
Abstract
Burns are a serious public health problem. Despite the decline in the global burden of burns, the burden of burns remains high in low- and middle-income regions, including BRICS countries. To analyse the trend of burn injury incidence in BRICS countries (Brazil, Russia, India, China, South Africa) from 1990 to 2019 and to provide a reference basis for burn injury prevention and management. Data were obtained from the Global Burden of Disease 2019 data, and an age‒period‒cohort model was used to analyse the burn injury incidence data of BRICS countries from 1990 to 2019 via the apc package of R 4.3.0 software. The incidence of burn injuries in BRICS countries decreased from 1990 to 2019, from 114.50 to 85.90 per 100,000, a decrease of 24.98%. Brazil had the largest decrease, 57.05%, and China had the smallest decrease, 7.66%. There was an overall decreasing trend in the incidence of burn injuries in Brazil and South Africa. The results of the age‒period‒cohort (APC) model revealed that the net drift values of burn injury incidence in India, China, South Africa, Russia, and Brazil were ( -0.05% [ 95% CI, -0.30 to 0.21 ] ), ( 0.19% [ 95% CI, 0.03 to 0.35 ] ), ( -1.35% [ 95% CI, -1.65 to -1.04 ] ), ( -0.91% [ 95% CI, -1.02 to -0.80 ] ), ( -3.33% [ 95% CI, -3.49 to -3.16 ] ), respectively. There was an overall decreasing trend in the localized drift curves in Brazil and China. The incidence of burns is greater in children and young adults. Between 1990 and 2019, the time trend had the most significant impact on Brazil’s burn incidence, and the period effect also contributed positively, making Brazil the most notable among the BRICS countries in terms of improvement trends. From 1990 to 2004, the period effect positively impacted China’s burn incidence, whereas from 2010 to 2019, it had a negative effect. In Brazil, South Africa, and Russia, the burden on cohorts born between 1990 and 2019 has been steadily decreasing, and the cohort effect has had a positive effect on the incidence of burns among later birth cohorts. However, in China, the burden borne by cohorts born from 1990 to 2019 has been consistently increasing. There was an overall decreasing trend in the incidence of burns in BRICS countries from 1990 to 2019. Children and adolescents have a high incidence of burns. It is recommended that burn prevention and control strategies be developed according to the age structure and economic level of different countries.
Similar content being viewed by others

Introduction
A burn is an injury to the skin or other organic tissue primarily caused by heat or due to radiation, radioactivity, electricity, friction or contact with chemicals1. Burns are a serious public health problem and are the fourth most common injury factor globally2. Data from a 2018 World Health Organization survey revealed that 11 million burns of all types occur worldwide each year, with approximately 180,000 deaths1. The burden of burns is greater in elderly individuals and children aged 1‒4 years3. Burns not only affect people’s physical and mental health4 but are also costly to care for and place an enormous burden on the National Health Service (NHS)5.
BRICS (Brazil, Russia, India, China) is an economic union of countries established in 2009 and joined by South Africa in 20106,7. From 1 January 2024, the BRICS countries will be expanded to a group of 10 countries including Saudi Arabia, Egypt, the United Arab Emirates, Iran, and Ethiopia, which is known as BRICS-plus8. This study is based on the GBD2019 database (1990–2019 thermal burns data), and in this paper, BRICS refers to the five countries of Brazil, Russia, India, China, and South Africa, with “BRICS” as its abbreviation.
The BRICS countries account for about half of the world’s population9. These countries are experiencing rapid socio-economic development, but they are all facing problems such as expanding and ageing populations and inequalities in health resources10. Studies have shown that the burden of burns decreased worldwide between 1990 and 2017, but the trend of decreasing incidence and mortality from burns has been lower in low- and middle-income regions11. According to 2023 World Health Organization survey data, most burns occur in low-and middle-income countries, and nearly two-thirds occur in regions of the World Health Organization (WHO) in Africa and Southeast Asia1. In India, an estimated 163,000 people die annually from fire injuries12. Ageing is likely to increase the morbidity and mortality of burns13,14.
Previous studies of the burden of disease in burn patients have focused on global, individual countries, selected regions, and age-specific populations15,16,17, but the methodology did not differentiate between the effects of time and age cohort effects. Using mortality data from the World Health Organization and economic data from the World Bank, Peck and Pressman explored the relationship between the economy and burn injuries and reported that burn injuries present a greater burden in low- and middle-income countries18. On this basis, it is estimated that the burden of burn disease is greater in BRICS countries. However, no study has yet comprehensively analysed trends in burn incidence in BRICS countries.
Therefore, this study used the GBD 2019 database to focus on the trend of burn incidence in the BRICS countries from 1990 to 2019, in order to clarify the temporal trend of burn burden in the BRICS countries. The age‒period‒cohort model(APC model) was used for analysis. In addition to reporting the number of cases, incidence, net drift and local drift of burns in BRICS countries, the relationship between the trend of burn incidence in BRICS countries and age, period and birth cohort was further evaluated. These findings can provide enlightenment for the formulation of evidence-based health policies, help the BRICS countries to formulate scientific burn prevention and management strategies according to their own needs and conditions, and promote the rational allocation of medical resources.
Methods
Data sources
The data used in this study were obtained from the Global Burden of Disease Study (GBD2019) database (http://ghdx.healthdata.org/gbd-results-tool).
The database provides not only population data for 204 countries and territories from 1990 to 2019 but also morbidity, mortality, and disability adjusted life years (DALY) rates for 369 diseases and injuries from 1990 to 2019 for 204 countries and territories19.
The GBD 2019 diagnosis of Burns is based on the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (https://icd.who.int/browse10/2019/en). The subject of this study was burns and the criteria and codes for burns are detailed in Attachment 1. This study used data from the GBD database of burns caused by fire, heat and hot substances.
Statistical analysis
This study obtained data on burn incidence, mortality and disability-adjusted life years (DALYs) for all age groups in BRICS countries from 1990 to 2019 from the GBD2019 database, collated the data and estimated the incidence rates via R 4.3.0.
