
Abstract
Previous studies exploring the effects of the business cycle on sleep have mostly focused on the general population, and their results have been inconclusive. This study aimed to explore the effects of the 2008 economic crisis and personality traits on the subjective sleep quality of outpatients with mood disorders. In this cross-sectional study, patients with mood disorders were recruited from two medical centers and a psychiatric hospital. Socio-demographics, the Eysenck Personality Questionnaire-Revised, and the Pittsburgh Sleep Quality Index (PSQI) were collected through in-person interviews. Candidate predictors significantly associated with PSQI scores in univariate analysis were included in a multiple linear regression model. There were 334 participants; 29% had unipolar depression, and 71% had bipolar affective disorder. The average PSQI score was 11.0 (±4.0). A higher degree of neuroticism [β(se) = 0.49 (0.07), p < 0.001] and recession period (vs. recovery period) [β(se) = 1.72 (0.47), p < 0.001] were associated with a higher PSQI score after adjusting for education, occupational class, and diagnosis. In conclusion, neuroticism and macroeconomy were independent predictors of subjective sleep quality in patients with mood disorders. This study suggests that large-scale economic crises have negative impacts on the sleep health of high-risk clinical populations.
Similar content being viewed by others


Introduction
The Great Recession in 2008 was the first global financial crisis since World War II. According to the countercyclical hypothesis, economic fluctuations are closely associated with changes in psychiatric hospitalization rates. During economic recessions, people who lose their jobs suffer from mental illnesses, while the mental health of those who continue to work is also negatively impacted by the contextual effect of high unemployment rates (Brenner, 1973). In fact, suicide rates have been shown to increase in parallel with unemployment rates in many countries during economic crises in recent years (Chang et al., 2013, 2009). Meanwhile, supporters of the procyclical relationship between business cycles and morbidity propose that an increase in work-related stress during economic booms heightens the risk of unhealthy behaviors. Better income has also been reported to increase fat, alcohol, and tobacco consumption (Ruhm, 2000; Tapia Granados, 2005; Tapia Granados and Ionides, 2008).
Sleep plays a crucial role in good mental health, and its relationship with economic cycles has yielded varied conclusions. Some studies suggest that economic expansions may reduce sleep time among working individuals, while economic recessions could lead to more sufficient sleep (Barnes et al., 2016; Cardon et al., 2018). Job insecurity and financial distress have been associated with decreased sleep duration, while higher regional unemployment rates were linked to longer sleep duration (Antillón et al., 2014; Mai et al., 2019; Perales and Plage, 2017). Nevertheless, solely evaluating mental distress based on sleep duration may be questionable due to the trade-off between sleep duration and work time. Moreover, the conceptual split of sleep into quality and duration appears to be well-established, with sleep quality being recognized as a more critical public health concern than sleep duration (Bin, 2016). Self-reported sleep quality has higher predictive power for physical and psychiatric comorbidities compared to sleep duration (Cappuccio et al., 2010; Seow et al., 2020). Public health interventions based solely on population averages may not account for individual differences in sleep needs; however, interventions to improve sleep quality have the potential to benefit all individuals (Bin, 2016).
To comprehensively investigate the effect of macroeconomic factors on the sleep quality of a clinical population and understand the underlying mechanisms, it is crucial to consider the dynamic interplay between individual susceptibility and external stressors. The stress-diathesis model offers a valuable framework in this context, emphasizing that individuals with predisposing factors (e.g., genetic, physiological, psychological) may develop acute sleep disturbances when faced with precipitating stressors (Colodro-Conde et al., 2018; Ingram and Luxton, 2005; Spielman et al., 1987). This model highlights the role of both predisposition and environmental factors in the development of sleep disturbances, suggesting that a combination of these factors is necessary for their occurrence (Spielman et al., 1987). While previous studies have explored how economic fluctuations affect subjective sleep quality, they have predominantly focused on the general population, overlooking the higher prevalence of predisposing factors to stress-induced insomnia among people with mental illnesses (Ohayon and Guilleminault, 2005). Notably, no prior research has investigated this issue among psychiatric patients in a clinical setting.
In our study, we focused on two personality dimensions proposed by Eysenck, namely neuroticism/stability and extraversion/introversion, which are known to influence emotional stability and interpersonal interactions (Eysenck, 1963). People with high neuroticism tend to experience heightened negative emotions and poor sleep quality when faced with adverse events (Calkins et al., 2013; Duggan et al., 2014), while those high in extraversion exhibit energetic and prosocial tendencies, which can serve as a protective factor against depression and sleep disturbance (Allen et al., 2016; Dørheim et al., 2016; Dekker et al., 2017). These personality traits have been found to play a crucial role in shaping individuals’ responses to stress and affecting sleep quality.
