
Abstract
AIT (autoimmune thyroiditis) is a complex disease influenced by genetic and environmental factors as well as immune dysregulation. Epigenetics has unveiled potential connections among environmental factors, gene expression and thyroid autoimmunity. Among epigenetic modifications, DNA methylation is the first discovered and the most extensively-studied. Investigations both domestically and internationally indicate that iodine supplementation in areas with either excessive or insufficient iodine levels increases the incidence of AIT. Chemokines also play a crucial role in the pathogenesis of AIT. Therefore, does iodine influence the DNA methylation of chemokine genes of patients with AIT, and what are the potential mechanisms involved?. Healthy controls and patients with AIT were matched at the ratio of 1:1 according to age, sex, BMI and residential address, and a total of 176 patients with AIT together with 176 controls were included from regions with varying iodine levels. DNA methylation and mRNA expression levels were analyzed in whole blood using MethylTarget and qRT-PCR methods. At the same time, the GSE138198 and GSE54958 datasets were downloaded from GEO to obtain transcriptional datasets of thyroid tissues from patients with AIT. AIT patients had lower DNA methylation levels in CCL5_2 and CXCL8_1 target regions than controls, while the mRNA expression of CCL5 and CXCL8 genes was significantly higher. A negative correlation was found between the DNA methylation of CCL5_2 and its CpG sites as well as CCL5 gene expression. Higher CCL5 mRNA expression was validated in the thyroid tissues of patients with AIT using GSE datasets. DNA methylation differences at different iodine levels were mainly observed in CCL5_1, CCL5_2, CXCL8_1 and CXCR5_1. CXCL8_1 showed a positive correlation with UIC (urinary iodine concentration). This study demonstrates an association between the DNA methylation status of CCL5 and CXCL8 genes and AIT. The DNA methylation level of the CCL5 gene can serve as an epigenetic marker and biological indicator for AIT. Additionally, long-term iodine deficiency supplementation has a more pronounced impact on the DNA methylation levels of CCL5 and CXCL8 genes.
Similar content being viewed by others

Introduction
Iodine, an essential trace element for the human body, serves as a crucial raw material in the synthesis of thyroid hormones1, playing a vital role in maintaining the overall health2. Currently, approximately 88% of the global population resides are in regions covered by iodized salt3. While iodine deficiency disorders have been controlled, the incidence of excessive iodine intakes is on the rise worldwide4,5. In certain regions of China, the consumption of high-iodine drinking water is also considered a major factor contributing to excessive iodine intakes6,7, which can lead to hyperthyroidism, hypothyroidism, goiter and AIT8. Prolonged exposures to excessive iodine can trigger AIT, partly due to the increased immunogenicity of thyroglobulin induced by high iodine levels. The commonly-used method for salt iodization can also yield effects9. Findings from surveys conducted both domestically and internationally indicate that iodine supplementation in regions with excessive or deficient iodine levels can increase the incidence of AIT10,11. Therefore, conducting research on the relationship between environmental iodine exposure and the pathogenesis of AIT is of significant importance.
AIT, also known as HT (Hashimoto’s thyroiditis) or chronic lymphocytic thyroiditis, is the most common type of AITD (autoimmune thyroid diseases)12. The hallmark feature of AIT is lymphocytic infiltration, particularly T cell infiltration, leading to follicular destruction and subsequent hypothyroidism13. Globally, the incidence of AIT is estimated to be 0.3–1.5 cases per 1000 individuals per year, affecting approximately 2% of the world’s population14. While the exact mechanisms remain incompletely understood, the pathogenesis of AIT is believed to result from a combination of environmental and genetic factors leading to immune dysregulation15. The immune dysregulation in AIT is primarily driven by the activation of self-reactive CD4+ T cells, which include helper T cells (Th1, Th2, Th17, etc.) and Treg (regulatory T cells)16.
Cytokines and chemokines play crucial roles in the immunopathogenesis of AIT. Within thyroid tissues, recruited Th1 cells may be responsible for promoting the production of IFN-γ and TNF-α, thereby stimulating the secretion of CXCL10 and other IFN-γ-dependent chemokines from thyroid cells. This sets up an amplification loop that initiates and sustains the autoimmune process17. Chemokines, a class of cytokines with chemotactic properties, ranging from 8-14Kd in size, induce the migration of immune cells during inflammatory responses, guiding these cells to inflammation sites where their functions can be exerted. Based on a conserved amino-terminal cysteine motif, chemokines are classified into the CC, CXC, CX3C and C subfamilies18.
Epigenetics provides a potential link among environmental influence, gene expression and thyroid autoimmunity19, playing a significant role in many autoimmune diseases20,21,22. Research on epigenetics primarily encompasses DNA methylation, the post-translational modifications of histones, chromatin, microRNAs, siRNAs and other related factors23. Shalaby et al. found that hypomethylation in the promoter region of the ICAM-1 gene induced the upregulation of ICAM-1 expression, contributing to the pathogenesis of AIT24. Furthermore, research has shown that the occurrence of AIT among children and adolescents is associated with the DNA methylation status of the PTN22 gene promoter region25. DNA methylation is the first-discovered epigenetic modification and the most extensively-studied form of epigenetic modification, which refers to a process through which the fifth carbon atom of cytosine in CpG (cytosine-phosphate-guanine) dinucleotides is methylated under the action of DNA methyltransferases, resulting in the formation of 5-mC (5-methylcytosine)26,27. DNA methylation is often described as a repressive epigenetic mark.
In conclusion, research on the DNA methylation of AIT-related chemokine genes at different iodine levels will undoubtedly advance our understanding of the pathogenesis of AIT, which can furthermore guide molecular diagnostics, facilitate the development of novel therapeutic approaches and provide a theoretical basis for scientific iodine supplementation. Therefore, this case-control study aimed to investigate the methylation patterns of candidate chemokine genes in whole blood samples obtained from individuals with AIT and health controls residing at regions with different iodine levels in Shandong Province. Subsequently, we further validated the mRNA expression levels of CXCL8 (C-X-C motif ligand 8) and CCL5 (C-C chemokine ligand 5) chemokine genes and explored the correlations between methylation and mRNA levels. To obtain more compelling evidence, we retrieved gene sets GSE138198 and GSE54958 from the GEO database to validate the expression of candidate chemokine factor genes in the thyroid tissues of patients with AIT.
