
Abstract
Consuming foods high in vitamin A and iron is crucial for children’s growth and well-being. However, deficiencies remain a public health problem in Bangladesh. This study explores spatial variation and determinants of vitamin A and iron-rich food consumption among children aged 6–23 months. In this study, data from 2528 children from the Bangladesh Demographic and Health Survey (BDHS) 2022 was used. BDHS 2022 employed a cross-sectional study design to collect data. The outcomes measured were vitamin A and iron-rich foods consumption within 24 h preceding the survey by including factors such as mother’s age, education, occupation, child age, sex, Antenatal care (ANC) visits, medical illness (diarrhea, fever, cough), use of deworming drugs, wealth index, place of residence, division etc. Spatial patterns were analyzed with ArcGIS version 10.8 and associated factors were assessed using multilevel mixed effect logistic regression model. The prevalence of vitamin A and iron-rich foods consumption was 72% (95% CI 0.70–0.74) and 61.8% (95% CI 0.60–0.64) respectively. Clustering of vitamin A (Moran’s I: 0.055, p < 0.001) and iron-rich food (I: 0.101, p < 0.001) consumption was observed, with hot spots in Rangpur, Rajshahi, and Khulna. From the mixed effects logistic regression analysis, maternal employment (aOR = 1.6; 95% CI 1.2–2.0), maternal education (aOR = 2.0; 95% CI 1.1–3.5), paternal education (aOR = 2.0; 95% CI 1.4–3.0), ≥ 4 ANC visits (aOR = 1.7; 95% CI 1.1–2.6), older children aged 18–23 months (aOR = 4.0; 95% CI 3.0–5.3), deworming drugs (aOR = 1.6; 95% CI 1.2–2.2) and residing in Khulna (aOR = 2.3; 95% CI 1.5–3.5), Rajshahi (aOR = 1.9; 95% CI 1.2–2.9) have shown statistically significant association with increased consumption of vitamin A and iron-rich foods. Furthermore, a lower likelihood of iron-rich food consumption was observed among children having diarrhea (aOR = 0.7; 95% CI 0.5–0.9), compared to children who didn’t have diarrhea. Poor consumption of vitamin A-rich foods was found in Chittagong (aOR = 0.6; 95% CI 0.4–0.98) and Sylhet (aOR = 0.6; 95% CI 0.4–0.9). The findings revealed significant disparities both in regions and protective factors associated with vitamin A and iron-rich food intake among children in Bangladesh. Understanding these spatial variations and key determinants can guide targeted interventions, particularly in cold spot regions, to improve child nutrition in Bangladesh.
Similar content being viewed by others

Introduction
Vitamin A and iron deficiencies continue to be significant public health concerns worldwide, particularly in low- and middle-income countries (LMICs) such as Bangladesh. Vitamin A deficiency (VAD) contributes to blindness in 250,000–500,000 children each year and is responsible for an estimated one million childhood deaths annually1. An estimated 190 million (33.3%) preschool children are vulnerable to VAD, with 124 million children requiring vitamin A-rich foods or supplements1,2. Additionally, 269 million (39.8%) under-five children experience anemia3, with 25% of these cases attributed to iron deficiency4. Iron deficiency anemia (IDA), one of the most severe forms of iron deficiency, develops when a person does not have enough iron in his/her body to produce healthy red blood cells5. IDA affects 20–25% of preschool children worldwide6.
Despite global efforts to reduce VAD, it still remains high in South Asia, with nearly 30–50% of preschool children experiencing malnutrition and VAD; which contributes to high mortality rates in Bangladesh and India7. Also, 21.1% of children under the age of five in Bangladesh continue to suffer from anemia8. A recent survey in 2019-20 also revealed that 42.8% of children under five were mildly deficient (serum retinol 10–19 µg %) and 7.2% were moderately deficient (serum retinol 20–30 µg %). VAD was higher in children aged 6–23 months (60.7%) than those aged 24–59 months (46.3%). Additionally, 15.1% were iron deficient with a prevalence of 31.3% in children aged 6–23 months compared to 9.1% in those aged 24–59 months8.
Vitamin A and iron both play a vital role in early childhood development. Vitamin A supports vision, reproduction, immune function, cellular differentiation, gene expression9, while iron is critical for cognitive development and the central nervous system by acting as a cofactor in neurotransmitter synthesis and supporting brain energy metabolism10. Since these nutrients cannot be synthesized by the human body, children rely on dietary sources to meet the recommended daily intake of 400–700 µg of vitamin A9 and 10–12.5mg of ferrous iron11. Inadequate intake of both vitamin A and iron during the first two years of life can result in often irreversible health outcomes that include a higher susceptibility to infections, cognitive impairments, anemia, stunted growth, weakened immune systems, and even mortality12,13.
While supplementation efforts have been implemented to help prevent vitamin A and iron deficiencies, supplementation alone may not be beneficial. Vitamin A supplements provide only temporary relief from VAD and do not offer the same benefits as naturally occurring vitamin A found in foods14. Similarly, iron supplementation can pose risks, such as increasing susceptibility to bacterial infections that cause diarrhea and disrupting gut microbiota15. However, in populations with severe deficiencies or limited food access, supplementation is the only preventive measure that can provide immediate relief and limit complications, especially in children and pregnant women9,13. The best approach would be to combine supplementation with dietary approaches to ensure sustainable outcomes. This dual approach, along with vitamin C-rich foods that enhance iron absorption, is a cornerstone and foundation of global public health efforts16. Therefore, sustainable food-based agricultural production, diverse dietary practices, and food fortification are essential to combat these deficiencies17.
The Sustainable Development Goal (SDG)−2 aims to eradicate all forms of malnutrition and ensure access to nutritious food by 203018. Despite Bangladesh’s progress in economic growth and hunger reduction, the country faces a double burden of malnutrition, with both undernutrition and overnutrition contributing to nutritional deficiencies in children19. Poor infant and young child feeding practices, limited dietary diversity, and minimal bioavailability of micronutrient-rich foods further exacerbate these issues. Additionally, limited knowledge among parents and persistent infections compound these challenges of achieving optimal child nutrition20,21.
