for the prevention and treatment of perinatal depression, which emphasises the integration of PPD screening into routine postpartum home visits and the provision of mental health support for women identified at high risks15. However, despite high coverage of PPD screening at some local levels, the acceptance of psychological interventions among women with positive screening results remains low (ranging from 1 in 248 women to 19%)12,16. Identifying factors that influence PPD intervention acceptance can help enhance the efficacy of routine screening17 and support the implementation of the national guideline. Given China’s significant burden of PPD due to the enormous population size, understanding these factors is crucial for improving the mental health outcomes of millions of women and their families.
The existing literature on factors influencing PPD intervention uptake largely comprises qualitative studies. In a thematic synthesis of such literature, Hadfield et al. identified common barriers to those with positive PPD screening results seeking and receiving further support. These include the perception that the services might not be helpful, reluctance to take antidepressant medication due to concerns over side effects, the internalised stigma related to PPD, and a general lack of knowledge about the disease18. Another review found that healthcare providers’ influences, such as responses to the women’s emotional and practical needs, may also interfere with their decision to seek psychological treatment19. However, these reviews were limited to studies conducted in high-income countries with healthcare systems that differ significantly from those in China, which hampers the generalisability of the conclusions. Furthermore, there is a noticeable dearth of large-scale, quantitative studies in this realm, underscoring the necessity for robust, data-driven research in diverse settings to better understand the nuances of intervention-seeking behaviours among postpartum women.
In China, studies focusing on factors affecting PPD intervention uptake are limited. Gong et al. qualitatively surveyed 161 women who declined treatments, of which 128 (79.5%) believed they could manage their depressive symptoms on their own while 142 (88.2%) turned to their family members for support16. Another qualitative inquiry involving 46 women with positive PPD screening results found that the women’s adherence to referral recommendations was influenced by their understanding of the disease, perceived necessity for help, attitudes towards healthcare providers, and the support they received from their families20. Yet, mirroring global studies, these investigations are qualitative in nature, carrying inherent limitations like small sample sizes and limited representativeness. Moreover, these studies overlooked some important factors, such as the women’ sociodemographic characteristics, history of mental illness, childbirth experiences, and infant-related factors, which could significantly shape their help-seeking behaviours19,21.
To bridge the gaps mentioned above, a retrospective study was conducted using routine data from a government-funded universal PPD screening and intervention programme in Shenzhen Municipality, Southern China. Initiated in 2013, this programme offers free depression screening to all women who give birth in Shenzhen, regardless of their resident status, during routine postpartum home visits (held between 2 and 6 weeks after delivery). PPD is measured using a well validated Chinese version of the Edinburg Postnatal Depression Scale (EPDS)22,23, with cut-off scores of 10 and 13 indicating ”possible depression” and ”probable depression”, respectively12. These thresholds are internationally recognised and have been widely validated in China23,24,25. As required by the programme guideline26, women with EPDS scores of 10 ~ 13 are referred to clinical psychology departments within municipal or district-level maternal and child health institutions for further evaluation and consultation, while women with EPDS scores > 13 are referred to the municipal psychiatric specialty hospital or psychiatric departments within general hospitals for diagnosis and treatment. All women who screen positive are followed up for at least 4 weeks. The home visits and referrals are arranged by the local community health service centers (CHSCs) where the women live. Since its inception, the programme has screened 170,000 to 180,000 postpartum women annually, maintaining a coverage rate of approximately 80%12.
Utilising the programme data, this study aimed to ascertain the actual proportion of women who screened positive for PPD receiving psychological interventions, as well as to identify potential factors associated with adherence to intervention referrals. Given the dearth of large-scale quantitative evidence, the findings will provide important insights into the efficacy of existing PPD screening programmes and inform the development of strategies to improve treatment engagement, thereby reducing the burden of PPD on affected women and their families.
Methods
Study population
A retrospective study was conducted on women who gave birth in a public or private hospital in Shenzhen between January 1st, 2016 and December 31st, 2020 and were detected positive for PPD during postpartum home visits (EPDS score ≥ 10). According to the programme management information system, a total of 1,038,861 women were screened for PPD during this period, of whom 35,390 met the inclusion criteria and were included in the analysis. With China’s hospital delivery rate exceeding 99%27 and Shenzhen’s universal programme maintaining a high depression screening rate of 80% among all postpartum women12, this sample was viewed as representative of those with positive PPD screening results in the city. This study was approved by the Medical Ethics Committee of Shenzhen Maternity and Child Healthcare Hospital, Women and Children’s Medical Center, Southern Medical University [SFYLS[2024]004]. All methods were performed in accordance with the relevant guidelines and regulations.