Materials and methods
Survey areas and survey participants
Based on the monitoring data on iodine deficiency disease and the investigation data on high-iodine areas in water sources nationwide in recent years, combined with the iodized salt coverage rate, the following three areas have been selected as investigation sites: (1) Iodine-fortification areas (IFAs): Qianlv Village and Dongtan Village in Jining City, Shandong Province (water iodine level < 10 µg/L, iodine salt coverage rate > 90%); (2) Iodine-adequate areas (IAAs): Liuxiangzhuang Village and Dongding in Jining City, Shandong Province (water iodine level 40–100 µg/L, non-iodine salt supplied); (3) Iodine-excessive areas (IEAs): Jieyuanji Village in Heze City, Shandong Province (water iodine level > 100 µg/L, non-iodized salt supplied). A total of 1225 subjects were included in the AIT screening, including 409 from IFAs, 392 from IAAs and 424 from IEAs28. All subjects provided a written informed consent, and the study was approved by the Ethics Review Committee of Harbin University (hrbmuecdc20200320) and conducted in accordance with the Helsinki Declaration. Selection criteria for adult participants were: (1) Age over 18; (2) Residing in the selected area for more than 5 years. Exclusion criteria included: (1) Pregnant women; (2) Patients with acute or chronic diseases, congenital thyroid disorders or other autoimmune diseases; (3) Consumption of iodine-rich foods within the last three days; (4) Use of antithyroid medications or hormonal treatments in the past year. The diagnosis criteria for AIT were positive serum TPOAb (thyroid peroxidase antibody) and/or TgAb (thyroglobulin antibody) with thyroid dysfunctions or subclinical thyroid dysfunctions. The healthy controls were matched with patients with AIT at a ratio of 1:1 based on age, gender, BMI and residence. A total of 176 patients with AIT and 176 controls were finally included in this study, including 89 cases and 89 controls from IFAs, 40 cases and 40 controls from IAAs, as well as 47 cases and 47 controls from IEAs.
Testing indicators and laboratory testing methods
All urine samples of the subjects were collected on site, placed in sealed plastic tubes and stored at 4 °C. Urinary iodine was determined using the As3+-Ce4+ catalytic spectrophotometry method (WS/T 107.1–2016) in according with Chinese National Health Standards. After 8 h in an empty stomach, venous blood samples were collected from the subjects, and serum was separated through centrifugation at 3000 g and stored at -80 °C. Serum iodine concentration was determined using the inductively-coupled plasma mass spectrometry (ICP-MS) system (PerkinElmer NexION 350) with a reference range of 52–109 pmol g/L. Serum FT3 (free triiodothyronine3), FT4 (free thyroxine), TSH (thyroid-stimulating hormone), TPOAb and TGAb were detected using an immunochemiluminescent procedure (the test kit was bought from Siemens Healthcare Diagnostics Lnc, America). The reference ranges were as follows: FT3, 3.1–6.8 pmol/L; FT4, 11.5–22.7 pmol/L; TSH, 0.27–4.2 µIU/mL; TPOAb, 0–60 U/mL; and TgAb, 0–60 U/mL.
DNA extraction and the detection of DNA methylation
Genomic DNA was extracted from whole blood using a TIANGEN gel extraction kit (TIANGEN) under the manufacturer’s instructions and stored at -80 °C before detecting DNA methylation. Sample quality control: A. sample type: intact, uncontaminated genomic DNA; B. sample quality requirements: The quality of genomic DNA was assessed using a Nanodrop 2000 (Nano Drop Technologies, USA) according to the following criteria: concentration should be ≥ 400ng, and the sample purity should meet the following parameters: OD260/280 = 1.7–1.9 and OD260/230 ≥ 2.0; C. sample integrity: agarose gel electrophoresis analysis, requiring a clear main band with no significant smearing or trailing. The MethylTarget (Genesky Corporation, Shanghai, China), developed using a second-generation sequencing platform, allows for the simultaneous capture sequencing of multiple specific CpG islands. With high-depth sequencing data, it enables the quantitative detection of methylation levels at each CpG site. Based on the previous Illumina Methylation EPIC 850k Beadchip analysis results of our research group, we found the differential methylation of chemokine-related genes between patients with AIT and healthy controls29. Therefore, in combination with relevant literatures, we ultimately chose 4 chemokine-related genes as candidate genes: CCL5, CXCL8, CXCR5 (C-X-C motif chemokine receptor 5) and CXCL14 (C-X-C motif chemokine ligand 14) and validated them by expanding the samples through the MethylTarget technology. The primer sequences of CCL5, CXCL8, CXCR5 and CXCL14 are shown in Supplementary Table 1.
Total RNA extraction and the detection of mRNA expression
According to the instructions provided by Takara (Dalian, China), we extracted the total RNA from whole blood using a Trizol reagent as well as measured RNA concentration and purity using a NanoDrop 2000 C spectrophotometer r (NanoDrop Technologies, USA), taking the absorbance ratio at 260–280 nm (A260/280 = 1.8-2.0). Next, we performed a reverse transcription using a PrimeScript™ RT kit with a gDNA eraser (TAKARA BIO INC). Finally, we used a SYBR green kit (Roche Diagnostics GmbH) to detect the expression levels of the CXCL8 and CCL5 genes in real-time quantitative polymerase chain reactions on a QuantStudio 5 platform (AB Applied Biosystems, USA). The PCR reaction was carried out according to the following conditions: hold stage: step 1, 95 °C 10 min; PCR stage (forty cycles): step 1, 95 °C 15 s, step 2, 60 °C 1 min; melt curve stage: step 1, 95 °C 15 s, step 2, 60 °C 1 min, step 3, 95 °C 15 s. We used the 2−△△ CT method to normalize the relative expression levels of CCL5 and CXCL8 using endogenous controls. The forward and reverse sequences of CCL5, CXCL8 and β-actin are shown in Supplementary Table 2.
