
Abstract
It is well known that one of the main causes of mortality and reduced life expectancy is air pollution, which carries the highest burden of diseases attributed to environmental factors. The poor air quality in Iranian cities leads to a wide range of acute and chronic health effects. This study estimates the natural deaths, ALRI, COPD, lung cancer, IHD, and strokes caused by air pollutants in Bukan, a southern city in West Azerbaijan Province, from 2011 to 2019. Population data was obtained from government organizations, and pollutant data for 2011–2019 was collected from the Bukan Environmental Protection Organization. Analyses were performed using Excel, and the data was subsequently entered into the WHO’s AirQ+ model to extract the results. The study found that long-term exposure to PM10, PM2.5, NO2, and O3 resulted in an estimated 316, 241, 14, and 52 deaths, respectively. By comparing the air quality over the 8-year period, it was determined that the air quality in Bukan city is not in good condition, with particulate matter levels exceeding relevant standards. Given the increasing trend of air pollution and associated health impacts, it is essential to implement effective control policies to improve the city’s air quality. This information provides a crucial step for city managers, policymakers, and health officials to mitigate the health effects caused by air pollution.
Similar content being viewed by others
Introduction
Extensive epidemiological research indicates that non communicable chronic illnesses accounted for almost two-thirds of deaths worldwide in 2020, and that percentage is predicted to increase to 77% by 2030. Air pollution is now estimated to be as significant as any other major global health hazard, growing the burden of non-communicable diseases worldwide1. Approximately 20% of all air pollution-related fatalities globally take place in wealthy countries in Europe, and North America, while more than 50% of these deaths are caused by exposure to air pollution in China and South Asia2. In 2013, outdoor air pollution was categorized as a Group 1 human carcinogen by the International Agency for Research on Cancer (IARC). Hazardous and carcinogenic substances are present in air pollution, with particulate matter less than 2.5 microns (PM2.5) being the most critical among the six primary pollutants that cause health effects3,4. The respiratory tract is where the majority of these contaminants enter the body, and epidemiological studies have confirmed both short-term and long-term consequences of these particles on human health. A meta-analysis conducted in 2020 by Orellano et al.5 discovered a positive correlation between mortality from all causes and exposure to PM2.5, PM10, O3, and NO2. An yearly total of more than one million premature deaths are linked to exposure to PM2.5, with these deaths disproportionately concentrated in urban areas. Between 2000 and 2019, global mortality from exposure to PM2.5 has steadily increased. This pattern is especially noticeable in parts of Africa and South and East Asia6. According to estimates, approximately 29% of lung cancer deaths, 24% of deaths from stroke, 25% of deaths from ischemic heart disease (IHD), and 43% of deaths from chronic obstructive pulmonary disease (COPD) occur globally as a result of air pollution7. Environmental pollution also impacts national economies. The anticipated yearly environmental costs of human activity exceeded USD 6.6 trillion in 2008. By 2050, it is estimated that human activities will cost the environment USD 28.6 trillion8. It is projected that the annual welfare losses caused by air pollution exceed 5 trillion USD in worldwide economic harm9. Iran’s air pollution is projected to cost the economy $13 billion, or 2.2% of the gross domestic product of the country (GDP)10. The adverse health impacts of air pollution have been the subject of several studies. Therefore, health impact assessments from air pollution must be conducted using precise and efficient tools to aid in planning for the world, a city, or a nation. Quantifying the health burden of air pollution is essential, and these assessments are currently conducted using AirQ+, released by WHO11,12. Several computer-based tools facilitate air pollution health impact assessments, with AirQ+ and BenMAP-CE (U.S. EPA) being the most widely used. AirQ+ is particularly popular due to its simple and intuitive user interface, making it accessible for users who may not have advanced technical expertise. This ease of use is a key advantage over other more complex modeling tools. The software maintains consistency in its core functionality and algorithms across versions, ensuring that assessments remain comparable over time. This feature makes it a reliable tool for long-term studies and consistent monitoring. AirQ+ can utilize a wide range of data, including air quality data at different spatial scales and epidemiological study data, such as time-series and cohort studies, to estimate health impacts. This flexibility in handling diverse datasets is an advantage over some other tools that may have stricter data requirements. By processing data through Excel and estimating relative risks, AirQ+ provides detailed outputs in terms of diseases and mortality, making the results easy to interpret and use for policy decisions. AirQ+ is widely adopted globally, has a high level of credibility, and supports precise data processing, which makes it a rational and effective choice for evaluating the health impacts of air pollution13,14,15,16,17. Iran is an arid country that has experienced severe drought, soil erosion, excessive exploitation of water resources, and the drying up of rivers over the past 2 decades, leading to an increase in dust storms. Lake Urmia, the largest saltwater lake in the Middle East and one of the world’s largest saline lakes, is located in northwestern Iran, between Tabriz and Urmia in West Azerbaijan Province. Bukan, a city in the south of Lake Urmia in West Azerbaijan Province, lies in a mountainous region with a moderate climate. It is the third most populous county in the province and holds geographical and climatic significance. Bukan was chosen due to its unique environmental challenges, including its proximity to Lake Urmia (which has been severely affected by drought) and its exposure to dust and salt storms. Unlike major Iranian cities such as Tehran or Isfahan, which also experience air pollution but primarily from industrial and vehicular sources, Bukan faces pollution exacerbated by both natural and anthropogenic factors, including dust storms from Iraq and environmental degradation around Lake Urmia. Additionally, Bukan’s mountainous and semi-arid climate influences pollution dispersion and accumulation, potentially worsening its air quality issues. Comparing Bukan’s pollution levels and health impacts with other similar cities in Iran or the Middle East would also provide a more comprehensive understanding of the issue18,19,20. Bukan represents a unique case study where air quality is influenced by both natural factors (dust storms, drought, and soil erosion) and human activities. Studying Bukan allows us to analyze the health impacts of pollution in a region where climatic and environmental conditions play a dominant role, a perspective that is often overlooked in studies focusing solely on urban industrial pollution. So, this research aims to assess the trends in the concentrations of pollutants (PM10, PM2.5, O3, and NO2) in Bukan’s air and calculate the consequences on health (including total natural mortality, acute lower respiratory infection (ALRI), COPD, lung cancer, IHD, and stroke) in the air of Bukan city using the WHO-recommended AirQ+ software from 2011 to 2019.