In this study, an age‒period‒cohort model was used to analyse the data. The effects of age, period and cohort on burn incidence trends were analysed via the Age-Period-Cohort Web Tool (APC Web Analysis Tool) (https://analysistools.cancer.gov/apc/)20 and the Poisson distribution21. For APC analysis, the incidence of burns in specific age groups and time periods is presented in a two-dimensional linked table (Attachment 2 and 3). To keep the number of APC model parameters at a manageable level and to obtain reasonably smooth time‒effect curves, we divided the age-specific incidence rates into 5-year groups (0‒4 years, 5‒9 years, and 10‒14 years.90‒94 years), resulting in 19 age groups. The APC model requires that ages and periods be divided at equal intervals. Therefore, this study divides the period from 1990 to 2019 into six consecutive five-year periods (1990‒1994, 1995‒1999, …, 2015‒2019). Since the birth cohort is defined by the age of the subject and the date of the incident, that is cohort = period-age, the corresponding birth cohort is 1903‒1907 (median,1905)‒1988‒1992 (median, 1990). When the age interval and the period interval are equal in width, the diagonal line of the age-period-specific burn incidence rate two-dimensional contingency table represents the birth cohort. The age groups form the rows of Attachment 2 and Attachment 3, and the period forms the columns, the diagonal line from the lower left corner to the lower right represents the birth cohort. Age effects represent different outcome risks for different age groups; period effects represent changes in outcomes over time, affecting all age groups at the same time; and cohort effects relate to changes in outcomes for people with the same year of birth. Net drift represents the overall log-linear trend by period and birth cohort and represents the overall annual percentage change in expected age-adjusted rates over time; localized drift represents the log-linear trend by period and birth cohort by age group and represents the annual percentage change in expected age-specific rates over time; and the longitudinal age profile represents expected age-specific rates in the reference cohort, adjusted for period effects.
The APC model was fitted via the Age-Period-Cohort Web Tool provided by the National Cancer Institute20, and parameter estimation was performed via the Wald chi-square test with a test level of α = 0.05 (two-sided). The data were organized via Excel 2019 software, and the results were output and plotted via R 4.3.0 software22.
Results
Trends in burn incidence
Table 1; Fig. 1 show the trends in burn incidence in BRICS countries. In 2019, a total of 2,776,229 burn cases were reported in BRICS countries. From 1990 to 2019, there was a general decrease in the incidence of burns in BRICS countries, from 114.50 to 85.90 per 100,000, with the highest rate of decrease in Brazil (57.05%) and the lowest in China (7.66%). In 2019, Russia had the highest incidence of burns among BRICS countries (235.60 per 100,000). Three of the countries, China, India and South Africa, have similar burn incidence rates, all of which are less than 100 per 100,000 people.

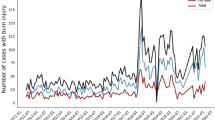
Number of new burn injuries and incidence rates in Brazil, China, India, Russia, and South Africa from 1990 to 2019.
Attachment 2 and Attachment 3 show the number of new burn injuries and the incidence of burn injuries in BRICS countries by age, period, and median birth cohort. From 1990 to 2015, the incidence of burns in Brazil, South Africa, India and China showed a general downward trend. Among them, the incidence of burns in Brazil decreased the most, which was 56.36% ( from 311.55 / 100 000 in 1990 to 135.96 / 100 000 in 2015 ). At the same time, the incidence of burns in India and China decreased less than that in the other two countries. From 2015 to 2017, the incidence of burns in Brazil increased by 1.96% ( from 135.96 / 100,000 in 2015 to 138.62 / 100,000 in 2017 ). Over the same period, the incidence of burns in China increased by 14.48% ( from 70.79 / 100,000 in 2015 to 81.04 / 100,000 in 2017 ).
From 1990 to 2000, the incidence of burns in Russia increased by 15.04% ( from 337.08 / 100,000 in 1990 to 387.76 / 100,000 in 2000 ), and the incidence of burns decreased by 39.25% from 2000 to 2019 ( from 387.76 / 100,000 in 2000 to 235.58 / 100,000 in 2019 ).
Age-specific incidence of burns
In the present study, the incidence of burns was organized over a consecutive 5-year period from 1990 to 1994 (median, 1992) to 2015‒2019 (median, 2017) and into 19 age groups, including those born from 1903 to 1907 (median, 1905) to 1988‒1992 (median, 1990). Includes persons born from 1903 to 1907 (median, 1905) to 1988‒1992 (median, 1990).
Figures 2, 3, 4, 5 and 6 show the trends in burn incidence in BRICS countries from 1990 to 2019. Figures 2, 3, 5 and 6 show that the incidence of burns in Brazil, China, Russia and South Africa had similar trends for males and females, with the exception that the incidence of burns was generally higher for males than for females in Russia. Figure 4 shows that there is a significant difference in the trend of burn incidence between males and females in India, with females having a significantly higher incidence of burns than males. Figure 4A shows that there are two peaks on the curve corresponding to the age groups 20‒30 years and 30‒40 years, indicating that the highest incidence of burns in Indian males is found in the age groups 20‒30 years and 30‒40 years. However, as shown in Fig. 4A, except for the curve for 2015‒2019, there was a peak in the incidence of burns in Indian males aged 20‒30 years. Figure 4B shows that there is a peak on the curve indicating that the incidence of burns in Indian females is highest at the age of 15‒25 years. Figure 6 shows that the incidence of burns in South Africa is generally higher for females than for males.

Age-specific incidence of burns in Brazil by period between 1990 and 2019. Note: The survey years were organized into 5 consecutive years, from 1990 to 1994 (median, 1992 1995 to 1999 (median, 1997), 2000 to 2004 (median, 2002), 2005 to 2009 (median, 2007), and 2010 to 2014 (median, 2012 ), and 2015 through 2019 (median, 2017). Longitudinal yearly curves were estimated from age-period-cohort models and represent expected age-specific rates of burn incidence. Age specific curves for males are shown in zone (A) of each graph, whereas age-specific curves for females are shown in zone (B).