Acquisition of expression spectrum data
We acquired the GSE13898 and GSE54958 datasets from NCBI-GEO, both of which were analyzed using a GPL6244[hugene-1_0-st] Affymetrix human gene 1.0 ST array [transcript (gene version)] to examine gene expression. Since these datasets originate from the same microarray platform, they can be merged and are subjected to data normalization. The GSE138198 dataset comprises 13 cases of HT, 3 cases of normal thyroid, 12 cases of papillary thyroid carcinoma (PTC) and 8 cases of PTC with concurrent HT. The GSE54958 dataset consists of 7 normal thyroid specimens and 25 papillary thyroid carcinoma specimens.
The GSE138198 and GSE54958 datasets have been normalized. Clinical information from the sample data on the expression matrix was extracted for subsequent sample classifications. These two datasets were merged based on gene ID, and batch effects were eliminated using the SVA package and combat function of R. After processing, we obtained a final dataset comprising 10 normal thyroid samples as the control group and 12 HT samples as the case group. This dataset will be utilized to validate the mRNA expression levels of candidate chemokine genes in thyroid tissues.
Statistical analysis
This study employed SPSS (version 13.0) and GraphPad Prism (version 8.0.1) software for statistical analyses and graphing. Continuous data that conformed to a normal distribution was expressed as mean ± standard deviation (SD). Student’s t test was used for comparisons between two groups, while one-way ANOVA was employed for comparisons among multiple groups. LSD (Least Significant Difference) test was used for pairwise comparisons if there were significant differences among multiple groups. Non-normally-distributed data was analyzed using the Mann-Whitney U test, with median and interquartile range (IQR) used to describe the results. DNA methylation = the number of methylated reads at the site (i.e., the number of reads detecting the base C) / the total number of reads at the site. The relationship between candidate gene methylation levels and age, UIC, SIC, FT3, FT4 as well as TSH was explored using the Pearson correlation or the Spearman rank correlation. Analyses of GSE13898 and GSE54958 datasets were completed through R(Version 4.3.1). P < 0.05 was considered statistically significant, and all calculated P values were two-sided.
Results
The characteristics of research subjects
Based on different iodine levels of the regions, 352 subjects were divided into 3 groups. The data on gender, age, BMI, UIC, SIC, TSH, FT3, FT4, TGAb+, TPOAB+ and TPOAb+ & TGAb+ of the AIT group and the control group is shown in Table 1.
Methylation levels of candidate genes in AIT and controls
This study detected the methylation levels of 4 candidate genes, covering 5 target regions and a total of 75 CpG methylation sites. Among these 5 target regions, the methylation levels of target regions CCL5_2 and CXCL8_1 in the AIT group were lower than those in the control group (80.2 ± 6.2 vs. 82.1 ± 4.9, P = 0.002; 24.6 ± 1.1 vs. 25.0 ± 1.3, P = 0.003). The DNA methylation differences in target regions CCL5_1, CXCR5_1 and CXCL14_1 were not statistically significant between patients with AIT and controls (P > 0.05) (Table 2).
Supplementary Tables 3 and Fig. 1 show that among the associated CpG sites, 1 CpG site in the CCL5_1 target region shows lower methylation (P < 0.05), while the methylation levels of 2 CpG sites are higher than those of the control group (P < 0.05). In CCL5_2, the methylation levels of all CpG sites are lower than those of the control group (P < 0.05). In CXCL8_1, 1 CpG site shows a higher methylation level than that of the control group (P < 0.05), while the methylation levels of 8 CpG sites are lower than those of the control group (P < 0.05). The methylation levels of 3 CpG sites in CXCR5 and 1 CpG site in CXCL14_1 are lower than those of the control group (P < 0.05). The methylation level of 1 CpG site in CXCL14_1 is higher than that of the control group (P < 0.05).

DNA methylation levels of CpG sites between cases and controls. (A) CCL5_1; (B) CCL5_2; (C) CXCL8_1; (D) CXCR5_1; (E) CXCL14_1.
Methylation levels of candidate genes between AIT and controls in three areas
According to Table 3, the methylation levels of the CCL5_2, CXCL8_1 and CXCR5_1 target regions in IFAs are significantly lower than those of the control group (78.6 ± 6.2 vs. 82.0 ± 5.0, P < 0.001; 24.5 ± 1.1 vs. 25.2 ± 1.3, P < 0.001; 95.4 ± 0.4 vs. 95.5 ± 0.4, P = 0.035). In IAAs, the methylation level of CCL5_1 is higher than that in the control group (96.3 ± 0.6 vs. 95.9 ± 0.8, P = 0.011). In IEAs, the methylation level of CCL5_1 is lower than that in the control group (96.0 ± 0.8 vs. 96.5 ± 0.8, P = 0.008).
Supplementary Tables 4 and Fig. 2 show that in IFAs, the methylation levels of the CCL5_1 target region at 4 CpG sites and that of the CXCL14_1 target region at 2 CpG sites are higher than those in the control group (P < 0.05). Meanwhile, the methylation levels of all CpG sites in CCL5_2, 6 CpG sites in CXCL8_1 and 4 CpG sites in CXCR5_1 are lower in the AIT group than in the control group (P < 0.05). In IAAs, the methylation levels of 6 CpG sites in CCL5_1 and 1 CpG site in the CXCL8_1 target region are higher than those in the control group (P < 0.05). In IEAs, the methylation levels of 6 CpG sites in CCL5 _1 and 1 CpG site in CXCL14_1 are lower than those in the control group (P < 0.05). Meanwhile, the methylation levels of 1 CpG site in the CXCL14_1 target region, 2 CpG sites in CXCL8_1 and 1 CpG site in CXCR5_1 are higher than those in the control group (P < 0.05).