Data collection
By 2020, the universal programme had successfully extended its coverage to all 647 communities across the 10 districts of Shenzhen. Designated health workers from the CHSCs bore the primary responsibilities for conducting routine postpartum home visits and follow-ups. During the home visits, they assisted postpartum women in completing the EPDS to screen for PPD and gathered information on the women’s sociodemographic, psychological, obstetric, and neonatal care through a pre-designed questionnaire. Women who screened positive were then given referral messages (including alerts about their depression risks and the necessity of receiving psychological interventions, address of psychology or psychiatric departments, and links of appointment registration) and followed up with by phone over a period of four weeks. The phone calls aimed to collect information on whether they had sought mental health support, which institution they had visited, what psychological interventions they had received, and whether their depressive symptoms had increased or decreased. This information was then validated by cross-referencing with the women’s medical records at psychology/psychiatric departments in the programme management information system. All women were informed prior to the screening that their data might be used for research and publication purposes, and they had the right to withdraw from the study at any time. Written INFORMED consent was obtained from each woman before enrolment.
Data from the postpartum home visits and follow-ups, along with information on the women’s intervention uptake, were manually entered into the programme management information system and double-checked for accuracy. Shenzhen Maternity and Child Healthcare Hospital, Women and Children’s Medical Center, Southern Medical University was responsible for coordinating the programme. To enhance programme implementation and data quality, the hospital organised periodic trainings for relevant CHSC health workers and conducted quality controls by randomly sampling and checking individual case records within the information system. For the purpose of this study, the original data was exported by authorised personnel, adhering strictly to the programme’s data privacy and security protocols. Access to the study database was restricted to the authors only.
Assessment of potential influencing factors
The study collected data on a range of variables relating to the sociodemographic, psychological, obstetric, and neonatal characteristics of postpartum women. These factors, potentially affecting psychological intervention acceptance, were identified through literature review19,21 and expert consultation, and were mostly assessed using single questions. Sociodemographic characteristics encompassed maternal age, education level (junior school and below, high school, bachelor’s degree, and master’s degree or higher), resident status (permanent resident, temporary resident – with a residence card, and floating population – without a residence card), family structure (nuclear family, living with parents, and living with parents-in-law), and annual family income in Chinese yuan (CNY) (below 120,000, 120,000 ~ 240,000, above 240,000). Psychological characteristics included EPDS score (10 ~ 13 and > 13), recent stressful life events (such as divorce, job loss, serious illness, or death of family members), family history of mental illness, and previous history of psychological issues. The women were specifically asked whether they had been screened positive for depression and anxiety during pregnancy. Obstetric characteristics included the women’s gravidity, parity, gestational age at delivery, and mode of delivery (vaginal delivery and caesarean delivery). Neonatal characteristics encompassed the presence of multiple births, Apgar score (7 ~ 10 and 0 ~ 6) and birth weight (low birth weight, normal, and high birth weight) of the infants, as well as their feeding patterns (breast, mixed, and bottle-fed).
Measurement of adherence to intervention referrals
Adherence to psychological Intervention referrals was defined as having at least one documented visit to a psychology or psychiatric department following referral, as recorded in the programme management information system. These visits occurred within public maternal and child healthcare institutions, a psychiatric specialty hospital or general hospitals in Shenzhen. It is possible that some women may have accessed care in private or online mental health facilities, which were not captured in the information system. However, according to feedback from follow-up personnel involved in the programme, such cases were relatively uncommon.
Statistical analysis
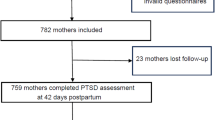
All statistical analysis were conducted using R version 4.0.2. Among the 35,390 postpartum women who screened positive for PPD and were included in the study (Fig. 1), referral and intervention rates were calculated by dividing the number of women who received referral messages and those who subsequently visited psychology or psychiatric departments, respectively. Trends over time in referral and intervention rates were assessed using the trend chi-square test, with a p-value < 0.05 considered statistically significant.
