
Abstract
Research on how loneliness, as a subjective experience, affects suicide risk remains insufficient. It also remains unclear whether the effects vary according to family composition. This study aimed to investigate the associations among loneliness, suicidal ideation, and psychological distress in a rural population in Japan. A cross-sectional survey was conducted between August and September 2023 in a rural town in Akita Prefecture. Of the 5,000 surveyed residents, data from 1,842 respondents were analyzed. The exposure variable was loneliness, as assessed by the University of California Los Angeles Loneliness Scale short form. The main outcome was the presence or absence of suicidal ideation, which was measured using a self-reported questionnaire. The secondary outcome was psychological distress, which was measured using the Kessler Psychological Distress Scale (K6). The collected data were analyzed using multivariate logistic regression and stratified analysis based on family composition. Loneliness was strongly associated with suicidal ideation and psychological distress. The loneliness–psychological distress association persisted regardless of family composition. Loneliness independently affected suicidal ideation and psychological distress among rural residents in Japan. To develop effective suicide prevention strategies in rural areas, it is essential to address both social isolation and the subjective experience of loneliness.
Similar content being viewed by others
Introduction
Suicide is a serious global problem1. Numerous epidemiological studies have identified various risk factors for suicide, including a history of suicide attempts, family history of suicide, depression, social isolation, disasters, physical illness, and economic hardship2,3,4,5,6,7,8. Despite these advances, identifying clear causal pathways for suicide mechanisms remains a significant challenge. This has not prevented, nevertheless, several suicide prevention theoretical models and guidelines being proposed. Among these, the interpersonal theory of suicide, which explains that suicidal ideation arises when individuals simultaneously experience perceived burdensomeness and thwarted belongingness, has gained prominence in recent years9. Suicidal ideation occurs at an early stage of the progression of suicide attempts and completed suicides, is critical for such progression10,11, and reflects the emergence of psychological distress that can escalate if not intervened against. These characteristics render the construct an important indicator of suicide risk. Importantly, suicide results from the complex interplay of multiple factors12, making it such that prevention is key for effectively addressing both the personal and social factors related to suicide13.
Loneliness and social isolation are recognized as global problems and are associated with adverse mental health outcomes, such as depression14,15. They also heighten the risk of morbidity and mortality from chronic diseases16; therefore, they are regarded as critical targets for intervention in mental and public health. In recent years, loneliness and social isolation have also become pressing concerns in Japan. For example, from 2005 to 2020, the number of single-person households increased by six million (accounting for 40% of all households nationally)17, raising concerns about the potential decline in interactions among residents. This becomes even more paramount if we consider the concomitant phenomena in Japan of the shrinking population, falling birthrates, and aging society18. Since the enactment of the Basic Act on Suicide Countermeasures in 2006, the national government has implemented specific suicide prevention policies addressing social issues such as unemployment and economic hardships19. However, loneliness has often been overlooked as a critical factor in this context.
Japan has a higher suicide rate than other countries20, but the national suicide prevention efforts conducted over the past decade have gradually reduced suicide rates. Despite these attempts, suicide rates have recently increased among women and younger populations, indicating a demographic shift in suicidal tendencies at the national level21. One factor contributing to this shift in trends is that, beyond economic factors alone, reduced social interactions have exacerbated feelings of loneliness, leading to an increase in the number of suicides22. Additionally, a large Japanese study suggested loneliness as a significant factor contributing to the increased risk of suicide during the COVID-19 pandemic23.
Although often perceived as synonymous, loneliness and social isolation are distinct concepts. The first refers to a subjective sense of distress that occurs when social connections are perceived as inadequate/unfulfilling, whereas the latter is an objective indicator of estrangement in which social connections are limited or absent24,25,26. Therefore, the two concepts often conflate but do not always co-occur, in that isolated individuals may not feel lonely and those with abundant social connections can still experience loneliness27,28. Furthermore, although living alone has been suggested as a risk factor for suicide in previous studies29,30, there is data from a 2022 Japanese report showing that approximately two-thirds of suicide victims lived with others at the time of death (number of suicides among people not living alone, 14,266 vs. living alone, 7,414)31. In another study, individuals living only with their parents were found to have a higher risk of suicide32.