Several key determinants of children’s vitamin A and iron-rich foods consumption include mother’s age, occupation, education, child age, child sex, birth order, media exposure, wealth index, antenatal and postnatal care, place of delivery, common childhood illness like diarrhea, cough, intestinal parasites, place of residence, administrative division2,12,13,22. However, there is a lack of research investigating the spatial distribution of vitamin A and iron-rich food consumption among children in Bangladesh. Geospatial analysis, using Geographic Information Systems (GIS), can help identify hot spots and cold spots of nutrient-rich food consumption among children. Hot spots are defined as clusters of high data values while cold spots are clusters of low data value. Hot and cold spots can help detect areas with high and low prevalence of vitamin A and iron-rich food consumption among children in specific regions of Bangladesh23.
A few studies have highlighted the determinants of VAD24, vitamin A supplement coverage25, the subclinical vitamin A nutrition status26 and determinants contributing to anemia in Bangladesh27,28. However, there is a paucity of studies that inspect the spatial distribution and identify the factors that influence the dietary consumption of vitamin A and iron-rich food among children 6–23 months in Bangladesh. Therefore, this study aims to address this gap by exploring the spatial variation and determinants of vitamin A and iron-rich food consumption among children aged 6–23 months in Bangladesh using nationally representative data.
Materials and methods
Study settings, data source, study design, and participants
Bangladesh, located in the northeastern part of South Asia (20° 34’−26° 38’ N, 88° 01’−92° 41’ E), is one of the most densely populated countries, with a population of 165.2 million, including 15.6 million children under the age of five. It comprises of 64 districts along with eight administrative divisions: Dhaka, Mymensingh, Barishal, Khulna, Sylhet, Rajshahi, Rangpur, and Chattogram. Each division is denoted by the major city within its jurisdiction acts as the administrative capital for that division29. The Demographic and Health Survey (DHS) conducted its ninth national survey in Bangladesh to provide key insights into the health and demographics of women and their families30.
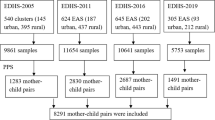
This study utilized data from a secondary source of Bangladesh Demographic and Health Survey (BDHS) 2022. The BDHS 2022 is a nationally representative cross-sectional survey conducted by the National Institute of Population Research and Training (NIPORT), and the Health Education and Family Welfare Division of the Ministry of Health and Family Welfare, Bangladesh30. The BDHS 2022 employed a two-stage stratified sampling approach. Initially, 675 enumeration areas (EAs) were chosen, with 237 in urban areas and 438 in rural areas, using probability proportional to size. Subsequently, 45 households were systematically selected from each EA, resulting in a total sample of about 30,375 households. In this survey, interviews were conducted with 30,078 ever-married women aged 15 to 49 years to gather information regarding reproductive health, child health, feeding and nutritional indicators that cover all administrative divisions of Bangladesh. The EAs were considered as clusters and primary sampling units (PSUs) of the survey. We utilized the Kids Recode (KR) file of the BDHS 2022 dataset that included information on the health, and nutrition of 8,784 children aged 0–59 in Bangladesh30. In this study, children aged 6–23 months who were alive, last born and living with their caregivers during the survey were included. The final sample size was weighted to adjust for differences in the probability of selection and interview between cases in the sample, ensuring the data was representative both at the national and division level. A detail of the sample selection is shown in Fig. 1.

Sample selection of children aged 6–23 months in Bangladesh, BDHS 2022.
Outcome variable
The study focuses on two outcome variables: vitamin A and iron-rich foods consumption among children aged 6–23 months. The BDHS 2022 data collection took place from June 27 to December 12, 2022. Twenty teams comprising supervisors, interviewers, health technicians, and logistics staff participated in the country-wide data collection process through interviews. During the interview process, individuals were asked about vitamin A and iron-rich food consumption within 24 hours preceding the interview. Vitamin A-rich food consumption was assessed by asking their mother if the child ate any vitamin A-rich foods like eggs; meat (beef, pork, lamb, chicken, etc.); pumpkin, carrots, squash (yellow or orange inside); any dark green leafy vegetables; mangoes, papayas, other vitamin A fruits; liver, heart, other organs; fish or shellfish, at any time in the past 24 hours preceding the interview. If at least one such food was consumed, it was coded as ‘Yes’, otherwise a ‘No’ was noted31.
If the child had eaten at least one of the iron-rich foods, including eggs; meat (beef, pork, lamb, chicken, etc.); liver, heart, other organs; fish or shellfish, at any time in the last 24 h preceding the interview, then it was categorized as “Yes = 1”, otherwise “No = 0” iron-rich food consumption13,32. Since the study aimed to assess the determinants associated with the consumption of vitamin A and iron-rich foods among children aged 6–23 months, a response of “yes” was coded as 1 and “no” was coded as 0.
Explanatory variables
The explanatory variables were grouped into two categories: individual- and community-level variables. Individual-level variables included: the age of the respondents33, maternal occupational status13, maternal educational status34, husband/ partner’s educational status34, household family size35, child’s medical illness (diarrhea, fever, short, rapid breathing)13,34, age of the child33, child sex33, birth order36, use of maternal health services, (antenatal care (ANC)37, post-natal-check (PNC) within 2 months38, place of delivery33), household wealth index36, media exposure33. The household wealth index was assessed using principal component analysis and categorized into poorest, poorer, middle and richer, richest. Media exposure was measured as ‘yes’ if the respondents have access to all three media (newsletter, radio, television) at least once a week, otherwise coded as ‘no’. These variables were classified based on prior literature. The deworming or intestinal drugs were measured for children aged 6–23 months whether they had been given for the last six months or not13. Community-level variables, such as place of residence34 and division34 were included.
Data processing and statistical analysis
Data were extracted, cleaned, recoded, and analyzed using STATA version 18.0. The data was initially adjusted for using sampling weights, primary sampling units, and strata to make the survey more representative and improve the reliability of the results. Descriptive statistics were applied to present frequencies and percentages.
