
Abstract
There is limited data on high-intensity statin for secondary prevention in elderly acute myocardial infarction (AMI) patients above 75 years. This study aimed to assess the impact of high-intensity statin on 3-year outcomes in elderly AMI patients (> 75 years) who underwent percutaneous coronary intervention (PCI) with drug-eluting stents (DES). From the Korea AMI registry (KAMIR)-National Institutes of Health (NIH), 2,063 elderly patients were divided into three groups based on statin therapy at discharge: high-intensity statin group (n = 521), low/moderate-intensity statin group (n = 1,419), and no statin group (n = 123). The primary endpoint was the 3-year composite of cardiac death and recurrent myocardial infarction (MI). The high-intensity statin group had a similar primary endpoint incidence compared to the low/moderate-intensity statin group (11.5% vs. 12.5%; aHR: 1.053; 95% CI: 0.780–1.423; P = 0.739), but a significantly lower incidence compared to the no statin group (11.5% vs. 22.0%; aHR: 2.433; 95% CI: 1.377–4.298; P = 0.002). Major adverse cardiac events were lower in the high-intensity statin group compared to the no statin group but similar to the low/moderate-intensity statin group. High-intensity statin significantly reduced 3-year outcomes in elderly AMI patients after PCI compared to no statin, with similar benefits to low/moderate-intensity statin.
Similar content being viewed by others
Introduction
It is well established that high-intensity statin therapy plays an important role in reducing the risk of fatal and nonfatal cardiovascular events after acute myocardial infarction (AMI)1,2,3,4. The current guidelines recommend that in all AMI patients with no contraindications, high-intensity statin therapy should be started or continued as early as possible, regardless of the initial levels of low-density lipoprotein (LDL)-cholesterol (LDL-C)5,6. However, the role of high-intensity statin therapy for secondary prevention in elderly patients (> 75 years old) remains a subject of debate, even within established guidelines and substantial trials5,6,7,8. The recent guidelines recommend that older patients should receive maximal tolerated statin therapy similar to younger patients, with the European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) advocating this6but it does not provide specific recommendations for patients aged over 75 years. The American College of Cardiology (ACC)/American Heart Association (AHA) suggesting a preference for moderate-intensity statin in those over 75 years old with atherosclerotic cardiovascular disease (ASCVD), considering the decision based on potential benefits versus concurrent comorbidities5.
The elderly population is growing in proportion within society, accompanied by a substantial increase in patients with myocardial infarction (MI) > 75 years of age9. Therefore, the role of statin therapy in secondary prevention after AMI might be particularly important for elderly patients (> 75 years), particularly in current generation drug-eluting stents (DES) era. However, it is crucial to note that the safety and potential drawbacks of statins warrant special attention in the elderly patients due to factors such as comorbidities, polypharmacy, and changes in pharmacokinetics and pharmacodynamics10. Moreover, the lack of data on high-intensity statin therapy in elderly patients is primarily due to their common exclusion in randomized controlled or large-scaled trials.
Therefore, the aim of this study was to investigate the impact of high-intensity statin therapy on 3-year clinical outcomes in elderly AMI patients (> 75 years) underwent successful percutaneous coronary intervention (PCI) with DES in comparison to low/moderate-intensity statin therapy as well as no statin therapy.
Results
The baseline clinical characteristics of the patients are shown in Table 1. There were no significant differences in gender and age distribution among the three groups. The left ventricular ejection fraction (LVEF) was significantly lower in the no statin group compared to the other two groups (51.7 ± 10.7% versus 50.5 ± 11.4% versus 46.6 ± 11.0%, P < 0.001). There were no significant differences among the three groups in terms of the incidence of STEMI at initial diagnosis and the distribution of risk factors. The high-intensity statin group exhibited significantly elevated levels of total cholesterol (178 ± 42 mg/dL versus 167 ± 41 mg/dL versus 151 ± 38 mg/dL, P < 0.001), triglyceride (114 ± 82 mg/dL versus 102 ± 79 mg/dL versus 98 ± 60 mg/dL, P < 0.001), high-density lipoprotein (HDL) cholesterol (HDL-C) (44 ± 11 mg/dL versus 43 ± 12 mg/dL versus 41 ± 12 mg/dL, P = 0.023), and LDL-C (114 ± 38 mg/dL versus 104 ± 36 mg/dL versus 83 ± 29 mg/dL, P < 0.001) compared to the other two groups. The serum glucose level was highest in the no statin group (164 ± 75 mg/dL versus 168 ± 80 mg/dL versus 186 ± 81 mg/dL, P = 0.041).
