
Abstract
We investigated whether dietary intakes of saturated fat (SFA), monounsaturated fat (MUFA), or polyunsaturated fat (PUFA) were associated with plasma inflammatory markers among breast cancer survivors in Korea. This cross-sectional study included 419 female breast cancer survivors aged 30 to 78 years. Dietary intake was assessed using 3-day dietary records (DRs) or food frequency questionnaires (FFQs). Plasma levels of adiponectin, high-sensitivity C-reactive protein (hs-CRP), interleukin (IL)-6, IL-8, and tumor necrosis factor (TNF)-α were measured. We calculated an inflammatory composite score by summing the z-scores of each inflammatory marker, with adiponectin assigned a negative sign. Least-squares means (LS-means) and 95% confidence intervals (CIs) of inflammatory markers were estimated according to SFA, MUFA, and PUFA intakes using the generalized linear models. We found that increasing dietary MUFA intake was associated with increasing levels of adiponectin, but decreasing levels of hs-CRP (p for trend = 0.042 and 0.032, respectively). Similarly, higher dietary PUFA intake was associated with higher levels of adiponectin (p for trend = 0.023), but lower levels of hs-CRP and inflammatory composite score (p for trend < 0.001 and 0.036, respectively). However, no significant associations were found between SFA intake and plasma inflammatory markers. In conclusion, our results suggest that a higher intake of MUFA or PUFA is associated with a more favorable inflammatory profile among Korean female breast cancer survivors, which may potentially help in managing chronic inflammation.
Similar content being viewed by others

Introduction
Breast cancer is the most frequently diagnosed cancer among women globally, accounting for 24.5% of all cancer diagnoses in women in 20201. In Korea, the age-standardized incidence rate of breast cancer in women has been on a steady increase, reaching 59.9 per 100,000 in 20202. The expansion of health screenings, promoting early detection, in conjunction with advancements in treatment modalities3,4, significantly improved the 5-year relative survival rate for breast cancer in Korea, which escalated from 79.3% in 1993–1995 to 93.8% in 2016–20202. The rising incidence and improved survival rates of breast cancer emphasize the importance of long-term prognosis management.
Inflammation affects various physiological and pathological processes involved in the development and progression of cancer and acts as an important predictor of prognosis5. Inflammation can induce mutations, genomic instability, epigenetic modifications, angiogenesis, and immunosuppression, thereby promoting tumor formation and the proliferation of premalignant cells, which can lead to cancer development and metastasis6. Consequently, these mechanisms can significantly influence the prognosis of cancer patients. It has been suggested that certain inflammatory markers including C-reactive protein (CRP), interleukin (IL)-6, or tumor-associated inflammatory indicators, are related to the survival rates of cancer patients7,8,9. The hypothesis that inflammation predisposes to cancer prognosis has also been corroborated in studies involving breast cancer survivors10,11,12. For instance, a meta-analysis revealed that there was a significant decrease in overall survival, disease-free survival, and cancer-specific survival with an increase in CRP levels10. Furthermore, levels of adiponectin have been identified as associated with improvements in both overall and disease-free survival rates11.
Fats, as essential components of the human diet, play crucial roles in various physiological processes13. The fatty acids are not only indispensable for normal cellular functions but also significantly influence inflammatory pathways14,15. Saturated fatty acids activate the toll-like receptor 4 and the nuclear factor-κB pathways, leading to an increase in pro-inflammatory cytokines16. In contrast, monounsaturated fatty acids activate the peroxisome proliferator-activated receptors (PPARs), reducing pro-inflammatory cytokines while increasing adiponectin17. Polyunsaturated fatty acids, including dihomo-gamma-linolenic acid, arachidonic acid, and eicosapentaenoic acid, produce a variety of eicosanoids18. Among these eicosanoids, prostaglandins, whose types are determined by the originating fatty acids, exhibit varying effects on inflammation19.
To date, the collective findings from research indicating that the type and quantity of dietary fats have a greater impact on health than total fat intake20, combined with the potential effects of dietary fats on inflammation and cancer development, have facilitated further cancer prevention studies across various populations21,22,23,24. However, in breast cancer survivors, research examining the association between specific types of dietary fat intake and inflammatory markers has been limited. Therefore, we investigated the association between the intake of saturated fat (SFA), monounsaturated fat (MUFA), and polyunsaturated fat (PUFA) and the levels of plasma inflammatory markers among breast cancer survivors in Korea. Our study may provide evidence-based information that can contribute to the healthcare and improved prognosis of breast cancer survivors.