Spatial autocorrelation and hot spot analysis
Global spatial autocorrelation (Global Moran’s-I) statistics was conducted to examine the spatial patterns of vitamin A and iron-rich foods consumption among children aged 6–23 months using ArcGIS version 10.8. This analysis helped to determine whether the consumption of these foods was dispersed, clustered or randomly distributed in Bangladesh. Positive Moran’s I value (close to + 1) indicates geographic clustering for the vitamin A and iron-rich foods consumption, the negative Moran’s value (close to −1) indicates dispersion, while Moran’s I value 0 indicates randomly distributed. A statistically significant Moran’s value (p< 0.05) had a chance to reject the null hypothesis, suggesting the presence of spatial autocorrelation. Hot spot analysis using the Getis-Ord Gi* Statistic calculates z-scores and p-values. These z-scores and p-values indicate whether the observed spatial clustering of high or low values is more pronounced than would be expected in a random distribution. Areas with statistically significant high z-scores represent clusters of high prevalence (hotspots), and significant low z-scores including negative values (cold spots) represent clusters of low prevalence of vitamin A and iron-rich foods consumption among children39.
Ordinary kriging Spatial interpolation
The spatial interpolation method was used to predict vitamin A and iron-rich food consumption among children in the un-sampled areas based on sampled EAs. Considering the linear trends of the prevalence of both outcomes, Kriging spatial interpolation was used to predict the prevalence of vitamin A and iron-rich foods consumption among children in the unobserved areas of Bangladesh. It generates a map of the outcome variable by forecasting it in enumerated areas.
Multilevel analysis
Since the Demographic and Health Survey data are hierarchical, it defies the assumptions of independent observation and homogeneity of variance31. So, multilevel logistic regression analysis was used for inferential statistics. The ICC (Intra-class Correlation Coefficient) value which ranges from 0 to 1, was checked for the presence of a clustering effect. ICC value greater than zero indicates the presence of a clustering effect40. Four separate models were fitted for both vitamin A and iron-rich foods consumption among children aged 6–23 months: Null model, Model I (only individual variables), Model II (only community-level variables), and Model III (both individual and community-level variables). Finally, multivariable multilevel regression analysis was conducted to estimate the likelihood of individual and community-level variables by calculating the adjusted odds ratio (aOR). We presented only Model III in this study (Table 1). Variables with p-value < 0.05 were considered statistically significant at 95% confidence intervals (CIs). For a measure of variation, median odds ratio (MOR) and proportional change in variation (PCV) were calculated, while the Akaike Information Criterion (AIC) was used to assess the model fit. The multicollinearity of predictor variables was also checked using Variation Inflation Factors (VIF < 5).
Ethical consideration
The Bangladesh Demographic and Health Survey 2022 are publicly accessible and were made available upon request to Measure DHS (http://www.dhsprogram.com). BDHS data collection procedures were approved by the Institutional Review Board (IRB) of the ICF International, Rockville, MD, USA and National Research Ethics Committee of Bangladesh. No other ethical approval is required to conduct this study using secondary data. The authorities adhered to ethical guidelines by ensuring informed consent, confidentiality, anonymity, privacy of the study participants. Furthermore, the data were not altered or used for any other purposes.
Results
Characteristics of the respondents and study children
A total of 2,528 (weighted) mothers/respondents with children aged 6–23 months were included in this study. The sociodemographic characteristics of the study participants and children aged 6–23 months are detailed in Table 2. The majority of the mothers (76.7%) were between 20 and 34 years old, had secondary education (54.7%), and had no formal employment (77.5%). Of the total children, 38.1% were aged 6–11 months, 28.8% were 12–17 months and 33.1% were 18–23 months, with half (50.2%) being male. The majority of the mothers, 52.2% and 63.2%, respectively, attended 1 to 3 ANC visits and gave birth in health facilities. However, only 41.1% of the babies received post-natal-check (PNC) within 2 months, and 34.9% of the children had a cough within the last two weeks from the time of data collection (Table 2).
Vitamin A and iron-rich foods consumption among 6–23 months aged children
Overall, 72% of children consumed foods rich in vitamin A within the previous 24 h, and 61.8% consumed foods rich in iron within the same period. Eggs were the most commonly consumed food, while the liver, heart, and other organs were the least consumed for both vitamin A and iron (Supplementary Table 01).
Spatial distribution of vitamin A and iron-rich foods taking coverage among children
The red areas on the map represent divisions with a high percentage (hot spot areas) of children aged 6–23 months who consume vitamin A and iron-rich foods, while blue areas (cold spot areas) indicate divisions with a low percentage of such children. From Fig. 2a and 2b Rangpur, Rajshahi, and Khulna were identified as hotspot areas for the consumption of both vitamin A and iron-rich foods among children aged 6–23 months whereas Sylhet was pinpointed as a cold spot for vitamin A-rich food, Sylhet and Barishal were noted as cold spot areas for iron-rich food consumption. The global Spatial autocorrelation analysis showed that the spatial distribution of vitamin A (Global Moran’s Index: 0.055; z-score: 3.390; p < 0.001) and iron (Global Moran’s Index: 0.101; z-score: 6.134; p < 0.001) rich foods consumption among children aged 6–23 months were clustered and non-random in Bangladesh (Supplementary Fig. 1a and Fig. 1b).

(a) ArcGIS version 10.8 (https://www.arcgis.com/index.html) result for the spatial distribution of consuming vitamin A-rich food among children aged 6–23 months in Bangladesh, 2022. (b) ArcGIS version 10.8 (https://www.arcgis.com/index.html) result for the spatial distribution of consuming iron-rich food among children aged 6–23 months in Bangladesh, 2022.
The result of the Kriging interpolation approach predicted the highest and lowest coverage of vitamin A and iron-rich foods consumption among children aged 6–23 months. The highest predicted prevalence of children consuming vitamin A-rich foods (ranging from 88 to 98%) was found in Rangpur, Rajshahi, and Khulna while the lowest predicted prevalence (40–50%) was detected in Sylhet (Fig. 3a). Comparably, Rajshahi and Khulna were predicted to have a high prevalence (ranging from 84 to 95%) whereas Sylhet, Barishal, and some of the regions of Dhaka were predicted to have a low prevalence (31–42%) of children consuming iron-rich foods in Bangladesh (Fig. 3b).

