
Abstract
This study aims to analyze changes in the disease burden of cystic echinococcosis in China from 1990 to 2019 and to predict trends from 2020 to 2044. Using the Global Burden of Disease 2019 (GBD 2019) database, we analyzed the trends in annual percentage change (APC) and average annual percentage change (AAPC) for incidence, prevalence, death, and disability-adjusted life years (DALY) rates of cystic echinococcosis in China via the Joinpoint Regression Program 4.8.0.1 software. Additionally, we applied Nordpred modeling to predict future trends in disease burden over the next 25 years. From 1990 to 2019, the incidence and prevalence of cystic echinococcosis in the Chinese population showed an overall increasing trend, whereas the death and DALY rates exhibited an overall decreasing trend. The disease burden of cystic echinococcosis was greater in males than in females, with significant differences across age groups. The highest incidence and prevalence rates were observed in the 10–24 years age group, whereas the lowest occurred in the 0–9 years age group. Fatalities and DALY rates increased with age, particularly in the 70 and older age groups. According to the Nordpred modeling results, the incidence, prevalence, and DALY rates of cystic echinococcosis in China are expected to rise slightly over the next 25 years. The overall disease burden of cystic echinococcosis is projected to increase gradually between 2020 and 2044, with men exhibiting higher incidence, prevalence, and DALY rates than women.
Similar content being viewed by others
Introduction
Echinococcosis is a zoonotic disease caused by the larval stage of the Echinococcus tapeworm, which parasitizes both humans and animals globally1,2,3,4. Without treatment, the 10-year mortality rate exceeds 90%5–6. Echinococcosis poses significant public health challenges and economic burdens7–8. The life cycle of echinococcosis parasites involves carnivores as final hosts and intermediate host species that develop into an infective metazoan stage following oral egg ingestion. In China, the two most common types of human echinococcosis are cystic echinococcosis (CE), caused by fine-grained tapeworm larvae, and alveolar echinococcosis (AE), caused by multihost echinococcal tapeworm larvae9. Cystic echinococcosis affects mainly rural and suburban regions, where access to healthcare is frequently limited10–11. The disease substantially threatens livestock production and has a profound impact on human health, public health security, and ecological stability, contributing to poverty among farmers and herders12. As a neglected tropical disease (NTD) and zoonosis, cystic echinococcosis is globally prevalent, except in Antarctica. It has been identified as one of the 17 neglected diseases that the World Health Organization (WHO) aims to control or eliminate by 205013, with a global prevalence rate estimated at 5-10%14. In regions with inadequate treatment, the death rate may exceed the expected range of 2–4%9. In China, the western region has a high prevalence of cystic echinococcosis15, which hinders economic development. Despite existing studies focusing on regional distribution, diagnosis, and prevention knowledge among farmers and herders, comprehensive assessments of the impact of cystic echinococcosis on public health are lacking. Therefore, this study utilizes the GBD 2019 database to evaluate the disease burden of cystic echinococcosis in China from 1990 to 2019 and to predict trends from 2020 to 2044, providing a scientific basis for understanding epidemiological trends and formulating effective prevention and control strategies.
Content and methodology
Data sources
The burden of disease data for this study were obtained from the GBD 2019 database (https://vizhub.healthdata.org/gbd-results/), including data on incidence, prevalence, deaths, and disease burden. The demographic data used for projections were also sourced from this database (https://ghdx.health-data.org/data-type/estimate). The GBD 2019 employs a harmonized methodology to evaluate the burden of disease for 264 diseases across 195 countries and territories, including cystic echinococcosis in China.
Analyzing indicators
The disease burden associated with cystic echinococcosis in China was extracted from the GBD 2019 database for the years 1990–2019. The burden of disease was assessed via the age-standardized rate (ASR), which included incidence, prevalence, death, DALY rates, and age-standardized measures.