Previous research on suicide prevention in rural areas has often focused on older adults, who are particularly vulnerable to loss and social isolation33,34. The past literature has also reported on a link between living alone and depression among older adults35, but there is also importance in focusing on loneliness as a key factor in mental health and suicide prevention36. Based on previous studies, we hypothesize that loneliness has an independent influence on suicidal ideation and psychological distress, irrespective of family composition. This study aims to examine the association between loneliness, suicidal ideation, and psychological distress in Japanese rural residents. Rural towns in Japan face unique challenges that make them critical settings for studying loneliness and suicide prevention. These areas are characterized by significant population aging, which may be associated with increased loneliness and social isolation. Additionally, rural towns often have limited resources for mental health care and community support, emphasizing the need for practical and sustainable interventions suited to their specific circumstances. The results of this study have implications for the development of effective measures to address loneliness and social isolation, which may contribute to suicide prevention efforts in rural areas of Japan.
Materials and methods
Study design and data collection
Akita Prefecture is one of the most rapidly aging prefectures in Japan, with a higher proportion of older adult residents compared to other regions. It also had the highest suicide rate among Japan’s 47 prefectures over the past two decades17,37. The suicide mortality rate varies significantly among the 25 municipalities within Akita Prefecture, with rural areas generally exhibiting higher rates than urban areas. Nearly half of the suicide victims in Akita Prefecture, are aged 60 years or older, indicating that addressing older adult suicides is a key concern in these regions37. Suicide prevention measures designed to address the characteristics of rural areas, including aging populations and higher suicide rates, are considered essential for reducing the overall suicide mortality in Akita.
Akita has a history of implementing suicide prevention initiatives, with municipalities organizing mental health lectures and other community-based interventions38,39. Addressing factors such as social isolation and loneliness in rural areas is anticipated to contribute to lowering suicide rates across the prefecture.
This cross-sectional study was based on a mental health survey conducted between August and September 2023 among residents aged 20 to 84 years in a rural town in Akita Prefecture, northern Japan. The town had approximately 14,000 residents at the time of the survey. In Japan, all prefectures and municipalities are required to develop regional suicide prevention plans tailored to the local context. This survey was conducted to develop suicide countermeasures for rural populations based on Japan’s General Principles of Suicide Countermeasures Policy40. The prevalence of suicidal ideation in Akita Prefecture has been estimated to be approximately 3.7%37. To ascertain the prevalence of suicidal ideation with an accuracy of 3.7% and a 1% margin of error, the required sample size was 2028. Assuming a response rate of approximately 40%, the sample size was set to 5000. Using stratified random sampling based on sex and age distribution, 5000 residents aged 20 to 84 were selected from a population of approximately 14,000. Sampling was conducted using the basic resident register managed by the municipality. This register contains information about one’s date of birth, sex, and address.
This survey will serve as a baseline survey for formulating countermeasure plans, with a follow-up survey scheduled for 2025 to assess longitudinal trends. The purpose of the survey was explained in the town’s public newsletter to ensure the smooth distribution of the questionnaires. It was also announced that all personal information necessary for follow-up surveys would be managed by the local government. The extraction of participant addresses and the management of personal information were handled by public health nurses from the municipality, who also led the coordination and announcement process in the town’s public newsletter. We excluded individuals certified as support level 2 or higher under the Japanese Long-Term Care Insurance (LTCI) system, as these individuals had functional disabilities that could hinder independent survey completion.
Anonymous questionnaires were mailed to 5,000 residents between August and September 2023. Returning a completed questionnaire was considered a consent to participate in the study; an explanation of the research purpose was provided alongside the survey. Participants were also informed about a follow-up survey scheduled for 2025 and their right to withdraw consent. Those wishing to withdraw consent by December 2023 could do so by submitting a withdrawal letter or answering a Google Form. Individuals who withdrew consent were excluded from the analysis, and measures were taken to ensure they would not receive the follow-up survey.
The questionnaire included items on demographic characteristics, loneliness, suicidal ideation, and psychological distress. This study followed the STROBE guidelines for reporting observational studies41.
Measures
Sex was classified as male or female. Age was categorized into three groups: 20–39 years, 40–59 years, and ≥ 60 years. Family composition was defined as either living alone or living in a household with multiple occupants. Marital status was grouped into never married, married, separated, widowed, or missing. Subjective economic status was assessed on a five-point scale ranging from good to poor, or missing. Medical history was categorized into four groups: disease-free, having physical health conditions, having mental health conditions, multimorbidity (physical and mental health conditions), or missing.