Age-specific incidence rates of burns by period in China, 1990–2019. The survey years were organized into 5 consecutive years, from 1990 to 1994 (median, 1992 1995 to 1999 (median, 1997), 2000 to 2004 (median, 2002), 2005 to 2009 (median, 2007), and 2010 to 2014 (median, 2012 ), and 2015 through 2019 (median, 2017). Longitudinal yearly curves were estimated from age-period-cohort models and represent expected age-specific rates of burn incidence. Age-specific curves for males are shown in zone (A) of each graph, whereas age-specific curves for females are shown in zone (B).

Age-specific incidence of burns in India by period between 1990 and 2019. The survey years were organized into 5 consecutive years, from 1990 to 1994 (median, 1992 1995 to 1999 (median, 1997), 2000 to 2004 (median, 2002), 2005 to 2009 (median, 2007), and 2010 to 2014 (median, 2012 ), and 2015 through 2019 (median, 2017). Longitudinal yearly curves were estimated from age-period-cohort models and represent expected age-specific rates of burn incidence. Age-specific curves for males are shown in zone (A) of each graph, whereas age-specific curves for females are shown in zone (B).

Age-specific incidence of burns in Russia by period between 1990 and 2019. The survey years were organized into 5 consecutive years, from 1990 to 1994 (median, 1992 1995 to 1999 (median, 1997), 2000 to 2004 (median, 2002), 2005 to 2009 (median, 2007), and 2010 to 2014 (median, 2012 ), and 2015 through 2019 (median, 2017). Longitudinal yearly curves were estimated from age-period-cohort models and represent expected age-specific rates of burn incidence. Age-specific curves for males are shown in zone (A) of each graph, whereas age-specific curves for females are shown in zone (B).

Age-specific incidence of burns in South Africa by period between 1990 and 2019. The survey years were organized into 5 consecutive years, from 1990 to 1994 (median, 1992 1995 to 1999 (median, 1997), 2000 to 2004 (median, 2002), 2005 to 2009 (median, 2007), and 2010 to 2014 (median, 2012 ), and 2015 through 2019 (median, 2017). Longitudinal yearly curves were estimated from age-period-cohort models and represent expected age-specific rates of burn incidence. Age-specific curves for males are shown in zone (A) of each graph, whereas age-specific curves for females are shown in zone (B).
Net and localized drift in different age groups
Net drift represents the overall annual percentage change over the entire study period, whereas localized drift represents the annual percentage change in incidence relative to the net drift for each age group (Fig. 7). Attachment 4 shows that among the BRICS countries, the overall net drift values of four countries are below 0, including Brazil ( -3.33% [ 95% CI, -3.49 to -3.16 ] ), India ( -0.05% [ 95% CI, -0.30 to 0.21 ] ), Russia ( -0.91% [ 95% CI, -1.02 to -0.80 ] ), South Africa ( -1.35% [ 95% CI, -1.65 to -1.04 ] ). The overall net drift value in China was greater than 0, indicating an upward trend in the incidence of burns throughout the study period ( 0.19% [ 95% CI, 0.03 to 0.35 ] ).

Local drift with net drift values for burn incidence rate in Brazil, China, India, Russia, South Africa from 1990 to 2019. (A–C) use the same set of legends; (B) and (C) are the result of data on men and women, respectively.
Brazil had the largest overall annual percentage decrease (-3.33% [95% CI, -3.49 to -3.16]), indicating a significant decrease in burn incidence throughout the study period. The overall annual percentage decreases were greater in Russia, South Africa, and Brazil than in China and India. In Brazil, a clear sex difference was found, with a greater decrease in incidence in females than in males, at (-3.53% [95% CI, -3.76 to -3.29]) and (-3.17 [95% CI, -3.33 to -3.00]), respectively.
Localized drift indicates additional age changes in the incidence trend. For example, for South African females aged 0‒74 years, a localized drift value of < 0 indicates a decrease in the incidence of burns. Figure 7 shows that China, India, and South Africa had local drift values of burn incidence above 0 for certain age groups. In China, it was for ages 0‒49, ranging from 1.54–0.02%.(Attachment 5) In India, it was for ages 40‒94, varying from 0.16 to 0.05%. In South Africa, it was for individuals aged 75‒94 years, ranging from 0.17 to 0.02%. Among all age groups in the BRICS countries, the most significant decrease in incidence was observed in Brazil among those aged 80–90 years. Figure 7A shows that local drift peaked among older adults in India, Russia, and South Africa, contrary to what was observed among older adults in other countries.
The effect of age-period-cohort on the incidence of burns
Figures 8 and 9, and 10 present the estimated impacts of age, period, and cohort effects on the incidence of burns. Figure 8 shows a rapidly increasing trend in the incidence of burns among persons aged 0‒5 years in all age groups in BRICS countries, with the highest incidence of burns in the 5‒24 years age group.

Parameter estimates of the age effect on burn incidence in Brazil, Russia, India, China, and South Africa from 1990 to 2019. All data are analyzed by sex, with block (A) corresponding to males and block (B) to females.

Parameter estimates for the period effect of burn incidence in Brazil, Russia, India, China and South Africa from 1990 to 2019. All data are analyzed by sex, with block (A) corresponding to males and block (B) to females.

Parameter estimates of cohort effects for burn incidence in Brazil, Russia, India, China, and South Africa from 1990 to 2019. All data are analyzed by sex, with block (A) corresponding to males and block (B) to females.
As shown in Fig. 8, the incidence of burns among male individuals in Russia is significantly higher than that among females, whereas the incidence of burns among females in South Africa is notably higher compared to that among males.
The incidence of burns in Brazil, South Africa and China showed an overall decreasing trend in the 25‒94 years age group, with the most pronounced decreasing trend in Brazil. In Russia, the incidence of burns is rapidly decreasing in the 25‒69 years age group and increasing in the 79‒94 years age group, with a rapid increase in males.
Figure 9 shows that during the entire study period, the period effect had the most significant impact on the incidence of burns in Brazil, and the period effect played a positive role, making Brazil the most significant country in the improvement trend of the BRICS countries. Between 1990 and 2000, the incidence of burns in Russia showed a worsening trend, and the period effect had a negative impact on the incidence of burns in Russia. From 2005 to 2019, the burn incidence ratios of Russia, South Africa and Brazil were all less than 1, and all showed an improvement trend, indicating that the period effect had a positive impact on the burn incidence in these countries during the 15-year period.