(a) ArcGIS version 10.8 (https://www.arcgis.com/index.html) result for the spatial interpolation of vitamin A-rich food consumption among children aged 6–23 months in Bangladesh, 2022. (b) ArcGIS version 10.8 (https://www.arcgis.com/index.html) result for the spatial interpolation of iron-rich food consumption among children aged 6–23 months in Bangladesh, 2022.
Determinants of vitamin A-rich foods consumption among children
Children whose mothers/ caregivers had formal employment were 1.6 (aOR = 1.6; 95% CI 1.2–2.0) times, and those with secondary and higher education were 1.7 times (aOR = 1.7; 95% CI 1.04–2.6) and 2.0 times (aOR = 2.0; 95% CI 1.2–3.5) respectively, more likely to consume vitamin A-rich foods compared to their counterparts. Similarly, children whose fathers attained primary education had 40% higher odds of consuming vitamin-rich foods (aOR = 1.4; 95% CI 1.01–1.9), and those with higher education had 70% (aOR = 1.7; 95% CI 1.1–2.6) of higher odds than those who had no education. Looking at the frequency of ANC visits, children whose mothers attended 4–7 ANC visits were 1.7 (aOR = 1.7; 95% CI 1.1–2.6) times more likely to consume vitamin A-rich foods than their counterparts. In terms of age, the odds of vitamin A-rich foods consumption were 2.5 (aOR = 2.5; 95% CI 1.9–3.2) and 4.0 (aOR = 4.0; 95% CI 3.0–5.3) times higher for the age groups of 12–17 months and 18–23 months, respectively as compared with children aged 6–11 months. The result also shows that the odds of consuming vitamin A-rich foods among children who took medication for intestinal parasites were increased by 60% (aOR = 1.6; 95% CI 1.2–2.2) compared to children who did not take the medication. At the community-level, children residing in the Chittagong (aOR = 0.6; 95% CI 0.4–0.98) and Sylhet division (aOR = 0.6; 95% CI 0.4–0.9) were less likely to consume vitamin A-rich foods than those who resided in Barishal (Table 1).
Determinants of iron-rich foods consumption among children
For children whose mothers/caregivers had employment and higher education, the odds of consuming any one of the iron-rich foods were increased by 40% (aOR = 1.4; 95% CI 1.1–1.7) and 70% (aOR = 1.7; 95% CI 1.01–2.9), respectively, as compared with their counterparts. Similarly, children whose fathers had primary, secondary and higher education were 1.4 times (aOR = 1.4; 95% CI 1.1–1.9), 1.4 times (aOR = 1.4; 95% CI 1.01–1.9) and 2.0 times (aOR = 2.0; 95% CI 1.4–3.0) respectively, more likely to consume iron-rich foods than those who had no education. Children from wealthier households had 1.4 times (aOR = 1.4; 95% CI 1.02–2.0) higher odds of consuming iron-rich foods than those from the poorest households while children born to mothers who attended 4–7 and 8 or more ANC visits were 1.7 times (aOR = 1.7; 95% CI 1.2–2.5) and 1.9 times (aOR = 1.9; 95% CI 1.1–3.4) higher than their counterparts. The result also shows that the odds of receiving any one of the iron-rich foods were 2.4 (aOR = 2.4; 95% CI 1.9–3.0) times higher for children aged 12–17 months and 3.9 (aOR = 3.9; 95% CI 3.0–5.0) times higher for the children aged 18–23 months, compared to children aged 6–11 months. Children with diarrhea were 30% (aOR = 0.7; 95% CI 0.5–0.9) less likely to consume iron-rich foods, while those who took drugs for intestinal worms in the last 6 months were 50% (aOR = 1.5; 95% CI 1.2–2.0) more likely to do so, than their counterparts. Regarding community-level variables, children in Khulna (aOR = 2.3; 95% CI 1.5–3.5) and Rajshahi (aOR = 1.9; 95% CI 1.2–2.9) were more likely to consume iron-rich foods compared to those in Barishal (Table 1).
Discussion
The consumption of vitamin A and iron-rich foods among children aged 6–23 months in Bangladesh is 72% and 61.8%, respectively. Based on the Bangladesh Demographic and Health Survey, vitamin A-rich food consumption among children was 77% in 2017-18, while iron-rich food consumption was 70% in the same periods41. Studies have also revealed a decline in the consumption of meats, fish, and vitamin A-rich fruits compared to previous years42,43. Factors driving this decline include food inflation or higher food prices44 and child food poverty, which affects two-thirds of children under five. As a result, approximately 10 million children consume fewer than the five recommended food groups45. Low socio-economic status, food insecurity and changing food intake behaviors can be attributed to reduced consumption20,46. Compared to other countries in South Asia, the consumption rate is higher than in Nepal47, Sri Lanka48 and India31.
The study found that the children of working mothers were more likely to consume vitamin A and iron-rich foods compared to their counterparts, which concurred with the previous study13,33,38,49. This may be attributed to cash earnings that enable mothers to provide their children with vitamin A and iron-rich meals50. On top of that, working mothers tend to have higher education, economic status, and access to information from colleagues, all of which are positively associated with improved diet quality and enhanced nutrition knowledge51,52.
Mothers’ higher education is a significant predictor of vitamin A and iron-rich food consumption among children, corroborating studies conducted in other countries2,36,49,53,54. Much research has shown the direct influence of maternal education on the health and development of children as educated mothers are more likely to provide nutrient-rich food due to greater awareness of nutrition55, healthier dietary practices42, dietary information-seeking behaviors2, avail more ANC services56, and are better positioned to make decisions about food purchases for their children57.