Statistical analysis
Data calculations were performed using age-standardization. Raw and age-standardized data for incidence, mortality, prevalence, and DALYs were downloaded from the GBD database. The purpose of age-standardization is to remove the effect of differences in age structure. We analyzed the Age-standardized incidence rate (ASIR), Age-standardized prevalence rate (ASPR), Age-standardized mortality rate (ASMR) and Age-standardized DALY rate (ASDR). The burden of disease and changes in cystic echinococcosis were analyzed by age groups: 0–9 years, 10–24 years, 25–49 years, 50–69 years, and ≥ 70 years. Trend analysis was performed via the Joinpoint Regression Program 4.8.0.1 software16, which employs log-linear regression models to calculate annual percentage changes (APC) and average annual percentage changes (AAPC) for different time periods.
In light of recent trends, a log-linear age–period–cohort model was employed to predict the rates of incidence, prevalence, mortality, and DALYs spanning from 2020 to 2044. The Nordpred software package, which was developed and implemented using R, has demonstrated excellent empirical performance in projecting these recent trends forward17–18. Specifically, it extrapolates the most recent observed periods of either 3 or 4 years (depending on the availability of national or regional registries, where applicable) out of a total 5-year window, leveraging a power function to moderate the growth curve. Subsequently, during the second, third, and fourth prediction intervals, the linear trend of the past decade is fine-tuned, with its slope being either reduced or enhanced by 25%, 50%, and 75% respectively. The details can be found elsewhere18.
For the purposes of statistical analysis and visualization, we utilized the Joinpoint Regression Software (Version 4.8.0.1, developed by the Statistical Research and Applications Branch of the National Cancer Institute) in conjunction with R Version 4.1.3. All statistical tests were of a two-sided nature, and a P-value lower than 0.05 was regarded as statistically significant.
Results
Trends in the disease burden of cystic echinococcosis in China
The Age-standardized incidence rate (ASIR) of cystic echinococcosis in China increased from 0.41/100,000 in 1990 to 0.46/100,000 in 2019. It declined to 0.4/100,000 from 1992 to 1999 and then increased in 2000 without further decline. The Age-standardized prevalence rate (ASPR) rose from 1.84/100,000 in 1990 to 2.07/100,000 in 2019, declining from 1992 to 1997 before a slow rise starting in 1998. The age-standardized mortality rate (ASMR) decreased from 0.01/100,000 in 1990 to less than 0.01/100,000 in 2019, remaining at this level since 1996. The Age-standardized DALY rate (ASDR) decreased from 0.46/100,000 in 1990 to 0.27/100,000 in 2019, declined annually to 0.18/100,000 from 1990 to 2017, and then increased to 0.27/100,000 from 2018 to 2019 (Table 1).
Joinpoint regression analysis
Stratification by sex
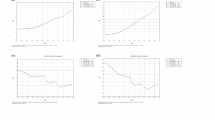
The Joinpoint regression analysis indicated that the ASIR [AAPC = 0.42%, 95% CI: (0.40%, 0.43%)] and ASPR [AAPC = 0.41%, 95% CI: (0.39%, 0.43%)] of cystic echinococcosis in China increased slightly annually from 1990 to 2019. Both the ASIR and ASPR in men and women also slightly increased (Fig. 1A, B). The ASIR in males slightly decreased from 1990 to 1993 [APC = -0.22%, 95% CI: (-0.45%, -0.06%)], followed by a yearly increase from 1993 to 2019 (Fig. 1A). The ASPR in males decreased slightly from 1990 to 1993 [APC = -0.23%, 95% CI: (-0.32%, -0.32%, -0.32%, -0.32%)]. The female ASPR decreased from 1990 to 1993 [APC = -0.51%, 95% CI: (-0.77%, -0.29%)], which was more pronounced than that of males during the same period. A year-to-year upward trend was observed from 1998 to 2019 (Fig. 1A). Overall, the ASIR and ASPR of cystic echinococcosis were greater in males than in females (Fig. 1A, B) (Table 2). The ASMR [AAPC = -1.64%, 95% CI: (-3.67%, 0.44%)] and ASDR [AAPC = -1.63%, 95% CI: (-2.37%, -0.89%)] of cystic echinococcosis in China showed decreasing trends from 1990 to 2019. The male and female ASMR and ASDR also demonstrated decreasing trends (Table 2) (Fig. 1C, D).