The angiographic and procedural characteristics and medications at discharge are presented in Table 2. The use of Biolimus A9-eluting stents was highest within the low/moderate-intensity statin group (15.1% versus 20.7% versus 17.0%, P = 0.017), whereas the use of Sirolimus-eluting stents was most prevalent in the high-intensity statin group (7.1% versus 2.5% versus 2.4%, P < 0.001). However, there were no significant differences observed among the three groups in terms of other angiographic and procedural characteristics. Among the discharge medications, the high-intensity statin group exhibited a higher prevalence of prescribing ticagrelor (19.1% versus 16.5% versus 5.6%, P = 0.001), angiotensin II type I receptor blockers (ARB) (40.3% versus 33.2% versus 26.8%, P = 0.003), atorvastatin (61.0% versus 50.1% versus 0.0%, P < 0.001), and rosuvastatin (38.9% versus 31.6% versus 0.0%, P < 0.001) in comparison to the other two groups. In the low/moderate-intensity statin group, the frequency of using cilostazol (5.5% versus 13.8% versus 7.3%, P < 0.001), beta-blockers (BB) (81.5% versus 84.0% versus 66.6%, P < 0.001), and angiotensin-converting enzyme inhibitors (ACEI) (38.1% versus 47.9% versus 42.2%, P < 0.001) was higher compared to the other two groups. Simvastatin, pitavastatin, fluvastatin, and pravastatin were prescribed within the low/moderate-intensity statin group. There was a greater use of clopidogrel within the no statin group when contrasted with the other two groups (78.5% versus 81.6% versus 91.0%, P = 0.005). Additionally, oral anticoagulants were prescribed at discharge in 3.1%, 3.6%, and 2.4% of patients in the high-intensity, low/moderate-intensity, and no statin groups, respectively (P = 0.711). Triple antithrombotic therapy (TAT), including an oral anticoagulant, was used in 5.9%, 13.7%, and 5.7% of the three groups, respectively (P < 0.001).
Tables 3 and 4 show the cumulative incidences of major clinical outcomes according to statin treatment during the 3-year follow-up. After adjustment, the cumulative incidences of primary endpoint in the high-intensity statin group were lower compared to the no statin group (11.5% versus 22.0%; adjusted hazard ratio [aHR]: 2.432; 95% confidence interval [CI]: 1.377–4.297; P = 0.002), but were similar to those in the low/moderate-intensity statin group (11.5% versus 12.5%; aHR: 1.052; 95% CI: 0.779–1.421; P = 0.739) (Tables 3 and 4; Fig. 1A, and Fig. 1B). Similarly, the cumulative incidences of major adverse cardiac events (MACE) (aHR: 2.668; 95% CI: 1.735–4.104; P < 0.001), target lesion failure (TLF) (aHR: 3.270; 95% CI: 1.842–5.804; P < 0.001), target vessel failure (TVF) (aHR: 2.722; 95% CI: 1.625–4.561; P < 0.001), and procedure free cardiac events (PFCE) (aHR: 3.027; 95% CI: 1.986–4.614; P < 0.001) in the high-intensity statin group were lower compared to the no statin group, but were similar to those in the low/moderate-intensity statin group (Tables 3 and 4). In addition, the cumulative incidences of total death (aHR: 3.122; 95% CI: 1.903–5.120; P < 0.001), cardiac death (aHR: 3.325; 95% CI: 1.798–6.149; P < 0.001), and re-hospitalization due to heart failure (HF) (aHR: 4.006; 95% CI: 1.885–8.513; P < 0.001) in the high-intensity statin group were lower compared to the no statin group, showing similarity to those in the low/moderate-intensity statin group (Tables 3 and 4). The incidence of hemorrhagic stroke was low across all groups and showed no statistically significant difference between the high-intensity, low/moderate-intensity, and no statin groups (0.4% vs. 0.8% vs. 0.8%, respectively; P = 0.566) (Table 3).

