
Abstract
Signaling molecules released from the urothelium by mechanical stretch are known to play a sensory role in bladder contractions via neuronal signaling. It is also theorized that these molecules released from the urothelium could act locally to induce urothelial cell-mediated local bladder contractions. In this study, we specifically stimulated the urothelial cells using optogenetics to investigate how the urothelial released signaling molecules can influence bladder contractions locally. Using an ex-vivo whole bladder preparation, we stimulated the urothelial cells by activating channelrhodopsin-2 (ChR2) with blue light and initiated the urothelial cell-mediated local bladder contractions. The P2X receptor antagonist, PPADS, nearly abolished the contractions. The muscarinic receptor antagonist, atropine, significantly inhibited the contractions. Nifedipine, which blocks extracellular Ca2+ entry, abolished the contractions. G protein-coupled receptor inhibitor YM–254,890 significantly inhibited the contractions. Hemichannel inhibitor carbenoxolone disodium and the exocytotic pathway of transmitter release inhibitor brefeldin A also showed significant inhibition of the contractions. In conclusion, we validated the previous hypothesis that urothelial release factors can influence bladder contractions locally without the need for signaling from the central nervous system. Further studies are needed to determine the relevance of this signaling pathway in normal bladder physiology and pathophysiologic conditions.
Similar content being viewed by others


Introduction
The innermost layer of the bladder, the urothelium, contributes to sensory signaling and communicates environmental changes to other associated tissues, including nerve endings and the detrusor muscle1’2. Recently, using a transgenic mouse model, we showed that direct stimulation of the urothelial cells results in pelvic nerve afferent firing, which leads to bladder contractions3. Additionally, in ex vivo bladder preparations, we showed that stimulation of the urothelial cells can also produce a smaller bladder contraction without an intact CNS3. These findings led us to conduct the present study to explore the signaling mechanisms involved in the urothelial cell-mediated local bladder contractions.
Spontaneous contractile activity was observed in the urothelium-intact muscle preparations and disappeared when the mucosa (including the urothelium) was removed, suggesting that the urothelium influenced this spontaneous detrusor activity4. The intraluminal application of ATP induced contractions in isolated intact bladder preparations, which were significantly inhibited by atropine, and the removal of the urothelium caused a similar reduction of contractions as elicited by atropine5. Together, these results suggest that the urothelium can influence detrusor contractions.
Understanding the precise role of the urothelium in facilitating local bladder contractions remains a complex challenge. This is partly due to the presence of ATP and acetylcholine (ACh) receptors, the primary mediators of the detrusor contractions, in the urothelium, afferent nerve endings in the lamina propria, and the detrusor muscle. Isolating the specific contribution of the urothelium in local contractions using a pharmacological approach is complicated by this distribution of receptors. Furthermore, the close proximity of these cell types and their capacity to release similar signaling molecules adds to the difficulty of this work.
To overcome these limitations, we developed a mouse model where ChR2, a light-activated non-selective cation channel, is selectively expressed in the urothelial cells. This urothelial-specific ChR2 mouse model allowed us to specifically stimulate the urothelial cells with light and study its downstream effects on the detrusor muscle. Using an ex vivo bladder preparation, we showed that the urothelial cells can evoke local bladder contractions by releasing ATP and ACh that act on the detrusor muscles. The signaling mechanism for these urothelial cell-mediated local bladder contractions seems to activate the existing pathways of purinergic and muscarinic receptors, leading to the contractions of the detrusor smooth muscles. Our approach in this study will have a long-lasting impact on biomedical research regarding how we study the urothelial-to-detrusor muscle communication and the changes that may occur under disease conditions.
Materials and methods
Animals
All experiments were approved by the University of Florida Institutional Animal Care and Use Committee (IACUC). Experiments and mice handling were done in strict accordance with the National Institutes of Health (NIH) Guide for the Care and Use of Laboratory Animals. Male mice aged 9–17 weeks old were used in this study, and all experiments were performed during the light cycle (0600–1800 h). Mice were housed on a 12:12-hour light-dark cycle and provided food and water ad libitum. Transgenic mice were produced by crossing the Ai32 line (No. 024109, The Jackson Laboratory) that expresses ChR2 in the presence of Cre, with uroplakin II (UPK2)-cre mice (No. 029281, The Jackson Laboratory) that expresses cre recombinase in the bladder urothelium3,6,7. This transgenic mouse line expresses ChR2 within the urothelium and allows for the targeted activation of the urothelial cells with exposure to blue light. These mice will be referred to as UPK2-ChR2 throughout the manuscript. We showed in our recently published paper that no overt differences were observed in optogenetic-evoked bladder contractions between male and female mice3. We used male mice in this study due to the technical advantage of securing fiber optics through the urethra compared to female mice, as males have a longer remaining urethra adjacent to the bladder neck.
Tissue Preparation
The ARRIVE guidelines were followed for the experiments conducted with mice. Following exposure of mice to 2–3% isoflurane and confirmation of anesthetic plane, mice were quickly euthanized with cervical dislocation. The urinary bladders were quickly excised and placed in a petri dish filled with Kreb’s solution containing (in mM) 119 NaCl, 4.7 KCl, 24 NaHCO3, 1.2 KH2PO4, 2.5 CaCl2, 1.2 MgSO4, and 11 glucose at pH 7.3–7.4. The urinary bladder was freed from the connective and adipose tissues. The optical fiber (FT200UMT, Thor Labs) was inserted through the opening of the remaining urethra and secured with a 5–0 nylon suture (No. 07-809-8813, Patterson Veterinary). The prepared whole bladder was taken for isometric tension recording. The two ends of the bladder (dome and neck) were tied with 4–0 silk suture (07-891-0230, Patterson Veterinary) where a loop of thread was made at the bottom end (dome) to allow the tissue to be mounted to the isometric recording system (Fig. 1a). The bladder lumen remained open to the Krebs’ solution through the urethra. The fiber optic did not completely obstruct the solution from getting to the lumen through the urethral opening.