Self-reported loneliness was the exposure variable. Loneliness was measured using the six-item University of California, Los Angeles (UCLA) Loneliness Scale (ver. 3), a loneliness scale developed by Russel42. We specifically used its six-item short form, which has been validated in Japanese by Toyoshima and Sato43. Items were responded to on a four-point scale, with total scores ranging from 0 to 24 and being calculated by summing the scores of all items. As there was no established cut-off point for this scale, we followed prior studies and distinguished the presence of loneliness based on the upper quartile of the distribution44. That is, a score in the third quartile or above (UCLA score ≥ 15) was defined as experiencing loneliness, and a binary variable was created to classify loneliness presence or absence.
The outcome variables were suicidal ideation and psychological distress, both of which were self-reported. Suicidal ideation was measured using the following question, “Did you think about committing suicide in the past month?” To which participants responded with “yes,” “no,” or “unsure,” with a “yes” answer representing that the respondent experienced suicidal ideation. Since suicidal ideation precedes suicide attempts or completion10,11, it can be regarded as a key predictor of suicide risk. This study used only this single-item to measure this construct in an attempt to simultaneously deal with the ethical concerns surrounding studies on suicide and to promote ease of response for participants. We aimed to minimize the number of questions on suicide while focusing on identifying “suicidal ideation,” which is considered essential for implementing effective interventions. The item used in this survey was adapted from the Ministry of Health, Labour and Welfare’s 2021 Survey on Attitudes Toward Suicide Countermeasures45.
Psychological distress was measured using the Kessler Psychological Distress Scale (K6), a six-item questionnaire that evaluates mood and anxiety experienced in the last 30 days46. The total K6 scores ranged from 0 to 24. We used the Japanese version of the K647, adopting a cut-off value of K6 ≥ 13 to indicate a state of psychological distress47,48. In Japan, the K6 is frequently used as a screening tool for depression49 and was designated as a secondary outcome of this study.
Social isolation was used as a covariate and measured based on responses to two questions, as follows: “How often do you go out, excluding visits to attend a hospital or shopping?” and “Do you have conversations with family or acquaintances?” Respondents who answered “less than once a week” to the first question and “rarely” to the second were identified as socially isolated. In Japan, going out less than once a week is commonly used as a general definition of being homebound. This item was established with reference to the definition of homebound individuals in Japan50 and a previous study23.
Ethical considerations
This study was approved by the Research Ethics Committee of Akita University (approval number: 3008, date: August 14, 2023) and followed the international ethical standards established in the Declaration of Helsinki. All participants were provided with information about consenting to participate in the study. Residents were informed through documents that participation was voluntary and that there would be no disadvantages for not participating. They were also informed that they could withdraw their consent to participate until December 2023 by submitting a withdrawal form, either in writing or through a Google Form, before the commencement of the analysis.
Statistical analysis
To examine the association of suicidal ideation and psychological distress with loneliness, we conducted a multivariate logistic regression analysis, estimating odds ratios (ORs) and 95% confidence intervals (CIs). The reference group for all models was the loneliness absent group (OR = 1.00), and the following three models were employed: Model 1 was the crude model; Model 2 adjusted for age, sex, marital status, subjective economic status, family composition, and medical history; Model 3 adjusted for all variables in Model 2 along with social isolation. Stratified analyses were conducted to investigate whether family composition (living alone or in a household with multiple occupants) influenced the associations between loneliness, suicidal ideation, and psychological distress. These analyses were stratified by family composition and adjusted for age, sex, subjective economic status, and medical history. All statistical analyses were performed using STATA version 18 (StataCorp LLC, College Station, TX, USA), and two-tailed tests were used to determine significance at the 5% level.
Results
We received 2,213 responses (response rate of 44.3%). Of these, 21 individuals with missing data on age (n = 5) or sex (n = 16) were excluded, leaving 2,192 participants. Among the study participants, 928 were male (42.3%) and 1,264 were female (57.7%). For males, 19.5% were aged 20–39 years in the initial allocation and 18.1% among study participants. Those aged 40–59 years accounted for 31.6% and 31.8%, respectively, while those aged 60 years or older accounted for 48.9% and 50.1%. For females, 17.0% were aged 20–39 years in the initial allocation and 18.5% among study participants. Those aged 40–59 years accounted for 29.6% and 27.1%, while those aged 60 years or older accounted for 53.4% and 54.4%. Among the participants, those with missing data on suicidal ideation (n = 109), K6 scores (n = 149), loneliness (n = 82), or family composition (n = 10) were excluded. Finally, the responses of 1,842 individuals were included in the analysis.