Methods
Study population
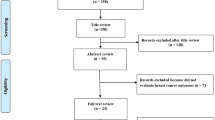
This cross-sectional study was conducted among female breast cancer survivors recruited from the five hospitals in Korea between March 2015 and June 2019, adhering to the following inclusion criteria: (1) those diagnosed with the American Joint Committee on Cancer (AJCC) stage I to III breast cancer as primary cancer, (2) those who had survived for at least six months post-surgery, (3) those without a history of recurrence or metastasis, or (4) those without any other cancer diagnosis after a breast cancer diagnosis. Among a total of 493 participants, we excluded one participant with missing data for all five inflammatory markers, and two participants with plasma high-sensitivity C-reactive protein (hs-CRP) levels exceeding 10 mg/L, which could be indicative of an acute infection or inflammatory condition25. Additionally, we excluded 68 participants who did not complete the dietary recall (DR) or food frequency questionnaire (FFQ), as well as three participants with unreliable dietary energy intake, defined as values exceeding ± 3 standard deviations (SDs) from the mean of the log-transformed energy intake. As a result, 419 participants were included in the present analysis. All methods were performed in accordance with the relevant guidelines and regulations. This study was approved by the Institutional Review Board of each participating hospital and written informed consent was obtained from all participants.
Dietary assessment
Dietary assessment was conducted using either 3-day DRs or a FFQ. Among 419 participants, 222 provided their dietary information via 3-day DRs including two weekdays and one weekend day; however, one participant completed 2-day DRs. To more accurately ascertain the amount of food and beverages consumed, we provided each participant with a food photograph booklet and an example of a 1-day DR. The foods and beverages recorded by the participants were analyzed using the Computer-Aided Nutritional Analysis Program (CAN-pro) version 4.0 (The Korean Nutrition Society, Seoul, Korea). This analysis, based on the food composition table of the Korean Nutrition Society and the Rural Development Administration26,27, allowed for the estimation of nutrients and energy content. These estimates were then calculated as the average daily intake. The diets of the remaining 197 participants were surveyed using an FFQ, validated against DRs collected over the course of a year28,29. In a validation study, the correlation coefficient for fat intake was 0.4829. Participants were asked to respond to the average frequency and amount of consumption over the past year for 123 items, categorized into nine groups. The standard portion size and nutrient content for each item were established based on the 24-hour recall data from the 2013 and 2014 Korea National Health and Nutrition Examination Survey (KNHANES) and the food composition table provided by the Korean Nutrition Society and the Rural Development Administration26,27,30.
Measurements of plasma inflammatory markers
Blood samples were collected from non-fasting participants by specialized nurses at each hospital at the study enrollment. These samples were then aliquoted and stored in a -85℃ deep freezer until subsequent assays. As the primary outcomes of this study, we included circulating levels of adiponectin, hs-CRP, IL-6, IL-8, and tumor necrosis factor (TNF)-α. All assays of inflammatory markers were carried out in external laboratories following the specified standard procedures. The measurement of adiponectin levels was performed with an enzyme-linked immunosorbent assay utilizing a microplate reader (VERSA Max, USA) at the CHA Bio Complex (CHA University, Seongnam, Korea). The intra-assay coefficients of variation (CVs) of adiponectin ranged from 4.2 to 5.0%. Plasma hs-CRP was analyzed with a particle-enhanced immunoturbidimetric assay using Cobas 8000 C702 (Roche, Germany) at the Seegene Medical Foundation (Seoul, Korea). The inter-assay CV of hs-CRP was 2.3%, and the lower limit of detection (LLOD) was 0.15 mg/L. We assigned values below the detection limit as 0.075 mg/L, which corresponds to half of the LLOD. Plasma IL-6, IL-8, and TNF-α were analyzed with multiplexing immunoassay at the Life is Art of Science laboratory (Gimpo, Korea) by using the Luminex 200 instrument (Luminex, Austin, TX, USA) and Bio-plex manager 6.0 (Bio-Rad, Hercules, CA, USA) for samples collected from 2015 to 2017, and the MAGPIX instrument (Luminex) and MasterPlex QT 2010 (MiraiBio, Hitachi, CA, USA) for samples collected from 2018 to 2019. The intra- and inter-assay CVs were 2.2% and 3.0% for IL-6, 3.2% and 2.8% for IL-8, and 3.5% and 3.0% for TNF-α, respectively.
Assessments of anthropometric, sociodemographic, lifestyle, and clinical factors
At the time of study enrollment, a professional research nurse asked the participants to complete a structured self-administered questionnaire. Through this questionnaire, information about the current height and weight, level of physical activity, education level, alcohol consumption, smoking status, and dietary supplement use was obtained. Clinical data, including the height and weight at diagnosis, the date of breast cancer diagnosis and surgery, AJCC stage, type of treatment, menopausal status at diagnosis, and types of chronic diseases before and after diagnosis, were acquired from medical records provided by each hospital. The body mass index (BMI) was determined by dividing the weight in kilograms by the height in meters squared. If height and weight information were unavailable at the time of study enrollment, BMI was calculated using measurements taken at diagnosis (n = 9). The physical activity was quantified in metabolic equivalent of task (MET) hours per week by multiplying the MET value for each type of activity by its frequency and duration, then summing these values31.