Method
Characteristics of the study area
The Bukan city is a subdivision of West Azerbaijan province, located approximately 200 km from the provincial capital, Urmia. Bukan is situated at geographical coordinates of 45° 41′ to 46° 32′ northern latitude and 36° 12′ to 36° 52′ eastern longitude. Additionally, the total area of Bukan County is approximately 2511 square kilometers, of which 30.31% is mountainous, 29.73% is hilly, and 39.96% is plains and flood-prone. It is at an average elevation of 1370 m above sea level. Figure 1 depicts the study site’s position.

Geographical location of the study area using ArcGIS 10.8 software.
Data collection
Air pollution data
To estimate the mortality rates from COPD, ALRI, lung cancer, stroke, IHD, and overall natural mortality caused by the exposure of Bukan residents to air pollutants between 2011 and 2019, we acquired hourly PM2.5, PM10, O3, and NO2 data from the Bukan Environmental Protection Agency. For the validation of each station, the following should be checked: The dataset should first have any values that are zero or negative deleted. Secondly, stations ought to be regarded valid only if they have access to over 75% of their hourly concentrations21. The data obtained from the Environmental Protection Agency for the years 2011–2019 were processed using Excel software, and finally, the 24-h average concentration from air pollutant measurement stations was used to quantify health effects using AirQ+ software.
Population data
The Statistics Center and Civil Registration Office in Iran record data related to the population and age groups. Following this, the Ministry of Health of Iran, as part of the healthcare system, provides a mortality profile report. Considering the demographic and epidemiological changes in countries and the increasing prevalence of non-communicable diseases, along with the need for planning and implementing effective interventions, one of the crucial informational needs for comprehensive management of these interventions is mortality data, highlighting the importance of accessing high-quality mortality data derived from continuous registration systems. The Iranian Statistics Centre provided the annual population and age groups of Bukan from 2011 to 2019 based on the provided data. Iran’s Civil Registration Office provided mortality cases divided down by age and group. Using the information gathered, the rates of death and the population at risk for ALRI, COPD, IHD, lung cancer, and stroke were finally computed.
AirQ+ software
The proportion of specific health outcomes that can be directly attributed to exposure to air pollution was calculated using the AirQ+ model from the WHO Regional Office for Europe. The software quantifies health effects for pollutants such as PM2.5, PM10, O3, and NO2. A user friendly-model for evaluating both the short- and long-term impacts of exposure to outdoor air pollution is included in AirQ+. Results can include a range of health outcomes relating to morbidity and death in both acute and chronic illnesses. Data on air pollution, population, baseline incidence, pollutant concentration, and relative risk are required inputs for estimating health consequences. AirQ+ bases all of its computations on techniques and concentration–response functions created by epidemiological research22,23.
AirQ+ software simulates the health effects of air pollution using epidemiological data, including Relative Risk (RR), Attributed Proportion (AP), and Baseline Incidence (BI). AP quantifies the fraction of health outcomes attributable to air pollution and is calculated based on RR values and exposure fractions. (Eq. 1)
Where RR, which is derived from concentration–response functions and epidemiological studies, is the relative risk of the health result for a specific health endpoint. P represents the population’s exposure to the air pollution as a proportion. The Impact of Exposure (IE) is calculated to determine the rate of health outcomes attributable to air pollutants exposure. (Eq. 2)
The number of cases linked to exposure (NE) is computed using Eq. (3)4:
Where BI and N are the baseline incidence of the specific health endpoint and the size of the population, respectively. The values of RR and BI were obtained in accordance with numerous conducted research and utilizing the default AirQ+ software24,25.
Results and discussion
Air pollutant concentrations
According to the study objectives, the results of this research are divided into two parts: (1) the trend of changes in the concentration of the studied pollutants; and (2) the mortality burden of each pollutant on the residents of the studied city. First, the results obtained from air data (the studied pollutants) are presented. The trend of variations in the amounts of air pollutants in the city of Bukan from 2011 to 2019 was examined using R software. The data obtained from the Bukan Environmental Protection Organization included 4239 data points (hourly concentrations) for every pollutant per year. Given that this study was conducted over an 8-year period.
The data screening was conducted following the AirQ+ software guide, which included stations with at least 75% valid data. Daily or 24 h averages for the pollutants of interest were calculated. From April to September, 31 daily concentrations were recorded each month (186 concentrations), while from October to March, 30 daily concentrations were recorded (180 concentrations). In total, 365 concentrations were obtained in 2011, and over the eight-year study period, 2920 concentrations were collected for each pollutant. Box plot charts for each pollutant were created using R software.