The cumulative incidences of primary endpoint (cardiac death or myocardial infarction) according to statin treatment, (A) using Kaplan-Meier analyses in crude population, (B) using adjusted Cox proportional hazards regression model. KM, Kaplan-Meier; MI, myocardial infarction; aHR, adjusted hazard ratio; CI, confidence interval.
Serial LDL-C levels during the 3-year follow-up are shown in Supplementary Fig. 1. At 1 year, mean LDL-C levels were lowest in the high-intensity statin group (70.2 mg/dL), followed by the low/moderate-intensity (73.4 mg/dL) and no statin groups (86.8 mg/dL). This trend remained consistent throughout the 3-year follow-up, with a marked increase in LDL-C levels in the no statin group by 3-year follow-up (92.2 mg/dL). Figure 2 shows the change of statin intensity during the 3-year follow-up period after AMI in real-world practice. Analyzing the changes in statin intensity over the 3-year follow-up period, it was observed that patients initially discharged with high-intensity statin had 37.6% of them switched to low/moderate-intensity statin after 1-year follow-up. Among patients initially on low/moderate-intensity statin, only 7.7% transitioned to high-intensity statin over the same period. Additionally, among patients not prescribed statins at discharge, 38.2% were shifted to low/moderate-intensity statin after 1-year follow-up. These trends have remained consistent during the 1- to 3-year follow-up. Incorporating landmark analysis that accounted for the intensity of statin use throughout the follow-up period, the results of primary endpoint remained consistent when considering the period from immediate post-PCI to 1 year post-PCI, as well as the period from 1 year post-PCI to 3 years post-PCI (Fig. 3A and B). Furthermore, we conducted an additional subgroup analysis to evaluate the impact of statin intensity changes on clinical outcomes, particularly the incidence of cardiac death or myocardial infarction. Patients who continuously maintained high-intensity statin therapy showed the most favorable outcomes, while those who remained on or switched to low-intensity statins had significantly higher event rates (Supplementary Fig. 2).

Sankey diagram showing changes in statin prescription rates over 3 years among elderly patients (> 75 years) after myocardial infarction. Statin use at each time point reflects the prescribed intensity at the time of clinical follow-up visit.

The cumulative incidences of primary endpoint (cardiac death or myocardial infarction) according to statin treatment based on the land-mark analysis, (A) using Kaplan-Meier analyses in crude population, (B) using adjusted Cox proportional hazards regression model. KM, Kaplan-Meier; MI, myocardial infarction; aHR, adjusted hazard ratio; CI, confidence interval.
Discussion
The main findings of this study are: (1) in high-intensity statin therapy, the cumulative incidences of primary endpoint (composite of cardiac death and MI), MACE, TLF, TVF, PFCE, total death, cardiac death, and re-hospitalization due to HF were lower than those in the no statin therapy; (2) the cumulative incidences of primary endpoint, MACE, TLF, TVF, PFCE, total death, cardiac death, and re-hospitalization due to HF were similar between the high-intensity statin therapy and low/moderate-intensity statin therapy in elderly AMI patients (> 75 years) who underwent successful PCI with DES over a 3-year follow-up.
Based on demographic predictions, individuals older than 75 years of age will account for more than 10% of the total population by 2050, and this age group experiences a cardiovascular mortality rate nearly three times higher than that of the younger population11,12. A comprehensive geriatric evaluation is essential for assessing cardiovascular risk in elderly patients, encompassing evaluations of functional capacity, multimorbidity, polypharmacy, frailty, cognitive function, and mental health13. As a result, physicians are required to engage in shared decision-making that takes into consideration potential benefits and risks.