Descriptive statistics were used to summarise the frequency distributions of potential influencing factors. To explore factors associated with adherence to intervention referrals, we focused on the subset of women who received referral messages (n = 30,408). Chi-square tests were used to examine differences in sociodemographic, psychological, obstetric, and neonatal characteristics between women who adhered to intervention referrals and those who did not. Age, the only continuous variable, was categorised into four groups (16 ~ 20, 21 ~ 27, 28 ~ 34, and ≥ 35) to satisfy the logistic regression assumption of a linear relationship between the continuous predictor and the log odds of the outcome.
Variables that showed significant differences (p < 0.05) in the chi-square tests were further analysed using stepwise logistic regression to estimate odds ratios (OR) and 95% confidence intervals (95% CI). A p-value < 0.05 was used as the criterion for variable removal in the stepwise procedure. Before conducting the regression, model assumptions were checked, including absence of multicollinearity among independent variables and the linearity of the logit for continuous variables. No significant violations were found. The first category of each ordered categorical variable served as the reference group. For unordered categorical variables (e.g., family structure, feeding pattern), dummy variables were created, using nuclear families and bottle feeding as the reference categories, respectively.

Participant flow diagram.
Results
Basic information
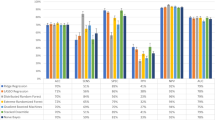
Among the 35,390 postpartum women who screened positive for PPD, 30,408 (85.9%) were given referral messages and followed up, among whom only 5,712 (16.1%) sought further interventions. As shown in Fig. 2, the proportion of women receiving referral messages increased steadily from 74.1% in 2016 to 97.2% in 2020 (χ2 = 1090.908, p < 0.001). This improvement reflects the expanding coverage and strengthening implementation of the universal screening and intervention programme across Shenzhen’s 647 communities. Nonetheless, given the citywide scale of implementation and decentralised delivery of postpartum services by community health workers, some variability in referral practices may have occurred, leading to incomplete referral delivery in earlier years or some districts.
Meanwhile, the uptake rate for psychological interventions remained relatively low, despite a gradual increase over time (χ2 = 1656.943, p < 0.001). The following univariate and multivariable analyses only pertain to women who have records of interventional referrals and follow-ups.

Referral and psychological intervention rates of women who screened positive for postpartum depression in Shenzhen, 2016–2020.
Sociodemographic characteristics of women who adhered to intervention referrals
The average age of the 30,408 women who received referral messages was 28.3 (standard deviation: 4.6, range: 16 ~ 50). As shown in Table 1, most of them (87.9%) were aged between 21 and 35. Regarding educational attainment, 35.0% had finished high school, and 46.4% had a bachelor’s degree or higher. The majority of the women held either permanent (29.5%) or temporary residence (61.4%) in Shenzhen, while 9.1% were part of the floating population. Nearly four-fifths (78.0%) reported an annual family income between CNY 120,000 and CNY 240,000. Half (49.0%) lived in nuclear families, while 38.8% lived with parents-in-law. Women with a high school education (χ2 = 49.662, p < 0.001) and permanent residence (χ2 = 59.730, p < 0.001) were more likely to adhere to referral recommendations. There was no statistically significant difference between those with different ages, economic statuses, and family structures.
Psychological characteristics of women who adhered to intervention referrals
Table 1 indicated that 34.2% of the women had EPDS scores > 13. Additionally, 20.4% and 34.3% had screened positive for depression and anxiety during pregnancy, respectively. Recent stressful life events were reported by 6.8% of women, while 1.0% and 0.9% reported a family history and a personal previous history of mental illness, respectively. Women with EPDS scores > 13 were less likely to undergo psychological intervention compared to those with lower scores (χ2 = 59.730, p = 0.025). In contrast, women who had screened positive for anxiety (χ2 = 59.730, p < 0.001) or depression (χ2 = 16.905 p < 0.001) during pregnancy were more likely to adhere to intervention referrals than women who had not. There was no statistically significant difference between women with experiences of stressful life events, family or previous history of mental illness, and those without.