Figure 10 displays the estimated impact of cohort effect on the incidence of burns. The cohort effect refers to changes in the frequency of diseases that occur due to variations in the level of exposure to risk factors across different generations. It is used to explain differences in disease frequency, health status, or behavioral patterns among different birth cohorts (i.e., groups of individuals born within the same time period) as a result of their exposure to different social, economic, and environmental factors.
Among the birth cohorts in BRICS countries, Brazil has been significantly impacted by the cohort effect, whereas India has been less affected. In Brazil, South Africa, and Russia, the burden on cohorts born between 1990 and 2019 has been steadily decreasing, and the cohort effect has had a positive impact on the incidence of burns among later birth cohorts. However, in China, the burden borne by cohorts born from 1990 to 2019 has been consistently increasing.
Discussions
In this study, the APC model was used for the first time to analyze the incidence of burns in BRICS countries. Compared with the previous 2019 GBD study15,23, the main contribution of our study is to provide a more comprehensive and in-depth understanding of burn trends, and to use age, period and cohort effects to distinguish different risk factors within the BRICS countries. Another noteworthy progress is the measurement of local drift in the age distribution of onset in the BRICS countries from 1990 to 2019. This method can clarify the time trend of the incidence of a specific age group, taking into account the effects of period and cohort effects. Based on the APC model, our analysis provides valuable information for policy makers and medical experts by studying the time trend of burn incidence in detail and evaluating the effectiveness of related medical services.
Among the BRICS countries, China had the smallest decrease in burn incidence. The reasons for the low incidence of early burns be as follows: Early China’s economic and social development was rapid, but the construction of health care did not keep pace with the rapid development24. Most of the population lacks knowledge of first aid for burns, and educational activities on burn prevention and first aid are recommended25. China lacks a national burn registration system, and there are biases in the recording of burn data26. In addition, medical insurance coverage in China was low before 2010 and a universal healthcare system had not been established, so some patients requiring specialised burn care may be less likely to be admitted to hospitals due to the high financial burden. Since 2010, the period effect and cohort effect have had a negative impact on the incidence of burns in China. The incidence of burns in China has been on the rise, with the highest incidence in the 10–25 age group. This may be related to the following reasons : Firstly, the economic development brought about by the reform and opening-up policy has enabled people to afford hospital expenses, thereby increasing outpatient and inpatient rates27. Secondly, in 2009, China initiated a significant healthcare reform that continuously expanded medical coverage28. This reform also introduced a higher reimbursement rate for inpatient treatment compared to outpatient care, which has led to a greater preference for inpatient hospitalization among the population29. Thirdly, the increased exposure of adolescents to risks and adventurous behaviors has elevated their vulnerability to injuries30. Furthermore, since the implementation of the one-child policy in the 1970s, numerous Chinese families have had only one child, resulting in heightened attention and priority given to the health of these only children by their parents31,32. In addition, aging may also be an influencing factor for the increase in the incidence of burns. Since China entered an aging society in 2000, the proportion of the elderly population has continued to grow33. At the same time, the elderly are more susceptible to burn injuries due to poor physiological tolerance, such as slow movement, weakened visual and sensory functions, skin atrophy, poor self-care ability, and decreased judgment and coordination34,35.
Between 1990 and 2019, Brazil experienced the greatest decrease in the incidence of burns. As shown in Fig. 9, the time trend had the greatest effect on burn incidence in Brazil, revealing the most significant improvement in the curve among the BRICS countries. This may be related to the following reasons: since 1990, Brazil has achieved some success in the field of public health, which can be attributed to the creation of the Unified Health System (SUS) at the end of the 1980s. Burn burden studies using the national inpatient database provided by the Brazilian Ministry of Information for the Unified Health System ( DATA-SUS ) are essential for the development of appropriate health policies36. The implementation of the family health care plan ( PSF ) and the community health service organization plan ( PACS ) is conducive to expanding health care coverage, promoting health prevention initiatives, achieving universal health care37, and promoting the regionalization of medical services on the basis of the medical network structure38. Another factor contributing to the decline in the incidence of burns in Brazil may be the government’s legal policies against burns.The Brazilian Federal Government systematically establishes that states and municipalities should comply with the provisions of the federal legislation on fire prevention and the scope of public safety, which favours federal, state and municipal fire prevention legislation to ensure the safety of the population39. In Rio Grande do Sul, a state law called the “Kiss of the Law” was approved in December 2013 and has since been signed into law. This law establishes standards for the safety, prevention and protection of buildings and fire risk areas in Rio Grande do Sul40. Notably, since 1990, there has been a downward trend in the incidence of burns in Brazil, and although this is a potentially good indicator, these data may be related to limited access to medical services. In low- and middle-income countries, only one-half to two-thirds of burn patients are treated in healthcare facilities41. In Brazil, only 18–40% of these patients are hospitalized42,43. This may also explain the decline in the incidence of burns in Brazil.
The slower decline in burn incidence in India may be related to the following reasons: In India, there is a significant gap in the availability of preventive education and first aid information on burn-related injuries44. In addition, studies have shown that burn incidence is associated with the economic development of a country, with low-income areas being more susceptible to fires, heat, and hot substances45, which may influence the incidence of burns in India. India responded to the burden of burns by establishing burn centers and launching the National Burn Prevention and Management Program in 2010, and in 2017, the new National Health Policy (NHP) set out aspirations to progressively achieve universal health coverage, which may be beneficial in reducing the burden of burn morbidity in India, despite issues such as inadequate healthcare infrastructure and limited coverage of burn services46. The possible reasons for the greater incidence of burn injuries in females than in males in India are as follows: burn injuries caused by interpersonal and gender-based violence are significant problems in India and most of the victims are female47. In India, approximately 65% of burn deaths occur in women, including self-immolation and incidents of domestic violence12, such as burning of brides for a lack of dowry. In India, most burn injuries occur in females, probably because females often use wood and kerosene devices without safety features for cooking and wear loose fitting clothes, risking accidental exposure to open flames48. During the period from 2000 to 2004, India experienced a notable increase in the incidence rate among its higher age group (Fig. 4). This surge can be attributed to several factors. India is facing an ageing population10. In India, the combination of poverty, substandard housing, and inadequate infrastructure heightens the vulnerability of individuals living in urban slums49. Injuries related to fires are a major public health problem in India, where the incidence of fires in the home environment is high, most of which are kitchen fires that can easily cause houses to burn12. According to research, flame burns and scalds are the primary causes of burns among older adults, with a high frequency of occurrence within their homes, particularly in kitchen environments50,51. Elderly individuals are more prone to burns because of their poor physiological tolerance and sluggish movements34,35. Notably, studies have emphasized the lack of continuous and comprehensive data collection in developing nations52. Discrepancies in injury records can be attributed to increased morbidity and mortality rates in certain nations2. To address these issues, we recommend establishing a national burn registry, bolstering infrastructure, improving housing conditions, intensifying fire prevention awareness and education, and increasing safety consciousness among people.