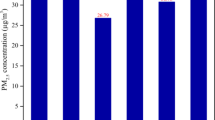
Figures 2 and 3 illustrate the changes in air pollutant concentrations from 2011 to 2019 at selected air quality monitoring stations in Bukan. The average concentrations of the pollutants PM2.5, PM10, O3, and NO2 over the eight-year study period were 31.67, 98.26, 15.57, and 26.55 µg/m3, respectively. Compared to the annual standards of 5 µg/m3 for PM2.5 and 15 µg/m3 for PM10, the levels of particulate matter were 6.3 and 6.5 times higher, respectively.

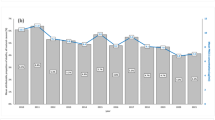
Box plot of pollutant concentration during the study period: (A) PM2.5, (B) PM10, (C) O3, (D) NO2.

Box diagram of pollutants in the study period by years.
Increased concentrations of PM in Asian cities, especially in Iran, are very common. According to a database provided by the WHO, Iranian cities rank among the world’s most polluted26.
Figure 3 shows that that the concentration of PM2.5 was highest in 2019 (50.20 µg/m3) and lowest in 2018 (20.03 µg/m3), with the highest variability in 2012 and the lowest in 2018. PM10 reached its peak concentration in 2012 (133.76 µg/m3) and lowest in 2011 (67.22 µg/m3), with the highest variability in 2014 and the lowest in 2019. O3 was highest in 2011 (15.91 µg/m3) and lowest in 2014 (14.86 µg/m3), with the highest variability in 2014 and the lowest in 2011. NO2 was highest in 2011 (59.62 µg/m3) and lowest in 2017 (7.76 µg/m3), with the highest variability in 2011 and the lowest in 2018. The findings show a general decreasing trend for PM2.5 from 2012 to 2018, although there was an increase during 2014–2015.
Wang et al. carried out a study in China and found that in the northern region, PM2.5 concentration decreased from 1980 to 1986, then increased relatively from 1985 to 1995, followed by a clear decrease over the past 15 years. In the northeastern region, it was observed that PM2.5 concentration significantly increased from 1980 to 2005 but decreased over the past 10 years, which was consistent with our findings27. For PM10, there were fluctuations in concentration. A decrease was observed in 2013, but an increase occurred in 2015, followed by a slight decrease in 2016, and finally an increase in 2017, with a subsequent decrease until 2019. Overall, it can be said that a sinusoidal trend was recorded for the annual concentration changes of PM10 over the study period. A research did in Tabriz by Barzeghar et al.28 showed that the concentration of suspended particles decreased from 2006 to 2017, which was consistent with our results. Regarding other pollutants (NO2 and O3), a relatively decreasing trend was observed. Additionally, according to the results, the concentration of PMs was higher in the cold seasons in contrast to the warm seasons. These outcomes were in line with those of Karimi et al.29 who demonstrated that particulate concentrations were noticeably greater during the cold season than they were throughout other seasons. However, Bahrami Asl found the highest particle concentrations in the spring and summer, while Miri’s study showed that the average concentration of PM2.5 was higher in winter than in spring, which was also consistent with our results11,12. A study in Pakistan on particulate matter showed that the annual average concentration of PM2.5 in one area was 71.7 µg/m3, approximately 14.3 times higher than the WHO annual guideline. The highest seasonal average concentration of PM2.5 occurred in winter and autumn, with the lowest concentration in spring, which was consistent with our results30. Asian countries generally have higher concentrations of particulate matter compared to European countries, largely due to their developing status. The findings of Yener, and Demirarslan showed that, similar to our study, PM2.5 concentrations varied seasonally, with the highest in winter (27.8 μg/m3) and the lowest in summer (20.7 μg/m3), resulting in an annual average of 25.1 μg/m331. Bukan, situated in the southernmost part of West Azerbaijan province and near Iraq (a source of dust storms), faces unique geographical challenges. The city, surrounded by mountains, is prone to pollutant accumulation, especially during cold seasons. Winter pollution increases primarily due to higher fossil fuel consumption for heating, atmospheric inversion in late autumn and early winter, and weather conditions such as low wind speeds. Additional factors, including increased coal and biomass combustion, lower precipitation, and colder temperatures, further contribute to particulate matter accumulation. Atmospheric conditions play a crucial role in pollutant transport, diffusion, and chemical reactions. During winter, high-pressure systems stabilize the atmosphere, trapping pollutants and leading to frequent high PM2.5 concentrations31,32,33.