Isometric tension recording
The isometric tension recording of the bladder was performed as a modified version of the previously described8. The optical fiber was connected to a 473 nm blue laser (BL473T8-150FC, Lasercentury). The prepared bladder was vertically mounted in a 10–mL organ bath (Radnoti organ bath system, RSBRAD504/C) filled with Kreb’s solution and continuously aerated with 95% O2 and 5% CO2. The loop made at the dome of the bladder was hooked with a glass rod, and the other end was attached to a force transducer (FORT10G, World Precision Instruments) (Fig. 1a). The transducer was attached with a Transbridge amplifier (TBM4, World Precision Instruments). The output of the amplifier was captured at a sampling rate of 1 kHz using a Micro 1401 data acquisition system (Cambridge Electronic Design) and Spike2 software (V10, Cambridge Electronic Design).

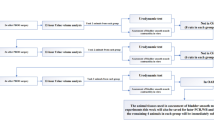
Ex-vivo bladder setup and recording the urothelial cell-mediated local bladder contractions. (a) An outline of the ex-vivo whole bladder isometric tension recording setup. The prepared bladder was set up in a 10–mL organ bath containing Kreb’s solution bubbled with carbogen, and temperature (37 °C) was maintained by using a circulating hot water bath. A fiber optic was inserted into the bladder through the remaining urethra and secured with nylon thread. One end of the bladder was attached to a glass hook, and the other to an isometric force transducer with silk thread to record the contractions in response to light or drugs. (b) A diagram showing how we measured the amplitude of the urothelial cell-mediated local bladder contraction. Light-evoked contractions were quantified by measuring the maximum contractile response during the 10-second light exposure (between 2 and 3) and subtracting the maximum in the 10 s previous to the stimulation as the baseline (between 1 and 2). Resulting in the amplitude of contraction illustrated by the orange line
The bladders were subjected to ~ 0.4–0.5 g of tension and allowed to equilibrate for 1 h in fresh oxygenated Kreb’s solution. The bladder chamber temperature was maintained at 37 °C with a circulating hot water bath (T72244004, Radnoti thermal bath/circulator).
After a one-hour equilibration period, we confirmed that bladders were viable and produced stable contractions by briefly (20–30 s) exposing the bladders to the hypertonic 70 mM KCl 3–5 times at 10–15 min intervals. Differences in contractile response between isotonic and hypertonic KCl have been observed in aorta smooth muscle recordings9. To our knowledge, this has not been explored in bladder tissue. We washed the bladders 3–5 times after each exposure with 70 mM KCl. After getting 2–3 consistent contractions with 70 mM KCl we applied 20 mW of blue light (5 s duration) 3 times at 2–3-minute intervals and induced the urothelial cell-mediated local bladder contractions. After establishing baseline bladder contractions, we directly applied different antagonists to the bath. After an incubation period (10–35 min), light was applied again 3 times to evoke the urothelial cell-mediated local bladder contractions. Light-evoked contractions were quantified by measuring the maximum contractile response during the 10-second light exposure and subtracting the maximum in the 10 s previous to the stimulation as the baseline (Fig. 1b). These light-evoked contractile responses were averaged and normalized relative to the corresponding high KCl contractions in the same bladder preparation.
After a drug incubation period and testing, the bladder was washed 3–5 times with Kreb’s solution and then refilled with Kreb’s solution. Therefore, depending on the incubation period of drugs (10–35 min), the refreshment of the bath solution varies from 40 to 65 min, including control experiments and experiments in the presence of drugs.
Drugs and dilutions
Pyridoxalphosphate-6-azophenyl-2’,4’-disulfonic acid tetrasodium salt (PPADS) (0625) and adenosine-5’-(γ-thio)-triphosphate tetralithium salt (ATP) (4080) were purchased from Tocris Bioscience. Carbachol (10217179) and atropine sulphate (AAA1023609) were obtained from ThermoFisher Scientific. Nifedipine (4013408), carbenoxolone disodium (102624936), brefeldin A (0000216670), and YM– 254,890 (0000244228) were purchased from Sigma Aldrich. PPADS, ATP, carbachol, atropine sulphate and carbenoxolone disodium were diluted with saline water, whereas nifedipine, brefeldin A, and YM– 254,890 were diluted with dimethyl sulfoxide (DMSO) (4101628926). The final concentrations of the DMSO for these drugs vary from 0.0001 to 0.01%. The diluted drugs were aliquoted and stored at 4 °C or −20 °C according to manufacturer instructions. The drug’s stock solutions concentrations were as follows (in mM): carbachol 10, ATP 50, PPADS 100, atropine 10, CBX 100, BFA 20, nifedipine 10, and YM–254,890 1. The following final concentrations of drugs used were PPADS (2 mM), atropine (2 µM), YM–254,890 (100 nM), nifedipine (2 µM), carbenoxolone disodium (100 µM) and brefeldin A (200 µM). 3.5 M KCl stock solution was prepared and stored at 4 °C to record high KCl (70 mM)-induced contractions. The incubation periods of drugs prior to light applications were as follows (in minutes): PPADS 15–20, atropine 10–15, CBX 30–35, BFA 30–35, nifedipine 15–20, and YM–254,890 15–20.
Data analysis
The peak contractions produced in response to light, muscarinic agonist carbachol, and purinergic agonist ATP were expressed relative to the percentage of the reproducible 70 mM KCl-induced contractions measured in the same bladder preparation. The inhibitory percentage of drugs for the urothelial cell-mediated local bladder contractions was determined relative to the percentage of the control contractions before the addition of drugs into the bath solutions. Data are expressed as the mean ± standard deviation (SD) of the mean, n = the number of animals used. The Student’s paired t-test (two-tailed) was performed to determine the statistical significance of differences. The Shapiro-Wilk normality (Gaussian) test was performed to determine whether the distribution of values is parametric or non-parametric by using GraphPad Prism version 10.0.2. If the values passed the normality test, then a parametric Student’s paired t-test was conducted. Otherwise, a non-parametric Student’s paired t-test was conducted. Differences were considered statistically significant when p < 0.05. The original traces and column graphs were constructed by using GraphPad Prism software (version 10.1.1), and the figures were designed using Affinity Designer version 2.2.1.