Statistical analysis
Dietary intakes of SFA, MUFA, and PUFA were calculated in grams per day, log-transformed, and then adjusted for total energy intake using the residual method32. These dietary fats were then classified into quartiles based on intake levels according to the dietary assessment methods of DRs and FFQ. Levels of plasma adiponectin, hs-CRP, IL-6, IL-8, and TNF-α were transformed by using the natural log or Box-Cox transformation to improve the normality33,34. Adiponectin, hs-CRP, and IL-6 levels were log-transformed, whereas IL-8 and TNF-α levels were modified using Box-Cox transformations with parameter values (λ) of -0.25 and 0.5, respectively. Afterward, these inflammatory markers were back-transformed to their original units to facilitate interpretation. We applied the residual method to log or Box-Cox transformed biomarkers in order to address potential differences between two measurement time points of these biomarkers. In other words, residuals were calculated in a linear regression, using log or Box-Cox transformed biomarkers as dependent variables and the time points (0 or 1) as independent variables. Because the mean of these residuals is zero, they can have both negative and positive values and thus do not clearly represent the actual level of the biomarker35. Therefore, we added the residuals derived from the aforementioned regression model to the sum of the y-intercept and the time points (0 or 1) × 0.5, thereby accounting for the individual variability captured by the residuals35. Considering the systemic intercorrelated nature of biomarkers and their utility in evaluating clinical outcomes across various disease states36,37, we also calculated an inflammatory composite score by summing the z-scores of the five individual biomarkers. The z-score of each biomarker was calculated using the formula z = (x – µ)/σ (x: the levels of inflammatory markers for each individual, µ: population mean, σ: population standard deviation). Adiponectin was added as a negative value in the inflammatory composite score because it is well known for its anti-inflammatory effect38.
We performed generalized linear models to estimate the least-squares means (LS-means) and 95% confidence intervals (CIs) of inflammatory markers according to the quartiles of SFA, MUFA, and PUFA intakes. We additionally categorized intakes into absolute cut-off values for associations that showed statistical significance. To estimate the linear trend in the LS-means of the outcome across the four categories of specific fat intake, we assigned the median value of each category as a representative value and treated these median values as continuous variables in the models. When the test of linear trend was significant, the post hoc Scheffe test was used for multiple comparisons among the groups.
In the multivariate analyses, we adjusted for the age at consent (years, continuous), center, physical activity (MET-hours/week, quartiles), total energy intake (log-transformed, kcal/day, continuous), education level (middle school or below, high school, and college or above), alcohol drinking status (non-drinkers, current drinkers), smoking status (never smokers, ever smokers), menopausal status at diagnosis (premenopausal, postmenopausal), dietary supplement use (no, yes), AJCC stage at diagnosis (I, II, and III), time since surgery (0.5 to < 2 years, 2 to < 5 years, and ≥ 5 years), radiotherapy use (no, yes), hormonal therapy use (no, yes), history of chronic disease including diabetes mellitus, cardiovascular diseases, or hypertension (no, yes). Considering that overweight and obesity are major factors in the elevation of inflammatory markers, BMI (log-transformed, kg/m², continuous) was further adjusted. All covariates were selected based on changes in both the regression coefficients (β) and LS-means, using a threshold of 7%. When we encountered missing variables, data on education level and AJCC stage at diagnosis (classified into I-III according to AJCC breast cancer stage criteria, but missing T stage information), alcohol drinking status, smoking status were allocated to the most frequent category. For dietary supplement use, a conservative approach was applied by assigning ‘no’ to the missing data. One participant, with missing menopausal status at diagnosis, was classified as postmenopausal. This classification was based on the age of 50 at breast cancer diagnosis and the consideration that the average age of menopause in Korean women is 49 years39. The missing data for smoking status was 6.4%, and the missing data for other variables adjusted in the models were below 2%.
We performed subgroup analyses by BMI (< 25 kg/m², ≥ 25 kg/m²), menopausal status at diagnosis (no, yes), AJCC stage (I, II-III), and time since surgery (< 2 years, ≥ 2 years). P for interaction was estimated by the Wald test by adding interaction terms in the multivariate models. Furthermore, we performed additional analyses to evaluate the association between dietary fat intake and the inflammatory composite score according to dietary assessment methods used. Sensitivity analyses were also conducted by excluding (1) participants with plasma hs-CRP levels below the LLOD (n = 70), (2) those with a history of diabetes mellitus or cardiovascular diseases (n = 32), or (3) those with missing covariate data (n = 36). All statistical analyses were conducted using SAS 9.4, and statistical tests were considered significant at p-value < 0.05 (two-sided).
Results
The characteristics of the study participants, categorized by quartiles of energy-adjusted intakes of SFA, MUFA, and PUFA are presented in Table 1. The average age of the participants was 52 ± 8 years (mean ± SD), with a range of 30–78 years.
The age distribution among participants was consistent across the categories of SFA, MUFA, and PUFA intake. Relative to participants with the lowest intake of SFA, those with the highest intake had a lower proportion of middle school or below in educational level and a higher proportion of current drinkers. Participants in the highest MUFA intake group were more likely to have a college or above educational level and to use dietary supplements compared to those with the lowest intake. Those with the highest PUFA intake exhibited higher physical activity levels and greater proportions of dietary supplement use and radiotherapy, compared to those in the lowest intake group.