Statins have been proven to reduce major cardiovascular events in patients with ASCVD, and the first-line drugs for secondary prevention after AMI14. However, there is a lack of compelling evidence regarding the efficacy and safety of statin use and intensity in elderly patients, and they have been historically underrepresented in clinical trials. In the Heart Protection Study (HPS) trial, patients aged 70–80 were included, demonstrating that simvastatin resulted in an 18% reduction in the rate of MACE compared to a placebo15. A previous systematic review that included patients aged 65 years and older from 23 trials showed significant reductions in all-cause mortality (relative risk [RR]: 0.80; 95% CI: 0.73–0.89), cardiovascular mortality (RR: 0.68; 95% CI: 0.58–0.79), and MACE (RR: 0.68; 95% CI: 0.61–0.77) among patients with ASCVD on statin therapy16. Nonetheless, these investigations had heterogenous study populations and have not provided evidence regarding the effectiveness and safety of statin use for secondary prevention in elderly patients when considering different levels of intensity. While the most recent trial involving AMI patients who underwent PCI showed no statistically significant difference in adverse clinical event rates between high- and low/moderate-intensity statin groups in elderly patients (11.4% vs. 10.6%, aHR: 1.1; 95% CI: 0.76–1.59; P = 0.63)17, it is important to acknowledge that this study had limitations, including a relatively short follow-up duration of just 1 year and the exclusion of patients who were not prescribed statins. In addition, several ongoing randomized controlled trials (RCTs), such as the PREVENTABLE (NCT04262206) and STAREE (NCT02099123) trials, are currently investigating whether statin therapy can improve outcomes in older adults, including cognitive function and cardiovascular risk. These studies aim to provide further insight into optimal LDL-C targets and the risk-benefit balance of statin use in the elderly population. The results of these trials are expected to help clarify whether intensive lipid lowering offers meaningful benefits in this age group.
Our study constituted a long-term observational investigation spanning 3 years, targeting a relatively unique and homogeneous group of AMI patients-those aged 75 and above who have treated by PCI with current generation DES. The results of this study demonstrated that high-intensity statin therapy was effective for secondary prevention in elderly patients, as compared to no statin treatment. Furthermore, our results indicated similarities in efficacy and safety between the high-intensity statins and low/moderate-intensity statins. In particular, the incidence of hemorrhagic stroke was low and comparable across all groups (0.4% vs. 0.8% vs. 0.8%, P = 0.566), indicating no increased risk with high-intensity statin use in this elderly population (Table 3). These outcomes remained consistent when conducting a landmark analysis at both the 1-year and 3-year post-PCI intervals. In the context of secondary prevention of cardiovascular events, there exists a lack of substantial evidence supporting the aggressive cholesterol lowering treatment among the elderly patients. Factors like medication side-effects, comorbidities, and poor compliance often contribute to a more conservative approach in prescribing statins in these patients. However, this study is noteworthy as 89.3% of patients in the statin-at-discharge group adhered to statin therapy for 3 years (Fig. 2). The significance lies in the fact that these patients exhibited remarkable improvements in clinical outcomes compared to the no statin group, and these results are in agreement with the findings of a recent comprehensive meta-analysis18. Therefore, it is important to recognize that despite their shorter life expectancy relative to younger patients, advanced age should not be used as a determinant for applying less intensive statin treatment strategy. In addition to, the similarity in outcomes between high-intensity statin therapy and low/moderate-intensity statin therapy in this study might be attributed to a lower efficacy of high-intensity statins in elderly patients, which could result from reduced endogenous cholesterol synthesis and increased cholesterol absorption in these population19. Moreover, the fact that around half of the patients shifted from high-intensity to low-intensity statin therapy in the real-world context, as demonstrated in this study, could serve as another contributing factor. This transition can be attributed to various reasons such as changes in health conditions, renal impairment, drug interactions, side effects, and poor compliance. Considering these findings, for elderly patients unable to tolerate high-intensity statins, it might be worth considering supplementary treatment options involving moderate statins, such as ezetimibe or Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) inhibitors20,21.