(A) Result of CCL5_1 CpG sites DNA methylation in iodine-adequate areas (IAAs). (B) Result of CCL5_1 CpG sites DNA methylation in iodine-excess areas (IEAs). (C) Result of CCL5_2 CpG sites DNA methylation in IFAs. (D) Result of CXCL8_1 CpG sites DNA methylation in IFAs. (E) Result of CXCL14_1 CpG sites DNA methylation in IFAs.
We conducted further analyses on the DNA methylation differences in target regions and sites among AIT cases in regions with different iodine levels. As shown in Table 4, there are significant statistical differences in the methylation levels of CCL5_2, CXCR5_1 and CXCL14_1 target regions among AIT cases in areas with different iodine levels (P = 0.002, P = 0.025, P = 0.013). Further pairwise LSD tests revealed that in IFAs, AIT cases had lower methylation levels in CCL5_2 compared to those in IAAs and IEAs (78.6 ± 6.2 vs. 81.8 ± 6.1, P = 0.005; 78.6 ± 6.2 vs. 81.9 ± 5.6, P = 0.003). In CXCR5_1, AIT cases in IFAs and IAAs exhibited higher methylation levels than those in IEAs (95.4 ± 0.4 vs. 95.1 ± 0.4, P = 0.008; 95.3 ± 0.4 vs. 95.1 ± 0.4, P = 0.048). Additionally, the methylation levels of the CXCL14_1 of AIT cases in IFAs were higher than those in both IAAs and IEAs (3.0 ± 1.0 vs. 2.4 ± 1.1, P = 0.008; 3.0 ± 1.0 vs. 2.6 ± 1.2, P = 0.038). The methylation differences in CpG sites are shown in Supplementary Table 5. A comparison of the 3 groups of cases show that there are significant methylation differences in 15 CpG sites of the CCL5 gene, 1 CpG site of the CXCL8 gene, 3 CpG sites of the CXCR5 gene and 8 CpG sites of the CXCL14 gene. Further pairwise LSD tests revealed that compared with IAAs and IEAs, the CCL5 gene in IFAs exhibited low methylation at 12 CpG sites while demonstrated high methylation at 2 CpG sites; the CXCL8 gene showed low methylation at 1 CpG site; and the CXCL14 gene exhibited high methylation at 3 CpG sites. Comparing IFAs with IEAs, the CXCR5 gene in IAAs showed low methylation at 2 CpG sites. In comparison to IAAs, CXCL14 in IFAs exhibited high methylation at 1 CpG site. Compared to IEAs, the CCL5 gene in IFAs displayed high methylation at 1 CpG site; the CXCR5 gene in IFAs demonstrated low methylation at 1 CpG site; and the CXCL14 gene in IFAs demonstrated a high methylation level at 4 CpG sites.
Correlations of the DNA methylation levels of target regions of candidate genes with the SIC, UIC, age and thyroid function of patients with AIT
According to the results of the correlation analysis in Supplementary Tables 6 and Fig. 3, there were no significant correlations observed between the DNA methylation levels of target regions CCL5_1, CCL5_2, CXCL14_1, CXCR5_1 and SIC, UIC, FT3, FT4, TSH. However, a negative correlation was found between the methylation levels of CCL5_2 and CXCR5_1 target regions and age (r:-0.309, P < 0.001; r:-0.217, P = 0.004), while a positive correlation was observed between the methylation levels of the CXCL14_1 target region and age (r:0.335, P < 0.001). Furthermore, the methylation level of the CXCL8 _1 target region showed a positive correlation with UIC (rs:0.150, P = 0.049) but no significant correlation with SIC, age, FT3, FT4, or TSH.

Correlation between DNA methylation levels of candidate genes and the SIC, UIC, age, FT3, FT4 and TSH of patients with AIT.
Analysis of transcription levels of CCL5 and CXCL8 genes and their correlations with DNA methylation
According to Supplementary Tables 7 and Fig. 4A, the mRNA expression levels of CCL5 and CXCL8 genes are significantly higher among patients with AIT compared to those of the control group (1.391 ± 0.857 vs. 1.008 ± 0.020, P < 0.001; 1.506 ± 1.300 vs. 1.006 ± 0.013, P < 0.001). As shown in Supplementary Tables 8 and Fig. 4(B, C), a stratified analysis is performed to investigate the impact of different iodine levels in various regions. The results demonstrate that in IFAs, there is a significant increase in the mRNA level of the CCL5 gene among patients with AIT compared to that of the control group (1.513 ± 0.882 vs. 1.008 ± 0.017, P < 0.001). However, no such difference was observed in other regions. Moreover, in IFAs, IAAs and IEAs, patients with AIT exhibited a statistically-significant elevation in the mRNA level of the CXCL8 gene compared to the control group (1.553 ± 1.366 vs. 1.004 ± 0.007, P = 0.002; 1.510 ± 1.273 vs. 1.006 ± 0.013, P = 0.041; 1.468 ± 1.250 vs. 1.009 ± 0.018, P = 0.042). In order to investigate the relationship among the CCL5 gene, the CXCL8 gene of mRNA expression and their methylation, we conducted a Pearson correlation analysis. According to the results shown in Fig. 4(D, E, F), there is no correlation between the CCL5 gene mRNA expression and the methylation level of CCL5_1 (r:0.039, P = 0.665). However, we observed a significant negative correlation between the CCL5 gene mRNA expression and the methylation level of CCL5_2 (r:-0.313, P < 0.001). Additionally, all CpG sites of the CCL5_2 methylation level demonstrated a significant negative correlation with its gene mRNA expression (Supplementary Table 9). Furthermore, we found no correlation between the CXCL8 gene mRNA expression and the methylation level of CXCL8_1 (r:-0.078, P = 0.393).

(A) mRNA expression levels of CCL5 and CXCL8 between cases and controls. (B) The mRNA expression levels of CCL5 between cases and controls from areas with different water iodine levels. (C) The mRNA expression levels of CXCL8 between cases and controls from areas with different water iodine levels. (D) Scatter plots of mRNA expression levels and DNA methylation levels of CCL5_1. (E) Scatter plots of mRNA expression levels and DNA methylation levels of CCL5_2. (F) Scatter plots of mRNA expression levels and DNA methylation levels of CXCL8_1.