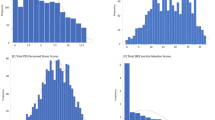
Table 1 shows participants’ demographic characteristics. Among the 1,842 respondents, 188 (10.2%) reported a K6 score of 13 or higher and 41 (2.2%) reported suicidal ideation. The number of participants experiencing loneliness was 541 (29.4%). The prevalence of loneliness was higher among men, but was similar among age groups, family compositions, marital status, history of physical illness, and social isolation. Meanwhile, individuals with a history of psychiatric illness, poor subjective economic condition, psychological distress (K6 ≥ 13), and suicidal ideation in the past month showed a higher prevalence of loneliness.
Table 2 shows the results of the associations between loneliness, suicidal ideation, and psychological distress. In Model 1, the presence of loneliness was significantly positively associated with suicidal ideation (OR = 12.39, 95% CI = 5.46–28.14, p < 0.001) and psychological distress (OR = 13.73, 95% CI = 9.38–20.09, p < 0.001). These significant positive associations remained so in Model 2 adjusted for all confounding factors (suicidal ideation: OR = 10.56, 95% CI = 4.31–25.86, p < 0.001; psychological distress: OR = 11.97, 95% CI = 8.05–17.80, p < 0.001) and Model 3 additionally adjusted for social isolation (suicidal ideation: OR = 10.91, 95% CI = 4.45–26.79, p < 0.001; psychological distress: OR = 11.69, 95% CI = 7.84–17.42, p < 0.001).
Table 3 presents the results of the stratified analysis. Due to an absence of cases of suicidal ideation among individuals living alone, it was not possible to calculate an odds ratio (OR) for the association between loneliness and suicidal ideation in this group. However, when examining psychological distress, among individuals who were lonely both those living alone (OR = 8.28, 95% CI = 1.13–61.31, p < 0.05) and in multi-person households (OR = 11.64, 95% CI = 7.81–17.34, p < 0.001) had significantly higher odds of psychological distress compared to the reference group, which encompassed those with absence of loneliness.
Discussion
Our results revealed that loneliness is strongly associated with suicidal ideation and psychological distress among rural residents in Japan. Consistent with previous studies23,29,51, loneliness was identified as a major risk factor, underscoring the need for support to those experiencing this phenomenon. Even when social isolation was included as a covariate in the analysis, the association between loneliness and psychological distress remained strong, reaffirming that loneliness is an independent risk factor affecting psychological health and its importance in suicide prevention efforts.
The stratified analysis showed that loneliness was strongly associated with psychological distress regardless of family composition. While some studies have highlighted the risk of suicide in individuals living alone29,30, our findings indicate that loneliness is a significant risk factor both for those living alone and those living with others in the same household. What follows is that importance should be given to indicators other than objective ones (e.g., family composition) when considering measures to address loneliness. Corroborating this assertion, extant research describes the need to consider individual coping strategies52 and the buffering model of social support53 when addressing stressors such as loneliness. Future studies should examine the effectiveness of interventions that enhance adaptive coping strategies and social support mechanisms to reduce loneliness in the general population.
It is also of importance that loneliness is influenced by cultural and social contexts, and this relationship requires careful consideration. For example, an Organisation for Economic Co-operation and Development survey indicated that loneliness in Japan often stems from a lack of emotional support, such as the absence of close friends54. In contrast, in countries like Turkey and the United States of America, existential loneliness (i.e., a feeling of fundamental separateness from others and the wider world) has been suggested as a significant factor contributing to loneliness. These cultural differences suggest that interventions to alleviate loneliness must be tailored to societal norms and expectations in a country55. Another study highlighted loneliness’s multifaceted and complex nature, emphasizing the need for interventions informed by a nuanced understanding of its components56. A problem here is that while structural factors such as family composition and living arrangements contribute to social isolation, they are difficult to address through external interventions, which creates a significant barrier to the implementation of effective measures. Despite these potential challenges, loneliness is a subjective and modifiable experience, making it an important focus for potential interventions.