PM2.5 concentrations and their health effects in ten Iranian cities were analyzed by Hopke et al. from March 2013 to March 2016. In most cities, PM2.5 levels decreased significantly in the third year compared to the first year, except in Ahvaz and Khorramabad, where the decrease was only significant from the second to third years. The highest levels of pollution were recorded in the cities of Ahvaz and Isfahan. Annual PM2.5 concentrations in all cities exceeded the WHO guideline of 10 μg/m3, posing serious health risks, which was consistent with our study34. The study investigated the relationship between air quality and health effects of PM10 in Khorramabad city, Iran. According to the findings, the highest PM10 concentration was recorded in August, and the overall annual average PM10 concentration was 80.59 μg/m3, with seasonal averages of 58.28 μg/m3 in winter and 80.59 μg/m3 in summer. The increase in PM10 levels in summer is mainly related to Middle Eastern dust storms originating from Iraq, Kuwait, and Saudi Arabia, which significantly affect western and southwestern Iran. While human activities contribute to PM10 emissions, these dust storms are likely the main driver of seasonal variations35. A research assessed trends in global urban exposure to O3, PM2.5 and NO2 from 2000 to 2019 using reanalysis data and ground-based monitoring networks. Exposure to PM2.5 decreased slightly globally. Improvements were observed in the eastern United States, Europe, southeastern China and Japan. NO2 concentrations increased globally. While they decreased in North America and Europe. Exposure to O3 increased globally36. A study estimated time trends and health effects associated with exposure to NOx, NO2, O3 and PM10 in three Swedish cities—Stockholm, Gothenburg and Malmö—from the 1990s to 2015. The trends were different for each pollutant: NOx and NO2 decreased in all cities, with the reduction in NOx and NO2 mainly due to reduced emissions from traffic. O3 showed an increasing trend in all cities, and PM10 had different trends—decreasing in Stockholm, increasing in Gothenburg and stable in Malmö. The trends for pollutants were similar to our study37. A study in Tehran analyzed the trends in concentrations of major air pollutants (CO, SO2, NO2, O3, PM2.5, and asbestos) from 2005 to 2016. A significant decrease (around 50%) in CO and SO2 concentrations was observed, attributed to improvements in fuel quality and vehicle emission standards during 2012–2013. Between 2011 and 2015, PM2.5 concentrations decreased by about 30%, similar to our study38.
Results from the AirQ+ software
The local WHO office in Europe created the AirQ+ software, a tool for measuring the health consequences of air pollution. Users can calculate the possible health effects of air pollution exposure with AirQ+. This software bases all of its computations on concentration–response functions and methodology that are obtained from meta-analyses and systematic reviews of epidemiological data39. It is possible to use this software to analyze pollutants like PM2.5, PM10, NO2, O3, and black carbon. A simple-to-use model for evaluating impacts of exposure to outdoor air pollution is included in AirQ+.
Total mortality
Studies conducted over several years, along with the sudden increase in diseases such as IHD, lung cancer, COPD, ALRI, stroke, cardiovascular and respiratory hospitalizations and mortality, have shown that many pollutants present in the air can have detrimental impacts on human health40,41,42.
The WHO’s suggested methodology (AirQ+) was utilized to determine the natural death rate in persons over 30 who had long-term exposure PM10, PM2.5, NO2, and O3 between 2011 and 2019. As seen in Tables 1, 2, 3 and 4, approximately 241, 316, 14, and 52 deaths were estimated due to exposure to PM2.5, PM10, O3, and NO2, respectively, over the study period for the citizens of Bukan. On the other hand, the study period’s the highest and lowest death cases were due to particulate matter and the pollutant NO2, respectively. Faridi et al.43 research showed that in 2015, about 3800 deaths were caused by exposure to ambient PM2.5 in Tehran. Shahsavani et al.44 reported that the total mortality associated with particulate matter concentrations was 1131 in the Ahvaz city. According to Khorsandi et al.45, there were approximately 89 cases of deaths in Urmia that were linked to NO2 pollution overall. The study’s objective was to estimate and quantify the health impacts of NO2 pollutants in the city’s air. Marzouni et al. also conducted a study about calculating the consequences of PM10 pollution exposure on health in Kermanshah City in 2016, and showed that the ratio of deaths attributed to the examined pollutant to the total deaths was 7.6 percent46. Another study by Hadi et al.47 in Tehran found that over three years, there were 4192, 4336, 1363, 2830, and 1216 deaths associated to PM10, PM2.5, O3, NO2, and SO2. The AirQ+ tool was utilized by Hermayurisca in Thailand to calculate the rate of premature death brought on by PM2.5 exposure. In Thailand, the average annual PM2.5 concentration was 24.15 µg/m3, and the natural mortality rate was calculated to be approximately 1107 per 100,000 people countrywide. Analysis showed that decreasing PM2.5 levels down to WHO standards could prevent 159 premature deaths per 100,000 people48. These findings can help policymakers and stakeholders develop strategies to mitigate the harmful effects of pollutant exposure.
Ischemic heart disease (IHD)
Air pollution is undoubtedly a factor in the emergence of non-communicable diseases. The primary cause of complications and death is IHD, which is typically brought on by risk factors negatively affecting the cardiovascular system. In a time-series study, Xie et al. investigated the association between fine particulate and IHD. This association was found to be nonlinear. Additionally, they demonstrated that for every 10 µg/m3 rise in PM2.5 concentration, there is a 0.27% increase in IHD mortality49.
The AirQ+ software considers the death rate due to IHD for populations over 25. Table 1 illustrates the 286 deaths in Bukan over the research period that were caused by PM2.5 exposure. This investigation’s findings are slightly lower than Ansari et al.'s study. This is because in our investigation, the number of people exposed to PM2.5 was smaller. The number of deaths from all causes—IHD, stroke, COPD, lung cancer, and acute respiratory infection—was 6710, 3797, 1145, 172, 135 and 27, according to Ansari and Ehrampoush’s 2019 research in Tehran utilizing AirQ+ software50. More recent data indicates that, even after controlling for cardiovascular risk factors, elevated PM2.5 is linked to elevated leucopoietic activity and arterial inflammation51.
Faridi et al. in a study conducted in Tehran, stated that during the years 2006 to 2015, the annual average PM2.5 and O3 ranged from 24.7 to 38.8 and 35.4 to 76 µg/m3, respectively, and significantly decreased in the last six years. However, Tehran residents were nevertheless subjected to yearly exposures that exceeded WHO guidelines. The estimation of health effects due to PM2.5 showed that mortality from IHD had the highest respiratory mortality attributed to PM2.543.