Figure 8 shows that from 1990 to 2019, the incidence of burns among women in South Africa was significantly greater than that among men, which may be related to the following reasons: the home environment has been identified as the most common location for burn injuries. This is due primarily to several factors, including poverty, inadequate housing conditions, the absence of crucial safety measures, and the widespread use of kerosene lamps, which collectively increase the incidence of such injuries53,54. A study in South Africa revealed that kerosene stoves play a significant role in shack fires, accounting for 71% of burn cases55. Shacks, which are informal settlements common in the region, are known for their flammability, overcrowding ability, and limited access to basic such as water and electricity52,55. These conditions exponentially increase the risk of fire outbreaks. In such environments, women often bear the primary responsibility for domestic cooking. This regular exposure to open flame devices, especially kerosene stoves, significantly increases their risk of suffering burn injuries. Additionally, scalding injuries resulting from hot liquids represent a significant proportion of burn cases in South Africa53,56. These injuries are frequently linked to daily household activities, particularly those involving the handling of hot liquids such as water and oil. Women who engage in these activities more regularly are thus disproportionately affected by such scalds. While studies have indicated a higher incidence of burns among South African men, often attributed to factors such as scalds, domestic violence, and intentional harm, these findings may be biased. This bias could arise from limitations in data collection, as some studies have relied primarily on data from large hospitals, overlooking the fact that nonurban residents are more likely to seek treatment at smaller, local healthcare facilities56,57. On the basis of these findings, the establishment of enforceable legislation is strongly recommended. This legislation should address housing standards and infrastructure, as well as set production standards for certified kerosene stoves. Such measures could promote the design of safer cooking stoves and facilitate research into more secure biofuels and materials for shack construction, ultimately reducing the incidence of burn injuries in vulnerable communities. Notably, there is a lack of burn specialists in South Africa, and poor professional management predisposes individuals to high burn morbidity and mortality58. Unreasonable resource allocation and a lack of basic infrastructure in low- and middle-income countries are also great challenges to the development of work in the field of burn prevention59. Medical resources should be allocated and utilized rationally, burn professionals should be trained, and scientific standards for burn management should be developed. Localized drift has shown an increasing trend in burn incidence among people aged 75‒80 years in South Africa. This may be due to the increase in the number of elderly people as a result of global aging, which, coupled with the slower mobility of the elderly as a result of reduced body functions, may contribute to the increase in the incidence of burns. There has been a significant decrease in burn incidence in South Africa since 2000, with positive time and cohort effects, which may be related to the following factors. In 1996, the Paraffin Safety Association of Southern Africa (PSASA) was established as a nongovernmental organization to promote the safe use of paraffin wax in the home. Since 2003, the PSASA has been testing most of the commonly available paraffin stoves and conducting public awareness and education programs. In addition, to reduce the number of burns, South Africa has called for a ban on the manufacture and sale of unsafe paraffin equipment60. It is recommended that burn prevention education be targeted at poor and at-risk populations and that the government legislate and monitor production standards for fuels and equipment.
Russia had a high incidence of burns between 1995 and 2000. Studies have shown that national political and social instability is associated with injury mortality61. Major political and economic upheavals in countries that were once part of the Union of Soviet Socialist Republics (USSR) may be responsible for the increasing trend in fire and burn deaths, which began to increase around the time of the dissolution of the USSR in 1991 18. By the late 1990s, as capitalism and democracy began to replace communism, the death rate once again began to decline61. The period effect and cohort effect of burn incidence in Russia showed a decreasing trend after 2004. Possibly related to the NPPH program, in 2005, President Putin announced four national priorities, including education and health. The project was launched in 2006 with the aim of improving the supply of material, technical and human resources in the health sector and thus improving the health of the population. The NPPH program is a two-year initiative that proposes prioritizing the improvement of access to primary care, disease prevention, and tertiary care62. In addition, with the development of the social, economic and health care system in Russia, there may have been a favorable impact on the incidence of burns. From 1990 to 2019, the incidence of burns among males in Russia was generally higher than that among females, and the incidence of burns among people aged 75 and over increased significantly in all years, especially among males. (Fig. 8). This may be due to the following reasons: In Russia, the higher incidence of burns among males than females can be attributed, on the one hand, to their more frequent alcohol consumption and, on the other hand, to the precarious labor conditions that render them susceptible to occupational injuries63,64. The cold regions of Russia are characterized by high levels of alcohol intake, with the majority of the population having developed a habit of drinking65. Notably, alcohol consumption and rates of alcoholism are significantly higher among males than females66. Within the adult population of the Russian Federation, injuries resulting from accidents and other external causes are more prevalent among males (55.71%), who constitute the primary workforce in industrial production sectors67. Between 1990 and 2019, Russia experienced an escalation in population aging, marked by a continual increase in the proportion of elderly individuals68, who are prone to physiological decline and reduced mobility.