No significant associations were found between SFA intake and plasma inflammatory markers (Table 2). When we further adjusted for BMI, the association remained null. We observed that an increase in dietary MUFA intake was associated with increasing levels of adiponectin (p for trend = 0.042) and decreasing levels of hs-CRP (p for trend = 0.032) (Table 3). These associations persisted even after further adjustment for BMI. Similarly, an increase in PUFA intake was associated with decreases in the inflammatory composite score (p for trend = 0.036) and hs-CRP levels (p for trend < 0.001), and also with elevated levels of adiponectin (p for trend = 0.023) in the multivariate model (Table 4). These associations with PUFA intake remained consistent after further BMI adjustment. When we used the absolute cut-off values for SFA, MUFA, and PUFA intakes, we observed similar associations (Supplementary information: Table S1).
In the sensitivity analyses, which excluded participants who either (1) had levels of hs-CRP below the LLOD, (2) had a history of diabetes mellitus or cardiovascular disease, or (3) had missing covariate data, the associations between specific types of dietary fat intake and inflammatory markers remained similar, as detailed in Supplementary information: Tables S2-4. The associations between specific types of dietary fat intake and the inflammatory markers according to dietary assessment methods also remained similar (Table S5). Furthermore, there were no statistically significant interactions for dietary SFA, MUFA, or PUFA intakes by BMI, menopausal status at diagnosis, AJCC stage, and time since surgery (Table S6).
Discussion
In a cross-sectional study of Korean breast cancer survivors, we did not observe a significant association between SFA intake and inflammatory markers. However, we observed that increasing MUFA intake was associated with increased levels of adiponectin and decreased levels of hs-CRP. Similarly, an increasing PUFA intake was associated with elevated adiponectin levels and reduced hs-CRP levels.
The associations between SFA intake and inflammatory markers have been inconsistent across studies. In an observational study involving patients with heart failure, a high SFA intake was associated with elevated levels of serum TNF-α (p < 0.05)40. A cross-sectional study of Malaysian breast cancer survivors reported that a dietary pattern high in SFA was linked to lower levels of adiponectin (ß: -0.410; 95% CI: -0.806, -0.014; p = 0.043)41. Additionally, a US cross-sectional study showed that high SFA intake was associated with elevated hs-CRP levels (> 3.0 mg/L) (third vs. first quartile odds ratio (OR): 1.58; 95% CI: 1.02–2.44)21. However, other cross-sectional studies, including one involving US adults and another with young Japanese women, found no association between SFA intake and hs-CRP levels. The researchers suggested that this lack of association may be due to the failure to control for chronic diseases and the low prevalence of elevated hs-CRP levels (≥ 1.0 mg/L), which was only 5.6%22,42. Also, a cross-sectional study of the EPIPorto study observed no association between SFA intake and serum adiponectin levels43. These mixed findings suggest that the association between SFA intake and inflammatory markers is complex and may be influenced by various factors such as population characteristics, the presence of chronic diseases, the distribution of specific fat intakes, and different levels of inflammation.
Regarding MUFA and PUFA intake, our study findings were in agreement with a few previous observational and intervention studies. A meta-analysis of placebo-controlled randomized clinical trials indicated that fish oil treatment led to an elevation of adiponectin levels by 0.37 µg/mL (95% CI: 0.07–0.67; p = 0.02)23. Furthermore, the Hunter Community Study (HCS) identified reduced levels of hs-CRP with high MUFA intake24, and the US National Health and Nutrition Examination Survey (NHANES) study observed lower CRP levels with high PUFA intake22. Although we were not able to distinguish between n-3 and n-6 intake partly because of the lack of a database during the study period, previous research suggests that n-3 PUFA was associated with decreased levels of CRP, IL-6, and TNF-α, and that the balance between n-3 and n-6 fatty acids may play an important role in regulating inflammation44,45. These findings highlight the potential anti-inflammatory effects of both MUFA and PUFA intake, though further research is needed to clarify their specific roles.
Our findings may be supported by biological mechanisms. Monounsaturated fatty acids activate PPARs, which modulate the expression of genes related to lipid metabolism and inflammation, including PPAR-γ and fatty acid transport protein17,46, which result in a decrease in the production of pro-inflammatory cytokines and an increase in adiponectin levels16. Regarding polyunsaturated fatty acids, their role in modulating inflammatory responses is closely linked to the generation of eicosanoids, whose types and roles in inflammation vary based on their fatty acid precursors18. Eicosanoids derived from eicosapentaenoic acid, including prostaglandin-3, prostacyclin-3, and thromboxane-3, inhibit the release of arachidonic acid from cell membrane phospholipids and aid in inflammation regulation by producing anti-inflammatory resolvins47. In contrast, eicosanoids from arachidonic acid, including prostaglandin-2, thromboxane-2, and leukotriene-4, are traditionally associated with inducing inflammation16. However, studies have shown that prostaglandin E2 may have anti-inflammatory effects and that arachidonic acid can lead to the production of anti-inflammatory mediators, including lipoxin A448,49. These mechanisms suggest that both MUFA and PUFA may play crucial roles in regulating inflammation, albeit through complex and sometimes opposing pathways.
