
Abstract
To examine employment status amongst people with multiple sclerosis (pwMS) in Israel, identify predictors of employment status, and investigate factors contributing to absenteeism amongst employed individuals. This cross-sectional study included 119 pwMS (65 women, mean age, 40.1 years, mean disease duration, 10.0 years). Participants completed self-reported questionnaires assessing employment status, absenteeism, work-related difficulties, perceived fatigue, perceived mobility, bladder and bowel function, fear of falling, and psychological and cognitive factors. The level of disability and information processing speed were also evaluated. Statistical analyses included ANOVA, t-tests, and regression models. Almost half of the participants (49.6%) were fully employed, 29.4% were partially employed, and 21.0% were unemployed. Unemployed pwMS reported higher levels of fatigue, mobility challenges, bladder and bowel dysfunction, and fear of falling. Perceived fatigue, specifically the physical and cognitive subscales, distinguished fully employed from partially employed individuals and was the most significant predictor of absenteeism (52.7%) of employed participants reported missing work due to multiple sclerosis. No significant differences were observed in depression, anxiety, or cognitive function across employment groups. Fatigue emerged as a critical determinant of employment status and absenteeism in pwMS, in conjunction with physical and functional barriers. Interventions addressing fatigue, mobility, bladder issues, and workplace accommodations are essential for improving employment outcomes. Longitudinal research is warranted to explore causal relationships and guide comprehensive strategies for employment retention.
Similar content being viewed by others

Introduction
Multiple sclerosis (MS) is a chronic autoimmune disorder of the central nervous system characterized by demyelination and neurodegeneration, leading to disrupted neural transmission1. Common symptoms include fatigue, mobility difficulties, mood disorders, sensory impairments, and cognitive dysfunction. MS typically manifests between ages 20–40, with a female-to-male prevalence ratio of ~ 3:12. Whereas immunomodulatory therapies aim to reduce relapse rates and slow disease progression, MS remains incurable3.
Employment changes often occur within a few years after a MS diagnosis, with unemployment being a frequent outcome4,5. A recent analysis based on several European MS registries reported adjusted unemployment rates ranging from 19.8% in Sweden to 53.2% in Poland6. Similar trends have been reported in other countries, i.e., only 36.1% of surveyed pwMS in the United States were employed, whereas 47.8% of pwMS in Canada declared that unemployment was due to the disease7,8.
Unemployment amongst working-age adults significantly impacts psychological, emotional, and social well-being9. It is closely linked to heightened stress, anxiety, and depression due to financial insecurity, loss of routine, and diminished self-worth10. Chronic unemployment can also foster health issues, such as sleep disturbances and weakened immunity, whereas social isolation from stigma and perceived failure erodes support networks11. For pwMS, unemployment has profound consequences, exacerbating financial insecurity, limiting access to necessary healthcare and adaptive equipment, and increasing the risk of depression and anxiety12,13. Furthermore, unemployment reduces opportunities for physical and cognitive activity, consequently possibly accelerating MS symptom progression and disability.
Identifying the key factors influencing employment status in pwMS is critical for guiding effective interventions and health management. While prior research has identified predictors such as disease severity, fatigue, and cognitive impairments14, significant limitations persist15. Variability in sample characteristics, socio-economic factors, cultural contexts, and healthcare systems limits the generalizability of findings. Furthermore, varying definitions of employment and the lack of standardized assessment tools hinder cross-study comparisons. Rigorous methodologies are warranted to understand these factors better, eventually aiding in developing strategies to support employment amongst pwMS.
It is important to note that employment outcomes in pwMS are shaped by a wide array of non-disease-related factors, including workplace accommodations, social support, stigma, access to vocational rehabilitation, and broader socio-economic conditions. While this study focuses on disease-specific variables, these broader influences are essential for understanding the full context of employment challenges in MS.