Conclusions and limitations
The incidence of burns is influenced by demographics, politics, economics, and the environment. The experiences of Brazil and South Africa demonstrate the crucial importance of enacting relevant laws for burn prevention, improving infrastructure, enhancing housing conditions, and strengthening educational training on burn prevention. Additionally, developing countries often face a lack of comprehensive, continuous, and effective statistical data on burns. GBD2019 burn data are based on secondary data from existing registries. Burn data from BRICS may be missing because of factors such as regional remoteness. It is recommended that monitoring and research on the epidemiological problems of burns be strengthened through the establishment of a high-coverage and systematic burn data center, which will in turn allow for a more accurate assessment of trends in the incidence of burns. Improving national medical statistical systems can provide valuable references for the BRICS countries in formulating policies related to burn prevention.
Nevertheless, the APC model employed in this study possesses certain limitations that could potentially influence the results. Firstly, there exists an overlap in the birth cohort, as individuals born within a specific period may belong to two different age groups or span across two time periods. Secondly, the birth cohort is calculated as the period minus the age, revealing a linear dependency among these three variables.
In conclusion, the incidence rates have been calculated over the past 30 years using the APC model, thus yielding age-period-cohort effect equivalents in these five countries. Comparisons have been made between countries regarding the changes in incidence rates over time and the exposure risk of specific populations. The results not only provide insight into the pattern of change but also have the potential to predict future trends. Our data serves as a basis for BRICS to formulate a targeted approach aimed at reducing the burden of burns.
Data availability
Data is provided within the manuscript or supplementary information files. All data in this study were obtained from the GBD2019 database, and the corresponding author can provide all original data upon request.
References
WHO. Burn data, (2023). https://www.who.int/news-room/fact-sheets/detail/burns
Smolle, C. et al. Recent trends in burn epidemiology worldwide: A systematic review. Burns 43, 249–257. https://doi.org/10.1016/j.burns.2016.08.013 (2017).
Chen, Z. et al. Global burden of thermal burns, 1990–2017: unbalanced distributions and Temporal trends assessed from the global burden of disease study 2017. Burns 48, 915–925. https://doi.org/10.1016/j.burns.2021.08.002 (2022).
Mason, S. A. et al. Increased rate of Long-term mortality among burn survivors: A Population-based matched cohort study. Ann. Surg. 269, 1192–1199. https://doi.org/10.1097/SLA.0000000000002722 (2019).
Hemington-Gorse, S. J., Potokar, T. S., Drew, P. J. & Dickson, W. A. Burn care costing: the Welsh experience. Burns 35, 378–382. https://doi.org/10.1016/j.burns.2008.08.012 (2009).
BRICS. History of BRICS, (2024). https://infobrics.org/page/history-of-brics/
Harmer, A. & Fleck, F. The BRICS countries: a new force in global health? Bull. World Health Organ. 92, 394–395. https://doi.org/10.2471/blt.14.030614 (2014).
Cheng, F. et al. Epidemiological trends and age-period-cohort effects on ischemic stroke burden across the BRICS-plus from 1992 to 2021. BMC Public. Health. 25, 137. https://doi.org/10.1186/s12889-025-21310-9 (2025).
Acharya, S. et al. BRICS and global health. Bull. World Health Organ. 92 (386A), 386. https://doi.org/10.2471/BLT.14.140889 (2014).
Jesus, T. S. et al. Physical rehabilitation needs in the BRICS nations from 1990 to 2017: Cross-National analyses using data from the global burden of disease study. Int. J. Environ. Res. Public. Health. 17 https://doi.org/10.3390/ijerph17114139 (2020).
James, S. L. et al. Epidemiology of injuries from fire, heat and hot substances: global, regional and National morbidity and mortality estimates from the global burden of disease 2017 study. Inj Prev. 26, i36–i45. https://doi.org/10.1136/injuryprev-2019-043299 (2020).
Sanghavi, P., Bhalla, K. & Das, V. Fire-related deaths in India in 2001: a retrospective analysis of data. Lancet 373, 1282–1288. https://doi.org/10.1016/s0140-6736(09)60235-x (2009).
Liu, Y. et al. Epidemiologic investigation of burns in the elderly in Sichuan Province. Burns 39, 389–394. https://doi.org/10.1016/j.burns.2012.04.012 (2013).
Emami, S. A., Motevalian, S. A., Momeni, M. & Karimi, H. The epidemiology of geriatric burns in Iran: A National burn registry-based study. Burns 42, 1128–1132. https://doi.org/10.1016/j.burns.2016.03.011 (2016).
Yakupu, A. et al. The epidemiological characteristic and trends of burns globally. BMC Public. Health. 22, 1596. https://doi.org/10.1186/s12889-022-13887-2 (2022).
Saavedra, P. A., deBrito, E. S., Areda, C. A., Escalda, P. M. & Galato, D. Burns in the Brazilian unified health system: a review of hospitalization from 2008 to 2017. Int. J. Burns Trauma. 9, 88–98 (2019).
Wu, H., Xi, M. & Xie, W. Epidemiological and clinical characteristics of older adults with burns: a 15-year retrospective analysis of 2554 cases in Wuhan Institute of burns. BMC Geriatr. 23, 162. https://doi.org/10.1186/s12877-023-03883-5 (2023).
Peck, M. & Pressman, M. A. The correlation between burn mortality rates from fire and flame and economic status of countries. Burns 39, 1054–1059. https://doi.org/10.1016/j.burns.2013.04.010 (2013).
Collaborators, G. B. D. D. global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the global burden of disease study 2019. Lancet 396, 1160–1203. https://doi.org/10.1016/S0140-6736(20)30977-6 (2020).
Rosenberg, P. S., Check, D. P. & Anderson, W. F. A web tool for age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol. Biomarkers Prev. 23, 2296–2302. https://doi.org/10.1158/1055-9965.EPI-14-0300 (2014).
Liu, X., Yu, C., Bi, Y. & Zhang, Z. J. Trends and age-period-cohort effect on incidence and mortality of prostate cancer from 1990 to 2017 in China. Public. Health. 172, 70–80. https://doi.org/10.1016/j.puhe.2019.04.016 (2019).
Yadav, C. P., Sharma, A. & National Institute of Malaria Research-Malaria Dashboard (NIMR-MDB). A digital platform for analysis and visualization of epidemiological data. Lancet Reg. Health Southeast. Asia. 5, 100030. https://doi.org/10.1016/j.lansea.2022.100030 (2022).