Results

Optogenetic activation of urothelial cells produced local bladder contractions. (a) Representative recording of the urothelial cell-mediated local bladder contractions evoked by blue light (20 mW, 5 s) and red light (20 mW, 5 s), showed that only the blue light activates the ChR2 expressed into the urothelial cells in UPK2-ChR2 Cre+ mice and produces contractions. (b) Unlike the UPK2-ChR2 Cre+ mice, UPK2-ChR2 Cre– mice that do not express ChR2 into the urothelial cells did not produce contractions in response to blue light (20 mW, 5 s). (c) Summarized data of the urothelial cell-mediated local bladder contractions. The amplitude of the urothelial cell-mediated local bladder contractions was expressed as a percentage of the 70 mM KCl-evoked contractions in the same preparation. Each point represents the mean ± SD of the mean (n = 5 for UPK2-ChR2 Cre+ mice and n = 4 for UPK2-ChR2 Cre–mice). Blue or red bars correspond to light stimulation
Optogenetic activation of the urothelial cells elicits local bladder contractions ex vivo
We have previously demonstrated that the application of blue light (20 mW, 5 s) produces a urothelial cell-mediated local bladder contraction in excised bladders as measured by intraluminal pressure3. In the present study, we showed the urothelial cell-mediated local bladder contractions specifically in ex vivo using an isometric force transducer from the excised bladder of UPK2-ChR2 mice. The urothelial cell-mediated local bladder contractions produced by light can clearly be distinguished from the baseline spontaneous contractions (Fig. 2a). We also applied red light in the same Cre+ UPK2-ChR2 mice (Fig. 2a) and blue light in Cre– UPK2-ChR2 mice (Fig. 2b), which produced almost no contractions (Fig. 2c). These results suggest that these contractions produced by activation of the urothelial cells are specific to blue light that depends on the expression of ChR2 into the urothelial cells. The urothelial cell-mediated local bladder contractions relative to the 70 mM KCl-evoked contractions in the same preparations were 2.804 ± 0.28% (n = 35). There were no significant differences (p = 0.128, n = 10) between the initial 70 mM KCl-evoked contractions and the final 70 mM KCl-evoked contractions after completion of light-evoked contractile studies with drugs (PPADS, atropine, YM–254890, carbenoxolone, and brefeldin A). However, the 70 mM KCl-evoked contractions before and after the experiments with nifedipine were largely reduced. It has been reported to have different resting tension of the aorta with the exposure of isotonic K+ (30 mM K+ substituted with 30 mM Na+) and hypertonic high K+(30 mM K+, not substituted with Na+) with different pretensions applied (1–3.5 g)9. We applied a tension of 0.4–0.5 g and used hypertonic high K+ (70 mM K+, only for 20–30 s, followed by washing 3–5 times) for testing bladder contractility and normalizing the light-evoked responses. We found no remarkable changes in the baseline resting tension after the completion of the experiment, which excludes the possible alteration of bladder tonicity by hypertonic high K+.

Effects of purinergic receptor inhibitor PPADS and muscarinic receptor antagonist atropine on the urothelial cell-mediated local bladder contractions. (a, d) Contractions evoked by 70 mM KCl and blue light (20 mW, 5 s). Blue light evoked urothelial cell-mediated local bladder contractions were recorded in the presence of vehicle and PPADS (2 mM) and atropine (2 µM), respectively. (b, e) Summarized data showing the inhibitory effects of PPADS (2 mM) and atropine (2 µM) on the urothelial cell-mediated local bladder contractions, respectively. (c, f) Summarized data of the percentage of inhibition of the urothelial cell-mediated local bladder contractions by PPADS (2 mM) and atropine (2 µM), respectively. The amplitude of the urothelial cell-mediated local bladder contractions was expressed as a percentage of the 70 mM KCl-evoked contractions in the same preparation. Each point represents the mean ± SD of the mean (n = 4 for PPADS and n = 9 for atropine). **Significantly different (p = 0.007) from the corresponding control values. Blue bars correspond to light stimulation
Effects of non-specific p2 purinergic receptor inhibitor Ppads on the urothelial cell-mediated local bladder contractions
In this study, we investigated the role of ATP in producing urothelial cell-mediated local bladder contractions. Andersson, 2015 reviewed the role of ATP in activating purinergic receptors in inducing contractions of the bladder10. In our experiments, the urothelial cell-mediated local bladder contractions were significantly and almost completely inhibited by purinergic receptor inhibitor PPADS (2 mM) (Fig. 3a and b). The urothelial cell-mediated local bladder peak contractions relative to 70 mM KCl-evoked contractions before and after application of PPADS (2 mM) were 1.91 ± 0.32% and 0.09 ± 0.08% (n = 4), respectively (Fig. 3b). PPADS (2 mM) was able to inhibit optically activated contractile responses by 96.00 ± 3.01% (n = 4) when calculated as relative to percentage of control peak contractile responses (Fig. 3c). These results confirmed that purinergic receptors are critical in inducing the urothelial cell-mediated local bladder contractions, as the contractions were mostly ablated by their inhibition.