Revalidation of candidate gene transcription levels in thyroid tissues using the GSE dataset
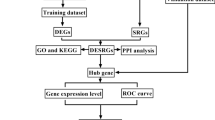
We initially performed quality checks on the data using the WGCNA R package without removing any sample (Supplementary Fig. 1). Subsequently, we identified DEGs (differentially-expressed genes) in HT using the criterion of |Log2FC|>2 and adjusted -P < 0.05. Only the CCL5 gene was included, and its mRNA expression level was found to be significantly higher than that in normal thyroid tissues (Log2FC = 2.064, adjust-P < 0.001). Additionally, Supplementary Table 10 provides individual characteristics of the participants.
Discussion
Certain environmental factors have been identified as risk factors of AIT, including radiation, smoking, infections, stress, medications and trace nutrients such as iodine, iron and selenium. Some reports suggest that smoking, iodine, infections and stress are associated with changes in DNA methylation19. The results of this study are consistent with previous research, indicating higher prevalence of AIT in regions with different iodine levels, showing higher rates in IFAs and IEAs compared to IAAs28. Additionally, variations in DNA methylation levels among patients with AIT were observed in regions with different iodine levels, particularly showing more significant impacts in iodine-deficient regions with iodine supplementation30.
The CC chemokine family is the largest subfamily of chemotactic factors, characterized by the presence of 4 cysteine residues in their molecular structure, with the first 2 cysteines adjacent to each other, hence terming the CC family. Members of the CC family recruit monocytes to inflammation sites. In the late stage of T cell activation, a significant increase in the expression of a gene is observed, known as RANTES (regulated on activation, with normal T cell expressed and secreted), also designated as CCL5 according to the systematic nomenclature of chemokines31. Many studies have reported increased expression levels of the CCL5 gene in the thyroid tissues of patients with AIT, while it is rarely expressed in non-autoimmune thyroid samples32,33. The levels of pro-inflammatory cytokines (IFN-γ and TNF-α) associated with RANTES induction were significantly elevated in patients with AIT compared to those of the control group. These pro-inflammatory cytokines stimulate the expression of the CC chemokine RANTES in endothelial cells, leading to a selective recruitment of circulating cells, indicating a similar role of the CCL5 gene produced in AIT to CXCL1034. In an 850 K methylation chip study on rheumatoid arthritis autoimmune diseases, researchers identified the CCL5 gene through a turquoise module based on a WGCNA analysis and a PPI-constructed network module. 2 CpG sites of this gene were found near the promoter region, which demonstrated a low methylation status35. These findings are consistent with the results of our study. In our study, the DNA methylation sites of candidate chemokine genes are predominantly located in the promotor regions and first exons (Supplementary Table 1). The CCL5_2 target region showed lower methylation in patients with AIT, and all CpG sites also exhibited a hypomethylated state. Our study also found a significant negative correlation between the DNA methylation level of the CCL5_2 target region (and all CpG sites within the CCL5_2) and the mRNA expression of the CCL5 gene in whole blood samples. These results suggest that the hypomethylation of the CCL5 gene may lead to increased mRNA expression, thus influencing the development of AIT.
Sequencing and microarray techniques, in conjunction with bioinformatics analyses, have proven to be effective for uncovering the molecular mechanisms of various diseases36. To provide strong evidence of candidate chemokines involved in AIT, we integrated transcriptomic datasets from thyroid tissues. Applying rigorous selection criteria, we discovered a significant upregulation of the CCL5 gene in the thyroid tissues of patients with AIT. These observations imply that CCL5 plays a role in the inflammatory response of thyroid tissues. However, to ensure the accuracy of these conclusions, further experiments and an expansion of the sample size are necessary.
A member of the CXC chemokine subfamily with an indeterminate amino acid residue X between the first 2 conserved cysteine residues is known as the CXC family. A subgroup of CXC chemokines has a characteristic ELR (glutamate-leucine-arginine) domain at the n-terminal of the molecule, also known as the CXC chemokine of ELR+, whose primary role is to recruit neutrophils to inflammation sites37. CXCL8, as one of the extensively-studied and earliest chemokines, which belongs to the ELR (Glu-Leu) -Arg+ CXC chemokine family, primarily functions as a pro-inflammatory chemotatic factor38. Rotondi et al.‘s study suggests that CXCL8 may be involved in tumor-related inflammation. In human thyroid cells, IFN-γ inhibits the secretion of CXCL8, while TNF-α stimulates it39. Muzza et al. found significantly-increased expression of the CXCL8 gene in PTC (papillary thyroid cancer) tissues40. These findings suggest that CXCL8 is associated with tumorigenesis rather than AIT41. However, these results contrast with our study, in which patients with AIT exhibited low levels of DNA methylation in the CXCL8 gene, accompanied by significantly-increased mRNA expression, especially in IFAs. But we did not find a correlation between DNA methylation levels and the CXCL8 gene mRNA expression, which might be due to the lower frequency of low methylation-dependent transcriptional activation compared to high methylation-dependent transcriptional silencing42. As we have studied, the effects of iodine on the CXCL8 gene are not taken into account in their study. Iodine positively regulates the expression of the CXCL8 gene, thereby attracting TNF-α into the thyroid gland43. TNF-α can also synergistically activate a large number of inflammation-related genes44, for example, in coordination with IFN-γ, the secretion of CXCL10 can be increased by 10 times43. Furthermore, in a study on the associations between different water iodine exposures and thyroid cancer in China, differences in the incidence of thyroid cancer at different water iodine levels were assessed, with the highest cumulative incidence of thyroid cancer being 86.61/100,000 (95% CI: 78.10-95.11) in iodine-deficient areas (0-40ug/L)45. Patients with AIT and nodular deformities are at the risk of PTC46. Based on the above, we speculated that under the influence of iodine intake, CXCL8 DNA methylation was abnormal among patients with AIT, and that this abnormal epigenetic modification regulated CXCL8 expression, which might explain the correlations between AIT and the increased incidence of thyroid cancer to a certain extent.