A study in Andimeshk was conducted to assess the effects of PM10 particles on cardiovascular disease deaths in 2022–2023 using the AirQ+ program. According to the findings, the city under investigation had a high concentration of dust particles, indicating pollution. During a year, PM10 concentration did not exceed the standard in only 8 days. According to AirQ+ estimations, there were 43 deaths and a 39.31% short-term exposure mortality rate linked to PM10. Additionally, long-term exposure mortality rate due to PM10 was 5.66%, with 11 cardiovascular deaths52. In another study, using data from 25 monitoring sites, the annual exposure to PM in the northern area of Colombia was calculated between 2011 and 2019. AirQ+ was used to estimate mortality. According to estimates, the annual mortality rate attributed to ALR diseases in children ≤ 4 years old and deaths in adults over 18 years old due to COPD, IHD, lung cancer, and stroke per 100,000 inhabitants were 33, 17, 49, 8, and 27, respectively39. Despite scientific advancements, unhealthy air can still claim many victims.
Respiratory diseases
Air pollution is an avoidable risk factor that imposes a significant burden on society due to increased mortality and high socio-economic costs, particularly in countries with low and medium incomes. Substantial evidence indicates that air pollution leads to respiratory diseases such as acute infections, lung cancer, and COPD. Even at very low levels of pollution, harmful effects on respiratory health are observed.
Regarding mortality from ALRI due to exposure to particulate matter, younger children under 5 years old are more affected, and research on this topic is limited. In our study, 15 deaths due to ALRI attributed to PM2.5 occurred in Bukan from 2011 to 2019. There have been reports of 27 cases in Tehran50. In Shahrekord, mortality rates attributable to PM2.5 for IHD, lung cancer, COPD, ALRI, and stroke were 176, 0, 7, 10, and 105, respectively15.
When discussing lung cancer, most people think of smoking, which is the primary cause. However, environmental factors like air pollution, which also contributes to lung cancer, should not be overlooked. According to a meta-analysis on lung cancer, after being exposed to PM2.5, there was a 1.08 (95% CI 1.03–1.12) and 1.11 (95% CI 1.05–1.18) relative risk (RR) of lung cancer incidence and mortality, respectively. Continental analysis also showed that the RR of mortality from lung cancer associated with PM2.5 was estimated to be 1.15, 1.12, and 1.05 in North America, Asia, and Europe, respectively53. Pablo-Romero et al. demonstrated in their study that a 10 µg/m3 decrease in PM2.5 concentration may contribute to reduction in paediatric hospitalizations for respiratory illnesses (0.09 cases per year)54. The strong link between air pollution and lung cancer has been the subject of numerous investigations. There were 26 lung cancer-related deaths from PM2.5 exposure during the study period in the current study.
One of the most sensitive populations to air pollution is patients with COPD. A non-communicable illness with several side effects is COPD. Research indicates that there is a growing risk of hospitalization and death from COPD. Air pollution exposure significantly contributes to the development of COPD worldwide, with recent estimates suggesting that this factor (air pollution) accounts for 50% of the total risk of the disease. Research has shown that both gaseous and particulate pollutants are involved in the onset of COPD. Additionally, no level of air pollution is completely safe, and there is a linear association between respiratory episodes and air pollution levels55. Thirty-four COPD-related deaths in Bukan were linked to PM2.5 exposure in our study, while 38 deaths were linked to PM10 exposure. Hajizadeh et al. assessed exposure to PM2.5 between 2014 and 2019 in Iran. According to the results, PM2.5 was found to be responsible for 15% of all COPD deaths and 17% of all lung cancer deaths56. In a 2019 study, Sicard et al. used the AirQ+ software to evaluate the effects of PM2.5, PM10, and O3 on respiratory and cardiovascular diseases in cities in France, Iran, and Italy. They discovered that exposure to these pollutants resulted in 8200 accidental deaths, 2400 deaths from respiratory diseases, 540 deaths from cardiovascular diseases, 220 deaths from COPD, 18,800 hospitalizations for cardiovascular diseases, and 3400 hospitalizations for respiratory diseases57. In Turkey, a study aimed at calculating COPD and lung cancer mortality attributable to PM2.5 using AirQ+ software was conducted in 2019. In Turkey, the annually averages for PM2.5 and PM10 were determined to be 28.82 µg/m3 and 48.08 µg/m3, respectively. The death rates associated with PM2.5 for lung cancer and COPD were estimated to be 15% and 22%, respectively58. Implementing pollution source control measures could prevent one in six deaths from lung cancer and one in five deaths from COPD. Fifty-two deaths from respiratory illnesses as a result of ozone exposure were recorded in our study during the study period. Due to its high oxidizing capability, ozone can react with respiratory tissues upon inhalation, leading to an overload in the respiratory system, which can result in mortality. A review study indicated that respiratory disease mortality significantly increases by 0.55% for every 10 µg/m3 increase in 8-h average maximum ozone concentration59.