In 2024, the Act on Promotion of a Policy for Loneliness and Isolation came into effect in Japan, emphasizing the need for comprehensive strategies to tackle these issues nationwide57. Local governments are tasked with developing specific measures to alleviate loneliness and reduce social isolation. Recently, internationally recognized interventions, such as Social Prescribing (SP), have garnered attention for their focus on addressing social determinants of health58,59, These approaches may hold particular promise in Japan, where rural areas face significant challenges related to population decline and social isolation. While introducing innovative approaches like SP is important, strengthening existing human resources is equally crucial. Implementing practical and sustainable programs is essential in rural areas, where financial and human resources are often limited. For instance, providing additional training for public health nurses, gatekeepers, and other professionals could enhance their capacity to recognize and address feelings of loneliness more effectively. Such training could enable them to intervene early and offer targeted support to those in need. Moreover, fostering collaborations with non-profit organizations (NPOs) that address loneliness and social isolation could play a vital role in strengthening local support systems. In rural and mountainous areas, where community cohesion and traditional support networks may still play a significant role, building on these existing strengths through such collaborations could enhance the effectiveness of future interventions.
To build on these strategies, further research is needed to refine our understanding of the complex relationships between loneliness, suicidal ideation, and psychological distress. Longitudinal studies can help identify causal pathways and inform the development of interventions that are both evidence-based and designed to address the specific needs of rural populations. Additionally, evaluating the effectiveness of context-specific interventions in various communities will be crucial for enhancing suicide prevention efforts and reducing psychological distress in these areas.
Limitations
This study had several limitations. First, because this was a cross-sectional study, causal associations could not be directly assessed. Second, the study was limited to one rural area, and thus we suggest caution when generalizing the results to other regions. Third, the sample size was small, as the prevalence of suicidal ideation in the past month was only 41 (2.3%) and the number of participants living alone was only 115 (6.2%) in a total sample of 1,842 valid participants. This may have resulted in wide confidence intervals and potentially imprecise estimates of the associations. This underrepresentation of single-person households (i.e., only 6.2% of the sample) also applies if we consider information at the municipal level, as the municipality’s demographic statistics show that these households accounted for 17.8% of the municipality in 202060. This discrepancy may limit the generalizability of our findings regarding loneliness and its association with suicidal ideation and psychological distress in this population. Future studies should consider larger sample sizes to allow for more reliable stratified analyses and more precise estimates of these associations. Fourth, the question used to assess suicidal ideation was adapted from a national survey on suicide prevention. While this direct phrasing was intended to facilitate intervention planning, it may have led to underreporting or non-response due to the topic’s sensitive nature. Future research should consider exploring alternative phrasing or designing more suitable items to capture this sensitive information better while minimizing bias and non-response. Finally, the measure used to assess loneliness (i.e., using a six-item self-administered questionnaire) may have fallen short of holistically capturing the nuances of this complex concept. Moreover, as the data were self-reported and included sensitive topics such as suicidal ideation, socially desirable responding may have influenced the results.
Conclusions
This study revealed that loneliness is strongly associated with suicidal ideation and psychological distress among rural residents in Japan. The strong association of loneliness with psychological stress persisted even after considering social isolation and living arrangements, suggesting that loneliness is an independent risk factor for psychological health deterioration. To develop effective suicide prevention strategies in rural areas of Japan, it is essential to address both social isolation (i.e., as an objective indicator) and the subjective experiences of loneliness.
Data availability
The data that support the findings of this study are available on request from the first author, [AI] or corresponding author, [FT].
References
World Health Organization. Suicide worldwide in 2019: Global health Estimates. (2021). https://iris.who.int/bitstream/handle/10665/341728/9789240026643-eng.pdf?sequence=1
Aihara, H. & Iki, M. An ecological study of the relations between the recent high suicide rates and economic and demographic factors in Japan. J. Epidemiol. 13, 56–61. https://doi.org/10.2188/jea.13.56 (2003).
Fujioka, K., Abe, S. & Hiraiwa, K. Lifetime social, psychological and physical background of suicides-research on the number of suicides during a year in Fukushima Prefecture (Article in Japanese). Seishin Shinkeigaku Zasshi. 106, 17–31 (2004).
Nugent, A. C., Ballard, E. D., Park, L. T. & Zarate, C. A. Research on the pathophysiology, treatment, and prevention of suicide: practical and ethical issues. BMC Psychiatry. 19, 332. https://doi.org/10.1186/s12888-019-2301-6 (2019).
Kavalidou, K., Smith, D. J. & O’Connor, R. C. The role of physical and mental health Multimorbidity in suicidal ideation. J. Affect. Disord. 209, 80–85. https://doi.org/10.1016/j.jad.2016.11.026 (2017).
Tanji, F. et al. Personality and suicide risk: the impact of economic crisis in Japan. Psychol. Med. 45, 559–573. https://doi.org/10.1017/S0033291714001688 (2015).