Trends in disease burden of cystic echinococcosis by sex.
Stratification according to age
Joinpoint regression analysis revealed that from 1990 to 2019, the ASIR of cystic echinococcosis in China were AAPC = 0.67% for the 0–9 age group, AAPC = 0.27% for the 10–24 age group, AAPC = 0.55% for the 25–49 age group, AAPC = 0.46% for the 50–69 age group, and AAPC = 0.10% for the 70 + age group, all indicating varying degrees of increase, with the highest rates in the 10–24 age group and the lowest in the 0–9 age group (Table 3; Fig. 2A). The ASPR were AAPC = 0.76% for the 0–9 age group, AAPC = 0.26% for the 10–24 age group, AAPC = 0.41% for the 25–49 age group, AAPC = 0.48% for the 50–69 age group, and AAPC = 0.18% for the 70 + age group, indicating different degrees of upward trends (Table 3; Fig. 2B).


Trends in disease burden of cystic echinococcosis by age.
The ASMR of cystic echinococcosis from 1990 to 2019 were AAPC = -6.97% for the 0–9 age group, AAPC = -3.82% for the 10–24 age group, AAPC = -2.41% for the 25–49 age group, AAPC = -1.60% for the 50–69 age group, and AAPC = 0.56% for the 70+-69 age group. The highest ASMR were observed in the 70 + year age group, with the lowest in the 10–24 year age group(Table 3; Fig. 2C). The ASDR were AAPC = -5.91% for the 0–9 age group, AAPC = -0.94% for the 10–24 age group, AAPC = -0.94% for the 25–49 age group, AAPC = -1.14% for the 50–69 age group, and not statistically significant for the 70 + age group, which displayed varying degrees of decrease (Table 3; Fig. 2D).
Projected disease burden of cystic echinococcosis in China, 2020 to 2044
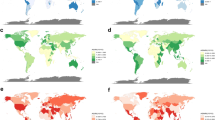
Nordpred model projections indicate that the ASIR, ASPR, and ASDR of cystic echinococcosis in China are expected to slightly increase from 2020 to 2044. ASMR were not included in the projections, as the ASMR was partially estimated to be 0.00/100,000 (Fig. 3). The ASIR is projected to increase from 0.46/100,000 in 2020 to 0.49/100,000 in 2044; the ASPR is expected to increase from 1.64/100,000 in 2020 to 1.71/100,000 in 2044; and the ASDR is forecasted to increase from 0.23/100,000 in 2020 to 0.29/100,000 in 2044 (Table 4). Notably, the ASIR, ASPR, and ASDR are anticipated to be higher in men than in women (Fig. 3; Table 4).

Projected disease burden of cystic echinococcosis in China, 1990–2044.
Discussion
Based on the GBD 2019 database, this study primarily examines changes in the disease burden of cystic echinococcosis in China from 1990 to 2019 and projects trends from 2020 to 2044 to enhance the understanding of the epidemiology of cystic echinococcosis. These findings indicate that the incidence and prevalence of cystic echinococcosis in China increased from 1990 to 2019, whereas fatalities and DALY rates decreased. This trend is attributed primarily to echinococcosis, which is a long-standing zoonotic parasitic disease with a lengthy incubation period19. The rapid development of animal husbandry in China, particularly after the reform and opening up, has increased the risk of human infection, leading to an overall rise in incidence and prevalence. Since 1987, pilot programs for the prevention and control of echinococcosis have been progressively initiated in Xinjiang, Sichuan, Gansu, Qinghai, and other regions across China. The principal comprehensive prevention and control strategy implemented was centered around “monthly deworming of all dogs”20. In certain areas, livestock vaccination measures were adopted21, while in a limited number of regions, a series of additional prevention and control initiatives were undertaken. These encompassed culling wild dogs, registering and tagging domestic dogs22, as well as establishing echinococcosis prevention and control funds through domestic dog management fees and social fundraising. In 2005, both the central government and local administrations at all tiers in China augmented their efforts in combating echinococcosis. Notably, in 2007, echinococcosis was designated as one of the major infectious diseases qualifying for free medical treatment by the state. Subsequently, the central government earmarked special funds to underpin a range of activities in the impoverished regions of central and western China. These activities comprised screening and treating echinococcosis patients, controlling infection sources, and conducting health education. Such concerted efforts have effectively catalyzed the advancement of echinococcosis prevention and treatment work, substantially alleviating the disease burden associated with this affliction. With China’s increasing focus on preventing and treating cystic echinococcosis, various action plans have been implemented, such as the Action Plan for Prevention and Treatment of Cystic Echinococcosis (2010–2015) and the National Plan for Prevention and Treatment of Cystic Echinococcosis and Other Key Parasitic Diseases (2016–2020). These policies mandate that central and local governments increase efforts to control zoonotic diseases, improve monitoring and early warning systems, and increase diagnostic capacity. However, A recent study reveals that during the period from 2004 to 202023, the number of reported