We found that the differences in inflammatory marker levels across the quartiles of SFA intake were not substantial. The absence of significant associations in our study may partly be due to the relatively lower SFA consumption levels, which may have been insufficient to elicit a measurable effect on inflammation50. The average SFA intake of the participants in this study was 11.4 g/d [5.76% of energy (%E)], which is lower than those in Western populations. For example, in the US, the SFA intake was reported at 24.0 g/d (11.0%E)51, in Denmark 30.4 g/d (13.8%E), in Italy 24.6 g/d (11.1%E), and in France 33.5 g/d (15.1%E)52. Further, the impact of SFA on inflammation may vary depending on their chain length, which is attributed to different metabolic pathways in the body53,54. Medium-chain SFA (C ≤ 12) is directly transported to the liver where it is rapidly metabolized. However, long-chain SFA is integrated into chylomicrons in the bloodstream, leading to the formation of chylomicron remnants that may contribute to the development of atherosclerotic plaques54.
This is the first study, to our knowledge, to examine the associations between SFA, MUFA, or PUFA intake and various inflammatory markers in Korean breast cancer survivors. Our study incorporates multiple inflammatory biomarkers, including adiponectin, hs-CRP, IL-6, IL-8, and TNF-α, and offers a comprehensive evaluation of inflammatory status by generating an inflammatory composite score that accounts for the interrelated nature of these biomarkers. This methodology provides more nuanced insights and enhances the clinical relevance of the findings compared to previous research. However, this study encompasses several limitations. Firstly, as a cross-sectional design, it is limited in clearly establishing a causal relationship between fat intake and inflammatory markers. Secondly, due to the nature of the study design, there is a possibility that residual or unmeasured confounding may exist. Thirdly, the potential for misclassification exists in the estimation of fat intake. However, it is anticipated that these errors may be non-differential. Fourthly, despite the nationwide recruitment of participants in this study, the relatively small sample size and the hospital-based nature of the sample present limitations that may impede the generalizability of our findings to all breast cancer survivors in Korea. Fifthly, our study did not include a detailed analysis of specific fatty acids, including butyric acid, lauric acid, omega-3, omega-6, and arachidonic acid, partly because of the absence of detailed fatty acid intake information. Moreover, self-reported BMI and physical activity data may have some measurement errors. However, self-reported BMI has been demonstrated to generally correspond closely with actual measurements and is deemed reliable when direct measurement is not feasible55,56,57. Additionally, self-reported physical activity is widely recognized for its positive effects on biological changes and chronic diseases such as cardiovascular disease, cancer, and diabetes58,59, with our previous research demonstrating significant correlations between physical activity levels and validated health-related quality of life (HRQOL) measures60. Finally, we used both DRs and FFQs in this study, but the differing characteristics of these two methods should be considered when interpreting the results. However, considering that previous studies have shown a generally acceptable level of agreement between the two methods29, and that additional analyses in our study revealed that the associations between specific types of dietary fat intake and inflammatory composite score remained consistent regardless of the dietary assessment methods used, the impact of this difference on our findings is likely to be limited.
The observed associations between MUFA and PUFA intake and inflammatory markers suggest important implications for public health policy, clinical practice, and future research. Specifically, dietary recommendations encouraging the intake of MUFA and PUFA in breast cancer survivors may contribute to the regulation of inflammation and the improvement of long-term health outcomes, aligning with global trends that advocate for the consumption of unsaturated fats to support cardiovascular health and inflammation regulation. In clinical practice, healthcare providers may consider placing greater emphasis on the types of dietary fats consumed by breast cancer survivors, particularly by recommending foods rich in MUFA and PUFA. However, due to the inherent limitations of a cross-sectional study, caution should be exercised when interpreting these findings, as causality cannot be inferred. Consequently, future research should aim to confirm these associations through longitudinal or interventional studies, with a focus on specific fatty acids and their effects on inflammation, to refine dietary guidelines.
Conclusions
In our study of Korean female breast cancer survivors, we examined the associations between the intake of SFA, MUFA, or PUFA and plasma inflammatory markers. While no significant linear associations were found between SFA intake and inflammatory markers, higher intake of MUFA or PUFA was associated with increased levels of adiponectin and decreased levels of hs-CRP. Our study holds clinical significance by providing evidence-based information for developing dietary recommendations and intervention strategies tailored to breast cancer survivors.
Data availability
The data for this study cannot be made publicly available because the study is still ongoing, and participants were not informed during the consent process that their information would be stored in a publicly accessible database. However, the data used in this study can be made available upon reasonable request to the corresponding author.
References
Sung, H. et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71 (3), 209–249. https://doi.org/10.3322/caac.21660 (2021).
Kang, M. J. et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2020. Cancer Res. Treat. 55 (2), 385–399. https://doi.org/10.4143/crt.2023.447 (2023).
Kang, S. Y. et al. Breast Cancer statistics in Korea in 2017: data from a breast Cancer registry. J. Breast Cancer. 23 (2), 115–128. https://doi.org/10.4048/jbc.2020.23.e24 (2020).