Given Israel’s universal healthcare system, comprehensive disability benefits, and employment protection laws, workforce participation in pwMS may be influenced by unique structural and cultural factors. These contextual elements underscore the importance of localized research to inform country-specific interventions and policies. Therefore, the primary objective of this study was to examine the employment status of pwMS in Israel. Moreover, we aimed to identify disease-related factors that can predict employment status. We also investigated work absenteeism for the past six months in employed pwMS, and examined which disease-related factors best predicted absenteeism from work due to MS.
Methods
Study design and participants
After local ethical approval, a convenience sample of 119 pwMS, 65 women and 54 men, aged 40.4 (SD = 11.4) from the Multiple Sclerosis Center, Sheba Medical Center, Tel-Hashomer, Israel, were admitted to the study. Participants were recruited through direct contact with the study’s staff or local advertising. While recruitment was based on a convenience sample, the Sheba MS Center is the largest in Israel and serves approximately 60% of the national MS population, with referrals from across the country. Nevertheless, the potential for selection bias remains. Inclusion criteria included: (1) a diagnosis of MS according to the revised McDonald Criteria 201716, and (2) an age range of 21–65 years. Exclusion criteria included: (1) major depression or cognitive decline limiting the ability to understand the study instructions or complete the study protocol, (2) pregnancy, (3) blurred vision, (4) MS clinical relapse or treatment with corticosteroid therapy within six months prior to the examination (5) and cardiovascular disorders. These criteria aimed to minimize confounding from non-MS-related factors. The study was approved by the Sheba Institutional Review Board (Ref# SMC-8328-21). All subjects signed an informed consent form before participation. All methods were carried out in accordance with relevant guidelines and regulations.
Study protocol
An experienced health professional performed and collected all outcome measures during a single session. The session included recording the participant’s demographic and clinical information (age, gender, disease duration, type of MS, family status, and home location). Subsequently, participants completed a questionnaire about their employment status over the past six months, including their average weekly working hours. Based on this, employment was categorized as full-time (30–40 h/week), part-time (less than 30 h/week), or unemployed (not currently working). Employed participants were also asked whether they had missed work due to MS during that period (yes/no), and if so, to report the total number of workdays missed. Furthermore, participants completed a self-report questionnaire on work difficulties (MS Work Difficulties Questionnaire). Next, they completed a battery of patient-reported outcome measures related to mobility, cognition, perceived fatigue, fear of falling, bladder and bowel function, depression, and anxiety. In addition, they completed testing of their information processing speed as an indicator of cognitive status. The Expanded Disability Status Scale (EDSS) score17 was retrieved from the patient’s computerized medical records.
Outcome measures
MS work difficulties questionnaire shortened scale
The MS Work Difficulties Questionnaire shortened scale (MSWDQ-23)18, a shortened self-report survey of the original MS Work Difficulties Questionnaire19 examined work difficulties in pwMS across three broad domains: psychological/cognitive, physical, and external barriers. Subscale scores for physical, psychological/cognitive, and external barriers are computed as a percentage by summing the observed item scores, divided by the total possible item scores in each subscale, and then multiplying the value by 100, presenting a maximum total score in each subscale of 100. The high scores indicated more significant difficulties. This survey has shown good concurrent validity to future work expectations in currently employed pwMS. A 2012 study found that Cronbach’s alpha values for the three subscales were 0.89, 0.81, and 0.80, respectively, indicating excellent internal consistency19.
Perceived fatigue
Perceived fatigue was assessed by the Modified Fatigue Impact Scale (MFIS), a multidimensional 21-item questionnaire that acquired data relating to the effects of fatigue-physical (9-items), psychosocial (2-items), and cognitive (10-items) domains over four weeks. pwMS rated the 21 items using a 5-point Likert-type scale, ranging from never (0) to always (4); the higher the score, the more perceived fatigue. The MFIS has demonstrated good reliability over a six-month period and has strongly correlated with the Fatigue Severity Scale results20.
Perceived mobility
Perceived mobility was measured by the 12-item MS Walking scale (MSWS-12). The MSWS-12, a valid self-reported questionnaire assessing walking ability in pwMS, is the most widely used patient-reported measure of perceived limitation in walking attributable to MS21. It has been used in numerous clinical trials in the pwMS population due to its excellent psychometric properties22,23.