There are some limitations in this study. First, as this study was executed through a multicenter national prospective registry, substantial variations emerged in the baseline characteristics of the enrolled patients. Although the registry itself was prospective, the present analysis was performed retrospectively, and no formal statistical power or sample size calculation was conducted in advance. Nevertheless, we countered this by employing IPTW analysis to eliminate confounding factors, thus aiming to provide insights into outcomes that align with the real-world clinical practices among elderly AMI patients. However, as with any observational study using IPTW, the possibility of residual confounding due to unmeasured variables or model misspecification cannot be entirely excluded. As a result, these findings are expected to significantly aid in the refinement of management and prevention approaches for elderly patients with AMI. Second, the clinical impact of statin therapy according to intensity was compared based on the patients’ medications at discharge. While medication adherence was inferred from prescription records at each follow-up time point, detailed information on actual pill-taking behavior or pharmacy refill data was not available. Moreover, the specific reasons for not initiating statin therapy in some patients such as frailty, comorbidities, or physician preference were not captured in the registry, which may have introduced unmeasured confounding. In addition, the incidence of adverse events, including bleeding complications, as well as the and various causes of discontinuation or change in the intensity of statins were not available in this study. Although hemorrhagic stroke was analyzed, more detailed data on other bleeding events such as gastrointestinal or minor bleeding were not available, limiting a comprehensive safety assessment. Furthermore, well-known safety concerns of high-intensity statins in elderly patients—such as myopathy, liver enzyme elevation, and new-onset diabetes—could not be evaluated in this study due to limitations of the registry. These factors may have led to an underestimation of potential safety concerns and limited our ability to assess the true long-term adherence and tolerability of statin therapy in this population. The duration and rationale for dual antiplatelet therapy, particularly in the no statin group, were not collected. Similarly, the presence of atrial fibrillation or flutter and the indications for oral anticoagulant (OAC) use were not systematically documented, and the reasons for initiating triple antithrombotic therapy at discharge were not specified, which may have implications for interpreting bleeding risk and medication strategies in this population. Lastly, because this study population consisted exclusively of Korean patients belonging to a single race, the generalizability of our findings to patients from different racial and ethnic backgrounds remains limited. Further investigations encompassing diverse patient populations are warranted.
In conclusion, high-intensity statin therapy was associated with significantly reduced 3-year major adverse clinical outcomes than no statin therapy but similar efficacy was observed with low/moderate-intensity statin therapy in elderly patients (> 75 years) with AMI underwent PCI with DES. These results are expected to be more definitively established through further studies, especially among elderly AMI patients undergoing PCI with current generation DES with larger study population and multi-ethnicity to reflect current clinical practice in the future.
Methods
Study population
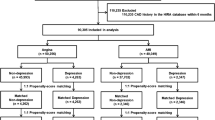
The study population was derived from the Korea AMI registry (KAMIR), a prospective, multicenter online registry established to reflect the real-world practices in treating Korean AMI patients since November 2005. The study design of the KAMIR has been previously outlined in several studies4,22with the details of the registry available on the KAMIR website (http://www.kamir.or.kr). Specifically, the KAMIR-national institute of health (NIH) registry subset was selectively analyzed to accurately represent the prevailing clinical practices for all Korean AMI patients and their current epidemiology and clinical outcomes. From November 2011 to December 2015, a total of 13,104 AMI patients were enrolled in the nationwide KAMIR-NIH registry. Out of 9829 patients who underwent successful PCI with second-generation DES, 7766 patients were aged 75 years or younger than 75 years. A total of 2063 elderly patients (> 75 years) were divided into three groups based on their statin treatment at discharge; the high-intensity statin group (n = 521), the low/moderate-intensity statin group (n = 1419), and the no statin group (n = 123). Because the Asian population often receives moderate-dose statin treatment due to lower average body weights, high-intensity statins were defined as atorvastatin (≥ 40 mg), rosuvastatin (≥ 20 mg), simvastatin (≥ 40 mg), pitavastatin (≥ 4 mg), and pravastatin (≥ 40 mg), while other statins were categorized as low/moderate-intensity statins23in comparison with the current guidelines24.