Song, S. Y. et al. Trends in breast cancer screening rates among Korean women: results from the Korean National Cancer screening survey, 2005–2020. Epidemiol. Health 44 https://doi.org/10.4178/epih.e2022111 (2022).
Sabaawy, H. E., Ryan, B. M., Khiabanian, H. & Pine, S. R. JAK/STAT of all trades: linking inflammation with cancer development, tumor progression and therapy resistance. Carcinogenesis 42 (12), 1411–1419. https://doi.org/10.1093/carcin/bgab075 (2021).
Grivennikov, S. I., Greten, F. R. & Karin, M. Immunity, inflammation, and cancer. ;140(6):883–899. (2010). https://doi.org/10.1016/j.cell.2010.01.025
Li, Y. W. et al. Hs-CRP and all-cause, cardiovascular, and cancer mortality risk: A meta-analysis. Atherosclerosis 259, 75–82. https://doi.org/10.1016/j.atherosclerosis.2017.02.003 (2017).
Feng, L. Y. et al. Serum levels of IL-6, IL-8, and IL-10 are indicators of prognosis in pancreatic cancer. J. Int. Med. Res. 46 (12), 5228–5236. https://doi.org/10.1177/0300060518800588 (2018).
Roxburgh, C. S. D. & McMillan, D. C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 6 (1), 149–163. https://doi.org/10.2217/Fon.09.136 (2010).
Guo, L. W. et al. Prognostic role of C-reactive protein in breast cancer: an updated systematic review and meta-analysis. Int. J. Clin. Exp. Med. 9 (9), 17715–17726 (2016).
Guven, H. E., Dogan, L., Gulcelik, M. A., Gulcelik, N. E. & Adiponectin A predictor for breast Cancer survival?? Eur. J. Breast Health 15 (1), 13–17. https://doi.org/10.5152/ejbh.2018.4349 (2019).
Ahmad, N. et al. IL-6 and IL-10 are associated with good prognosis in early stage invasive breast cancer patients. Cancer Immunol. Immun. 67 (4), 537–549. https://doi.org/10.1007/s00262-017-2106-8 (2018).
Hulbert, A. J., Turner, N., Storlien, L. H. & Else, P. L. Dietary fats and membrane function: implications for metabolism and disease. Biol. Rev. 80 (1), 155–169. https://doi.org/10.1017/S1464793104006578 (2005).
Calder, P. C. Functional roles of fatty acids and their effects on human health. Jpen-Parenter Enter. 39, 18s–32s. https://doi.org/10.1177/0148607115595980 (2015).
Fritsche, K. L. The science of fatty acids and inflammation. Adv. Nutr. 6 (3), 293s–301s. https://doi.org/10.3945/an.114.006940 (2015).
Lottenberg, A. M., Afonso, M. D., Lavrador, M. S. F., Machado, R. M. & Nakandakare, E. R. The role of dietary fatty acids in the pathology of metabolic syndrome. J. Nutr. Biochem. 23 (9), 1027–1040. https://doi.org/10.1016/j.jnutbio.2012.03.004 (2012).
Ali, S. et al. Relationship between monounsaturated fatty acids and sarcopenia: a systematic review and meta-analysis of observational studies. Aging Clin. Exp. Res. https://doi.org/10.1007/s40520-023-02465-0 (2023).
Tapiero, H., Ba, G. N., Couvreur, P. & Tew, K. D. Polyunsaturated fatty acids (PUFA) and eicosanoids in human health and pathologies. Biomed. Pharmacother. 56 (5), 215–222. https://doi.org/10.1016/S0753-3322(02)00193-2 (2002).
Bagga, D., Wang, L., Farias-Eisner, R., Glaspy, J. A. & Reddy, S. T. Differential effects of prostaglandin derived from ω-6 and ω-3 polyunsaturated fatty acids on COX-2 expression and IL-6 secretion. P Natl. Acad. Sci. USA 100 (4), 1751–1756. https://doi.org/10.1073/pnas.0334211100 (2003).
Willett, W. C. Dietary fats and coronary heart disease. J. Intern. Med. 272 (1), 13–24. https://doi.org/10.1111/j.1365-2796.2012.02553.x (2012).
King, D. E., Egan, B. M. & Geesey, M. E. Relation of dietary fat and fiber to elevation of C-reactive protein. Am. J. Cardiol. 92 (11), 1335–1339. https://doi.org/10.1016/j.amjcard.2003.08.020 (2003).
Mazidi, M., Gao, H. K., Vatanparast, H. & Kengne, A. P. Impact of the dietary fatty acid intake on C-reactive protein levels in US adults. Medicine 96 (7). https://doi.org/10.1097/MD.0000000000005736 (2017).
Wu, J. H. Y., Cahill, L. E. & Mozaffarian, D. Effect of fish oil on Circulating adiponectin: A systematic review and Meta-Analysis of randomized controlled trials. J. Clin. Endocr. Metab. 98 (6), 2451–2459. https://doi.org/10.1210/jc.2012-3899 (2013).