Anxiety and depression
Anxiety and depression were assessed by the Hospital Anxiety and Depression Scale (HADS), widely used in clinical practice and validated in the pwMS population24. The scale, consisting of 7 items, rates two components - anxiety and depression. The questionnaire includes three cut-off scores indicative of different levels describing clinically relevant distress: a score between 0 and 7 = normal status, 8–10 = borderline, and 11–21 = an abnormal depression rate25.
Cognition
The Symbol Digit Modalities Test (SDMT), a cognitive outcome measurement tool was administered utilizing standardized procedures26. The SDMT is a measure of information processing speed. The primary SDMT outcome is the raw score. Substantial evidence supports the psychometric properties of the SDMT27,28 which has been recommended as the cognitive test of choice for MS clinical trials26.
Fear of falling
Fear of falling was assessed by the Falls Efficacy Scale International (FES-I) self-reported questionnaire29,30. The questionnaire assessed the level of concern regarding falling during 16 activities of daily living, ranging from basic to more demanding activities, including social activities that may have contributed to the participants’ quality of life. The level of concern for each item was scored using a four-point scale (1 = not at all concerned, 4 = very concerned). The total FES-I score ranges from 16 to 64, with higher scores indicating greater concern about falling. Although no universal cut-off is established for the MS population, scores above 23 typically suggest elevated fall-related concern. The FES-I has been shown as appropriate for research and clinical purposes in pwMS31.
Bladder and bowel function
Bladder and bowel function were assessed by the Bladder Control Scale (BLCS) and the Bowel Control Scale (BWCS). Both scales are components of the MS Quality of Life Inventory (MSQLI), which is both generic and MS-specific32. The BLCS (four-item instrument) and the BWCS (five-item instrument) provide a brief assessment of bladder/bowel control and how much bladder/bowel problems impact everyday activities. Higher scores indicate more problems. The BLCS and BWCS have a Cronbach’s alpha of 0.82 and 0.78, respectively.
Statistical analysis
Descriptive statistics were used to determine demographic characteristics (gender, home location, family status, and education), clinical characteristics (disease duration, disability (EDSS), type of MS), fear of falling, MS-related measures (mobility, bladder/bowel function, perceived fatigue, depression, anxiety, and cognition), and work-related measures (employment status and work difficulties via the MSWDQ-23). Only the total MFIS score was used in analyses to avoid multicollinearity with its subscales. Pearson’s correlation analysis examined the relationships between the outcome measures. A one-way ANOVA assessed differences in the outcome measures based on employment status (full-time/part-time/unemployed). Given the exploratory nature of the study, multiple ANOVAs and t-tests were performed without formal correction for multiple comparisons. While post hoc Tukey HSD tests were applied for pairwise group comparisons in the ANOVA, we acknowledge the increased risk of Type I error and advise cautious interpretation of the p-values.
We assessed normality of distributions using the Shapiro-Wilk test and examined homogeneity of variances with Levene’s test. Although certain variables (e.g., EDSS and fatigue scores) showed mild deviations from normality, ANOVA was retained given its robustness in moderately sized samples. We acknowledge the ordinal nature of the EDSS and note this as a limitation in applying parametric tests to this variable.
An ordinal logistic regression analysis was conducted to identify which study variables predicted employment status. The outcome variable was coded such that a higher value indicated a greater employment impairment (full-time = 1, part-time = 2, unemployed = 3). Only variables that showed significant differences between employment groups in the preceding one-way ANOVA analyses were included in the model. All selected variables were entered simultaneously into the regression model (i.e., no stepwise selection was applied). The proportional odds assumption was tested using the Test of Parallel Lines in SPSS and was not violated (p > 0.05), supporting the appropriateness of the ordinal logistic regression model. To assess multicollinearity among predictors, we calculated variance inflation factors (VIFs) for all included variables. All VIFs were below 2.0, indicating no significant multicollinearity.