Orui, M., Harada, S. & Hayashi, M. Changes in suicide rates in disaster-stricken areas following the great East Japan earthquake and their effect on economic factors: an ecological study. Environ. Health Prev. Med. 19, 459–466. https://doi.org/10.1007/s12199-014-0418-2 (2014).
Nakagawa, M. et al. Characteristics of suicide attempters with family history of suicide attempt: a retrospective chart review. BMC Psychiatry. 59, 32; (2009). https://doi.org/10.1186/1471-244X-9-32
Joiner, T. E. Why People Die by Suicide (Harvard University Press, 2005).
Van Orden, K. A. et al. Jr. The interpersonal theory of suicide. Psychol. Rev. 117, 575–600. https://doi.org/10.1037/a0018697 (2010).
Beck, A. T., Brown, G. K., Steer, R. A., Dahlsgaard, K. K. & Grisham, J. R. Suicide ideation at its worst point: a predictor of eventual suicide in psychiatric outpatients. Suicide Life Threat. Behav. 29, 1–9; (1999). https://doi.org/10.1111/j.1943-278X.tb00758 (1999).
World Health Organization. Preventing suicide A global imperatives. (2014). https://iris.who.int/bitstream/handle/10665/131056/9789241564779_eng.pdf?sequence=1
Yoshimasu, K., Kiyohara, C. & Miyashita, K., & stress research group of the Japanese society for hygiene. Suicidal risk factors and completed suicide: meta-analyses based on psychological autopsy studies. Environ. Health Prev. Med. 13, 243–256. https://doi.org/10.1007/s12199-008-0037-x (2008).
Heinrich, L. M. & Gullone, E. The clinical significance of loneliness: a literature review. Clin. Psychol. Rev. 26, 695–718. https://doi.org/10.1016/j.cpr.2006.04.002 (2006).
Motillon-Toudic, C. et al. Social isolation and suicide risk: literature review and perspectives. Eur. Psychiatry. 65, e65. https://doi.org/10.1192/j.eurpsy.2022.2320 (2022).
Friedler, B., Crapser, J. & McCullough, L. One is the deadliest number: the detrimental effects of social isolation on cerebrovascular diseases and cognition. Acta Neuropathol. 129, 493–509. https://doi.org/10.1007/s00401-014-1377-9 (2015).
Statistics Bureau of Japan. Population Census. Ministry of Internal Affairs and Communications. (2021). https://www.stat.go.jp/data/kokusei/2020/kekka/pdf/outline_01.pdf
Iijima, K. et al. Toward the development of a vibrant, super-aged society: the future of medicine and society in Japan. Geriatr. Gerontol. Int. 8, 601–613. https://doi.org/10.1111/ggi.14201 (2021).
Kaga, M., Takeshima, T. & Matsumoto, T. Suicide and its prevention in Japan. Leg. Med. (Tokyo). 11, 18–21. https://doi.org/10.1016/j.legalmed.2009.01.015 (2009).
OECD. Suicide rates Total, Deaths per 100 000 inhabitants. (2020). https://www.oecd.org/en/data/indicators/suicide-rates.html
Ministry of Health, Labor, and Welfare (MHLW). Suicide Statistics in Japan in 2022. (2023). https://www.mhlw.go.jp/content/R4kakutei01.pdf
Horita, N. & Moriguchi, S. COVID-19, young people, and suicidal behaviour. Lancet Psychiatry. 10, 484–485. https://doi.org/10.1016/S2215-0366(23)00159-1 (2023).
Tachikawa, H. et al. Impact of loneliness on suicidal ideation during the COVID-19 pandemic: findings from a cross-sectional online survey in Japan. BMJ Open. 13, e063363. https://doi.org/10.1136/bmjopen-2022-063363 (2023).
De Gierveld, J. Personal relationships, social support, and loneliness. J. Soc. Pers. Relat. 6, 197–221. https://doi.org/10.1177/026540758900600204 (1989).
De Jong Gierveld, J. & Havens, B. Cross-national comparisons of social isolation and loneliness: introduction and overview. Can. J. Aging. 23, 109–113. https://doi.org/10.1353/cja.2004.0021 (2004).
Tomaka, J., Thompson, S. & Palacios, R. The relation of social isolation, loneliness, and social support to disease outcomes among the elderly. J. Aging Health. 18, 359–384. https://doi.org/10.1177/0898264305280993 (2006).
Hawkley, L. C. & Cacioppo, J. T. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 40, 218–227. https://doi.org/10.1007/s12160-010-9210-8 (2010).