Lai, J. S. et al. Inflammation mediates the association between fatty acid intake and depression in older men and women. Nutr. Res. 36 (3), 234–245. https://doi.org/10.1016/j.nutres.2015.11.017 (2016).
Pearson, T. A. et al. Markers of inflammation and cardiovascular disease application to clinical and public health practice - A statement for healthcare professionals from the centers for disease control and prevention and the American heart association. Circulation 107 (3), 499–511. https://doi.org/10.1161/01.Cir.0000052939.59093.45 (2003).
The Korean Nutrition Society. Food Values. Seoul (Korea): The Korean Nutrition Society. 788 (2009).
Rural Resources Development Institute, Rural Development Administration. Food Composition Table. 7th edn. (Rural Development Administration, 2006).
Shin, W. K. et al. Development of a FFQ for breast cancer survivors in Korea. Brit J. Nutr. 116 (10), 1781–1786. https://doi.org/10.1017/S000711451600372x (2016).
Moon, S. E. et al. Validity and reproducibility of a food frequency questionnaire for breast cancer survivors in Korea. Nutr. Res. Pract. 16 (6), 789–800. https://doi.org/10.4162/nrp.2022.16.6.789 (2022).
National Academy of Agricultural Science, Rural Development Administration. Korean Food Composition Table. 8th edn. (Rural Development Administration, 2011).
Ainsworth, B. E. et al. 2011 Compendium of physical activities: A second update of codes and MET values. Med. Sci. Sport Exer. 43 (8), 1575–1581. https://doi.org/10.1249/MSS.0b013e31821ece12 (2011).
Willett, W. C., Howe, G. R. & Kushi, L. H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 65 (4), 1220–1228. https://doi.org/10.1093/ajcn/65.4.1220S (1997).
Box, G. E. P. & Cox, D. R. An analysis of transformations. J. Roy Stat. Soc. B 26 (2), 211–252. https://doi.org/10.1111/j.2517-6161.1964.tb00553.x (1964).
Bickel, P. J. & Doksum, K. A. An analysis of transformations revisited. J. Am. Stat. Assoc. 76 (374), 296–311. https://doi.org/10.2307/2287831 (1981).
Willett, W. C. Monographs in Epidemiology and Biostatistics. 3rd ed. Vol. 40, Nutritional Epidemiology. 274 (Oxford University Press, 2012).
Morrison, L. et al. Inflammatory biomarker score and cancer: A population-based prospective cohort study. ;16, 80. https://doi.org/10.1186/s12885-016-2115-6 (2016).
Chi, G. C. et al. Inflammatory biomarkers predict Domain-Specific cognitive decline in older adults. ;72(6):796–803. https://doi.org/10.1093/gerona/glw155 (2017).
Ouchi, N. & Walsh, K. Adiponectin as an anti-inflammatory factor. Clin. Chim. Acta. 380 (1–2), 24–30. https://doi.org/10.1016/j.cca.2007.01.026 (2007).
Park, C. Y., Lim, J. Y. & Park, H. Y. Age at natural menopause in Koreans: secular trends and influences thereon. Menopause 25 (4), 423–429. https://doi.org/10.1097/Gme.0000000000001019 (2018).
Lennie, T. A., Chung, M. L., Habash, D. L. & Moser, D. K. Dietary fat intake and Proinflammatory cytokine levels in patients with heart failure. J. Card Fail. 11 (8), 613–618. https://doi.org/10.1016/j.cardfail.2005.06.434 (2005).
Shahril, M. R. et al. Energy-Dense, High-SFA and Low-Fiber’ Dietary Pattern Lowered Adiponectin but Not Leptin Concentration of Breast Cancer Survivors. Nutrients 13 (10). https://doi.org/10.3390/nu13103339 (2021).
Murakami, K. et al. Total n-3 polyunsaturated fatty acid intake is inversely associated with serum C-reactive protein in young Japanese women. Nutr. Res. 28 (5), 309–314. https://doi.org/10.1016/j.nutres.2008.03.008 (2008).
Santos, S., Oliveira, A., Casal, S. & Lopes, C. Saturated fatty acids intake in relation to C-reactive protein, adiponectin, and leptin: A population-based study. Nutrition 29 (6), 892–897. https://doi.org/10.1016/j.nut.2013.01.009 (2013).
Li, K. L., Huang, T., Zheng, J. S., Wu, K. J. & Li, D. Effect of Marine-Derived n-3 polyunsaturated fatty acids on C-Reactive protein, Interleukin 6 and tumor necrosis factor Α: A Meta-Analysis. Plos One. 9 (2). https://doi.org/10.1371/journal.pone.0088103 (2014).
Alfano, C. M. et al. Fatigue, inflammation, and ω-3 and ω-6 fatty acid intake among breast Cancer survivors. J. Clin. Oncol. 30 (12), 1280–1287. https://doi.org/10.1200/Jco.2011.36.4109 (2012).