Independent-sample t-tests examined the differences in outcome measures between employed (full or partly) pwMS who were or were not absent from work during the past 6 months. Unemployed patients were excluded from this analysis. Based on the t-test results, a logistic regression was conducted to determine which outcome measures best-predicted work absenteeism due to MS.
All analyses were performed using the SPSS software (version 28.0 for Windows; SPSS Inc., Chicago, IL, USA). The data were examined for normality violations, outliers, errors, and missing values. All reported p-values were two-tailed, with the significance level set at p < 0.05.
Results
One hundred and nineteen pwMS (65 females, mean age 40.1 (SD = 11.4) years, mean disease duration 10.0 (SD = 7.7) years) participated in the study. Most pwMS had minimal to mild levels of disability (57%). Regarding employment, 49.6% were fully employed, 29.4% were partially employed, and 21.0% were unemployed. Demographics, clinical and disease-related measures, and employment status are presented in Table 1.
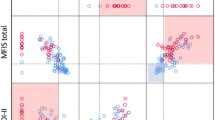
Outcome measures according to employment status are presented in Table 2. Unemployed pwMS reported more work-related barriers (based on the MSWDQ), specifically in the physical domain, than employed (partly or fully) participants. Additionally, unemployed pwMS reported poor bladder and bowel function, more difficulties in mobility, higher fear of falling, and elevated perceived fatigue (including physical, cognitive, and psychosocial subscales) compared with fully employed pwMS. Non-significant differences between employment groups were demonstrated in work-related external barriers (i.e., work/home balance difficulties, financial security concerns) and cognitive barriers (Fig. 1). When comparing fully and partially employed groups, perceived fatigue (total, physical, and cognitive subscales) was the only significant difference, with partially employed participants reporting higher fatigue levels. No differences between the three employment groups were found in terms of gender distribution, years of education, anxiety, depression, disease duration, and information processing speed.

Scores of the MS Work Difficulties Questionnaire (MSWDQ) according to fully employed (n = 59), partially employed (n = 35), and unemployed (n = 25) groups.
Table 3 presents the findings of the ordinal logistic regression analysis aimed at identifying variables that distinguish between the three employment groups (fully employed, partially employed, and unemployed). The variables included in the model were those that showed significant group differences in the preceding ANOVA analyses. The overall model, incorporating all predictors simultaneously, was statistically significant, χ²(8) = 8.57, p = 0.017, and explained 21% of the variance in employment status (Nagelkerke’s pseudo-R²=0.207). However, none of the individual predictors reached statistical significance in the model, indicating that no single variable independently explained differences in employment status once the other variables were accounted for. This may reflect overlapping variance among predictors or limited statistical power; conceptually relevant variables were retained to preserve interpretability and avoid excluding potentially meaningful predictors.
As for absenteeism from work amongst the employed participants (fully or partly), 52.7% reported that there were days when they were absent from work due to MS during the past 6 months. Among those who reported absenteeism, the mean number of missed workdays was 40.1 (SD = 58.8). Participants who reported absenteeism from work, scored significantly higher on the MSWDQ (total and subdomains) compared to the non-absent subgroup (Fig. 2). Furthermore, the absentee subgroup experienced more bladder and bowel difficulties, increased fear of falling, elevated perceived fatigue (including subscales), higher anxiety, and depression compared to the non-absentee subgroup. Non-significant differences between the absenteeism subgroups were found for age, education, disease duration, level of disability, perceived mobility, and information processing speed. Table 4 presents the scores of the employed participants divided by absenteeism from work subgroups.

MSWDQ scores according to absenteeism subgroups (Yes, n = 48; No, n = 43).
Discussion
This study examined employment status and absenteeism in working-age individuals with MS living in Israel. We focused on key disease-related factors that potentially can affect these outcomes. Our findings are consistent with prior research highlighting high unemployment rates amongst pwMS, with 21% of participants unemployed and 29.4% working part-time. Moreover, over half of the employed participants (52.7%) reported missing work due to MS within the past six months. Notably, given the relatively young cohort in this sample (mean age, 40.1), the results align with a recent systematic review encompassing ~ 190,000 pwMS across 29 countries, which reported a pooled unemployment rate of 35.6%33. These findings underscore the significant impact of the MS disease on workforce participation, mirroring trends observed in other countries, including the United States and Canada.