Effects of muscarinic receptor inhibitor Atropine on the urothelial cell-mediated local bladder contractions
Previous findings showed that contractions evoked by the application of exogenous ATP inside the bladder lumen were inhibited by muscarinic receptor inhibitor atropine in ex vivo whole bladder preparation of rat5. These authors proposed that ATP may have a role in mediating the release of acetylcholine from the urothelial cells. Therefore, we investigated the possibility of whether the urothelial cell-mediated local bladder contractions involve muscarinic signaling pathways. Atropine (2 µM), a muscarinic receptor antagonist, significantly inhibited the urothelial cell-mediated local bladder contractions (Fig. 3d and e). The mean peak amplitudes of the urothelial cell-mediated local bladder contractions relative to the 70 mM KCl-evoked contractile amplitudes before and after the application of atropine (2 µM) were 3.19 ± 0.67% and 2.19 ± 0.70% (n = 9), respectively (Fig. 3e). The percentage of inhibition of contractions in the presence of atropine (2 µM) was 35.90 ± 5.77% (n = 9) relative to the corresponding control contractions (Fig. 3f). These results suggest that muscarinic receptors also contribute to inducing the urothelial cell-mediated local bladder contractions.

YM–254,890 attenuates the urothelial cell-mediated local bladder contractions. (a) Representative recordings of the contractions evoked by 70 mM KCl and blue light (20 mW, 5 s). Blue light evoked urothelial cell-mediated local bladder contractions were recorded in the presence of vehicle and YM–254,890 (100 nM). (b) Summarized data showing the inhibitory effects of YM–254,890 (100 nM) on the urothelial cell-mediated local bladder contractions. (c) Summarized data of the percentage of inhibition of the urothelial cell-mediated local bladder contractions by YM–254,890 (100 nM). (d) Representative recordings of the contractions evoked by 70 mM KCl and carbachol (3 µM) and ATP (50 µM). (e, f) Summarized data showing the inhibitory effects of YM–254,890 (100 nM) on the carbachol (3 µM) and ATP (50 µM)-evoked contractile responses. The amplitude of the urothelial cell-mediated local bladder contractions was expressed as a percentage of the 70 mM KCl-evoked contractions in the same preparation. Each point represents the mean ± SD of the mean (n = 6 for YM–254890 on the urothelial cell mediated contractions and n = 5 for YM–254890 on carbachol and ATP-evoked contractions). *Significantly different (p = 0.045) from the corresponding control values. Blue bars correspond to light stimulation. NS = non-significant (p = 0.860). Blue bars correspond to light stimulation
Effects of G-protein coupled receptor inhibitor YM-254,890 on the urothelial-cell mediated local bladder contractions
G-protein coupled receptor (GPCR) signaling is activated through various receptors (M3, P2Y, H1, PGE2, etc.), which are involved in the contractions of the detrusor smooth muscles11,12,13,14. Here we investigated whether GPCR signaling is important for producing the urothelial cell-mediated local bladder contractions. YM–254,890, is a broad-spectrum inhibitor for Gq and Gs proteins and shows a biased inhibition on Gi/o signaling15. YM–254,890 (1 µM) was shown to abolish histamine (200 µM), and carbachol (200 nM) evoked contractions in the mouse bladder, indicating the involvement of histamine and muscarinic receptors coupling to Gq/1113. In our study, YM–254,890 (100 nM) significantly inhibited the urothelial cell-mediated local bladder contractions (Fig. 4a and b). The amplitudes of the peak contractions before and after the application of YM–254,890 (100 nM) were 3.37 ± 0.74% and 2.09 ± 0.40% (n = 6) (Fig. 4b), respectively. The inhibitory percentage of the contractions by YM–254,890 (100 nM) was 33.89 ± 7.42% (n = 6) relative to control (vehicle) values (Fig. 4c). These results suggest that GPCR signaling pathways are involved in producing the urothelial cell-mediated local bladder contractions.
It has been reported that acetylcholine-evoked muscarinic contractions in the detrusor smooth muscle require signaling through Gq/11 proteins11. On the other hand, it is not yet clear whether ATP-evoked purinergic contractions also need GPCR signaling to induce mouse bladder contractions. Therefore, we further investigated to specify the inhibitory effects of YM–254,890 (100 nM) on the urothelial cell-mediated local bladder contractions, whether it is linked to muscarinic or purinergic signaling, using carbachol and ATP, respectively. YM–254,890 (100 nM) significantly inhibited carbachol (3 µM)-evoked contractions but not ATP (50 µM)-evoked contractions (Fig. 4d, e and f). The mean peak amplitudes of the carbachol (3 µM)-evoked contractions relative to 70 mM KCl-evoked contractions before and after the application of YM–254,890 (100 nM) were 132.03 ± 16.11% and 82.39 ± 10.19% (n = 5) (Fig. 4e), respectively. Whereas the mean peak amplitudes of the ATP (50 µM)-evoked contractions relative to 70 mM KCl-evoked contractions before and after the application of YM–254,890 (100 nM) were 66.35 ± 7.89% and 65.50 ± 10.03% (n = 5) (Fig. 4f), respectively. Our data indicates that GPCR signaling is essential for acetylcholine but not for ATP-evoked purinergic signaling pathways in mouse bladder. Taken together, these results suggest that inhibition of the urothelial cell-mediated local bladder contractions by YM–254,890 (100 nM) could be due to the inhibition of acetylcholine-evoked GPCR signaling or somewhere else in this pathway that results in acetylcholine related contractions.