Obstetric characteristics of women who adhered to intervention referrals
The majority of women had been pregnant once (39.8%) or twice (31.3%), and had given birth to one child (56.7%) or two children (37.4%). Most women delivered between 37 and 41 gestational weeks (88.2%) and underwent vaginal delivery (64.0%). Table 1 revealed that women who were pregnant for three or more times were more likely to seek psychological interventions (χ2 = 9.737, p = 0.021). However, no statistical significance was found between different parity, gestational age, and delivery mode groups.
Neonatal characteristics of women who adhered to intervention referrals
According to Table 1, 2.1% of the women had multiple births. Of the infants, 99% had Apgar scores between 7 and 10, indicating good health. Additionally, 90.5% had normal birth weights, 6.4% had low birth weights, and 3.1% were classified as large baby for gestational age. About half (56.2%) of the infants were breastfed, while 37.3% received mixed feeding. Statistical analysis indicated a significant correlation between feeding pattern and the women’s adherence to referral advice (χ2 = 38.477, p < 0.001). Women who used bottle feeding and mixed feeding were more likely to seek psychological support compared to women who exclusively breastfed. However, no significant association was found between different numbers of fetuses, Apgar scores, and birth weights.
Multivariable analysis of factors influencing adherence to intervention referrals
The stepwise logistic regression model included all seven variables demonstrating significant differences between women who adhered to intervention referrals and those who did not. As shown in Table 2, six potential determinants of adherence were identified. First, women with high school education were 1.266 times (95% CI: 1.160 ~ 1.382) more likely to accept referral advice compared to women with junior school education or below. Second, temporary (OR = 0.860, 95% CI: 0.800 ~ 0.924) and floating (OR = 0.628, 95% CI: 0.550 ~ 0.713) residents were less likely to adhere to intervention referrals compared to permanent residents. Third, women with EPDS scores > 13 were less likely to seek mental health services (OR = 0.892, 95% CI: 0.836 ~ 0.952) than women with EPDS scores of 10 ~ 13. Fourth, women who had screened positive for anxiety during pregnancy were 1.126 times (95% CI: 1.048 ~ 1.210) more likely to accept intervention referrals compared to women who had not. Lastly, in terms of infant feeding patterns, bottle feeding and mixed feeding women were 1.368 (95% CI: 1.218 ~ 1.535) and 1.110 (95% CI: 1.043 ~ 1.181) times more likely to follow referrals, respectively, compared to breastfeeding women.
Discussion
This study on factors affecting adherence to psychological interventions among 35,390 women who screened positive for PPD is, to date, the largest quantitative investigation of its kind in China. Using routine data from the universal PPD screening and intervention programme in Shenzhen, the study revealed that although referral messages were given to 85.9% of women with positive PPD screening results, only 16.1% of them received psychological interventions between 2016 and 2020. The screening-intervention gap is consistent with findings reported in published studies. Byatt et al.’s systematic review has found that, without intervention, the proportion of postpartum women seeking mental health support for positive depression screenings is only 22% on average (range: 14%~33%)28, which is lower than the rates observed in other major disease screening programmes such as colon cancer29. Thombs et al. pointed out that a low coverage rate of psychological intervention can significantly reduce the effectiveness of universal PPD screening, ultimately affecting the overall prevention and treatment outcomes17. These findings highlight the importance of increasing adherence to intervention referrals among women with positive PPD screening results and improving access to mental health services more broadly.
The reasons for the low psychological intervention rate among women who tested positive for PPD are multifaceted. Existing literature cites various reasons such as time constraints, transient improvements in mood30,31,32, viewing postpartum depression as normal and not necessitating intervention33,34, and the impracticality of attending in-person counselling with an infant35. In the context of China, specific factors may explain this low uptake. The current mental health resources are seriously inadequate, with only 0.1 psychiatric hospitals or psychiatric departments in general hospitals, 2.2 psychiatrists, and 5.4 psychiatric nurses (including community mental health workers) per 100,000 people. These figures are far lower than those in high-income countries such as the United States and Japan36. Multiple studies have shown that poor accessibility to mental health services is a major barrier to the uptake of psychological interventions among women with positive PPD screening results18,37,38,39. Many women abandon seeking help due to concerns about high treatment costs, inconvenient transportation, and stigmatisation40,41. Conversely, most women who screened positive only have temporary or mild depressive symptoms and only need simple mental health support rather than having to visit professional institutions42.