cases in China exhibited an upward trend year by year. On the one hand, with the implementation of population screening programs, the awareness among residents of seeking medical attention proactively has been significantly augmented. This, in turn, has elevated the likelihood of case detection and led to a continuous expansion of the regions where cases are distributed. On the other hand, relevant medical institutions have stepped up their efforts in reporting echinococcosis cases. In China, the comparatively large number of reported cases in Xinjiang might potentially be attributed to the repeated reporting of past cases in the local area. Conversely, the relatively scant number of reported cases in Tibet is at odds with the actual local epidemic situation, making it imperative to reinforce the management of case reporting. In recent years, as indicated by reference24, the number of reported cases in non-endemic areas has been on a steady annual increase. Field epidemiological investigation results, as shown in references25 – 27, suggest that the majority of these are imported cases, although there are suspected locally infected cases in certain provinces. This implies that there could be latent endemic areas of echinococcosis in China. The increase in population migration due to work, tourism, and labor, as well as the circulation of livestock and other products between regions, may pave the way for the spread of echinococcosis from pastures to agricultural and urban areas28. The findings of epidemiological investigations into reported suspected locally infected cases demonstrate that, for the moment, no infected dogs have been detected and the cases are scattered sporadically. Nevertheless, some of the local livestock originate from endemic areas. People may become infected after inadvertently ingesting eggs carried by the hides of livestock. Alternatively, the disease might spread as a result of feeding diseased organs to dogs. All the aforementioned unstable factors will substantially augment the difficulty in forecasting the disease burden of cystic echinococcosis in the future.It is thus recommended that while implementing prevention and treatment measures for echinococcosis and enhancing public health awareness, the quarantine of host animals hailing from endemic areas should be tightened, the cross-regional movement of infected animals should be curbed, and the spread of echinococcosis should be averted.
The joinpoint sex-stratified analysis revealed that cystic echinococcosis imposes a greater disease burden on males than on females in China. This disparity may be attributed to the emphasis on economic development in animal husbandry, as well as the influence of age and occupational characteristics on the distribution of echinococcosis in the region29, 30. A significant proportion of young and middle-aged individuals in China are engaged in production and processing activities related to animal husbandry and fur, increasing their exposure to livestock. This, combined with poor working conditions, insufficient personal protective measures, and a lack of knowledge regarding echinococcosis prevention and treatment, contributes to a higher incidence and prevalence of cystic echinococcosis (CE). Moreover, over the past few decades, the incidence of canine cystic echinococcosis has been witnessing a continuous upward trend on a global scale. In the context of China, the distribution of dog breeding activities is considerably extensive. Dogs serve not only as the predominant option for individuals in pet-keeping but also constitute the principal domestic animals for safeguarding residences in grassroots regions. Particularly in numerous agricultural and pastoral areas, dog breeding prevails to a greater extent. Consequently, canine cystic echinococcosis exhibits a relatively broad epidemic scope. Once an outbreak occurs, there is a high propensity for the formation of an epidemic area, thereby giving rise to regional hazards31. Upon conducting investigations into the epidemic regions of canine cystic echinococcosis in recent years, it has been ascertained that the prevalent factors contributing to the spread of this disease primarily stem from breeders’ inadequate knowledge regarding canine cystic echinococcosis and their relatively weak preventive awareness. Irrespective of whether it pertains to small-scale backyard breeders or large-scale commercial farms, the traditional extensive management paradigm adopted by breeders throughout the breeding process has substantially exacerbated the occurrence of this ailment32.To effectively control cystic echinococcosis, it is essential to restrict sources of infection, enhance the management of livestock production, and promptly identify and eliminate sources of infection. Additionally, grassroots governments should actively cooperate with relevant departments such as grassroots epidemic prevention departments and veterinary departments to carry out publicity work on canine cystic echinococcosis. This can truly make breeders aware of the harm of canine cystic echinococcosis, so that they will attach importance to the prevention of this disease in terms of ideology.