Importantly, perceived fatigue, physical barriers (particularly mobility difficulties), bladder and bowel dysfunction, level of disability, and fear of falling emerged as significant factors related to pwMS’ unemployment. Nevertheless, according to the ordinal logistic regression analysis, none of these factors, including fatigue, remained significant predictors in isolation. This finding aligns with the literature, emphasizing that a multifactorial approach is essential when addressing employment-related challenges in pwMS, as these factors interact and collectively contribute to employment in this population34.
Interestingly, perceived fatigue (total, physical and cognitive subscales) was the only significant factor in isolation from other variables that distinguished fully employed from partially employed MS participants. It was also a significant predictor of absenteeism amongst employed pwMS, highlighting its central role in workplace limitations. This discovery is reinforced by Ramirez et al.‘s35 systematic literature review reporting on the epidemiology and burden of fatigue in pwMS. Based on data from 54 studies, the review consistently demonstrated a significant association between the presence or severity of fatigue and employment status, work capacity, and sick leave.
It is noteworthy that perceived mobility, although significantly associated with employment status, did not reach statistical significance in the absenteeism analysis. This may suggest that employed individuals with mobility limitations have adapted their work environments or roles, thereby reducing its direct influence on short-term work absence.
Notably, bladder/bowel dysfunction and fear of falling, while strongly associated with both employment status and absenteeism in univariate analyses, were not retained as independent predictors in multivariable models. This may reflect overlapping variance with fatigue or mobility measures. Future studies could consider testing interaction effects or conducting subgroup analyses (e.g., by gender or disability level) to explore these associations in greater depth.
Several factors may explain these patterns of association and non-significance observed in the multivariable models. Firstly, the unpredictable nature of MS-related fatigue makes it challenging to maintain consistent work schedules, often resulting in absenteeism or the need for frequent breaks, which may conflict with workplace expectations. Furthermore, fatigue is frequently misunderstood by employers and colleagues, who may misinterpret it as a lack of motivation or effort36. This misperception, combined with insufficient workplace accommodations such as flexible hours or remote work options, creates additional barriers to sustained employment. Over time, these challenges may cumulatively hinder career progression, as pwMS are often perceived as less capable of handling increased responsibilities, further affecting their long-term employment outcomes.
Somewhat surprisingly, no significant differences between employment groups were observed for depression, anxiety, education level, or information processing speed. Furthermore, depression, education, and cognition were similar between the absenteeism subgroups. While some studies align with these findings, i.e., Dorstyn et al.37, who found no association between employment and depression or anxiety in the MS population, others reported different results. For example, Clemens and Langdon14 identified cognitive impairment as a factor influencing employment difficulties and reduced work hours in MS. Forslin et al.38 found that baseline education level predicted work status after 10 years, and that deterioration in functioning, particularly in walking ability and fatigue, was associated with a transition from full-time employment to part-time work or unemployment, highlighting the impact of physical symptoms over time on sustained employment.
Several explanations may account for the current findings. Firstly, the relatively mild disability levels in the present sample may have limited the prevalence of severe psychological and cognitive impairments, which are more strongly associated with greater disease severity. Additionally, employed individuals might use coping strategies or benefit from workplace accommodations that mitigate the impact of mental health challenges or cognitive difficulties, enabling them to remain employed. Education levels were similar across groups as most individuals with MS typically complete their education before disease onset, making it less relevant to current employment status. Cognitive reserve may also play a role, helping participants maintain a comparable cognitive performance despite disease-related challenges. Finally, cultural and societal factors, such as the robust social support systems and access to mental healthcare services in Israel, could buffer the psychological and cognitive impacts of unemployment obscuring potential group differences.