Golden, J. et al. Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. Int. J. Geriatr. Psychiatry. 24, 694–700. https://doi.org/10.1002/gps.2181 (2009).
Shaw, R. J. et al. Living alone, loneliness and lack of emotional support as predictors of suicide and self-harm: a nine-year follow up of the UK biobank cohort. J. Affect. Disord. 279, 316–323. https://doi.org/10.1016/j.jad.2020.10.026 (2021).
Olfson, M., Cosgrove, C. M., Altekruse, S. F., Wall, M. M. & Blanco, C. Living alone and suicide risk in the united States, 2008–2019. Am. J. Public. Health. 112, 1774–1782. https://doi.org/10.2105/AJPH.2022.307080 (2022).
Ministry of Health, Labor, and Welfare (MHLW). Suicide statistics. (2024). https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsu_year.html
Poudel-Tandukar, K. et al. Differences in suicide risk according to living arrangements in Japanese men and women–the Japan public health Center-based (JPHC) prospective study. J. Affect. Disord. 131, 113–119 (2011).
Kaneko, Y., Motohashi, Y., Sasaki, H. & Yamaji, M. Prevalence of depressive symptoms and related risk factors for depressive symptoms among elderly persons living in a rural Japanese community: a cross-sectional study. Community Ment Health J. 43, 583–590. https://doi.org/10.1007/s10597-007-9096-5 (2007).
Niu, L. et al. Loneliness, hopelessness and suicide in later life: a case-control psychological autopsy study in rural China. Epidemiol. Psychiatr Sci. 29, e119. https://doi.org/10.1017/S2045796020000335 (2020).
Fukunaga, R. et al. Living alone is associated with depression among the elderly in a rural community in Japan. Psychogeriatrics 12, 179–185. https://doi.org/10.1111/j.1479-8301.2012.00402.x (2012).
Antonelli-Salgado, T. et al. Loneliness, but not social distancing, is associated with the incidence of suicidal ideation during the COVID-19 outbreak: a longitudinal study. J. Affect. Disord. 290, 52–60. https://doi.org/10.1016/j.jad.2021.04.044 (2021).
Akita Prefecture. [Suicide Countermeasures Policy in Akita Prefecture] Dai 2 ki akitaken zisatsutaisakukeikaku (in Japanese). (2023). https://www.pref.akita.lg.jp/uploads/public/archive_0000032769_00/%E3%80%90%E6%9C%80%E7%B5%82%E7%89%88%E3%80%91%E7%A7%8B%E7%94%B0%E7%9C%8C%E8%87%AA%E6%AE%BA%E5%AF%BE%E7%AD%96%E8%A8%88%E7%94%BB.pdf
Motohashi, K., Kaneko, Y., Fujita, K., Motohashi, Y. & Nakamura, A. Interest in dietary pattern, social capital, and psychological distress: a cross-sectional study in a rural Japanese community. BMC Public. Health. 13, 933. https://doi.org/10.1186/1471-2458-13-933 (2013).
Nakao, M., Takeuchi, T. & Yoshimasu, K. A proposed approach to suicide prevention in Japan: the use of self-perceived symptoms as indicators of depression and suicidal ideation. Environ. Health Prev. Med. 13, 313–321. https://doi.org/10.1007/s12199-008-0048-7 (2008).
The Ministry of. Health, Labour, and Welfare. The General Principles of Suicide Countermeasures Policy. (2022). https://www.mhlw.go.jp/content/001250885.pdf
Von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370, 1453–1457. https://doi.org/10.1016/S0140-6736(07)61602-X (2007).
Russell, D., Peplau, L. A. & Ferguson, M. L. Developing a measure of loneliness. J. Pers. Assess. 42, 290–294. https://doi.org/10.1207/s15327752jpa4203_11 (1978).
Toyoshima, A. & Sato, S. Development of a short form of the UCLA loneliness scale (Version 3) for multiple age groups. Rounenshinrigakukenkyu 2, 19–26. https://doi.org/10.50944/jjcgp.2.0_19 (2021). (Article in Japanese).
Victor, C. R. & Pikhartova, J. Lonely places or lonely people? Investigating the relationship between loneliness and place of residence. BMC Public. Health. 27, 20, (778). https://doi.org/10.1186/s12889-020-08703-8 (2020).
The Ministry of Health, Labour. and Welfare. Survey on Attitudes towards Suicide Countermeasures. (2021). https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/r3_ishikichousa.html
Kessler, R. C. et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry. 60, 184. https://doi.org/10.1001/archpsyc.60.2.184 (2003).