The results from the Joinpoint age stratification analysis indicated significant disparities in incidence and prevalence across different age groups, with similar trends observed in both metrics. The highest incidence and prevalence rates were recorded in the 10–24 years age group, whereas the lowest rates were found in the 0–9 years age group. Fatalities and DALY rates associated with cystic echinococcosis in China increased with age, with the 70 + age group exhibiting the highest rates. This trend can be attributed to the chronic nature of CE and the low sense of self-protection among young children in animal husbandry areas, which are influenced by their unique lifestyles and environmental factors. These conditions lead to frequent exposure to animals and a greater likelihood of infection with echinococcal tapeworms, with the probability of morbidity and prevalence increasing with age as cumulative exposure increases. This aligns with previous studies conducted by researchers such as Yu Wenjie and Wang Qian33. The disease burden in the 70 + age group is exacerbated by age-related immune system decline. Therefore, it is crucial to strengthen disease prevention education for young children and guardians of elderly individuals in western animal husbandry regions, improve awareness of disease prevention, and promote healthy living habits to effectively control infection sources34. Furthermore, centralizing the management of livestock waste is vital to prevent the establishment of infection chains due to contact, while accelerating immunization efforts in these regions will help reduce infection rates and mitigate the impact of Echinococcus species on human health.
The findings of this study demonstrate that cystic echinococcosis mortality and DALY rates in China have shown a consistent decreasing trend since 1990; however, a significant increase was observed from 2016 to 2019. This increase is attributable primarily to large-scale population screening initiatives, improved reporting of echinococcosis by healthcare organizations35, and the identification of expanded areas affected by the disease owing to increased human‒livestock contact15. According to Nordpred model predictions, the incidence, prevalence, and DALY rates of cystic echinococcosis in China are projected to increase slightly between 2020 and 2044. As previously reported, the number of cases in non-endemic provinces has been on the upswing23, and this upward trend is anticipated to endure28. Likely, the rise in case numbers can be ascribed, firstly, to the improved detection rate of cystic echinococcosis brought about by screening initiatives and the public’s growing propensity to seek healthcare. Secondly, the bolstered awareness of hospitals and county-level disease control centers in reporting notifiable diseases and cases is also a contributing factor of significance. Achieving these projections will require heightened national attention to prevention and treatment efforts for cystic echinococcosis, as well as improvements in healthcare capacity and public health awareness. This will increase the likelihood of detecting previously asymptomatic or undiagnosed cases and accurately reflect the current state of underdiagnosed cystic echinococcosis.
Because the data in this study came from the 2019 GBD database, the data are provided by the burden of disease on a country-by-country basis, and the level of health care in different provinces and regions varies greatly. The data may be imperfect and inaccurate, resulting in discrepancies between the results of the study and the actual situation in China, and further research is needed to validate the study in the future. Furthermore, our projections extending up to 2044, while firmly grounded in rigorous statistical models, nonetheless hinge upon specific assumptions that could potentially be swayed by external factors. Moreover, the historical scope of our research, which incorporates data dating back to 1990, is liable to have been impacted by the continuous evolution of diagnostic criteria and medical technologies throughout the years.
Data availability
This data has been provided in the supplementary document.