The main strength of this study lies in the comprehensive assessment of a broad range of disease-related and demographic factors, spanning physical, psychological, cognitive, and social domains, providing a multidimensional perspective on employment outcomes in pwMS. However, several limitations must be acknowledged. Firstly, the cross-sectional study design precludes causal inferences regarding the relationship between disease-related factors and employment outcomes. Furthermore, the use of convenience sampling may introduce selection bias, limiting the generalizability of the findings. However, it is worth noting that the study was conducted at the Sheba MS Center, the largest in Israel, which treats a diverse patient population and maintains contact with approximately 60% of pwMS nationally. Patients are referred from across the country, which enhances sample diversity to some extent, although the potential for selection bias remains. The exclusion of individuals with major depression, significant cognitive decline, or recent MS relapse, further restricts the applicability of the results to those with more severe disease manifestations, potentially underestimating the impact of these factors on employment. While self-reported measures of employment status, absenteeism, and work difficulties may be subject to recall bias, these data are challenging to obtain through other methods. In particular, absenteeism estimates may be affected by recall bias, as participants were asked to retrospectively report absences over a six-month period. Furthermore, cultural and societal factors unique to Israel, such as robust social support systems and universal healthcare, may limit the generalizability of the findings to other regions with varying healthcare systems and labor market dynamics. Lastly, the complex interplay of multiple factors influencing employment suggests interactions that the current analysis may not have fully captured, underscoring the need for more nuanced approaches in future research. Additionally, we acknowledge that some variables analyzed using ANOVA, such as EDSS, which is ordinal, may not fully meet parametric assumptions. While ANOVA is generally robust in moderate samples, this should be considered when interpreting these findings, particularly given the multiple comparisons performed.
Conclusion
Herein, we underscore the significant role of perceived fatigue, mobility challenges, bladder and bowel dysfunction, and fear of falling in influencing employment status and absenteeism amongst pwMS. Fatigue emerged as a critical factor, differentiating fully employed from partially employed individuals and predicting absenteeism. These findings highlight the need for targeted clinical interventions, such as fatigue management programs, workplace accommodations (e.g., flexible hours), and support for mobility and bladder issues, to enhance employment retention. Future research should focus on longitudinal studies to explore causal relationships and develop comprehensive strategies addressing the multifactorial barriers to employment in pwMS.
Data availability
All data will be available upon request by emailing the corresponding author.
References
Compston, A. & Coles, A. Multiple sclerosis. Lancet 372 (9648), 1502–1517. https://doi.org/10.1016/S0140-6736(08)61620-7 (2008).
Olsson, T., Barcellos, L. F. & Alfredsson, L. Interactions between genetic, lifestyle and environmental risk factors for multiple sclerosis. Nat. Rev. Neurol. 13 (1), 25–36. https://doi.org/10.1038/nrneurol.2016.187 (2017).
Yang, J. H., Rempe, T., Whitmire, N., Dunn-Pirio, A. & Graves, J. S. Therapeutic advances in multiple sclerosis. Front. Neurol. 13, 824926. https://doi.org/10.3389/fneur.2022.824926 (2022).
Zarghami, A. et al. Changes in employment status over time in multiple sclerosis following a first episode of central nervous system demyelination, a Markov multistate model study. Eur. J. Neurol. 31 (1), e16016. https://doi.org/10.1111/ene.16016 (2024).
Marck, C. H. et al. Predictors of change in employment status and associations with quality of life: a prospective international study of people with multiple sclerosis. J. Occup. Rehabil. 30 (1), 105–114. https://doi.org/10.1007/s10926-019-09850-5 (2020).
Ellenberger, D. et al. Comparison of employment among people with multiple sclerosis across Europe. Mult Scler. J. Exp. Transl Clin. 8 (2), 055217321006. https://doi.org/10.1177/20552173221090653 (2022).
Nicholas, J. A., Electricwala, B., Lee, L. K. & Johnson, K. M. Burden of relapsing-remitting multiple sclerosis on workers in the US: a cross-sectional analysis of survey data. BMC Neurol. 19 (1), 258. https://doi.org/10.1186/s12883-019-1495-z (2019).