Fathers having higher education are more likely to provide vitamin A and iron-rich foods to children compared to their counterparts which is consistent with other studies22,33,54. While mother-child dynamics are often prioritized, the critical role of both paternal and maternal education in improving children’s diets with vitamin A and iron is emphasized in several studies. These studies also highlighted an inverse association between parent education and child undernutrition58,59,60. In patriarchal societies like Bangladesh, fathers as household heads and decision-makers61, play a crucial role in influencing their children’s consumption of nutrient-rich foods. Moreover, educated couples tend to share financial and childcare responsibilities more equally and gain a deeper insight into children’s feeding practices, thereby reinforcing the findings22,33,60.
Children born to wealthy families were more likely to have good iron-rich foods consumption than those from low-income households, which aligns with previous studies22,36. This disproportion is clearly due to the higher economic status enabling access to and affordability of iron-rich food, a barrier faced by families with lower wealth indices22.
ANC visits predict vitamin A and iron-rich food consumption among children. This aligns with previous studies that revealed that mothers who had four or more ANC visits were observed to have higher odds of providing vitamin A and iron-rich foods to children2,13,22,38,47. The possible explanation might be that more frequent ANC visits are likely to increase nutrition counselling from health professionals and provide the opportunity to learn about healthy child nutrition38,56.
Children aged 12–17 months and 18–23 months have higher odds of vitamin A and iron-rich food consumption compared to those aged 6–11 months22,49,53. Mother’s perceptions, traditional beliefs, taboos, and practices might result in reduced consumption of foods rich in vitamin A and iron for children aged 6–11 months62as many mothers avoid animal-source foods for children under one year and offer more frequently to those older than 24 months47. Older children also benefit from the family meals through traditional shared plate eating, which enhances the dietary diversity63. Moreover, there have been trends towards later weaning practices among women, leading to delays in introducing solid foods to children64.
The use of deworming for intestinal parasites in the last 6 months for children aged 6–23 months has higher odds of consuming vitamin A and iron-rich foods than those without. This finding corresponds with studies on iron-rich food consumption among children from sub-Sahara Africa22, Uganda65, and Sierra Leone13. While the association between deworming and vitamin A-rich food consumption remains uncertain, this discrepancy could be explained by the role of deworming in eliminating worms, which prevents malabsorption and malnutrition, consequently enhances children’s overall dietary consumption of vitamin A and iron66. Deworming also enhances children’s appetite as the study suggests it increases the consumption of iron-rich foods65.
Children who had diarrhea were less likely to consume iron-rich foods among children as compared to their counterparts. The association between diarrhea and reduced iron-rich food consumption in children has not been widely reported in previous studies. A possible explanation is that diarrhea might hinder feeding due to appetite loss as well as the parent’s perception that feeding during illness could be detrimental to the child’s health48.
The spatial analysis and multivariable regression analysis revealed that, among the eight divisions, the significant hotspots for the consumption of vitamin A and iron-rich foods among children were identified in Rajshahi, Rangpur, and Khulna. In contrast, Sylhet and Chittagong were noted as a cold spot for vitamin A-rich food consumption, while both Sylhet and Barishal were observed as cold spots for iron-rich food consumption among children. This pattern aligns with other studies conducted in Bangladesh34,67,68. Production of micronutrient-rich small fishes such as “Mola”, “Darkina”, and “Dhela” has increased in Rangpur and Rajshahi, making a major contribution to children’s mineral and vitamin intake in those regions69,70. These small fishes are good sources of iron, vitamin A, and folic acid, which play pivotal roles in the physical and cognitive development of children. Moreover, the adult literacy rate exceeds 70% in these regions and Rangpur, Rajshahi, and Khulna have also made progress in reducing the poverty rate29. Moreover, the nutrition knowledge among parents is comparatively higher in Ragnpur and Rajshahi comapared to other divisions71,72. These likely explain the higher odds of vitamin A and iron-rich food consumption among children in those regions69. Conversely, declining consumption of vitamin A and iron-rich foods in Sylhet and Chittagong might be attributed to socio-economic factors. Despite increasing adult literacy rates (> 70%), the malnutrition and unemployment rate remains high in Sylhet and poverty has also increased in Sylhet and Barishal29. 68% of Sylhet’s population and one in two people in Chittagong live below the poverty line, making it remarkably difficult for many families to afford nutrient-rich foods. Another contributing factor is the poor knowledge of nutrition among physicians and parents particularly in Sylhet, which leads to lower consumption of nutrient-rich foods in the region73. To mitigate this situation, many national and international programs are actively promoting the consumption of locally available fish and vegetables to improve dietary diversity and combat malnutrition68,74. Moreover, disparities in education, occupation, socio-economic status and income levels in different regions in Bangladesh might influence the consumption of nutrient-rich foods among children.
Strengths and limitations of the study
This study has the strength of addressing a previously unexplored area in Bangladesh, providing a comprehensive analysis of the spatial patterns and determinants of consuming vitamin A and iron-rich foods in children aged 6–23 months using large country representative data. Using the 24-hour food consumption recall method also helps to minimize the chance of recall bias. Nonetheless, this study also has limitations that should not be overlooked. As a cross-sectional study, it fails to explain the causal association between independent and outcome variables and requires further research for a more thorough understanding. There are constraints related to respondents’ recall bias, insufficient data on bioavailability, seasonal variability, affordability, use of the internet to get relevant knowledge, and difficulty in determining both the quantity and quality of dietary sources, etc. Another limitation of this study was that coordinates were gathered at the clustered level instead of the individual level, which is challenging to obtain for the individual level. Excluding clusters without coordinates may also introduce selection bias. Besides, ordinary Kriging operates under the assumption that data follows a linear trend, which isn’t always true. As a result, non-linear relationships might necessitate more sophisticated modelling techniques. Additionally, the accuracy of Kriging estimates can be influenced by the number and distribution of sample points, whether they are sparsely distributed or clustered. These limitations may reduce the generalizability of the study.