References
Agudelo Higuita, N. I., Brunetti, E. & McCloskey, C. Cystic echinococcosis. J. Clin. Microbiol. 54, 518–523 (2016).
Kirigia, J. M. & Mburugu, G. N. The monetary value of human lives lost due to neglected tropical diseases in Africa. Infect. Dis. Poverty. 6, 165. https://doi.org/10.1186/s40249-017-0379-y (2017).
McManus, D. P., Zhang, W., Li, J. & Bartley, P. B. Echinococcosis Lancet 362: 1295–1304. doi:https://doi.org/10.1016/S0140-6736(03)14573-4. (2003).
Moro, P. & Schantz, P. M. Echinococcosis: a review. Int. J. Infect. Dis. Mar. 13 (2), 125–133 (2009).
McManus, D. P., Gray, D. J., Zhang, W. & Yang, Y. Diagnosis, treatment, and management of echinococcosis. BMJ (Clinical research ed.), 344, e3866. (2012). https://doi.org/10.1136/bmj.e3866
Qucuo, N. et al. Knowledge, attitudes and practices regarding echinococcosis in Xizang Autonomous Region, China. BMC Public. Health. 20 (1), 483. https://doi.org/10.1186/s12889-020-8314-8 (2020).
Cadavid Restrepo, A. M. et al. The landscape epidemiology of echinococcoses. Infect. Dis. Poverty. 5, 13. https://doi.org/10.1186/s40249-016-0109-x (2016).
Fu, M. H. et al. Advances in research on echinococcoses epidemiology in China. Acta Trop. 219, 105921doi. https://doi.org/10.1016/j.actatropica.2021.105921 (2021).
Budke, C. M., Deplazes, P. & Torgerson, P. R. Global socioeconomic impact of cystic echinococcosis. Emerg. Infect. Dis. 12 (2), 296–303. https://doi.org/10.3201/eid1202.050499 (2006).
Yin, J., Wu, X., Li, C., Han, J. & Xiang, H. The impact of environmental factors on human echinococcosis epidemics: spatial modelling and risk prediction. Parasites Vectors. 15 (1), 47. https://doi.org/10.1186/s13071-022-05169-y (2022).
Flisser, A. Eliminating cystic echinococcosis in the 21st century. Lancet Infect. Dis. 18 (7), 703–704. https://doi.org/10.1016/S1473-3099(18)30299-8 (2018).
Kui, Y. et al. Progress of national echinococcosis control in 2022[J]. Chin. J. Parasitol. Parasitic Dis. 42 (01), 8–16 (2024).
World Health Organization. Ending the neglect to attain the Sustainable Development Goals: A road map for neglected tropical diseases 2021–2030. -2021. 2030. (2021).
Widdicombe, J. et al. The economic evaluation of cystic echinococcosis control strategies focused on zoonotic hosts: a scoping review. PLoS Negl. Trop. Dis. 16 (7), e0010568. https://doi.org/10.1371/journal.pntd.0010568 (2022).
Wen, H. et al. Echinococcosis: advances in the 21st Century. Clin. Microbiol. Rev. 32 (2), e00075–e00018. https://doi.org/10.1128/CMR.00075-18 (2019).
Zhou, J. J. et al. Zhonghua Liu Xing Bing Xue Za Zhi = Zhonghua liuxingbingxue zazhi, 45(9), 1197–1203. (2024). https://doi.org/10.3760/cma.j.cn112338-20240312-00117
Arnold, M. et al. Is gastric cancer becoming a rare disease? A global assessment of predicted incidence trends to 2035. Gut 69, 823–829 (2020).
Luo, G. et al. Projections of lung cancer incidence by 2035 in 40 countries worldwide: population-based study. JMIR Public. Health Surveill. 9, e43651 (2023).
Yang, Z. et al. Changes in the global epidemiological characteristics of cystic echinococcosis over the past 30 years and projections for the next decade: findings from the global burden of Disease Study 2019. J. Global Health. 14, 04056. https://doi.org/10.7189/jogh.14.04056 (2024).