The statistical analysis revealed that the women’s adherence to intervention referrals was influenced by various sociodemographic, psychological, obstetric, and neonatal factors. Those with a high school education were more likely to accept psychological interventions compared to those with junior school education or below, while no significant difference was observed for those with a bachelor’s degree or above. It is inferred that women with lower education levels might face fewer time constraints and career pressures than women with higher education levels, facilitating their access to treatment43. Furthermore, women who had screened positive for anxiety during pregnancy might be more likely to seek support due to heightened awareness of their mental health status and existing contact with professionals, making the transition to depression treatments more seamless44. Regarding feeding pattern, women who adopted bottle or mixed feeding might have more time and flexibility for seeking psychological interventions compared to those who exclusively breastfeed. Bottle-feeding allows for the sharing of caregiving responsibilities with other family members, potentially reducing maternal stress and providing more opportunities for women to seek help. Some women might choose not to breastfeed due to pre-existing mental health conditions45, which might also explain a higher intervention adherence in this group.
This study revealed that women with EPDS scores > 13, indicative of higher levels of depressive symptoms, were less likely to seek mental health support. The debilitating symptoms of severe depression, including extreme fatigue or feelings of worthlessness, could hinder treatment-seeking19. Additionally, cognitive impairments caused by PPD, such as difficulties in concentration, decision-making, and memory4, could pose substantial barriers to accessing professional support. Furthermore, fears of social judgement or self-stigmatisation might exacerbate the women’s hesitancy to use mental health services46. Remarkably, it was observed that women with temporary or floating residence were less likely to adhere to intervention referrals compared to women with permanent residence. This could be attributed to the lack of stable access to local healthcare services and socio-economic challenges like unstable housing or employment47. Limited awareness of available mental health resources may also factor into their decreased treatment engagement48.
The utilisation of routine data from a universal PPD screening and intervention programme helped enhance quality of evidence49, offering a significant advancement over previous, predominantly qualitative studies based on smaller samples. The findings are likely more reflective of the reality given the high PPD screening and referral rates in Shenzhen. However, limitations do exist. First, given that adherence to intervention referrals was determined by the women’s electronic records at psychological/psychiatric departments within maternal and child health institutions or general hospitals, this study may have overlooked women who sought help at private or online mental health institutions. This could lead to an underestimation of the actual rate of intervention uptake. Second, the retrospective study design limits the ability to infer causality or temporal relationships between the variables studied. Third, the study was conducted in Shenzhen, a large and affluent city in China, limiting the generalisability of findings to rural areas or other parts of the country where mental health resources may be less accessible and cultural attitudes towards mental health may differ. Fourth, although stepwise logistic regression offers a practical approach for variable selection, it may increase the risk of overfitting and the omission of important confounding factors. This statistical method relies on automated selection criteria and may not fully account for theoretical or clinical relevance, which should be considered when interpreting the findings. Fifth, sensitivity analyses, such as using different EPDS cut-off points to define PPD, were not conducted. While EPDS ≥ 10 is a widely accepted threshold for identifying possible depression in Chinese populations, the absence of sensitivity analysis may limit the robustness of our findings across alternative scenarios. Sixth, although many influencing factors were included in the analysis, data on husbands and marital relationships were not available in the routine dataset. Prior research has shown that spousal support and relationship quality can significantly influence both the risk of PPD and women’s help-seeking behaviours50.
The findings of this study have important implications for PPD management in China. The large gap between the number of women who screened positive and those who received psychological interventions indicates an urgent need for improvement in the follow-up of PPD screening. This could involve strategies to encourage treatment engagement, such as psychoeducation, on-site counselling, addressing stigma, and providing supportive resources for help-seeking28,31. The various factors identified to influence the uptake of treatment referrals highlight the necessity of tailoring interventions to the specific needs and circumstances of different groups of women. For instance, more support might be needed for women with higher-level depressive symptoms, those with a history of anxiety during pregnancy, women with temporary or floating residence, and women who breastfeed. Considering that most women who screened positive for PPD only have temporary or mild symptoms, how to fully utilise limited mental health resources to construct a comprehensive intervention strategy that is personalised, equitable, destigmatised, and capable of effectively increasing the overall psychological intervention rate and sustaining implementation remains a challenging task at the current stage.