Yin, X. et al. The global, regional, and National burden of Burns: an analysis of injury by fire, heat, and hot substances in the global burden of disease study 2019. Injury 56, 111955. https://doi.org/10.1016/j.injury.2024.111955 (2025).
Yongqiang, F. et al. Epidemiology of hospitalized burn patients in Shandong Province: 2001–2005. J. Burn Care Res. 28, 468–473. https://doi.org/10.1097/BCR.0B013E318053D28B (2007).
Tse, T. et al. Paediatric burn prevention: an epidemiological approach. Burns 32, 229–234. https://doi.org/10.1016/j.burns.2005.08.025 (2006).
Li, H. et al. The progress of Chinese burn medicine from the third military medical University-in memory of its pioneer, professor Li Ao. Burns Trauma. 5, 16. https://doi.org/10.1186/s41038-017-0082-z (2017).
(NBS) & o., C. N. B. S. The Ninth Report on Economic and Social Development Achievements during the ‘Eleventh Five-Year Plan’ Period: Continuous Growth in Income and Significant Improvement in Quality of Life for Urban Residents Nationwide., (2011). https://www.stats.gov.cn/zt_18555/ztfx/sywcj/202303/t20230301_1920369.html
Yip, W. C. et al. Early appraisal of China’s huge and complex health-care reforms. Lancet 379, 833–842. https://doi.org/10.1016/s0140-6736(11)61880-1 (2012).
Li, L. & Fu, H. China’s health care system reform: progress and prospects. Int. J. Health Plann. Manage. 32, 240–253. https://doi.org/10.1002/hpm.2424 (2017).
Dowd, M. D., Keenan, H. T. & Bratton, S. L. Epidemiology and prevention of childhood injuries. Crit. Care Med. 30, 385–392. https://doi.org/10.1097/00003246-200211001-00002 (2002).
Basten, S. & Jiang, Q. China’s family planning policies: recent reforms and future prospects. Stud. Fam Plann. 45, 493–509. https://doi.org/10.1111/j.1728-4465.2014.00003.x (2014).
Zhu, L. et al. Hospitalized pediatric burns in North China: a 10-year epidemiologic review. Burns 39, 1004–1011. https://doi.org/10.1016/j.burns.2012.12.014 (2013).
China, N. B. o. S. o. Interpretation of the seventh national census bulletin., (2021). https://www.stats.gov.cn/sj/sjjd/202302/t20230202_1896484.html
Qian, W. et al. Epidemiological and clinical characteristics of burns in the older person: a seven-year retrospective analysis of 693 cases at a burn center in south-west China. Burns Trauma. 8, tkz005. https://doi.org/10.1093/burnst/tkz005 (2020).
Peck, M. D. Epidemiology of burns throughout the world. Part I: distribution and risk factors. Burns 37, 1087–1100. https://doi.org/10.1016/j.burns.2011.06.005 (2011).
Santos, J. V., Souza, J., Amarante, J. & Freitas, A. Burden of burns in Brazil from 2000 to 2014: A nationwide Hospital-Based study. World J. Surg. 41, 2006–2012. https://doi.org/10.1007/s00268-017-3988-5 (2017).
Menicucci, T. M. G. The unified National health system, 20 years: assessment and perspectives. Cad Saude Publica. 25, 1620–1625. https://doi.org/10.1590/s0102-311x2009000700021 (2009).
Silveira, D. M. & dos Santos, H. G. Access to neonatal healthcare services: analysis of displacement networks between municipalities in the state of Parana, Brazil. Cad Saude Publica. 39 https://doi.org/10.1590/0102-311xpt244422 (2023).
Gragnani, A., de Oliveira, A. F., Boro, D., Pham, T. N. & Ferreira, L. M. Response and legislative changes after the kiss nightclub tragedy in Santa Maria/RS/Brazil: learning from a large-scale burn disaster. Burns 43, 343–349. https://doi.org/10.1016/j.burns.2016.08.010 (2017).
Mackie, D. P., Koning, H. M., FATE OF MASS & BURN CASUALTIES - IMPLICATIONS FOR DISASTER PLANNING. Burns 16, 203–206, doi:https://doi.org/10.1016/0305-4179(90)90040-4 (1990).
Forjuoh, S. N. Burns in low- and middle-income countries: A review of available literature on descriptive epidemiology, risk factors, treatment, and prevention. Burns 32, 529–537. https://doi.org/10.1016/j.burns.2006.04.002 (2006).
Gawryszewski, V. P. et al. Public hospital emergency department visits due to burns in Brazil, 2009. Cad Saude Publica. 28, 629–640. https://doi.org/10.1590/s0102-311x2012000400003 (2012).
Orozco-Valerio, M. D., Miranda-Altamirano, R. A., Magana, A. C. M. & Celis, A. Trends in mortality by burns in Mexico, 1979–2009. Gac Med. Mex. 148, 349–357 (2012).
Hodgins, P., Potokar, T. & Price, P. Comparing rich and poor: burn prevention in Wales, Pakistan, India, Botswana and Zambia. Burns 37, 1354–1359. https://doi.org/10.1016/j.burns.2011.07.001 (2011).
Peck, M. D. Epidemiology of burns throughout the world. Part II: intentional burns in adults. Burns 38, 630–637. https://doi.org/10.1016/j.burns.2011.12.028 (2012).
Keshri, V. R. & Jagnoor, J. Burns in India: a call for health policy action. Lancet Public. Health. 7, e8–e9. https://doi.org/10.1016/s2468-2667(21)00256-5 (2022).
Natarajan, M. Differences between intentional and non-intentional burns in India: implications for prevention. Burns 40, 1033–1039. https://doi.org/10.1016/j.burns.2013.12.002 (2014).
Ahuja, R. B. & Bhattacharya, S. ABC of burns - Burns in the developing world and burn disasters. Br. Med. J. 329, 447–449. https://doi.org/10.1136/bmj.329.7463.447 (2004).
Subbaraman, R. et al. The psychological toll of slum living in Mumbai, India: a mixed methods study. Soc. Sci. Med. 119, 155–169. https://doi.org/10.1016/j.socscimed.2014.08.021 (2014).