CXCR5, a member of the CXC chemokine receptor family initially discovered in Burkitt’s lymphoma, is also known as Burkitt’s lymphoma receptor 147,48. Studies have shown increased expression of CXCR5 in patients with AIT as well as their crucial role in maintaining ectopic follicles and lymphocytic infiltrates of B and T cells in thyroid tissues of patients with autoimmune diseases49. An analysis using an 850 K DNA methylation chip revealed CXCR5 as a gene exhibiting DNA methylation differences in patients with AIT, displaying lower levels of methylation compared to the control group. Further validation using MethylTarget™ confirmed that 3 CpG sites were also found to be hypomethylated in patients with AIT. Due to the low expression of the CXCR5 gene in whole blood, we did not detect its presence. In addition, 1 CpG site within the CXCL14_1 target region exhibited a high methylation status, while another displayed a low one. Based on these findings, it is suggested that CXCL14 DNA methylation may not play a significant role in the pathogenesis of AIT.
To investigate the impact of varying iodine levels on the DNA methylation of candidate genes, we conducted analyses based on the iodine levels across different regions. In IAAs, the methylation level of CCL5_1 in patients with AIT was hypermethylated. However, in IFAs, CCL5_2 exhibited hypomethylation and in IEAs, CCL5_1 also exhibited hypomethylation. These results indicate that long-term iodine deficiencies followed by supplementation and excessive iodine have similar effects on DNA methylation patterns. Additionally, in IFAs, CXCL8_1 is characterized by a hypomethylated state. We conducted further analyses of methylation levels in target regions and CpG sites among patients with AIT at different iodine levels. The results showed that in comparison to IAAs and IEAs, patients with AIT in IFAs exhibited significantly lower DNA methylation levels in the CCL5_2 target region and all CpG sites within the CCL5_2 target region. These findings suggest that iodine supplementation after long-term iodine deficiencies have more significant effects on the DNA methylation level of the CCL5 gene. When there is a serious lack of iodine in the external environment, its intake in the human body will be seriously insufficient, which will cause iodine deficiency diseases. In order to eliminate such diseases, China implemented nationwide salt iodization in 199650. However, our findings suggest that this background may have an impact on the DNA methylation of CCL5 and CXCL8 genes, which may play a role in the occurrence or development of AIT. UIC is a good indicator of iodine nutrition in human population. In a correlation analysis of DNA methylation and UIC, the DNA methylation level of CXCL8_1 was positively correlated with UIC. As shown in Table 1, UIC in IFAs is relatively lower than that in other regions, which again confirms our hypothesis that iodine intake may affect the expression of CXCL8 by altering its DNA methylation level. This also suggests that the safe threshold for iodine may not be as wide as previously understood. Iodine supplementation should be moderate, as the adverse consequences of excessive iodine intake are equally significant and should not be overlooked, similar to iodine deficiencies.
We also investigated the correlations of the DNA methylation levels of the target region with SIC, UIC, age, FT3, FT4 and TSH. In terms of age-related analyses, we observed a negative correlation between the DNA methylation levels of CCL5_2 and CXCR5_1, and a positive correlation in the DNA methylation levels of CXCL14_1. Previous studies have suggested that DNA methylation and certain CpG sites are highly correlated with age51,52. This finding may partially explain the increasing trend of AIT incidence with age.
Our study has the following strengths and limitations. Firstly, we are the first to explore the associations between the DNA methylation of chemokine genes and AIT. Additionally, we analyzed the impacts of environmental factors (iodine exposure in water) on the DNA methylation of candidate chemokine genes. However, other factors may also influence methylation changes in the population with AIT, including age, gender, pregnancy status, dietary habits, lifestyle and medication use. To minimize the effects of these confounding factors, patients with AIT and healthy controls were matched at a ratio of 1:1 based on age, gender and BMI. We also used residential matching as an inclusion criterion to eliminate potential confounding variables related to sociodemographics. Secondly, we validated the significance of candidate genes in the pathogenesis of AIT by integrating RNA-SEQ datasets from both patients with AIT and normal thyroid tissues. However, since these datasets were not collected by us, we were unable to assess the DNA methylation levels of candidate chemokine genes in thyroid tissues. Moreover, despite our efforts to homogenize and merge the datasets, issues regarding sample representativeness could not be completely avoided. Lastly, our study only provides preliminary insights into the relationship between chemokine DNA methylation and AIT. Further in vitro and in vivo experiments are required to validate the underlying mechanisms.
Conclusion
In summary, our study shows that the DNA methylation status of CCL5 and CXCL8 genes is related to AIT. The DNA methylation level of the CCL5 gene can be used as an epigenetic mark and biological indicator of AIT. Furthermore, long-term iodine deficiencies followed by iodine supplementation have a significant impact on the DNA methylation levels of CCL5 and CXCL8 genes, which suggests that iodine supplementation should be appropriate and attention should be paid to the adverse consequences of excessive iodine supplementation.
Data availability
For detailed data or any inquiries, please contact the corresponding author (shenhm119@hrbmu.edu.cn).
References
Cavalieri, R. R. Iodine metabolism and thyroid physiology: current concepts. Thyroid 7 (2), 177–181. https://doi.org/10.1089/thy.1997.7.177 (1997).
Zhang, J. & Lazar, M. A. The mechanism of action of thyroid hormones. Annu. Rev. Physiol. 62, 439–466. https://doi.org/10.1146/annurev.physiol.62.1.439 (2000).
Zimmermann, M. B. & Andersson, M. GLOBAL ENDOCRINOLOGY: global perspectives in endocrinology: coverage of iodized salt programs and iodine status in 2020. Eur. J. Endocrinol. 185 (1). https://doi.org/10.1530/eje-21-0171 (2021).
Zimmermann, M. B. Iodine deficiency and excess in children: worldwide status in 2013. Endocr. Pract. 19 (5), 839–846. https://doi.org/10.4158/ep13180.Ra (2013).