Furukawa, T. A. et al. The performance of the Japanese version of the K6 and K10 in the world mental health survey Japan. Int. J. Methods Psychiatr Res. 17, 152–158. https://doi.org/10.1002/mpr.257 (2008).
Tanji, F., Tomata, Y., Zhang, S., Otsuka, T. & Tsuji, I. Psychological distress and completed suicide in Japan: A comparison of the impact of moderate and severe psychological distress. Prev. Med. 116, 99–103. https://doi.org/10.1016/j.ypmed.2018.09.007 (2018).
Sakurai, K., Nishi, A., Kondo, K., Yanagida, K. & Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 65, 434–441. https://doi.org/10.1111/j.1440-1819.2011.02236.x (2011).
Ministry of Health, Labor, and Welfare (MHLW). Manual for Support of Homebound Elderly in 2009. (2009). https://www.mhlw.go.jp/topics/2009/05/dl/tp0501-1g.pdf
Lim, M. H., Rodebaugh, T. L., Zyphur, M. J. & Gleeson, J. F. Loneliness over time: the crucial role of social anxiety. J. Abnorm. Psychol. 125, 620–630. https://doi.org/10.1037/abn0000162 (2016).
Folkman, S., Lazarus, R. S., Dunkel-Schetter, C., DeLongis, A. & Gruen, R. J. Dynamics of a stressful encounter: cognitive appraisal, coping, and encounter outcomes. J. Pers. Soc. Psychol. 50, 992–1003. https://doi.org/10.1037/0022-3514.50.5.992 (1986).
Cohen, S. & Wills, T. A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 98, 310–357. https://doi.org/10.1037/0033-2909.98.2.310 (1985).
OECD. Measuring social connectedness in OECD countries –a scoping review. (2024). https://www.oecd.org/content/dam/oecd/en/publications/reports/2024/09/measuring-social-connectedness-in-oecd-countries_02a04f4b/f758bd20-en.pdf
Hawkley, L., Browne, M. & Cacioppo, J. How can I connect with thee? Let me count the ways. Psychol. Sci. 16, 798–804. https://doi.org/10.1111/J.1467-9280.2005.01617.X (2005).
Cacioppo, J. & Cacioppo, S. The phenotype of loneliness. Eur. J. Dev. Psychol. 9, 446–452. https://doi.org/10.1080/17405629.2012.690510 (2012).
CABINET SECRETARIAT. Act on Promotion of Policy for Loneliness and Isolation. (2024). https://www.cao.go.jp/kodoku_koritsu/torikumi/pdf/law.pdf
Pescheny, J. V., Randhawa, G. & Pappas, Y. The impact of social prescribing services on service users: a systematic review of the evidence. Eur. J. Public. Health. 30, 664–673. https://doi.org/10.1093/eurpub/ckz078 (2019).
Araki, K., Takahashi, Y., Okada, H. & Nakayama, T. Social prescribing from the patient’s perspective: A literature review. J. Gen. Fam Med. 23, 299–309. https://doi.org/10.1002/jgf2.551 (2022).
Statistics Bureau, Ministry of Internal Affairs and Communications. The 2020 Population Census POPULATION AND HOUSEHOLDS OF JAPAN. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200521&tstat=000001136464&cycle=0&year=20200&month=24101210&tclass1=000001136466 (2021).
Acknowledgements
The authors deeply appreciate all participants and the municipal staff who supported the survey. We would like to thank Editage (www.editage.jp) for English language editing.
Funding
This study supported by JSPS KAKENHI Grant Number JP23K10383. These funding agencies had no role in collection, analysis, and interpretation of data, or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
A.I. and F.T. designed the study. A.I. and F.T. conducted the statistical analysis. S.M. coordinated the field research. K.N. contributed to the design of the survey instrument. A.I. wrote the first draft of the manuscript. All authors contributed to editing the manuscript and commenting on the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Iwasawa, A., Tanji, F., Miyamoto, S. et al. The association between loneliness, suicidal ideation, and psychological distress considering family compositions: a cross-sectional study in a Japanese rural area. Sci Rep 15, 11676 (2025). https://doi.org/10.1038/s41598-025-96205-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96205-1
Keywords
This article is cited by
-
Loneliness, Mental Health, and Suicidality in Japan, and the Protective Role of Mattering: A National Panel Survey
International Journal of Mental Health and Addiction (2025)