Rani, M. & Schwacha, M. G. Aging and the pathogenic response to burn. Aging Dis. 3, 171–180 (2012).
Keck, M., Lumenta, D. B., Andel, H., Kamolz, L. P. & Frey, M. Burn treatment in the elderly. Burns 35, 1071–1079. https://doi.org/10.1016/j.burns.2009.03.004 (2009).
Peck, M. D., Kruger, G. E., van der Merwe, A. E., Godakumbura, W. & Ahuja, R. B. Burns and fires from non-electric domestic appliances in low and middle income countries part I. The scope of the problem. Burns 34, 303–311. https://doi.org/10.1016/j.burns.2007.08.014 (2008).
Nthumba, P. M. Burns in sub-Saharan Africa: A review. Burns 42, 258–266. https://doi.org/10.1016/j.burns.2015.04.006 (2016).
Hlela, M., du Toit, C. & Davies, B. The role of alcohol and drug intoxication in Fire-Related incidents in Africa: A systematic review. Ann. Burns Fire Disasters. 35, 278–299 (2022).
Maritz, D., Wallis, L., Van Der Merwe, E. & Nel, D. The aetiology of adult burns in the Western cape, South Africa. Burns 38, 120–127. https://doi.org/10.1016/j.burns.2010.12.007 (2012).
Cloake, T., Haigh, T., Cheshire, J. & Walker, D. The impact of patient demographics and comorbidities upon burns admitted to Tygerberg hospital burns unit, Western cape, South Africa. Burns 43, 411–416. https://doi.org/10.1016/j.burns.2016.08.031 (2017).
Allorto, N. L., Oosthuizen, G. V., Clarke, D. L. & Muckart, D. J. The spectrum and outcome of burns at a regional hospital in South Africa. Burns 35, 1004–1008. https://doi.org/10.1016/j.burns.2009.01.004 (2009).
Allorto, N. L., Zoepke, S., Clarke, D. L. & Rode, H. Burn surgeons in South Africa: A rare species. S Afr. Med. J. 106, 186–188. https://doi.org/10.7196/SAMJ.2016.v106i2.9954 (2016).
Gupta, S. et al. Burn management capacity in low and middle-income countries: A systematic review of 458 hospitals across 14 countries. Int. J. Surg. 12, 1070–1073. https://doi.org/10.1016/j.ijsu.2014.08.353 (2014).
Peck, M. D. et al. Burns and injuries from non-electric-appliance fires in low-and middle-income countries. Part II. A strategy for intervention using the Haddon matrix. Burns 34, 312–319. https://doi.org/10.1016/j.burns.2007.08.009 (2008).
Peck, M. D., Shankar, V. & Bangdiwala, S. I. Trends in injury-related deaths before and after dissolution of the union of Soviet Socialist republics. Int. J. Injury Control Saf. Promotion. 14, 139–151. https://doi.org/10.1080/00207720701500534 (2007).
Popovich, L. et al. Health system review. Health Syst. Transition. 13, 1–190 (2011). xiii-xivRussian Federation.
Азолов, В. В. & Пономарева, Ж. В. А. Н А. Проблемы специализированной Помощи обожженным В России и Пути Их Решения. Международный Медицинский Журнал (2003).
Kuzina, O. E. et al. Оценка летальности и факторов риска получения ожоговой травмы среди мужчин и женщин трудоспособного возраста. Федеральное государственное бюджетное образовательное учреждение высшего образования «Уральский государственный медицинский университет» Министерства здравоохранения Российской Федерации (2019).
von Fingerhut, G. et al. [Relations of alcohol consumption and sleep among community-dwelling elderly living in cold region of Russia: a cross-sectional study]. Nihon Ronen Igakkai Zasshi. 57, 458–466. https://doi.org/10.3143/geriatrics.57.458 (2020).
Malyutina, S. et al. Alcohol consumption and binge drinking in Novosibirsk, Russia, 1985-95. Addiction 96, 987–995. https://doi.org/10.1046/j.1360-0443.2001.9679877.x (2001).
Егиазарян, К. А., Аттаева, Ч. С. Н. & Л Ж. Анализ Структуры Первичной Заболеваемости По Классу Травмы, отравления и Некоторые другие Последствия воздействия Внешних Причин Взрослого Населения Российской федерации. Кафедра Травматологии И Ортопедии, 25–27 (2017).
Alla Ivanova, E. Z., Sabgayda, T., Semyonova, V. & Zubko, A. Irina Kryukova demographic ageing, health status and life quality of the elderly in Russia. China Popul. Dev. Stud. 7, 130–159 (2023).
Acknowledgements
We appreciate the contributions made by GBD study in Data.
Funding
This study was funded by the Special Project for Popularization of Science of Jiangxi Provincial Social Science Foundation in 2022 (Project No. 22KP16).
Author information
Authors and Affiliations
Contributions
LXY: Conceptualization, Methodology, Software, Validation,Writing - Original Draft,Visualization,Conceptualization,Investigation, Formal analysis. ZQX: Conceptualization, Methodology, Software,Validation,Formal analysis,Data Curation,Visualization,Investigation, Writing - Review & Editing. GHG: Supervision,Project administration,Data Curation,Writing - Review & Editing. DWL:Supervision,Project administration,Data Curation,Writing - Review & Editing. YYD: Formal analysis,Investigation,Writing - Review & Editing. SHC: Formal analysis,Investigation,Writing - Original Draft. XQW: Formal analysis,Writing - Original Draft,Investigation. ZQW: Conceptualization,Visualization,Formal analysis. PYZ: Conceptualization, Methodology, Software,Validation,Data Curation. ZY: Conceptualization,Writing - Review & Editing,Supervision,Project administration,Funding acquisition,Validation,Investigation. XHD: Conceptualization,Writing - Review & Editing,Supervision,Project administration,Funding acquisition,Validation,Investigation. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yi, L., Xie, Z., Wang, Z. et al. Time trends in thermal burns incidence among Brazil, Russia, India, China, and South Africa (BRICS), an age-period-cohort analysis from the GBD 2019. Sci Rep 15, 6877 (2025). https://doi.org/10.1038/s41598-025-90935-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-90935-y