Hategeka, C., Traboulsee, A. L., McMullen, K. & Lynd, L. D. Association of unemployment and informal care with stigma in multiple sclerosis: evidence from the survey on living with neurological conditions in Canada. Int. J. MS Care. 21 (5), 214–225. 10.7224/ 1537-2073.2017-108 (2019).
Mousteri, V., Daly, M. & Delaney, L. The scarring effect of unemployment on psychological well-being across Europe. Soc. Sci. Res. 72, 146–169. https://doi.org/10.1016/j.ssresearch.018 (2018).
Morrish, N., Mujica-Mota, R. & Medina-Lara, A. Understanding the effect of loneliness on unemployment: propensity score matching. BMC Public. Health. 22 (1), 740. doi10.1016/j.ssresearch.2018.01.007 (2022).
Vancea, M. & Utzet, M. How unemployment and precarious employment affect the health of young people: A scoping study on social determinants. Scand. J. Public. Health. 45 (1), 73–84. https://doi.org/10.1177/1403494816679555 (2017).
Strober, L. B. et al. Unemployment in multiple sclerosis: the contribution of personality and disease. Mult Scler. 18 (5), 647–653. https://doi.org/10.1177/1352458511426735 (2012).
Ponzio, M. et al. Work difficulties in people with multiple sclerosis. J. Occup. Rehabil. 34 (3), 606–617. https://doi.org/10.1007/s10926-023-10149-9 (2024).
Clemens, L. & Langdon, D. How does cognition relate to employment in multiple sclerosis? A systematic review. Mult Scler. Relat. Disord. 26, 183–191. https://doi.org/10.1016/j.msard.2018 (2018).
Rodriguez Llorian, E. et al. Employment status, productivity loss, and associated factors among people with multiple sclerosis. Mult Scler. 29 (7), 866–874. https://doi.org/10.1177/13524585231164295 (2023).
Thompson, A. J. et al. Diagnostic of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 17, 162–173. https://doi.org/10.1016/S1474-4422(17)30470-2 (2018).
Kurtzke, J. F. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33, 1444–1452. https://doi.org/10.1212/wnl.33.11.1444 (1983).
Honan, C. A., Brown, R. F. & Hine, D. W. The multiple sclerosis work difficulties questionnaire (MSWDQ): development of a shortened scale. Disabil. Rehabil. 36 (8), 635–641. https://doi.org/10.3109/09638288.2013.805258 (2014).
Honan, C. A. et al. The multiple sclerosis work difficulties questionnaire. Mult Scler. 18 (6), 871–880. https://doi.org/10.1177/1352458511431724 (2012).
Learmonth, Y. C. et al. Psychometric properties of the fatigue severity scale and the modified fatigue impact scale. J. Neurol. Sci. 331 (1–2), 102–107. https://doi.org/10.1016/j.jns.2013.05.023 (2013).
Hobart, J. C., Riazi, A., Lamping, D. L., Fitzpatrick, R. & Thompson, A. J. Measuring the impact of MS on walking ability: the 12-Item MS walking scale (MSWS-12). Neurology 60 (1), 31–36. https://doi.org/10.1212/wnl.60.1.31 (2003).
Baert, I. et al. Responsiveness and clinically meaningful improvement, according to disability level, of five walking measures after rehabilitation in multiple sclerosis: a European multicenter study. Neurorehabil Neural Repair. 28 (7), 621–631. https://doi.org/10.1212/wnl.60.1.31 (2014).
Kalron, A. et al. Improving our Understanding of the most important items of the multiple sclerosis walking Scale-12 indicating mobility dysfunction: secondary results from a RIMS multicenter study. Mult Scler. Relat. Disord. 46, 102511. https://doi.org/10.1016/j.msard.2020.102511 (2020).
Honarmand, K. & Feinstein, A. Validation of the hospital anxiety and depression scale for use with multiple sclerosis patients. Mult Scler. 15 (12), 1518–1524. https://doi.org/10.1177/35248509347150 (2009).
Zigmond, A. S. & Snaith, R. P. The hospital anxiety and depression scale. Acta Psychiatr Scand. 67 (6), 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x (1983).