Conclusion
The present study highlighted that more than half of the children aged 6–23 months consumed foods high in vitamin A (72%) and iron (61.8%), though the dietary practices are still below WHO’s recommendation. Various factors at both individual (educational status of parents, working status of mothers, ANC visits, child age, taking deworming drugs, history of diarrhea) and community level including divisions influenced adequate consumption of nutrient-rich foods. Future research and interventions to promote vitamin A and iron-rich food intake should particularly focus on children whose parents are uneducated, unemployed, from low-income households, and to those aged between 6 and 11 months while encouraging women to attend more ANC visits. Future interventions could be designed focusing on enhancing parental education, raising awareness on child feeding, disseminating nutrition messages through media, offering parental guidance and counseling, providing access to community-based programs, and promoting locally available indigenous vitamin A and iron-rich foods. Regions with lower prevalence of vitamin A and iron-rich foods consumption, Sylhet, Chittagong, and Barishal require coordinated efforts from governments, healthcare providers and programmers to improve access to nutrient-dense foods. Moreover, these insights can aid policymakers in designing effective strategies to enhance the consumption of vitamin A and iron-rich foods among children aged 6–23 months.
Data availability
Data availabilityThe datasets are publicly available in the Bangladesh Demographic and Health Survey data repository, 2022, from the (http://www.dhsprogram.com).
Abbreviations
- ANC:
-
Antenatal care (ANC) is essential care a woman receives from health professionals during pregnancy. It is also known as pregnancy care or maternity care
References
Song, P. et al. The prevalence of vitamin A deficiency and its public health significance in children in low- and middle-income countries: A systematic review and modelling analysis. J. Glob Health 13, 04084 (2023).
Merid, M. W. et al. Wealth-related inequality in vitamin A rich food consumption among children of age 6–23 months in Ethiopia; Wagstaff decomposition of the 2019 mini-DHS data. PLOS One 19, e0302368 (2024).
Hailu, M. K., Wudu, M. A., Gebriye, D. B., Birhanu, T. A. & Bekalu, Y. E. Prevalence of Anemia and its associated factors among 6–59 months age children visiting public hospitals at Afar region, Northeast Ethiopia: A hospital-based cross-sectional study. BMC Pediatr. 24, 589 (2024).
Yadav, K. et al. Prevalence and determinants of anemia due to micronutrient deficiencies among children aged 12–59 months in India—evidence from comprehensive National nutrition survey, 2016–18. PLOS Glob. Public. Health 4, e0002095 (2024).
Anemia - Iron. -Deficiency Anemia | NHLBI, NIH (2022). https://www.nhlbi.nih.gov/health/anemia/iron-deficiency-anemia
Gedfie, S., Getawa, S. & Melku, M. Prevalence and associated factors of Iron deficiency and Iron deficiency anemia among under-5 children: A systematic review and meta-analysis. Glob. Pediatr. Health 9, 2333794X221110860 (2022).
Kumar, R., Oruna-Concha, M. J., Niranjan, K. & Vimaleswaran, K. S. A review on vitamin A deficiency and depleted immunity in South Asia: From deficiency to resilience. Nutrition 124, 112452 (2024).
Institute of Public Health Nutrition (IPHN), National Micronutrient Survey in Bangladesh 2019–2020. Dhaka, Bangladesh: IPHN, Icddr,b, Global Allaince for Improved Nutrition (GAIN), Nutrition International, and National Nutrition Services (2021). Https://Nnsop.Gov.Bd/Storage/Files/File-2023-08-08-64d1dbdd5fb30.Pdf.
Awasthi, S. & Awasthi, A. Role of vitamin A in child health and nutrition. Clin. Epidemiol. Glob. Health 8, 1039–1042 (2020).
Kulaszyńska, M., Kwiatkowski, S. & Skonieczna-Żydecka, K. The Iron metabolism with a specific focus on the functioning of the nervous system. Biomedicines 12, 595 (2024).
Andersen, C. T. et al. Oral iron supplementation and anaemia in children according to schedule, duration, dose and cosupplementation: A systematic review and meta-analysis of 129 randomised trials. BMJ Glob. Health 8, e010745 (2023).
Kundu, S., Rai, B. & Shukla, A. Prevalence and determinants of vitamin A deficiency among children in India: Findings from a national cross-sectional survey. Clin. Epidemiol. Glob. Health 11, 100768 (2021).
Semagn, B. E., Gebreegziabher, Z. A. & Abebaw, W. A. Iron-rich food consumption and associated factors among children aged 6–23 months in Sierra Leone: Multi-level logistic regression analysis. BMC Public. Health 23, 1793 (2023).
Hamer, D. H. & Keusch, G. T. Vitamin A deficiency: Slow progress towards elimination. Lancet Glob. Health 3, e502–e503 (2015).
Cross, J. H. et al. Oral iron acutely elevates bacterial growth in human serum. Sci. Rep. 5, 16670 (2015).
Skolmowska, D. & Głąbska, D. Effectiveness of dietary intervention with iron and vitamin C administered separately in improving iron status in young women. Int. J. Environ. Res. Public. Health 19, 11877 (2022).
Nair, M. K., Augustine, L. F. & Konapur, A. Food-based interventions to modify diet quality and diversity to address multiple micronutrient deficiency. Front. Public. Health 3, 277 (2016).
Sustainable Development Goal 2. Zero Hunger | United Nations in Bangladesh. https://bangladesh.un.org/en/sdgs/2
Tariqujjaman, M. et al. Determinants of double burden of malnutrition among school children and adolescents in urban Dhaka: A Multi-Level analyses. Front. Public. Health 10, 926571 (2022).
Ahmed, F., Prendiville, N. & Narayan, A. Micronutrient deficiencies among children and women in Bangladesh: Progress and challenges. J. Nutr. Sci. 5, e46 (2017).
Roy, A. et al. Prevalence of infant and young child feeding practices and differences in estimates of minimum dietary diversity using 2008 and 2021 definitions: Evidence from Bangladesh. Curr. Dev. Nutr. 6, nzac026 (2022).
Akalu, Y. et al. Iron-rich food consumption and associated factors among children aged 6–23 months in sub-Saharan Africa: A multilevel analysis of demographic and health surveys. PLoS ONE 16, e0253221 (2021).
Derseh, N. M., Shewaye, D. A., Agimas, M. C., Alemayehu, M. A. & Aragaw, F. M. Spatial variation and determinants of inappropriate complementary feeding practice and its effect on the undernutrition of infants and young children aged 6 to 23 months in Ethiopia by using the Ethiopian Mini-demographic and health survey, 2019: Spatial and multilevel analysis. Front. Public. Health 11, 1158397 (2023).