Zimmermann, M. B. & Andersson, M. Update on iodine status worldwide. Curr. Opin. Endocrinol. Diabetes Obes. 19 (5), 382–387. https://doi.org/10.1097/MED.0b013e328357271a (2012).
Lv, S. et al. Drinking water contributes to excessive iodine intake among children in Hebei, China. Eur. J. Clin. Nutr. 67 (9), 961–965. (2013).
Sui, H. X. et al. Dietary iodine intake in the Chinese population. Biomed. Environ. Sci. 24 (6), 617–623. https://doi.org/10.3967/0895-3988.2011.06.005 (2011).
Farebrother, J., Zimmermann, M. B. & Andersson, M. Excess iodine intake: sources, assessment, and effects on thyroid function. Ann. N Y Acad. Sci. 1446 (1), 44–65. https://doi.org/10.1111/nyas.14041 (2019).
Hu, S. & Rayman, M. P. Multiple nutritional factors and the risk of Hashimoto’s Thyroiditis. Thyroid 27 (5), 597–610. https://doi.org/10.1089/thy.2016.0635 (2017).
Miranda, D. M. et al. Impact of nutritional iodine optimization on rates of thyroid hypoechogenicity and autoimmune thyroiditis: a cross-sectional, comparative study. Thyroid 25 (1), 118–124. https://doi.org/10.1089/thy.2014.0182 (2015).
Flores-Rebollar, A. et al. Prevalence of autoimmune thyroiditis and thyroid dysfunction in healthy adult mexicans with a slightly excessive iodine intake.Nutr. Hosp. 32 (2), 918–924. https://doi.org/10.3305/nh.2015.32.2.9246 (2015).
Ralli, M. et al. Hashimoto’s thyroiditis: An update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmun. Rev. 19 (10). https://doi.org/10.1016/j.autrev.2020.102649 (2020).
Orgiazzi, J. Thyroid autoimmunity. Presse Med. 41 (12), 2. https://doi.org/10.1016/j.lpm.2012.10.002 (2012).
Caturegli, P. et al. Hashimoto’s thyroiditis: celebrating the centennial through the lens of the Johns Hopkins hospital surgical pathology records. Thyroid 23 (2), 142–150. https://doi.org/10.1089/thy.2012.0554 (2013).
Zaletel, K. & Gaberšček, S. Hashimoto’s Thyroiditis: from genes to the Disease. Curr. Genom. 12 (8), 576–588. https://doi.org/10.2174/138920211798120763 (2011).
Li, Y. et al. IL-9-Producing Th9 cells participate in the occurrence and development of Iodine-Induced Autoimmune Thyroiditis. Biol. Trace Elem. Res. 201 (11), 5298–5308. https://doi.org/10.1007/s12011-023-03598-z (2023).
Antonelli, A. et al. Autoimmune thyroid disorders. Autoimmun. Rev. 14 (2), 174–180. (2015).
Fang, Y., Zhao, L. & Yan, F. Chemokines as novel therapeutic targets in autoimmune thyroiditis. Recent. Pat. DNA Gene Seq. 4 (1), 52–57. https://doi.org/10.2174/187221510790410787 (2010).
Lafontaine, N., Wilson, S. G. & Walsh, J. P. DNA methylation in autoimmune thyroid disease. J. Clin. Endocrinol. Metab. 108 (3), 604–613. https://doi.org/10.1210/clinem/dgac664 (2023).
Chen, Z. et al. Epigenomic profiling reveals an association between persistence of DNA methylation and metabolic memory in the DCCT/EDIC type 1 diabetes cohort. Proc. Natl. Acad. Sci. U. S. A. 113 (21), E3002. https://doi.org/10.1073/pnas.1603712113 (2016).
Paul, D. S. et al. Increased DNA methylation variability in type 1 diabetes across three immune effector cell types. Nat. Commun. 7, 13555. https://doi.org/10.1038/ncomms13555 (2016).
Tahara, T. et al. Comprehensive DNA methylation profiling of inflammatory mucosa in Ulcerative Colitis. Inflamm. Bowel Dis. 23 (1), 165–173. https://doi.org/10.1097/mib.0000000000000990 (2017).
Li, Y. Modern epigenetics methods in biological research. Methods 187, 104–113. (2021).
Shalaby, S. M. et al. Promoter methylation and expression of intercellular adhesion molecule 1 gene in blood of autoimmune thyroiditis patients. Mol. Biol. Rep. 46 (5), 5345–5353. https://doi.org/10.1007/s11033-019-04990-6 (2019).
Kyrgios, I. et al. DNA hypermethylation of PTPN22 gene promoter in children and adolescents with Hashimoto thyroiditis. J. Endocrinol. Invest. 44 (10), 2131–2138. https://doi.org/10.1007/s40618-020-01463-7 (2021).
Du, J. et al. DNA methylation pathways and their crosstalk with histone methylation. Nat. Rev. Mol. Cell. Biol. 16 (9), 519–532. https://doi.org/10.1038/nrm4043 (2015).
Torres, I. O. & Fujimori, D. G. Functional coupling between writers, erasers and readers of histone and DNA methylation. Curr. Opin. Struct. Biol. 35, 68–75. https://doi.org/10.1016/j.sbi.2015.09.007 (2015).
Wan, S. et al. Autoimmune thyroid diseases after 25 years of universal salt iodisation: an epidemiological study of Chinese adults in areas with different water iodine levels. Br. J. Nutr. 124 (8), 853–864. https://doi.org/10.1017/s0007114520001786 (2020).
Zhou, Z. et al. Genome-wide DNA methylation pattern in whole blood of patients with Hashimoto thyroiditis. Front. Endocrinol. https://doi.org/10.3389/fendo.2023.1259903 (2023).
Ren, B. et al. Effect of different iodine levels on the DNA methylation of PRKAA2, ITGA6, THEM4 and PRL genes in PI3K-AKT signaling pathway and population-based validation from autoimmune thyroiditis patients. Eur. J. Nutr. 61 (7), 3571–3583. https://doi.org/10.1007/s00394-022-02907-x (2022).