Benedict, R. H. et al. Validity of the symbol digit modalities test as a cognition performance outcome measure for multiple sclerosis. Mult Scler. 23 (5), 721–733. https://doi.org/10.1177/1352458517690821 (2017).
Strober, L. et al. Symbol digit modalities test: A valid clinical trial endpoint for measuring cognition in multiple sclerosis. Mult Scler. 25 (13), 1781–1790. https://doi.org/10.1177/1352458518808204 (2019).
LaRocca, N. G. et al. The MSOAC approach to developing performance outcomes to measure and monitor multiple sclerosis disability. Mult Scler. 24 (11), 1469–1484. https://doi.org/10.1177/1352458517723718 (2018).
Yardley, L. et al. Development and initial validation of the falls efficacy Scale-International (FES-I). Age Ageing. 34 (6), 614–619. https://doi.org/10.1093/ageing/afi196 (2005).
Hadjistavropoulos, T., Delbaere, K. & Fitzgerald, T. D. Reconceptualizing the role of fear of falling and balance confidence in fall risk. J. Aging Health. 23 (1), 3–23. 10.177/ (2011).
van Vliet, R., Hoang, P., Lord, S., Gandevia, S. & Delbaere, K. Falls efficacy scale-international: a cross-sectional validation in people with multiple sclerosis. Arch. Phys. Med. Rehabil. 94 (5), 883–889. https://doi.org/10.1016/j.apmr.2012.10.034 (2013).
Fischer, J. S. et al. Recent developments in the assessment of quality of life in multiple sclerosis (MS). Mult Scler. 5 (4), 251–259. https://doi.org/10.1177/135245859900500410 (1999).
Vitturi, B. K. et al. Spatial and Temporal distribution of the prevalence of unemployment and early retirement in people with multiple sclerosis: A systematic review with meta-analysis. PLoS One. 17 (7), e0272156. (2022).
Kavaliunas, A., Danylaitė Karrenbauer, V., Binzer, S. & Hillert, J. Systematic review of the socioeconomic consequences in patients with multiple sclerosis with different levels of disability and cognitive function. Front. Neurol. 12, 737211. https://doi.org/10.3389/fneur.021 (2022).
Oliva Ramirez, A. et al. Prevalence and burden of multiple sclerosis-related fatigue: a systematic literature review. BMC Neurol. 21 (1), 468. https://doi.org/10.1186/s12883-021-02396-1 (2021).
Helme, C., Hegarty, R. S. M., Stebbings, S. & Treharne, G. J. I actually just really need to stop work sometimes: exploring fatigue-related barriers to employment among people with rheumatic diseases. Musculoskelet. Care. 17 (1), 97–104. https://doi.org/10.1002/msc.1373 (2019).
Dorstyn, D. S., Roberts, R. M., Murphy, G. & Haub, R. Employment and multiple sclerosis: A meta-analytic review of psychological correlates. J. Health Psychol. 24 (1), 38–51. https://doi.org/10.1177/1359105317691587 (2019).
Forslin, M., Fink, K., Hammar, U., von Koch, L. & Johansson, S. Predictors for employment status in people with multiple sclerosis: a 10-year longitudinal observational study. Arch. Phys. Med. Rehabil. 99 (8), 1483–1490. https://doi.org/10.1016/j.apmr.2017.12.028 (2018).
Funding
Bituah Leumi, Israel’s National Social Security agency, supported this work, Grant #18467. The funding source had no role in the research’s design, implementation, or interpretation.
Author information
Authors and Affiliations
Contributions
A.I – Investigation, Formal analysis, Writing – Review & Editing, VisualizationS.M – Resources, Writing – Review & Editing, Project administration A. K – Conceptualization, Methodology, Supervision, Writing – Original draft, Funding acquisition.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Sheba Institutional Review Board (Ref# SMC-8328-21). All subjects signed an informed consent form before participation.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Iron, A., Menascu, S. & Kalron, A. Factors influencing employment and absenteeism in working age people with multiple sclerosis. Sci Rep 15, 36265 (2025). https://doi.org/10.1038/s41598-025-20165-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-20165-9