Conclusion
In conclusion, this study reveals the complex interplay of sociodemographic, psychological, obstetric, and neonatal factors influencing adherence to psychological intervention referrals among women who screened positive for PPD in Shenzhen, China. It highlights the critical gaps in treatment engagement, particularly among women with higher levels of depressive symptoms, anxiety during pregnancy, temporary or floating residence, and those who breastfeed. The findings underscore the need for a more personalised, comprehensive, and destigmatised approach to PPD management, which addresses the specific needs and circumstances of different groups of women. While the study advances our understanding of the factors influencing PPD intervention-seeking behaviours, further research is needed to develop and test strategies to increase intervention uptake and improve mental health outcomes among postpartum women in China.
Data availability
The datasets generated and analysed during the current study are not publicly available due to the data protection policies of the PPD screening and intervention programme in Shenzhen. However, the data are available from the corresponding author upon reasonable request and subject to approval by the Medical Ethics Committee of Shenzhen Maternity and Child Healthcare Hospital, Women and Children’s Medical Center, Southern Medical University.
Abbreviations
- PPD:
-
Postpartum depression
- EPDS:
-
Edinburg postnatal depression scale
- CHSC:
-
Community health service center
- CNY:
-
Chinese yuan
- OR:
-
Oddis ratios
- CI:
-
Confidence interval
References
Wang, Z. et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry. 11, 543 (2021).
O’Hara, M. W. Postpartum depression: current status and future directions. Annu. Rev. Clin. Psychol. 9, 379–407 (2013).
Howard, L. M., Molyneaux, E., Dennis, C. L., Rochat, T. & Stein, A. M. Non-psychotic mental disorders in the perinatal period. Lancet 384, 1775–1788 (2014).
RCPSYCH. Postnatal depression. [cited 2023 Jan 1]; Available from: https://www.rcpsych.ac.uk/mental-health/problems-disorders/post-natal-depression (2018).
Farías-Antúnez, S. & Xavier, M. O. Effect of maternal postpartum depression on offspring’s growth. J. Affect. Disord. 228, 143–152 (2018).
Mulraney, M., Giallo, R., Efron, D., Brown, S. & Nicholson, J. M. Maternal postnatal mental health and offspring symptoms of ADHD at 8–9 years: pathways via parenting behavior. Eur. Child. Adolesc. Psychiatry. 28, 923–932 (2019).
de Avila Quevedo, L. et al. Suicide risk and mood disorders in women in the postpartum period: a longitudinal study. Psychiatr Q. 92, 513–522 (2021).
Lindahl, V. & Pearson, J. L. Prevalence of suicidality during pregnancy and the postpartum. Arch. Womens Ment Health. 8, 77–87 (2005).
Lin, J. S. et al. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews, in Screening for Cognitive Impairment in Older Adults: An Evidence Update for the U.S. Preventive Services Task Force. Agency for Healthcare Research and Quality (US): Rockville (MD). (2013).
Yawn, B. P. et al. TRIPPD: a practice-based network effectiveness study of postpartum depression screening and management. Ann. Fam Med. 10, 320–329 (2012).
Avalos, L. A., Raine-Bennett, T., Chen, H. & Adams, A. S. Improved perinatal depression screening, treatment, and outcomes with a universal obstetric program. Obstet. Gynecol. 127, 917–925 (2016).
Jiang, L. et al. Towards universal screening for postpartum depression in china: lessons learned from a comprehensive prevention programme in Shenzhen. Matern Child. Health J. 26, 2109–2117 (2022).
Learman, L. A. Screening for depression in pregnancy and the postpartum period. Clin. Obstet. Gynecol. 61, 525–532 (2018).
Venkatesh, K. K., Nadel, H., Blewett, D., Freeman, M. P. & Kaimal, A. J. Implementation of universal screening for depression during pregnancy: feasibility and impact on obstetric care. Am. J. Obstet. Gynecol. 215, 517e1–517e8 (2016).
Work Plan for the Exploration of Depression Prevention and Treatment Specific Services. National Health Commission: Beijing. (2020).
Gong, W., Jin, X., Cheng, K. K., Caine, E. D. & Lehman, R. Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression. Int. J. Environ. Res. Public. Health 17. (2020).