Stroke
Stroke continues to be the second most common cause of death (11.6% of all deaths) despite recent improvements in prevention and treatment60. Stroke is a disease with diverse causes. In recent years, air pollution, due to industrial advancements in cities and countries, has become an environmental issue. Strong proof that the association between long-term exposure to ambient air pollution and stroke incidence and mortality has been found in cohort studies conducted in North America, Europe, and Asia42. A review study by Niu et al. examined 68 articles. The meta-analysis results showed that exposure to PM10, PM2.5, NO2, and SO2 was linked with an increased risk of mortality due to stroke61. While the exact mechanisms behind the relationship between exposure to air pollution and stroke remain unclear, other paths have been proposed, such as endothelial dysfunction, oxidative stress, and inflammation. As indicated in Table 1, 179 occurrences of stroke-related death linked to PM2.5 exposure were noted in Bukan during the study period (2011–2019). It can be said that Bukan has a high incidence of stroke as a result of air pollution, although other factors also contribute to stroke occurrence. Faridi et al. examined the effects of PM2.5 exposure over ten years in Tehran. According to the results, between 24.5 and 36.2% of deaths from cerebrovascular illness (stroke) was estimated to be due to PM2.5 exposure43. In Ardabil, the overall deaths from ALRI, COPD, lung cancer, IHD, and stroke due to exposure to PM2.5 was 73, 11, 7, 15, and 14, respectively, during the study period62. It has been discovered that increased levels of air pollutants, specifically PM2.5, can result in mild to severe strokes.
Conclusion
This study analyzed air pollution trends and their health impacts using the WHO-recommended AirQ+ software. The findings indicate that Bukan residents are exposed to PM2.5 and PM10 levels 6.3 and 6.5 times higher than WHO guidelines, significantly increasing mortality risks. We specifically selected AirQ+ for this study because it is a widely recognized tool developed by the WHO for estimating the public health impacts of air pollution and aligns well with our study objectives. Additionally, AirQ+ has been extensively used in epidemiological studies, particularly in regions adhering to WHO guidelines. While BenMAP-CE also provides robust estimates of health impacts and includes economic valuation, its primary application has been within the U.S. regulatory framework. However, we acknowledge its growing global adoption and the potential for comparative analysis. Studies have demonstrated that both AirQ+ and BenMAP-CE yield similar results when using the same input data. Nevertheless, we recognize that a direct comparison of multiple models within our study would further strengthen the validity of our results. However, it is important to acknowledge the limitations of this study, such as the single-model approach. Therefore, we recommend that future research incorporate BenMAP-CE and other models, such as GAINS, to enhance the robustness and cross-validation of findings. Beyond the health consequences, air pollution imposes substantial economic and social burdens, including rising healthcare costs, reduced labor productivity, and, in extreme cases, forced migration. Addressing this crisis requires stricter environmental regulations, investment in clean energy, and public awareness initiatives. A comprehensive air pollution management strategy is crucial for safeguarding public health, ensuring economic stability, and improving the overall quality of life. Additionally, exploring policy-driven interventions and their effectiveness in mitigating air pollution would be a valuable extension of this research.
Data availability
The datasets generated and analyzed during the current study were available from the corresponding author on reasonable request.
References
Münzel, T., Sørensen, M., Hahad, O., Nieuwenhuijsen, M. & Daiber, A. The contribution of the exposome to the burden of cardiovascular disease. Nat. Rev. Cardiol. 20, 651–669 (2023).
Pozzer, A. et al. Mortality attributable to ambient air pollution: A review of global estimates. GeoHealth 7, e2022GH000711 (2023).
Loomis, D. et al. The carcinogenicity of outdoor air pollution. Lancet Oncol. 14, 1262–1263 (2013).
Dehghani, M. H., Hopke, P. K., Asghari, F. B., Mohammadi, A. A. & Yousefi, M. The effect of the decreasing level of Urmia Lake on particulate matter trends and attributed health effects in Tabriz, Iran. Microchem. J. 153, 104434 (2020).
Orellano, P., Reynoso, J., Quaranta, N., Bardach, A. & Ciapponi, A. Short-term exposure to particulate matter (PM10 and PM2.5), nitrogen dioxide (NO2), and ozone (O3) and all-cause and cause-specific mortality: Systematic review and meta-analysis. Environ. Int. 142, 105876 (2020).
Yu, W. et al. Estimates of global mortality burden associated with short-term exposure to fine particulate matter (PM2.5). Lancet Planet. Health 8, e146–e155 (2024).
WHO. Ambient air pollution, (2022).
Pérez Medina, P., Galindo Mendoza, M. G., Álvarez Fuentes, G., Tenorio Martínez, L. D. & Barrera López, V. A. Economic assessment of the impact of the sugarcane industry: An empirical approach with two focuses for San Luis Potosí, México. J 6, 342–360 (2023).
Errigo, I. M. et al. Human health and economic costs of air pollution in Utah: An expert assessment. Atmosphere 11, 1238 (2020).
Mohajeri, A., Najafizadeh, S. A. & Sarlak, A. Relationship between CO2 and Iran’s economic growth with an emphasis on household welfare index (an economy with oil and economy without oil). Adv. Environ. Technol. 6, 119–130 (2020).
Asl, F. B. et al. Health impacts quantification of ambient air pollutants using AirQ model approach in Hamadan, Iran. Environ. Res. 161, 114–121 (2018).
Miri, M. et al. Mortality and morbidity due to exposure to outdoor air pollution in Mashhad metropolis, Iran. The AirQ model approach. Environ. Res. 151, 451–457 (2016).
Mirzaei, A., Tahriri, H. & Khorsandi, B. Comparison between AirQ+ and BenMAP-CE in estimating the health benefits of PM2.5 reduction. Air Qual. Atmos. Health 14, 807–815 (2021).
Amini, H. et al. Two decades of air pollution health risk assessment: Insights from the use of WHO’s AirQ and AirQ+ tools. Public Health Rev. 45, 1606969 (2024).