Effects of nifedipine, an L-type Ca2+ inhibitor, on the urothelial cell-mediated local bladder contractions. (a) Representative recordings of the contractions evoked by 70 mM KCl and blue light (20 mW, 5 s). Blue light evoked urothelial cell-mediated local bladder contractions were recorded in the presence of vehicle and nifedipine (2 µM). (b) Summarized data showing the inhibitory effects of nifedipine (2 µM) on the urothelial cell-mediated local bladder contractions. (c) Summarized data of the percentage of inhibition of the urothelial cell-mediated local bladder contractions by nifedipine (2 µM). The amplitude of the urothelial cell-mediated local bladder contractions was expressed as a percentage of the 70 mM KCl-evoked contractions in the same preparation. Each point represents the mean ± SD of the mean (n = 5). *Significantly different (p = 0.016) from the corresponding control values. Blue bars correspond to light stimulation
Effects of voltage-gated calcium channel inhibitor Nifedipine on the urothelial cell-mediated local bladder contractions
Nifedipine has been shown to inhibit L-type Ca2+ channels, thereby reducing bladder strip contractions by interfering with extracellular Ca2+ influx into the cells16. Signaling events of smooth muscle contractions are involved with Ca2+ influx through the voltage-gated Ca2+ channels and partly by intracellularly released Ca2+1718. In this study, we sought to see whether voltage gated calcium channels are involved in the urothelial cell-mediated local bladder contractions. Nifedipine (2 µM) completely abolished the urothelial cell-mediated local bladder contractions (Fig. 5a, b and c). These results suggest that the urothelial cell-mediated local bladder contractions require signaling pathways which involve Ca2+ influx through voltage-dependent Ca2+ channels.

Effects of hemichannels inhibitor carbenoxolone (CBX) and exocytotic release inhibitor brefeldin A (BFA) on the urothelial cell-mediated local bladder contractions. (a and d) Representative recordings of the contractions evoked by 70 mM KCl and blue light (20 mW, 5 s). Blue light evoked urothelial cell-mediated local bladder contractions were recorded in the presence of vehicles and CBX (100 µM) and BFA (200 µM), respectively. (b and e) Summarized data showing the inhibitory effects of CBX (100 µM) and BFA (200 µM) on the urothelial cell-mediated local bladder contractions, respectively. (c and f) Summarized data of the percentage of inhibition of the urothelial cell-mediated local bladder contractions by CBX (100 µM) and BFA (200 µM), respectively. The amplitude of the urothelial cell-mediated local bladder contractions was expressed as a percentage of the 70 mM KCl-evoked contractions in the same preparation. Each point represents the mean ± SD of the mean (n = 6 for CBX; n = 5 for BFA). Significantly different (**p = 0.005, and *p = 0.020) from the corresponding control values. Blue bars correspond to light stimulation
Effects of hemichannels inhibitor Carbenoxolone disodium and exocytotic molecules release inhibitor Brefeldin a on the urothelial cell-mediated local bladder contractions
ATP can be released from urothelial cells by several mechanisms. The two main pathways are diffusion through hemichannels, and exocytosis19,20. We investigated whether these two important pathways are involved in releasing ATP or acetylcholine from the stimulation of the urothelial cells to produce the urothelial cell-mediated local bladder contractions. Here we used carbenoxolone disodium (CBX) and brefeldin A (BFA), which can block hemichannels and exocytosis pathways, respectively21,22.
CBX (100 µM) significantly inhibited the urothelial cell-mediated local bladder contractions (Fig. 6a and b). The mean peak contractions relative to 70 mM KCl-evoked contractions were 2.18 ± 0.28%, which was reduced to 1.54 ± 0.20% (n = 6) by the addition of CBX (100 µM) into the bath solutions (Fig. 6b). BFA (200 µM) also significantly inhibited the urothelial cell-mediated local bladder contractions (Fig. 6d and e). The peak amplitudes of contractions relative to 70 mM KCl-evoked contractions were 2.29 ± 0.36%, which was reduced to 1.44 ± 0.26% (n = 5) after the addition of BFA (200 µM) into the bath solutions (Fig. 6e). The percentage of inhibition by CBX (100 µM) and BFA (200 µM) were 33.89 ± 7.42% (n = 6) and 36.75 ± 6.20% (n = 5), respectively (Fig. 6c and f). These results suggest that both hemichannels and exocytosis pathways are involved in releasing transmitter molecules from the stimulation of the urothelial cells.
Discussion
The urothelial cells respond to sensory signals due to chemical and mechanical stimuli and release a variety of cell signaling molecules that are important for normal bladder function. We propose that these responses signal sensory neurons to convey mechanosensory information to the central nervous system. In the present study, we found that the urothelial cells, when optogenetically stimulated, can signal to non-neuronal cells to elicit bladder contractile activity (Summarized in Fig. 7).
Role of ATP in the urothelial cell-mediated local contractions
During the micturition cycle, stretching of the urothelium occurs, followed by the release of different signaling molecules such as ATP, ACh, nitric oxide, and substance P2. We first explored ATP and purinergic receptors because many different studies have suggested that ATP is the key molecule for the urothelial cell-mediated reflex bladder contractions3,23,24. Our data supports the findings of other studies demonstrating the importance of purinergic receptors in initiating the urothelial cell-mediated local bladder contractions (Fig. 3).
We showed that PPADS at a concentration of 2 mM almost completely abolished the urothelial cell-mediated local bladder contractions (Fig. 3a-c). The IC50 of PPADS for different P2X receptors varies from 1 ~ 50 µM and P2Y receptors from ~ 0.9 mM to 15 mM25,26. Therefore, while we don’t know the exact concentration at the receptor the 2 mM PPADS used in this study may have effects on P2Y receptors in addition to P2X. Additionally, the permeability of PPADS from the bladder bath solutions could influence its action. For instance, the application of atropine and ATP to the bath solution outside of the bladder did not inhibit the atropine-sensitive component of ATP-evoked contractions like as it did upon application within the bladder5. This finding suggests difficulty of the external absorption of these substances, which limits their effects from the external environment to the urothelium.
Role of acetylcholine (ach) in the urothelial cell-mediated local contractions
In ex vivo rat bladder preparation, it has been shown that muscarinic receptor inhibition by atropine significantly reduced the exogenous ATP-evoked contractions5. This result indicates that ATP may play a role in evoking cholinergic contractions of the bladder by influencing the release of ACh. In the present study, our data shows that muscarinic receptor inhibition with atropine significantly inhibited the urothelial cell-mediated local bladder contractions (Fig. 3). This result was similar to the previous finding by Stenquist et al. 2017 which suggested that atropine-sensitive components of the urothelial cell-mediated local bladder contractions could be due to the influence of the predominant initial release of ATP from the urothelial cells leading to the release of ACh which activates the muscarinic receptors on the detrusor muscle5. Additional research is necessary to determine if the urothelial release of ATP and its atropine-sensitive role in the urothelial cell-mediated local bladder contractions can be altered in cases of bladder disease.