Hossain, M. M., Yeasmin, S., Abdulla, F. & Rahman, A. Rural-urban determinants of vitamin A deficiency among under 5 children in Bangladesh: Evidence from National survey 2017–18. BMC Public. Health 21, 1569 (2021).
Semba, R. D. et al. Coverage of vitamin A capsule programme in Bangladesh and risk factors associated with Non-receipt of vitamin A. J. Health Popul. Nutr. 28, 143–148 (2010).
Rahman, S. et al. Vitamin A deficiency and determinants of vitamin A status in Bangladeshi children and women: Findings of a National survey. Public. Health Nutr. 20, 1114–1125 (2017).
Rawat, R. et al. Anaemia in infancy in rural Bangladesh: Contribution of iron deficiency, infections and poor feeding practices. Br. J. Nutr. 111, 172–181 (2014).
Sunuwar, D. R. et al. Factors associated with anemia among children in South and Southeast Asia: A multilevel analysis. BMC Public. Health. 23, 343 (2023).
Population and Housing Census. Bangladesh Bureau of Statistics and Informatics Division Ministry of Planning Population & Housing Census 2022 Preliminary Report Government of the People’s Republic of Bangladesh (2022).
National Institute of Population Research and Training (Bangladesh), Mitra and Associates (Firm), MEASURE DHS (Program). Bangladesh Demographic and Health Survey, 2022: Final Report. National Institute of Population Research and Training, Ministry of Health and Family Welfare (2024).
Tiruneh, S. A., Fentie, D. T., Yigizaw, S. T., Abebe, A. A. & Gelaye, K. A. Spatial distribution and geographical heterogeneity factors associated with poor consumption of foods rich in vitamin A among children age 6–23 months in Ethiopia: Geographical weighted regression analysis. PLOS ONE 16, e0252639 (2021).
WHO Guideline: Use of multiple micronutrient powders for point-of-use fortification of foods consumed by infants and young children aged 6–23 months and children aged 2–12 years. World Health Org. (2016).
Engidaw, M. T. et al. Micronutrient intake status and associated factors in children aged 6–23 months in sub-Saharan Africa. Sci. Rep. 13, 10179 (2023).
Khan, J. R., Awan, N. & Misu, F. Determinants of anemia among 6–59 months aged children in Bangladesh: Evidence from nationally representative data. BMC Pediatr. 16, 3 (2016).
Rahman, M. S., Khatun, M., Rahman, M. A., Azam, M. G. & Sultana, S. Assessing the impact of credit on rice production and food security on farm households in Bangladesh. Int. J. Innov. Res. Dev. 3, 300–308 (2014).
Beressa, G. et al. Iron-rich food consumption and predictors among children aged 6–59 months old in Ethiopia: A multilevel complex sample analysis of the Ethiopian mini-demographic and health survey 2019 data. PLOS ONE. 19, e0305046 (2024).
New guidelines on antenatal care for a positive pregnancy experience. https://www.who.int/news/item/07-11-2016-new-guidelines-on-antenatal-care-for-a-positive-pregnancy-experience
Gebremedhin, T., Aschalew, A. Y., Tsehay, C. T., Dellie, E. & Atnafu, A. Micronutrient intake status and associated factors among children aged 6–23 months in the emerging regions of Ethiopia: A multilevel analysis of the 2016 Ethiopia demographic and health survey. PLOS ONE. 16, e0258954 (2021).
How Hot Spot Analysis. (Getis-Ord Gi*) works:ArcGIS Pro; pro.arcgis.com https://pro.arcgis.com/en/pro-app/latest/tool-reference/spatial-statistics/h-how-hot-spot-analysis-getis-ord-gi-spatial-stati.htm
Ahmmed, F. et al. The trend in exclusive breastfeeding practice and its association with maternal employment in Bangladesh: A multilevel analysis. Front Public. Health 10 (2022).
National Institute of Population Research and Training (Bangladesh), Mitra and Associates (Firm), MEASURE DHS (Program). Bangladesh Demographic and Health Survey, 2017-18: Key Indicators. Dhaka: National Institute of Population Research and Training, Ministry of Health and Family Welfare. 11(3), 184 (2020).
Ali, N. B. et al. Association of food security and other socio-economic factors with dietary diversity and nutritional statuses of children aged 6–59 months in rural Bangladesh. PLoS ONE. 14, e0221929 (2019).
Kabir, I. et al. Determinants of inappropriate complementary feeding practices in infant and young children in Bangladesh: Secondary data analysis of demographic health survey 2007. Matern Child. Nutr. 8, 11–27 (2012).
Headey, D. & Ruel, M. Food inflation and child undernutrition in low and middle income countries. Nat. Commun. 14, 5761 (2023).
2 in 3 children under five in Bangladesh face child food poverty - UNICEF. https://www.unicef.org/bangladesh/en/press-releases/2-3-children-under-five-bangladesh-face-child-food-poverty-unicef
Mottaleb, K. A., Rahut, D. B., Kruseman, G. & Erenstein, O. Changing food consumption of households in developing countries: A Bangladesh case. J. Int. Food Agribus Mark. 30, 156–174 (2018).
Baek, Y. & Chitekwe, S. Sociodemographic factors associated with inadequate food group consumption and dietary diversity among infants and young children in Nepal. PLOS ONE. 14, e0213610 (2019).
Senarath, U., Godakandage, S. S. P., Jayawickrama, H., Siriwardena, I. & Dibley, M. J. Determinants of inappropriate complementary feeding practices in young children in Sri Lanka: Secondary data analysis of demographic and health survey 2006–2007. Matern Child. Nutr. 8 (Suppl 1), 60–77 (2012).
Wolde, M. & Tessema, Z. T. Determinants of good vitamin A consumption in the 12 East Africa countries using recent demographic and health survey. PLOS ONE 18, e0281681 (2023).
Poudel, S. et al. Disempowered mothers have undernourished children: How strong is the intrinsic agency? Front Public. Health 10 (2022).