Naghan, D. J. et al. Estimation of the effects PM2.5, NO2, O3 pollutants on the health of Shahrekord residents based on AirQ+ software during (2012–2018). Toxicol. Rep. 9, 842–847 (2022).
Ngutuka Kinzunga, M. et al. Assessment of respiratory health impacts of PM2.5 by AirQ+ software in a Sub-Saharan African Urban Setting. Atmosphere 15, 1518 (2024).
Asgari, G. et al. Assessment of health impacts of PM2.5 by AirQ+ software in the city of Sanandaj, Iran (2018–2019). J. Adv. Environ. Health Res. 9, 45–56 (2021).
Kamarehie, B. et al. Quantification of health effects related to SO2 and NO2 pollutants by using air quality model. J. Adv. Environ. Health Res. 5, 44–50 (2017).
Karbassi, A., Bidhendi, G. N., Pejman, A. & Bidhendi, M. E. Environmental impacts of desalination on the ecology of Lake Urmia. J. Great Lakes Res. 36, 419–424 (2010).
Jalili, S., Kirchner, I., Livingstone, D. M. & Morid, S. The influence of large-scale atmospheric circulation weather types on variations in the water level of Lake Urmia, Iran. Int. J. Climatol. 32, 1990–1996 (2012).
De Hoogh, K. et al. Spatial PM2.5, NO2, O3 and BC models for Western Europe–evaluation of spatiotemporal stability. Environ. Int. 120, 81–92 (2018).
Sacks, J. D. et al. Quantifying the public health benefits of reducing air pollution: Critically assessing the features and capabilities of WHO’s AirQ+ and US EPA’s environmental benefits mapping and analysis program—community edition (BenMAP—CE). Atmosphere 11, 516 (2020).
Brito, J., Bernardo, A. & Gonçalves, L. L. Atmospheric pollution and mortality in Portugal: Quantitative assessment of the environmental burden of disease using the AirQ+ model. Sci. Total Environ. 815, 152964 (2022).
Azimi, F. et al. Temporal characteristics and health effects related to NO2, O3, and SO2 in an urban area of Iran. Environ. Pollut. 349, 123975 (2024).
Bonyadi, Z., Ehrampoush, M. H., Ghaneian, M. T., Mokhtari, M. & Sadeghi, A. Cardiovascular, respiratory, and total mortality attributed to PM 2.5 in Mashhad, Iran. Environ. Monit. Assess. 188, 1–6 (2016).
Hadei, M. et al. Estimation of lung cancer mortality attributed to long-term exposure to PM2.5 in 15 Iranian cities during 2015–2016; an AIRQ+ modeling. J. Air Pollut. Health 2, 19–26 (2017).
Yousefi, R. et al. Fine particulate matter (PM2.5) trends from land surface changes and air pollution policies in China during 1980–2020. J. Environ. Manag. 326, 116847 (2023).
Barzeghar, V., Sarbakhsh, P., Hassanvand, M. S., Faridi, S. & Gholampour, A. Long-term trend of ambient air PM10, PM2.5, and O3 and their health effects in Tabriz city, Iran, during 2006–2017. Sustain. Cities Soc. 54, 101988 (2020).
Karimi, A. et al. Concentrations and health effects of short-and long-term exposure to PM2.5, NO2, and O3 in ambient air of Ahvaz city, Iran (2014–2017). Ecotoxicol. Environ. Safety 180, 542–548 (2019).
Moyebi, O. D. et al. Fine particulate matter and its chemical constituents’ levels: A troubling environmental and human health situation in Karachi, Pakistan. Sci. Total Environ. 868, 161474 (2023).
Yener, İ & Demirarslan, K. O. Determining the factors affecting air quality in Marmara, Turkey, and assessing it using air quality indices. Doğal Afetler ve Çevre Dergisi 8, 383–395 (2022).
Cha, Y., Song, C.-K., Jeon, K.-H. & Yi, S.-M. Factors affecting recent PM2.5 concentrations in China and South Korea from 2016 to 2020. Sci. Total Environ. 881, 163524 (2023).
Wang, T. et al. Prediction of the impact of meteorological conditions on air quality during the 2022 Beijing Winter Olympics. Sustainability 14, 4574 (2022).
Hopke, P. K. et al. Spatial and temporal trends of short-term health impacts of PM2.5 in Iranian cities; A modelling approach (2013–2016). Aerosol Air Qual. Res. 18, 497–504 (2018).
Nourmoradi, H. et al. Air quality and health risks associated with exposure to particulate matter: A cross-sectional study in Khorramabad, Iran. Health Scope 5, e31766 (2016).
Sicard, P. et al. Trends in urban air pollution over the last two decades: A global perspective. Sci. Total Environ. 858, 160064 (2023).
Olstrup, H. et al. Trends in air pollutants and health impacts in three Swedish cities over the past three decades. Atmos. Chem. Phys. 18, 15705–15723 (2018).
Torbatian, S., Hoshyaripour, A., Shahbazi, H. & Hosseini, V. Air pollution trends in Tehran and their anthropogenic drivers. Atmos. Pollut. Res. 11, 429–442 (2020).
Arregocés, H. A., Rojano, R. & Restrepo, G. Health risk assessment for particulate matter: Application of AirQ+ model in the northern Caribbean region of Colombia. Air Qual. Atmos. Health 16, 897–912 (2023).
Manisalidis, I., Stavropoulou, E., Stavropoulos, A. & Bezirtzoglou, E. Environmental and health impacts of air pollution: A review. Front. Public Health 8, 14 (2020).