Thombs, B. D. et al. Depression screening and patient outcomes in pregnancy or postpartum: a systematic review. J. Psychosom. Res. 76, 433–446 (2014).
Hadfield, H. Women’s experiences of seeking and receiving psychological and psychosocial interventions for postpartum depression: A systematic review and thematic synthesis of the qualitative literature. J. Midwifery Womens Health. 62, 723–736 (2017).
Dennis, C. L. & Chung-Lee, L. Postpartum depression help-seeking barriers and maternal treatment preferences: a qualitative systematic review. Birth 33, 323–331 (2006).
Xue, W. et al. Barriers and facilitators for referring women with positive perinatal depression screening results in china: a qualitative study. BMC Pregnancy Childbirth. 23, 230 (2023).
Goodman, J. H. Detection, treatment, and referral of perinatal depression and anxiety by obstetrical providers. J. Womens Health (Larchmt). 19, 477–490 (2010).
Lee, D. T. et al. Detecting postnatal depression in Chinese women. Validation of the Chinese version of the Edinburgh postnatal depression scale. Br. J. Psychiatry. 172, 433–437 (1998).
Lau, Y., Wang, Y., Yin, L. & Chan, K. S. Validation of the Mainland Chinese version of the Edinburgh postnatal depression scale in Chengdu mothers. Int. J. Nurs. Stud. 47, 1139–1151 (2010).
Wu, D. & Jiang, L. Additional evidence on prevalence and predictors of postpartum depression in china: A study of 300,000 puerperal women covered by a community-based routine screening programme. J. Affect. Disord. 307, 264–270 (2022).
Gibson, J., McKenzie-McHarg, K., Shakespeare, J. & Price, J. A systematic review of studies validating the Edinburgh postnatal depression scale in antepartum and postpartum women. Acta Psychiatr Scand. 119, 350–364 (2009).
Work Plan for the Screening and Intervention of Postpartum Depression in Shenzhen. Shnzhen Health and Family Planning Commission: Shenzhen. (2013).
Xinhua China’s hospital delivery rate remains over 99%. https://english.www.gov.cn/statecouncil/ministries/202104/29/content_WS608ab2fbc6d0df57f98d8d27.html (2021).
Byatt, N., Levin, L. L., Ziedonis, D. & Moore Simas, T. A. Enhancing participation in depression care in outpatient perinatal care settings: A systematic review. Obstet. Gynecol. 126, 1048–1058 (2015).
Dalton, A. R. H. Incomplete diagnostic follow-up after a positive colorectal cancer screening test: a systematic review. J. Public. Health (Oxf). 40, e46–e58 (2018).
Trost, M. J., Molas-Torreblanca, K., Man, C., Casillas, E. & Sapir, H. Screening for maternal postpartum depression during infant hospitalizations. J. Hosp. Med. 11, 840–846 (2016).
Xue, W. Q., Cheng, K. K., Xu, D. & Jin, X. Uptake of referrals for women with positive perinatal depression screening results and the effectiveness of interventions to increase uptake: a systematic review and meta-analysis. Epidemiol. Psychiatr Sci. 29, e143 (2020).
Bauer, N. S., Ofner, S., Pottenger, A. & Carroll, A. E. Follow-up of mothers with suspected postpartum depression from pediatrics clinics. Front. Pediatr. 5, 212 (2017).
Rowan, P., Greisinger, A., Brehm, B. & Smith, F. M. R. Outcomes from implementing systematic antepartum depression screening in obstetrics. Arch. Womens Ment Health. 15, 115–120 (2012).
Drake, E. & Howard, E. Online screening and referral for postpartum depression: an exploratory study. Community Ment Health J. 50, 305–311 (2014).
Pinar, S., Ersser, S. J. & McMillan, D. Support and services for perinatal low mood and depression: A qualitative study exploring women’s and healthcare professionals’ experiences (Nurs Health Sci, 2022).
WHO. Global Health Observatory data repository: Mental health. [cited 2023 Jan 30]; (2023). Available from: https://apps.who.int/gho/data/node.main.MENTALHEALTH?lang=en
Maxwell, D. & Robinson, S. R. I keep it to myself: A qualitative meta-interpretive synthesis of experiences of postpartum depression among marginalised women. Health Soc. Care Commun.. 27, e23–e36 (2019).