Mechanisms of releasing transmitter signaling molecules from the urothelial cells
ATP is released from the urothelium by vesicular exocytosis and pannexin hemichannels in response to hydrostatic pressure or other stimulations4,27. In the present study, we provided direct evidence that the hemichannels inhibitor CBX significantly inhibited the urothelial cell-mediated local bladder contractions, indicating the involvement of hemichannels in releasing signaling molecules in response to local urothelial stimulation (Fig. 6a-c). However, CBX was also reported to inhibit voltage-gated Ca2+ channels in the retina28. We do not know how much the effects of CBX on voltage-gated Ca2+ channels in bladder smooth muscles and therefore, we cannot exclude the possibility that inhibition of urothelial cell-mediated local bladder contraction by CBX may be partially due to inhibition of voltage-gated Ca2+ channels in addition to inhibition of hemichannels. Furthermore, exocytosis inhibitor BFA also caused significant inhibition of the urothelial cell-mediated local bladder contractions, suggesting exocytosis pathways are also involved (Fig. 6d-f). Unfortunately, with this data, we cannot specify the independent mechanisms for releasing ATP and ACh from the urothelium. Future studies are also needed to explore if there are any changes in the pathways that release transmitter molecules in response to urothelial stimulation in bladder diseases, as this has been hypothesized to be a critical component of diseases such as interstitial cystitis/bladder pain syndrome29.
Involvement of G-protein receptor signaling in urothelial cell-mediated local contractions
We observed that urothelial cell-mediated local bladder contractions were significantly inhibited by a non-selective G-proteins inhibitor YM–254,890 (Fig. 4). Bladder contractions induced by muscarinic receptors are mediated via activation of Gq/11 proteins11. Jones et al., 2022 showed that YM–254,890 (1 µM) abolished carbachol (200 nM) evoked bladder strips contractions13. However, in our study, Y– 254,890 (200 nM) was not abolished but significantly reduced the carbachol (3 µM)-induced contractions. This difference may be due to the relatively lower dose (1 µM vs. 200 nM; 5 times lower) of YM–254,890 we used to inhibit the higher dose (200 nM vs. 3 µM; 5 times higher) of carbachol-evoked bladder contractions. Concentration-dependent inhibition of YM–254,890 was also observed for the inhibition of GTPγS binding to Gq30. Furthermore, we found no significant inhibition of ATP-evoked bladder contractions by YM–254,890. It has been proposed that ATP receptors in the bladder belong to two families: a P2X ion channel family and a P2Y G protein-coupled receptor family31. Bladder contractions are mediated predominantly via P2X receptors, while P2Y receptors mediate relaxation, which may be the possible reason for not inhibiting the ATP-evoked bladder contractions by YM–254,89032.
Calcium signaling events in producing the urothelial cell-mediated local contractions
An increase in intracellular cytoplastic Ca2+ concentration is fundamental to activate the contractile machinery either by Ca2+ influx or release of stored calcium from the intracellular sarcoplasmic reticulum33,34,35. In our present study, the urothelial cell-mediated local bladder contractions were abolished with calcium influx inhibitor nifedipine (Fig. 5). Therefore, our data suggests that the urothelial cell-mediated local bladder contractions primarily depend on signaling pathways, which lead to an increase in intracellular Ca2+ levels through Ca2+ influx via voltage-dependent Ca2+ channels from extracellular stores.
Our study showed that activation of ChR2 with 20 mW blue light produces much lower contractions compared to 70 mM KCl-evoked contractions. Increasing the intensities of light increased the urothelial cell-mediated local bladder contractions, which indicates possible activation of more ChR23. However, 70 mM KCl induces robust contraction via direct depolarization of smooth muscles36. The lower magnitude contraction with activation of ChR2 is due to the urothelial cells releasing signaling molecules, which lead to downstream signaling pathways that evoke smooth muscle contraction. These urothelial-released signaling molecules are unable to depolarize and activate as much smooth muscle as adding KCl to the solution.
Study limitations
In our study, we were unable to induce light-evoked distinguishable urothelial cell-mediated local bladder contractions from the mouse bladder strips (data not shown) and we were only able to evoke local contractions in the whole bladder preparations. This might be due to the decreased number of the urothelial cells in bladder strips, and their collective activation was not sufficient to produce a contraction. We also need to consider any potential damage to the urothelial cell layers and signaling potential when the bladder is cut into strips. With the whole bladder preparation, there is a sufficient population of cells available to activate the local contractions signaling pathway.
We showed that the urothelial cell-mediated local bladder contractions occur due to the release of ATP and ACh by activating ChR2 expressed into the urothelium (Fig. 3). We know that ChR2 activation can depolarize the cell and release ATP, similar to the activation of endogenous channels3. However, ChR2 is not normally expressed in the urothelial cells. However, there are other non-selective cation channels expressed in the urothelium, including for example P2 × 2, TRPV4, and Piezo1 channels37. ChR2 allows both monovalent (Na+, H+) and divalent (Ca2+, Mg2+) ions38which is similar to the selectivity of P2 × 2 and TRPV4394041. However, ChR2 is likely expressed at higher levels compared to TRPV4, P2 × 2, and Peizo1 in this model, which is regulated by the strong CAG promoter7. Further, there are potential differences in conductance and downstream signaling from these example non-selective cation channels, as well as many others that are expressed in the urothelium. The differences between exogenous ChR2 and endogenous non-selective cation channel activation need to be considered when interpreting these results. Future studies could utilize newly engineered opsins that can mimic endogenous receptor activity, thereby linking opsin activity to specific endogenous downstream intracellular signaling cascades42.