Data collection was consistently conducted using an identical web-based case report form across all participating centers. The study protocol adhered to the ethical principles outlined in the Declaration of Helsinki (1975) and was approved by the Institutional Review Board of Korea University Guro Hospital. As this was a multicenter registry-based study, each participating center obtained local institutional review board approval in accordance with national regulations. Prior to their inclusion, all patients provided written informed consent. During the study period, a total of 2063 patients completed a comprehensive 3-year clinical follow-up, which involved in-person-interviews at outpatient follow-up, telephone contact, or a thorough examination of medical records.
PCI procedure and medical treatment
Standardized techniques were employed for PCI procedures25. The initiation of PCI was carried out via either the femoral or radial artery, following the administration of a single dose of unfractionated heparin (70–100 U/kg). All patients were administered loading doses of aspirin (200–300 mg) and other antiplatelet agents such as clopidogrel, ticagrelor, or prasugrel before PCI. DES were deployed subsequent to balloon angioplasty with or without thrombus aspiration. The decision to employ anticoagulation therapy during PCI was at the discretion of the individual physician. Successful PCI was defined as achieving an angiographic residual stenosis of less than 10% without any MACE, in conjunction with a thrombolysis in MI (TIMI) blood flow grade 3. Dual antiplatelet therapy was sustained for a minimum of one year by the patients. During the in-hospital period, patients were prescribed medications such as BB, ACEI, ARB, calcium channel blockers (CCB), and statins. After discharge, patients were encouraged to maintain their hospital medication regimen if feasible, with the possibility of adjusting the type and dosage of medications based on the physician’s discretion.
Study definition and endpoint
The primary endpoint was defined as a composite of cardiac death and recurrent MI. The secondary endpoints included the occurrence of any clinical events such as total death, cardiac death, recurrent MI, any repeat revascularization including surgical coronary artery bypass graft (CABG) or repeat PCI, stroke, stent thrombosis, and re-hospitalization due to HF. MACE was defined as a composite of total death, recurrent MI, and any repeat revascularization. TLF was defined as a composite of cardiac death, ST-segment elevation myocardial infarction (STEMI), and target lesion revascularization (TLR). TVF was defined as a composite of cardiac death, recurrent MI, and target vessel revascularization (TVR). PFCE was defined as a composite of cardiac death, recurrent MI, and re-hospitalization due to HF. Total death was considered cardiac in origin, unless a non-cardiac origin was definitely documented. Recurrent MI was defined as recurrent symptoms with new ST-segment elevation or re-elevation of cardiac markers to at least twice the upper limit of normal. TLR was defined as repeat PCI within the index procedure stent or 5 mm edge. TVR was defined as any repeat PCI or surgical CABG involving any segment within the target vessel. Any repeat revascularization was defined as any repeat PCI or CABG of the target vessel or the non-target vessel. All participants were obligated to visit the outpatient cardiology department after one-month post-PCI, and subsequently every six months, as well as whenever angina-like symptoms occurred.
Statistical analysis
The normality test was carried out through the Kolmogorov-Smirnov test. Continuous variables were assessed for differences among the three groups using either analysis of the one-way ANOVA or Kruskal-Wallis test. Data were presented as mean ± standard deviations. Discrete variables were reported as numbers and percentages and were subjected to comparison using either the chi-square test or Fisher’s exact test, as deemed appropriate. To adjust for any potential confounders, an inverse probability of treatment weighting (IPTW) analysis was performed. We utilized generalized boosted models to estimate the propensity score weight of each treatment using methods developed for comparison of multiple treatments. The average treatment effect on the population weights was estimated using the multinomial propensity scores (MNPS) function in the Twang package (http://www.rand.org/statistics/twang/downloads.html/mnps_turorial_code.r.) in R Statistical Software (R Foundation for Statistical Computing, Vienna, Austria). We tested all available variables that could be of potential relevance: age, sex (male), LVEF, cardiovascular risk factors (e.g., hypertension, diabetes, dyslipidemia, stroke), co-medication treatment (aspirin, other antiplatelets, CCB, BB, ACEI, and ARB), angiographic and procedural characteristics (e.g., target vessel, number of diseased vessels, and DES type). Various clinical outcomes for up to 3 years are estimated by Cox-proportional hazards models analysis. Binary logistic regression analysis was used to assess the HR of the use of high-intensity statin group compared to the use of low/moderate-intensity statin group and the no statin group. The Kaplan-Meier analysis was employed to estimate various clinical outcomes for a period of 3 years, while differences between the groups were evaluated using the log-rank test. In all analyses, a p value less than 0.05 in two-sided tests was considered as indicating statistical significance. All data analysis was conducted using SPSS software (version 24.0, SPSS-PC, Inc., Chicago, Illinois) and R statistical software.