Wang, Q. et al. From endemic to basically under control: a 40-Year review of Echinococcosis Prevention and Control in Sichuan Province [J]. Chin. J. Parasitol. Parasitic Dis. 39 (02), 133–138 (2021).
Wang, J. X. et al. Report on the Prevention and Control of Hydatid Disease among Livestock in Ningxia in 2016 [J]. China Anim. Health. 19 (7), 69–71 (2017).
Jin Suyaladailai. Epidemiology, Pathogenic Characteristics and Prevention and Control Measures of Hydatid Disease in Sheep [J]. China Anim. Health. 25 (12), 1–2 (2023).
Han, S. et al. The endemic status of echinococcosis in China from 2004 to 2020. Chin. J. Parasitol. Parasit. Dis. 40 (4), 475–480. https://doi.org/10.12140/j.issn.1000-7423.2022.04.009 (2022).
Han, S., Wu, W. P. & Xue, C. Z. Analysis of echinococcosis cases from non-endemic areas of China in 2017 [J]. J. Pathog Biol. 14 (8), 901–904 (2019).
Zhang, S. R. et al. Clinical analysis of 5 cases of hepatic alveolar echinococcosis in non -endemic areas [J]. Chongqing Med. 40 (29), 2998 (2011).
Shi, Y. H. Clinical analysis of five local cases of hydatidosis in non-epidemic region of Mianyang in Sichuan Province [J]. J. Prev. Med. Inf. 34 (1), 41–43 (2018).
Jiang, C. P. Cysticohydatids of human and animal species have been found scattered in non-endemic areas in China in the past 10 years [J]. Chin. J. Epidemiol. 23 (6), 491 (2002).
Kui, Y. et al. Epidemiological Characteristics of Echinococcosis in Non-Endemic PLADs - China, 2017–2020. China CDC Wkly. 3 (51):1084–1088. doi:10.46234/ccdcw2021.262.
Chen, D., Liu, X.l., Liu, X.g. & Chen, X.g. (2011) Research progress on the epidemic trend of brucellosis and its control measures[J]. Chinese Journal of Endemic Disease Control, 26(01):26–28. (2011).
Gong, Y. J. et al. Serologic survey of brucellosis in Guangzhou City in 2014. South. China Prev. Med. (05), 468–469. https://doi.org/10.13217/j.scjpm.2016.0468 (2016).
Qi Xuanjie, X. & Shitian Prevention Strategies for Canine echinococcosis [J]. Jilin J. Anim. Husb. Veterinary Med. 45 (03), 160–162 (2024).
Renqing Zhuoma. Investigation Report on the Efficacy of Hydatid Disease Prevention and Control among Livestock in Gonghe County [J]1731–32 (China Livestock & Poultry Breeding, 2021). 11.
Yu, W. J. et al. ).2019 epidemiologic survey of echinococcosis in Seda County, Sichuan Province. Chin. J. Schistosomiasis Control. (06), 623–625. https://doi.org/10.16250/j.32.1374.2021194 (2021).
Yuting, W. X. X., Jing, D. & E., & Current status of cysticercosis and progress of candidate antigens for canine adult worm vaccine[J]. Chin. J. Veterinary Med. 44 (02), 403–412 (2024).
Shuai, H., Yan, K. & Chuizhao, X. Analysis of the national epidemic of echinococcosis from 2004 to 2020. Chin. J. Parasitol. Parasitic Dis. 40 (04), 475–480 (2022).
Acknowledgements
The authors thank Xinjiang Medical University for supporting this study.
Funding
This study was supported in part, by the 2023 Open Subjects of State Key Laboratory of Causes and Prevention of High Morbidity in Central Asia, jointly constructed by the Ministry and Provincial Government of China(SKL-HIDCA-2023-8).
Author information
Authors and Affiliations
Contributions
Jingjing Wei carried out the macro-design and supervision and guidance, and Jianping Li carried out the data collection and analysis, as well as the writing of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Wei, J. Trends in the disease burden of cystic echinococcosis in China, 1990–2044 analysis and forecasting study. Sci Rep 15, 4812 (2025). https://doi.org/10.1038/s41598-025-88403-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88403-8