Conclusion
In conclusion, we have demonstrated that optogenetic stimulation of the urothelial cells can produce the urothelial cell-mediated local bladder contractions. This validates the previous hypothesis that the urothelial release factors can influence bladder contractions locally, without the need for signaling from the central nervous system. Further studies are needed to determine the relevance of these local signaling pathways in normal bladder physiology and pathophysiologic conditions.

An outline of the predictive signaling events activated by stimulation of the urothelial cells leading to the urothelial cell-mediated local bladder contractions. (1) The urothelial cell stimulation causes the release of ATP. Then the released ATP activates the purinergic signaling components on the detrusor smooth muscles. (2) The released ATP also acts as a mediator of releasing ACh from the urothelium. The released ACh then activates the muscarinic signaling events on the detrusor smooth muscles. (3) G-protein coupled receptors (GPCR) are involved in producing the urothelial cell-mediated local bladder contractions and it is related to the ACh activation of muscarinic receptors which thereafter activates the GPCR signaling to produce depolarization and contractions. (4) The urothelial cell-mediated local bladder contractions signaling eventually causes the opening of voltage dependent Ca2+ channels to influx extracellular calcium into the cells. (5) Stimulation of the urothelial cells releases ATP and ACh by means of exocytosis and hemichannels
Data availability
The data supporting this study’s findings are available to the corresponding author upon reasonable request.
References
Dalghi, M. G., Montalbetti, N., Carattino, M. D. & Apodaca, G. The urothelium: life in a liquid environment. Physiol. Rev. 100 (4), 1621–1705 (2020).
Winder, M., Tobin, G., Zupančič, D. & Romih, R. Signalling molecules in the urothelium. BioMed. Res. Int. 2014, 297295 (2014).
Robilotto, G. L., Yang, O. J., Alom, F., Johnson, R. D. & Mickle, A. D. Optogenetic urothelial cell stimulation induces bladder contractions and pelvic nerve afferent firing. Am. J. Physiol-Ren Physiol. Am. Physiological Soc. 325 (2), F150–F163 (2023).
Sui, G. et al. Purinergic and muscarinic modulation of ATP release from the urothelium and its paracrine actions. Am. J. Physiol. - Ren. Physiol. 306 (3), F286–F298 (2014).
Stenqvist, J., Winder, M., Carlsson, T., Aronsson, P. & Tobin, G. Urothelial acetylcholine involvement in ATP-induced contractile responses of the rat urinary bladder. Eur. J. Pharmacol. 809, 253–260 (2017).
de la Ayala, F. et al. Loss of p53 and acquisition of angiogenic MicroRNA profile are insufficient to facilitate progression of bladder urothelial carcinoma in situ to invasive carcinoma. J. Biol. Chem. 286 (23), 20778–20787 (2011).
Madisen, L. et al. A toolbox of Cre-dependent optogenetic Transgenic mice for light-induced activation and Silencing. Nat. Neurosci. 15 (5), 793–802 (2012).
Alom, F. et al. Involvement of transient receptor potential melastatin 4 channels in the resting membrane potential setting and cholinergic contractile responses in mouse detrusor and ileal smooth muscles. J. Vet. Med. Sci. 81 (2), 217–228 (2019).
Guan, Y. F. et al. Hypertonic and isotonic potassium solutions have different effects on vessel contractility resulting in differences in optimal resting tension in rat aorta. Acta Pharmacol. Sin. 28 (5), 643–650 (2007).
Andersson, K. E. Purinergic signalling in the urinary bladder. Auton. Neurosci. 191, 78–81 (2015).
An, J. Y. et al. The intracellular pathway of the acetylcholine-induced contraction in Cat detrusor muscle cells. Br. J. Pharmacol. 137 (7), 1001–1010 (2002).
Maynard, J. P. & Sfanos, K. S. P2 purinergic receptor dysregulation in urologic disease. Purinergic Signal. 18 (3), 267–287 (2022).
Jones, B. M., Mingin, G. C. & Tykocki, N. R. Histamine receptors rapidly desensitize without altering nerve-evoked contractions in murine urinary bladder smooth muscle. Am. J. Physiol-Ren Physiol. Am. Physiological Soc. 322 (3), F268–F279 (2022).
Hou, R., Yu, Y. & Jiang, J. PGE2 receptors in detrusor muscle: drugging the undruggable for urgency. Biochem. Pharmacol. 184, 114363 (2021).
Peng, Q., Alqahtani, S., Nasrullah, M. Z. A. & Shen, J. Functional evidence for biased Inhibition of G protein signaling by YM-254890 in human coronary artery endothelial cells. Eur. J. Pharmacol. 891, 173706 (2021).
Maggi, C. A. et al. The effect of Nifedipine on spontaneous, drug-induced and reflexly-activated contractions of the rat urinary bladder: evidence for the participation of an intracellular calcium store to micturition contraction. Gen. Pharmacol. Vasc Syst. 19 (1), 73–81 (1988).
Alom, F. et al. Possible antagonistic effects of the TRPC4 channel blocker ML204 on M2 and M3 muscarinic receptors in mouse ileal and detrusor smooth muscles and atrial myocardium. J. Vet. Med. Sci. 80 (9), 1407–1415 (2018).
Phelps, C., Chess-Williams, R. & Moro, C. The role of intracellular calcium and Rho kinase pathways in G protein-coupled receptor-mediated contractions of urinary bladder urothelium and lamina propria. Am. J. Physiol-Cell Physiol. Am. Physiological Soc. 324 (3), C787–C797 (2023).
Burnstock, G. & Verkhratsky, A. Mechanisms of ATP Release and Inactivation. In: Burnstock G, Verkhratsky A, editors. Purinergic Signal Nerv Syst [Internet]. Berlin, Heidelberg: Springer; [cited 2024 Aug 8]. pp. 79–118. (2012). Available from: https://doi.org/10.1007/978-3-642-28863-0_4
Nakagomi, H. et al. Urothelial ATP exocytosis: regulation of bladder compliance in the urine storage phase. Sci. Rep. Nat. Publishing Group. 6 (1), 29761 (2016).