Megnin-Viggars, O., Symington, I. & Howard, L. M. Experience of care for mental health problems in the antenatal or postnatal period for women in the UK: a systematic review and meta-synthesis of qualitative research. Arch. Womens Ment Health. 18, 745–759 (2015).
Sambrook Smith, M., Lawrence, V. & Sadler, E. Barriers to accessing mental health services for women with perinatal mental illness: systematic review and meta-synthesis of qualitative studies in the UK. BMJ Open. 9, e024803. (2019).
Chen, H., Wang, J., Ch’ng, Y. C., Mingoo, R. & Lee, T. Identifying mothers with postpartum depression early: integrating perinatal mental health care into the obstetric setting. ISRN Obstet Gynecol. 2011, 309189. (2011).
Kim, J. J., La Porte, L. M., Corcoran, M., Magasi, S. & Batza, J. Barriers to mental health treatment among obstetric patients at risk for depression. Am. J. Obstet. Gynecol. 202, 312e1–312e5 (2010).
Bhat, A., Nanda, A., Murphy, L., Ball, A. L. & Fortney, J. A systematic review of screening for perinatal depression and anxiety in community-based settings. Arch. Womens Ment Health. 25, 33–49 (2022).
Wang, P. S. et al. Delay and Failure in Treatment Seeking after First Onset of Mental Disorders in the6177–185 (World Health Organization’s World Mental Health Survey Initiative. World Psychiatry, 2007).
Dennis, C. L. & Falah-Hassani, K. Prevalence of antenatal and postnatal anxiety: systematic review and meta-analysis. Br. J. Psychiatry. 210, 315–323 (2017).
Cooklin, A. R. et al. Physical health, breastfeeding problems and maternal mood in the early postpartum: a prospective cohort study. Arch. Womens Ment Health. 21, 365–374 (2018).
Barney, L. J., Griffiths, K. M. & Jorm, A. F. Stigma about depression and its impact on help-seeking intentions. Aust N Z. J. Psychiatry. 40, 51–54 (2006).
Burgard, S. A. & Seefeldt, K. S. Housing instability and health: findings from the Michigan recession and recovery study. Soc. Sci. Med. 75, 2215–2224 (2012).
Kawachi, I. Social ties and mental health. J. Urb. Health. 78, 458–467 (2001).
Kalra, D. Raising the impact of real world evidence. Stud. Health Technol. Inf. 258, 1 (2019).
Pilkington, P. D., Milne, L. C., Cairns, K. E. & Lewis, J. Modifiable partner factors associated with perinatal depression and anxiety: a systematic review and meta-analysis. J. Affect. Disord.. 178, 165–180 (2015).
Acknowledgements
The authors would like to express their gratitude to Shenzhen Maternity and Child Healthcare Hospital, Women and Children’s Medical Center, Southern Medical University for the coordination and support of this study. They also acknowledge the dedicated health workers involved in the PPD screening and intervention programme in Shenzhen. Furthermore, they extend their appreciation to all the postpartum women who consented to participate, making this study possible.
Funding
This study was supported by the National Natural Science Foundation of China [72374096], Shenzhen Science and Technology Program [JCYJ20230807120309020], Shenzhen Key Laboratory of Maternal and Child Health and Diseases [ZDSYS20230626091559006], and the Research Fund of Shenzhen Maternity and Child Healthcare Hospital [FYA2022001].
Author information
Authors and Affiliations
Contributions
D.W. conceptualised the study and prepared the manuscript. S. C. carried out the statistical analysis. S. L. and J. Z. undertook the literature review and made contributions to the manuscript. G. Z. was responsible for managing the programme management information system and assisted in data export. L. J. coordinated the PPD screening and intervention programme. J. H. provided valuable comments on the manuscript. All authors have reviewed and given approval for the final version of the article.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Shenzhen Maternity and Child Healthcare Hospital, Women and Children’s Medical Center, Southern Medical University [SFYLS[2024]004]. Written INFORMED consent was obtained from each woman before enrolment.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, D., Chen, S., Liu, S. et al. Factors influencing adherence to psychological intervention referrals among women who screened positive for postpartum depression in Shenzhen, China (2016–2020). Sci Rep 15, 31298 (2025). https://doi.org/10.1038/s41598-025-17281-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-17281-x