Yang, Z. H., Miyahara, H., Iwasaki, Y., Takeo, J. & Katayama, M. Dietary supplementation with long-chain monounsaturated fatty acids attenuates obesity-related metabolic dysfunction and increases expression of PPAR gamma in adipose tissue in type 2 diabetic KK-A mice. Nutr. Metab. 10. https://doi.org/10.1186/1743-7075-10-16 (2013).
Calder, P. C. n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am. J. Clin. Nutr. 83 (6), 1505s–19s. https://doi.org/10.1093/ajcn/83.6.1505S (2006).
Calder, P. C. et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. Brit J. Nutr. 106, S1–S78. https://doi.org/10.1017/S0007114511005460 (2011).
Calder, P. C. Polyunsaturated fatty acids and inflammation. Prostag Leukotr Ess. 75 (3), 197–202. https://doi.org/10.1016/j.plefa.2006.05.012 (2006).
Teng, K. T., Chang, C. Y., Chang, L. F. & Nesaretnam, K. Modulation of obesity-induced inflammation by dietary fats: mechanisms and clinical evidence. Nutr. J. 13, 12. https://doi.org/10.1186/1475-2891-13-12 (2014).
Wang, Y. T. et al. Dietary fatty acids and mortality risk from heart disease in US adults: an analysis based on NHANES. Sci. Rep. 13 (1). https://doi.org/10.1038/s41598-023-28738-2 (2023).
Mertens, E. et al. Geographic and socioeconomic diversity of food and nutrient intakes: a comparison of four European countries. Eur. J. Nutr. 58 (4), 1475–1493. https://doi.org/10.1007/s00394-018-1673-6 (2019).
Zheng, J. & Consortium, I. Association between plasma phospholipid saturated fatty acids and metabolic markers in eight European countries: a cross-sectional analysis in the EPIC-InterAct study. Diabetologia 60, S159–S60. https://doi.org/10.1186/s12916-017-0968-4 (2017).
Bohl, M., Bjornshave, A., Gregersen, S. & Hermansen, K. Whey and casein proteins and Medium-Chain saturated fatty acids from milk do not increase Low-Grade inflammation in abdominally obese adults. Rev. Diabet. Stud. 13 (2–3), 148–157. https://doi.org/10.1900/rds.2016.13.148 (2016).
Fayyaz, K. et al. Validity of measured vs. Self-Reported weight and height and practical considerations for enhancing reliability in clinical and epidemiological studies: A systematic review. Nutrients 16 (11). https://doi.org/10.3390/nu16111704 (2024).
Hodge, J. M., Shah, R., McCullough, M. L., Gapstur, S. M. & Patel, A. V. Validation of self-reported height and weight in a large, nationwide cohort of U.S. Adults. PLoS One 15 (4), e0231229. https://doi.org/10.1371/journal.pone.0231229 (2020).
Qin, B. et al. Validity of self-reported weight, height, and body mass index among African American breast cancer survivors. J. Cancer Surviv. 12 (4), 460–468. https://doi.org/10.1007/s11764-018-0685-9 (2018).
Mok, A., Khaw, K. T., Luben, R., Wareham, N. & Brage, S. Physical activity trajectories and mortality: population based cohort study. BMJ 365, l2323. https://doi.org/10.1136/bmj.l2323 (2019).
Pandey, A. et al. Performance of the American heart association/american college of cardiology pooled cohort equations to estimate atherosclerotic cardiovascular disease risk by Self-reported physical activity levels. JAMA Cardiol. 6 (6), 690–696. https://doi.org/10.1001/jamacardio.2021.0948 (2021).
Shin, W. K. et al. The association between physical activity and health-related quality of life among breast cancer survivors. Health Qual. Life Outcomes 15 (1), 132. https://doi.org/10.1186/s12955-017-0706-9 (2017).
Acknowledgements
We extend our gratitude to all the breast cancer survivors who participated in this study. Additionally, we would like to express our appreciation to the nurses and research staff who assisted in participant recruitment and data collection.
Funding
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea Government (Ministry of Science and ICT) (number 2019R1F1A1061017 and 2021R1F1A1062476).
Author information
Authors and Affiliations
Contributions
JEL designed the study and acquired funding; JK and JEL drafted the manuscript; JK and HJC analyzed the data; HJC, ZK, HJY, JC, JWM, YSK, and JEL acquired data. All authors reviewed, edited, and endorsed the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study received approval from the Institutional Review Board of Soon Chun Hyang University Bucheon Hospital (SCHBC 2014-12-004-001), Jeonbuk National University Hospital (CUH 2014-05-002-005 and CUH 2018-02-004-004), Keimyung University Dongsan Medical Center (DSMC 2015-03-026), Dankook University Hospital (DKUH 2016-07-001-002), and Chosun University Hospital (CHOSUN 2016-06-022-001 and CHOSUN 2018-06-004-001). All participants in the study submitted their informed consent forms.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kim, J., Cho, H.J., Kim, Z. et al. Intakes of saturated and unsaturated fat and circulating levels of inflammatory markers among breast cancer survivors. Sci Rep 15, 9481 (2025). https://doi.org/10.1038/s41598-025-92951-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-92951-4