Miller, J. et al. Dietary intake of working women with children does not appear to be influenced by hours of employment: A secondary analysis of the Australian health survey (2011–2013). Appetite 105, 106–113 (2016).
Onubogu, C. U. et al. Changes in breastfeeding and nutritional status of Nigerian children between 1990 and 2008, and variations by region, area of residence and maternal education and occupation. Paediatr. Int. Child. Health 36, 248–259 (2016).
Demsash, A. W. et al. Spatial distribution of vitamin A rich foods intake and associated factors among children aged 6–23 months in Ethiopia: Spatial and multilevel analysis of 2019 Ethiopian mini demographic and health survey. BMC Nutr. 8, 77 (2022).
Eshetu, H. B. et al. Individual and community-level factors associated with iron-rich food consumption among children aged 6–23 months in Rwanda: A multilevel analysis of Rwanda demographic and health survey. PLOS ONE. 18, e0280466 (2023).
Mangusho, G., Njogu, E., Baingana, R. K. & David-Kigaru, D. M. Vitamin A-related nutrition knowledge gaps and predictors among caregivers of preschool children in Eastern Uganda: A cross-sectional study. BMC Nutr. 10, 85 (2024).
Roba, A. A. et al. Antenatal care utilization and nutrition counseling are strongly associated with infant and young child feeding knowledge among rural/semi-urban women in Harari region, Eastern Ethiopia. Front. Pediatr. 10, 1013051 (2022).
Kebede, A. et al. Residential food environment, household wealth and maternal education association to preschoolers’ consumption of plant-based vitamin A-rich foods: The EAT addis survey in addis Ababa. Nutrients 14, 296 (2022).
Hossain, M. B. & Khan, M. H. R. Role of parental education in reduction of prevalence of childhood undernutrition in Bangladesh. Public. Health Nutr. 21, 1845–1854 (2018).
Semba, R. D. et al. Effect of parental formal education on risk of child stunting in Indonesia and Bangladesh: A cross-sectional study. Lancet 371, 322–328 (2008).
Nahar, M. Z. & Zahangir, M. S. The role of parental education and occupation on undernutrition among children under five in Bangladesh: A rural-urban comparison. PLOS ONE. 19, e0307257 (2024).
Chen, S. et al. Association between parental education and simultaneous malnutrition among parents and children in 45 low- and middle-income countries. JAMA Netw. Open. 6, e2251727 (2023).
Locks, L. M. et al. Using formative research to design a context-specific behaviour change strategy to improve infant and young child feeding practices and nutrition in Nepal. Matern Child. Nutr. 11, 882–896 (2015).
Domfe, C. A. et al. Objective assessment of shared plate eating using a wearable camera in urban and rural households in Ghana. Front. Nutr. 11, 1428771 (2024).
Bewket Zeleke, L., Welday Gebremichael, M. & Mehretie Adinew, Y. & Abebe Gelaw, K. Appropriate weaning practice and associated factors among infants and young children in Northwest Ethiopia. J. Nutr. Metab. 2017, 9608315 (2017).
Mokori, A., Schonfeldt, H. & Hendriks, S. L. Child factors associated with complementary feeding practices in Uganda. South. Afr. J. Clin. Nutr. 30, 7–14 (2017).
Sungkar, S., Ridwan, A. S. & Kusumowidagdo, G. The effect of deworming using triple-dose albendazole on nutritional status of children in perobatang village, Southwest Sumba, Indonesia. J. Parasitol. Res. 2017, 5476739 (2017).
Bermudez, O. I., Lividini, K., Smitz, M. F. & Fiedler, J. L. Estimating micronutrient intakes from household consumption and expenditures surveys (HCES): An example from Bangladesh. Food Nutr. Bull. 33, S208–S213 (2012).
Homegrown fish and vegetables. A solution to combat undernutrition in Bangladesh. https://worldfishcenter.org/pages/homegrown-fish-and-vegetables-solution-combat-undernutrition-in-bangladesh/
Fiedler, J. L., Lividini, K., Drummond, E. & Thilsted, S. H. Strengthening the contribution of aquaculture to food and nutrition security: The potential of a vitamin A-rich, small fish in Bangladesh. Aquaculture 452, 291–303 (2016).
Sun, D. Consumption of small fish increases in Rangpur. daily-sun (2018). https://www.daily-sun.com/printversion/details/329195
Nazrina, S. Nutritional Status of Under Five Years Children in Rangpur Cantonment (2020).
Uddin, I., Mamun, S., Nigar, S., Zaher, M. & Huq, D. A. K. O. Knowledge, attitude and practices about hidden hunger among the selected households at Rajshahi City in Bangladesh. Int. J. Biosci. IJB. 16, 2020 (2020).
Uddin, M., Islam, N. & Uddin, M. J. A survey on knowledge of nutrition of physicians in Bangladesh: Evidence from Sylhet data. South-East Asian J. Med. Educ. 2 (2008).
A healthy diet for women and children. Helvetas https://www.helvetas.org/en/bangladesh/what-we-do/how-we-work/our-projects/Asia/Bangladesh/bangladesh-poor-fighting-minorities
Acknowledgements
The authors extend deepest thanks to the DHS program for granting access to BDHS datasets and making publicly available the published DHS reports.
Author information
Authors and Affiliations
Contributions
F.S.R. contributed to the study design, acquisition of data, data analysis, result interpretation, manuscript drafting, revision, and final submission for publication. S.K. was involved in the spatial analysis, manuscript revision and interpretation. A.B.S. was involved in the idea generation, study design, supervision, review and the final approval of the submitted version of the manuscript. S.T. and T.J. were involved in multilevel analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Rima, F.S., Kundu, S., Tarannum, S. et al. Spatial variations and determinants of vitamin A and iron rich food consumption among Bangladeshi children aged 6–23 months. Sci Rep 15, 17881 (2025). https://doi.org/10.1038/s41598-025-92068-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-92068-8
Keywords
This article is cited by
-
Vitamin A rich food consumption and its predictors among children aged 6 up to 23 months old in Ethiopia
Scientific Reports (2025)