Data availability
The data that support the findings of this study are available from the Korea Acute Myocardial Infarction Registry (KAMIR)-National Institutes of Health (NIH), but restrictions apply to the availability of these data, which were used under license for the current study and are therefore not publicly available. The data presented in this study are available on request from the corresponding author.
References
Cannon, C. P. et al. Intensive versus moderate lipid Lowering with Statins after acute coronary syndromes. N Engl. J. Med. 351, 714–717 (2004).
Kim, Y. H. et al. Two-year outcomes of Statin therapy in patients with acute myocardial infarction with or without dyslipidemia after percutaneous coronary intervention in the era of new-generation drug-eluting stents within Korean population: data from the Korea acute myocardial infarction registry. Catheter Cardiovasc. Interv. 93, 1264–1275 (2019).
Desjobert, E. et al. Clinical outcomes with high-intensity Statins according to atherothrombotic risk stratification after acute myocardial infarction: the FAST-MI registries. Arch. Cardiovasc. Dis. 114, 88–95 (2021).
Kim, Y. H. et al. Comparative effect of Statin intensity between prediabetes and type 2 diabetes mellitus after implanting newer-generation drug-eluting stents in Korean acute myocardial infarction patients: a retrospective observational study. BMC Cardiovasc. Disord. 21, 386 (2021).
Grundy, S. M. et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 139, e1082–e1143 (2018).
Mach, F. et al. 2019 ESC/EAS guidelines for t he management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur. Heart J. 41, 111–188 (2020).
Efficacy Safety of Statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet 393, 407–415 (2019).
Thai, M. et al. Prevalence of statin-drug interactions in older people: a systematic review. Eur. J. Clin. Pharmacol. 72, 513–521 (2016).
Rosengren, A. Better treatment and improved prognosis in elderly patients with AMI: but do registers tell the whole truth? Eur. Heart J. 33, 562–563 (2012).
Han, B. H. et al. Effect of Statin treatment vs usual care on primary cardiovascular prevention among older adults: the ALLHAT-LLT randomized clinical trial. JAMA Intern. Med. 177, 955–965 (2017).
Tsao, C. W. et al. Heart disease and stroke statistics-2023 update: A report from the American Heart Association. Circulation 147, e93–e621 (2023).
Cobos-Palacios, L. et al. Statin therapy in very old patients: lights and shadows. Front. Cardiovasc. Med. 8, 779044 (2021).
Kleipool, E. E. et al. Treatment of hypercholesterolaemia in older adults calls for a patient-centred approach. Heart 106, 261–266 (2020).
Virani, S. S., Smith, S. C., Stone, N. J. & Grundy, S. M. Secondary prevention for atherosclerotic cardiovascular disease. Circulation 141, 1121–1123 (2020).
ARPC Trial. MRC/BHF heart protection study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 360, 7–22 (2002).
Ponce, O. J. et al. Lipid-Lowering agents in older individuals: A systematic review and Meta-Analysis of randomized clinical trials. J. Clin. Endocrinol. Metab. 104, 1585–1594 (2019).
Lee, K. et al. Clinical impact of Statin intensity according to age in patients with acute myocardial infarction. PloS One. 17, e0269301 (2022).
Gencer, B. et al. Efficacy and safety of Lowering LDL cholesterol in older patients: a systematic review and meta-analysis of randomised controlled trials. Lancet 396, 1637–1643 (2020).
Bach, R. G. et al. Effect of Simvastatin-Ezetimibe compared with Simvastatin monotherapy after acute coronary syndrome among patients 75 years or older: A secondary analysis of a randomized clinical trial. JAMA Cardiol. 4, 846–854 (2019).