Ye, Z. C., Oberheim, N., Kettenmann, H. & Ransom, B. R. Pharmacological cross-inhibition of connexin hemichannels and swelling activated anion channels. Glia 57 (3), 258–269 (2009).
Joseph, E. K., Green, P. G. & Levine, J. D. ATP release mechanisms of endothelial Cell–Mediated Stimulus-Dependent hyperalgesia. J. Pain. 15 (7), 771–777 (2014).
Stenqvist, J., Aronsson, P., Carlsson, T., Winder, M. & Tobin, G. In vivo paracrine effects of ATP-induced urothelial acetylcholine in the rat urinary bladder. Auton. Neurosci. Basic. Clin. 227, 102689 (2020).
Ferguson, D. R., Kennedy, I. & Burton, T. J. ATP is released from rabbit urinary bladder epithelial cells by hydrostatic pressure changes–a possible sensory mechanism? J. Physiol. 505 (Pt 2), 503–511 (1997).
Huo, H., Fryatt, A. G., Farmer, L. K., Schmid, R. & Evans, R. J. Mapping the binding site of the P2X receptor antagonist PPADS reveals the importance of orthosteric site charge and the cysteine-rich head region. J. Biol. Chem. 293 (33), 12820–12831 (2018).
Rost, S. et al. P2 receptor antagonist PPADS inhibits mesangial cell proliferation in experimental mesangial proliferative glomerulonephritis. Kidney Int. 62 (5), 1659–1671 (2002).
Wang, E. C. Y. et al. ATP and purinergic receptor–dependent membrane traffic in bladder umbrella cells. J. Clin. Invest. 115 (9), 2412–2422 (2005).
Vessey, J. P. et al. Carbenoxolone Inhibition of Voltage-Gated Ca channels and synaptic transmission in the retina. J. Neurophysiol. Am. Physiological Soc. 92 (2), 1252–1256 (2004).
Sun, Y. & Chai, T. C. Augmented extracellular ATP signaling in bladder urothelial cells from patients with interstitial cystitis. Am. J. Physiol. Cell. Physiol. 290 (1), C27–34 (2006).
Nishimura, A. et al. Structural basis for the specific inhibition of heterotrimeric Gq protein by a small molecule. Proc Natl Acad Sci. Proceedings of the National Academy of Sciences; ;107(31):13666–13671. (2010).
Burnstock, G. Purinergic signalling in the urinary tract in health and disease. Purinergic Signal. 10 (1), 103–155 (2014).
Aronsson, P., Andersson, M., Ericsson, T. & Giglio, D. Assessment and characterization of purinergic contractions and relaxations in the rat urinary bladder. Basic. Clin. Pharmacol. Toxicol. 107 (1), 603–613 (2010).
Kohda, M., Komori, S., Unno, T. & Ohashi, H. Carbachol-induced oscillations in membrane potential and [Ca2+]i in guinea-pig ileal smooth muscle cells. J. Physiol. 511 (2), 559–571 (1998).
Komori, S., Kawai, M., Pacaud, P., Ohashi, H. & Bolton, T. B. Oscillations of receptor-operated cationic current and internal calcium in single guinea-pig ileal smooth muscle cells. Pflüg Arch. 424 (5), 431–438 (1993).
Unno, T. et al. M2 and M3 muscarinic receptor-mediated contractions in longitudinal smooth muscle of the ileum studied with receptor knockout mice. Br. J. Pharmacol. 146 (1), 98–108 (2005).
Kirschstein, T. et al. High K+-induced contraction requires depolarization-induced Ca2+ release from internal stores in rat gut smooth muscle. Acta Pharmacol. Sin. 30 (8), 1123–1131 (2009).
Tempest, H. V. et al. P2X2 and P2X3 receptor expression in human bladder urothelium and changes in interstitial cystitis. BJU Int. 93 (9), 1344–1348 (2004).
Schneider, F., Gradmann, D. & Hegemann, P. Ion selectivity and competition in Channelrhodopsins. Biophys. J. 105 (1), 91–100 (2013).
North, R. A. Molecular physiology of P2X receptors. Physiol. Rev. Am. Physiological Soc. 82 (4), 1013–1067 (2002).
Voets, T. et al. Molecular determinants of permeation through the cation channel TRPV4*. J. Biol. Chem. 277 (37), 33704–33710 (2002).
Watanabe, H. et al. Modulation of TRPV4 gating by intra- and extracellular Ca2+. Cell. Calcium. 33 (5), 489–495 (2003).
Emiliani, V. et al. Optogenetics for light control of biological systems. Nat. Rev. Methods Primer Nat. Publishing Group. 2 (1), 1–25 (2022).
Acknowledgements
This study was supported by the Rita Allen Foundation Scholars Program Fund, Community Foundation of New Jersey and R01DK140233 (to A.D.M.); and 2022 Urology Care Foundation Research Scholar Award Program and Indian American Urological Association Sakti Das, MD Awards (to F.A.).
Author information
Authors and Affiliations
Contributions
F.A and A.D.M contributed to the conception and design of the study. F.A, K.J.R and B.T contributed to collecting and analyzing the data. F.A designed the figures and wrote the draft of the manuscript. A.D.M supervised the experiments, collected funds, interpreted the results, edited and reviewed the manuscript. F.A., K.J.R, B.T and A.D.M approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Alom, F., Ratcliff, K.J., Talluri, B. et al. Contractions of ex-vivo mouse bladder driven by activation of channelrhodopsin-2 expressed in urothelial cells. Sci Rep 15, 34617 (2025). https://doi.org/10.1038/s41598-025-18216-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-18216-2