Phosri, A. et al. Effects of ambient air pollution on daily hospital admissions for respiratory and cardiovascular diseases in Bangkok, Thailand. Sci. Total Environ. 651, 1144–1153 (2019).
Kulick, E. R., Kaufman, J. D. & Sack, C. Ambient air pollution and stroke: an updated review. Stroke 54, 882–893 (2023).
Faridi, S. et al. Long-term trends and health impact of PM2.5 and O3 in Tehran, Iran, 2006–2015. Environ. Int. 114, 37–49 (2018).
Shahsavani, A. et al. The evaluation of PM10, PM2.5, and PM1 concentrations during the Middle Eastern Dust (MED) events in Ahvaz, Iran, from April through September 2010. J. Arid Environ. 77, 72–83 (2012).
Khorsandi, H., Karimzade, S., Aghaei, M., Kargar, H. & Mousavi Moghanjooghi, S. The estimation and quantification of health effects attributed to no2 pollutant in the air of Urmia, Iran. Stud. Med. Sci. 26, 1054–1062 (2016).
Marzouni, M. B. et al. A comparison of health impacts assessment for PM10 during two successive years in the ambient air of Kermanshah, Iran. Atmos. Pollut. Res. 7, 768–774 (2016).
Hadei, M. et al. Estimation of mortality and hospital admissions attributed to criteria air pollutants in Tehran metropolis, Iran (2013–2016). Aerosol Air Qual. Res. 17, 2474–2481 (2017).
Hermayurisca, F. & Taneepanichskul, N. Estimation of premature death attributed to short-and long-term PM2.5 exposure in Thailand. Environ. Monit. Assess. 195, 1176 (2023).
Xie, W. et al. Relationship between fine particulate air pollution and ischaemic heart disease morbidity and mortality. Heart 101, 257–263 (2015).
Ansari, M. & Ehrampoush, M. H. Meteorological correlates and AirQ+ health risk assessment of ambient fine particulate matter in Tehran, Iran. Environ. Res. 170, 141–150 (2019).
Abohashem, S. et al. A leucopoietic-arterial axis underlying the link between ambient air pollution and cardiovascular disease in humans. Eur. Heart J. 42, 761–772 (2021).
Seihei, N. et al. Short-term and long-term effects of exposure to PM10. Clin. Epidemiol. Global Health 27, 101611 (2024).
Huang, F., Pan, B., Wu, J., Chen, E. & Chen, L. Relationship between exposure to PM2.5 and lung cancer incidence and mortality: A meta-analysis. Oncotarget 8, 43322 (2017).
de Pablo-Romero, M. P., Román, R., Limón, J. M. G. & Praena-Crespo, M. Effects of fine particles on children’s hospital admissions for respiratory health in Seville, Spain. J. Air Waste Manag. Assoc. 65, 436–444 (2015).
Sin, D. D. et al. Air pollution and COPD: GOLD 2023 committee report. Eur. Respir. J. 61, 2202469 (2023).
Hajizadeh, Y. et al. Concentrations and mortality due to short-and long-term exposure to PM2.5 in a megacity of Iran (2014–2019). Environ. Sci. Pollut. Res. 27, 38004–38014 (2020).
Sicard, P., Khaniabadi, Y. O., Perez, S., Gualtieri, M. & De Marco, A. Effect of O 3, PM 10 and PM 2.5 on cardiovascular and respiratory diseases in cities of France, Iran and Italy. Environ. Sci. Pollut. Res. 26, 32645–32665 (2019).
Yekdeş, D. H. et al. Chronic obstructive pulmonary disease and lung cancer mortality attributed to air pollution in Türkiye in 2019. Aerosol. Air Qual. Res. 23, 230144 (2023).
Zhang, Y. et al. Respiratory mortality associated with ozone in China: A systematic review and meta-analysis. Environ. Pollut. 280, 116957 (2021).
Feigin, V. L. et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 20, 795–820 (2021).
Niu, Z., Liu, F., Yu, H., Wu, S. & Xiang, H. Association between exposure to ambient air pollution and hospital admission, incidence, and mortality of stroke: An updated systematic review and meta-analysis of more than 23 million participants. Environ. Health Prev. Med. 26, 1–14 (2021).
Moradi, M., Mokhtari, A., Mohammadi, M. J., Hadei, M. & Vosoughi, M. Estimation of long-term and short-term health effects attributed to PM 2.5 standard pollutants in the air of Ardabil (using Air Q+ model). Environ. Sci. Pollut. Res. 29, 21508–21516 (2022).
Acknowledgements
The authors gratefully acknowledge the financial support from Iran University of Medical Sciences, Tehran, Iran (Grant Number: 99-1-75-18618) and (Grant Number: 1400-3-99-22345). Additionally, the cooperation of the Research Center for Environmental Health Technology in providing experimental equipment and supplies is greatly appreciated.
Author information
Authors and Affiliations
Contributions
Pegah Nakhjirgan: Conceptualization, Methodology, Investigation, Formal analysis, Writing–original draft. Ahmad Jonidi Jafari, Abbas Shahsavani, Zahra Kazemi, Zohre Kazemi, Farzad Fanaei: Methodology, Investigation, Formal analysis, Writing–review and editing. Majid Kermani: Methodology, Writing–review and editing, Supervision. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nakhjirgan, P., Jonidi Jafari, A., Kermani, M. et al. Assessment of disease burden and mortality attributable to air pollutants in northwestern Iran using the AirQ+ software. Sci Rep 15, 13566 (2025). https://doi.org/10.1038/s41598-025-97348-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-97348-x