Räber, L. et al. Effect of Alirocumab added to High-Intensity Statin therapy on coronary atherosclerosis in patients with acute myocardial infarction: the PACMAN-AMI randomized clinical trial. JAMA 327, 1771–1781 (2022).
Sinnaeve, P. R. et al. Effect of Alirocumab on cardiovascular outcomes after acute coronary syndromes according to age: an ODYSSEY OUTCOMES trial analysis. Eur. Heart J. 41, 2248–2258 (2020).
Kim, J. H. et al. Multicenter cohort study of acute myocardial infarction in Korea - interim analysis of the Korea acute myocardial infarction registry-National institutes of health registry. Circ. J. 80, 1427–1436 (2016).
Hwang, D. et al. Effects of Statin intensity on clinical outcome in acute myocardial infarction patients. Circ. J. 82, 1112–1120 (2018).
Grundy, S. M. et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 73, e285–e350 (2018).
Grech, E. D. ABC of interventional cardiology: percutaneous coronary intervention. II: the procedure. BMJ 326, 1137–1140 (2003).
Acknowledgements
This study was conducted with the support of Korean Circulation Society (KCS) to commemorate the 50th Anniversary of KCS. The KAMIR study group of the KSC was as follows: Korea University Guro Hospital, Seoul, South Korea (Seung-Woon Rha); Gachon University Gil Medical Center, Incheon, South Korea (Tae Hoon Ahn); Wonju Severance Christian Hospital, Wonju, South Korea (Junghan Yoon); Seoul National University Hospital, Seoul, South Korea (Hyo-Soo Kim); Seoul St. Mary’s Hopital, Seoul, South Korea (Ki-Bae Seung); Samsung Medical Center, Seoul, South Korea (Hyeon-Cheol Gwon), Kyungpook National University Hospital, Daegu, South Korea (Shung Chull Chae); Kyunghee University Hospital At Gangdong, Seoul, South Korea (Chong-Jin Kim); Pusan National University Hospital, Busan, South Korea (Kwang Soo Cha); Yeungnam University Medical Center, Daegu, South Korea (Jung-Hee Lee); Chonbuk National University Hospital, Jeongju, South Korea (Jei Keon Chae); Jeju National University Hospital, Jeju, South Korea (Seung-Jae Joo); Seoul National University Bundang Hospital, Bundang, South Korea (Chang-Hwan Yoon); Keimyung University Dongsan Medical Center, Daegu, South Korea (Seung-Ho Hur); Chungnam National University Hospital, Daejeon, South Korea (In-Whan Seong); Chungbuk National University Hospital, Cheongju, South Korea (Kyung-Kuk Hwang); Inje University Haeundae Paik Hospital, Busan, South Korea (Doo-Il Kim); Wonkwang University Hospital, Iksan, South Korea (Seok Kyu Oh); Gyeongsang National University Hospital, Jinju, South Korea (Jin-Yong Hwang); and Chonnam National University Hospital, Gwangju, South Korea (Myung Ho Jeong). We acknowledge the contributions of all KAMIR investigators for their efforts in patient enrollment and data collection.
Author information
Authors and Affiliations
Contributions
Her AY, Choi BG, Park S, Hyun SJ, Choi CU, Rha SW, Kim YH, Jeong MH – extraction and analysis of data; Her AY, Choi BG, Rha SW, Kim YH – design and drafting of the manuscript; Her AY, Choi BG, Rha SW, Kim YH – revision of the manuscript. All authors have read and agreed to the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflicts of Interest
Su Jin Hyun is currently employed by Yuhan Corporation (a pharmaceutical company); this employment began after the completion of the research and preparation of the manuscript. Yuhan Corporation had no role in the study design; data collection, analysis, or interpretation; writing of the report; or the decision to submit the article, and provided no funding for this work. No other conflicts of interest are declared.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Her, AY., Choi, B.G., Park, S. et al. High-intensity statin on 3-year clinical outcomes in elderly acute myocardial infarction patients underwent percutaneous coronary intervention with drug-eluting stents. Sci Rep 15, 35325 (2025). https://doi.org/10.1038/s41598-025-19385-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-19385-w