Pakianathan, D. R. et al. Distinct but overlapping epitopes for the interaction of a CC-chemokine with CCR1, CCR3 and CCR5. Biochemistry 36 (32), 9642–9648. https://doi.org/10.1021/bi970593z (1997).
García-López, M. A. et al. Thyrocytes from autoimmune thyroid disorders produce the chemokines IP-10 and Mig and attract CXCR3 + lymphocytes. J. Clin. Endocrinol. Metab. 86 (10), 5008–5016. (2001).
Kemp, E. H. et al. Detection and localization of chemokine gene expression in autoimmune thyroid disease. Clin. Endocrinol. (Oxf). 59 (2), 207–213. (2003).
Sultanova, A. et al. HHV-6 infection and chemokine RANTES Signaling Pathway Disturbance in patients with autoimmune thyroiditis. Viruses 12 (6). https://doi.org/10.3390/v12060689 (2020).
Zhang, R. et al. Identification of DNA methylation-regulated differentially expressed genes in RA by integrated analysis of DNA methylation and RNA-Seq data. J. Transl. Med. 20 (1), 481. https://doi.org/10.1186/s12967-022-03664-5 (2022).
Huo, X. et al. Identification of prognosis markers for endometrial cancer by integrated analysis of DNA methylation and RNA-Seq data. Sci. Rep. 9 (1), 9924. https://doi.org/10.1038/s41598-019-46195-8 (2019).
Strieter, R. M. et al. CXC chemokines in angiogenesis of cancer. Semin. Cancer Biol. 14 (3), 195–200. https://doi.org/10.1016/j.semcancer.2003.10.006 (2004).
Zhu, Y. et al. CXCL8 chemokine in ulcerative colitis. Biomed. Pharmacother. 138 https://doi.org/10.1016/j.biopha.2021.111427 (2021).
Rotondi, M. et al. Interferon-γ and tumor necrosis factor-α sustain secretion of specific CXC chemokines in human thyrocytes: a first step toward a differentiation between autoimmune and tumor-related inflammation? J. Clin. Endocrinol. Metab. 98 (1), 308–313. https://doi.org/10.1210/jc.2012-2555 (2013).
Muzza, M. et al. The tight relationship between papillary thyroid cancer, autoimmunity and inflammation: clinical and molecular studies. Clin. Endocrinol. (Oxf). 72 (5), 702–708. (2010).
Rotondi, M. et al. Role of chemokines in thyroid Cancer microenvironment: is CXCL8 the main player? Front. Endocrinol. (Lausanne). 9, 314. (2018).
Zafon, C. et al. DNA methylation in thyroid cancer. Endocr. Relat. Cancer. 26 (7). https://doi.org/10.1530/erc-19-0093 (2019). p. R415-r439.
Yamazaki, K. et al. Iodide-induced chemokines and genes related to immunological function in cultured human thyroid follicles in the presence of thyrotropin. Thyroid 20 (1), 67–76. https://doi.org/10.1089/thy.2009.0242 (2010).
Ohmori, Y., Schreiber, R. D. & Hamilton, T. A. Synergy between interferon-gamma and tumor necrosis factor-alpha in transcriptional activation is mediated by cooperation between signal transducer and activator of transcription 1 and nuclear factor kappaB. J. Biol. Chem. 272 (23), 14899–14907. (1997).
Chen, Y. et al. Association between different water iodine exposures and thyroid cancer: a retrospective study of high water iodine areas in China from 2009 to 2020. Chemosphere 346, 140581. (2024).
Januś, D. et al. Ultrasound variants of autoimmune thyroiditis in children and adolescents and their clinical implication in relation to papillary thyroid carcinoma development. J. Endocrinol. Invest. 41 (3), 371–380. (2018).
Legler, D. F. et al. B cell-attracting chemokine 1, a human CXC chemokine expressed in lymphoid tissues, selectively attracts B lymphocytes via BLR1/CXCR5. J. Exp. Med. 187 (4), 655–660. https://doi.org/10.1084/jem.187.4.655 (1998).
Gunn, M. D. et al. A B-cell-homing chemokine made in lymphoid follicles activates Burkitt’s lymphoma receptor-1. Nature 391 (6669), 799–803. https://doi.org/10.1038/35876 (1998).
Aust, G. et al. The role of CXCR5 and its ligand CXCL13 in the compartmentalization of lymphocytes in thyroids affected by autoimmune thyroid diseases. Eur. J. Endocrinol. 150 (2), 225–234. https://doi.org/10.1530/eje.0.1500225 (2004).
Zhao, J. & van der Haar, F. Progress in salt iodization and improved iodine nutrition in China, 1995–99. Food Nutr. Bull. 25 (4), 337–343. https://doi.org/10.1177/156482650402500403 (2004).
Jones, M. J., Goodman, S. J. & Kobor, M. S. DNA methylation and healthy human aging. Aging Cell. 14 (6), 924–932. https://doi.org/10.1111/acel.12349 (2015).
McLeod, D. S. et al. Variation in rates of autoimmune thyroid disease by race/ethnicity in US military personnel. Jama 311 (15), 1563–1565. (2014).
Funding
This work was supported by the National Natural Science Foundation of China (grant No. 82073490).
Author information
Authors and Affiliations
Contributions
Yun Chen: writing-original draft preparation, formal analysis. Jinjin Liu: writing-reviewing and editing. B.X.R., Z. Z., Y.H.H., F. L., M.H.J, L.X.L. and X.B.W.: investigation, validation. Hongmei Shen: supervision, funding acquisition. We guarantee that this work is original, has not been published previously and is not being considered for publication elsewhere. All authors have seen and approved the final version of this manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, Y., Liu, J., Ren, B. et al. Validation of DNA methylation and transcriptional characteristics in CCL5 and CXCL8 genes in autoimmune thyroiditis with varying iodine levels. Sci Rep 15, 6006 (2025). https://doi.org/10.1038/s41598-025-90499-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-90499-x