In our study involving patients with mood disorders, we aimed to explore the interaction between personality traits and macroeconomic factors, specifically the 2008 economic crisis, in relation to subjective sleep quality. Our hypotheses were twofold. First, following the countercyclical hypothesis (Brenner, 1973), we hypothesized that during an economic downturn, individuals with mood disorders would experience worse subjective sleep quality compared to periods of economic expansion. Second, in line with the stress-diathesis model, which suggests that susceptible individuals are more prone to psychopathology under external stressors, we hypothesized that individuals with high neuroticism would have poorer subjective sleep quality than those with low neuroticism, particularly during economic recessions.
Methods
Participants
This study was cross-sectional in design. We recruited outpatients who agreed to participate in different time periods and compared the composition of personality traits and sleep quality in each period. Psychiatric outpatients from two medical centers and a psychiatric hospital located in Taiwan were invited to participate in this study from July 2008 to February 2011. All study participants gave written informed consent, and the recruitment protocol was approved by the Institutional Review Board of the National Taiwan University Hospital (IRB No. 201907138RIND) as well as performed in accordance with guidelines in the Declaration of Helsinki. The recruitment criteria were patients who were aged 18 to 65 years and had been diagnosed with major depressive disorder (MDD) or bipolar affective disorder (BAD, including type I and type II) according to DSM-IV-TR and were not currently in acute episodes. Eligible cases were referred by psychiatrists and were then interviewed with the Schedule for Affective Disorder and Schizophrenia-Lifetime to confirm their diagnoses of mood disorders. Participants with total scores of the Hamilton Depression Rating Scale and Young Mania Rating Scale (YMRS) lower than 16 were included (Hamilton, 1960). Participants who had comorbid schizophrenia, organic psychosis, neurodevelopmental disorders, substance-induced mood disorder, or whose diagnosis changed during the study period were excluded (Lai et al., 2010).
Tools
Eysenck personality questionnaire-revised (EPQ-S)
Participants completed the Chinese version of the EPQ-S to measure the traits of neuroticism and extraversion (Wu et al., 2012). This version of the questionnaire demonstrated good reliability for neuroticism and extraversion in previous research, leading to their evaluation in this study. However, due to issues with reliability, psychoticism was excluded from the assessment (Su et al., 2018).
Pittsburgh sleep quality index (PSQI)
The PSQI was utilized to assess the subjective sleep quality of study participants over the past month. Comprising 19 items, the PSQI evaluates seven domains related to subjective sleep quality. The completion time for this assessment ranged from 5 to 10 min (Buysse et al., 1989). In this study, a higher PSQI global score was used to indicate worse subjective sleep quality during the previous month. The Chinese version of the PSQI has been confirmed to possess good validity and reliability (Tsai et al., 2005).
Definition of macroeconomic periods
We used the economic growth rate and the unemployment rate to differentiate between recession and recovery periods. The economic growth rate turned from positive to negative (−1.32%) in the third quarter of 2008, reached a trough in the first quarter of 2009 (−7.88%), and was then positive until the fourth quarter of 2009 (9.04%) (Directorate General of Budget, 2021). Meanwhile, the unemployment rate increased from 3.95% in June 2008 to 6.13% in August 2009 and then gradually declined. Therefore the 15-month period between July 2008 and September 2009 was defined as the economic crisis period, and October 2009 to February 2011 was defined as the recovery period.
With regard to the health impact of the economic crisis, some studies have suggested that the effects may have lasted from months to over a decade, although there is currently no consensus among researchers (Brenner, 1979; Tapia Granados, 2008; Yoon et al., 2012). From a macroeconomic viewpoint, the economic growth rate in Taiwan turned from negative to positive, and the unemployment rate fell to 4% in 2010, which seems to be closer to the pre-crisis situation in 2007 than the recession in 2009. Nevertheless, it can be argued that the economic crisis had an impact on the job market and that it was different from the pre-crisis period in 2007, such as an increase in the proportion of non-standard employment and a decrease in average income. Based on these uncertainties, we performed sensitivity analyses and used different definitions of the starting point of the economic recovery to compare the results in this study.
Procedure
The participants were interviewed by trained assistants to collect data including gender, age, marital status, educational attainment, occupation, and average monthly income, and they were asked to complete the Chinese version of the EPQ-S and the PSQI.
Statistical analysis
Statistical analyses were performed using Microsoft Excel 2016 and SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). The χ2 test, t-test, or ANOVA were used for univariate analysis. Pearson correlation analysis was conducted to evaluate the correlations among independent variables with the total PSQI score. A p-value < 0.05 was regarded as being statistically significant. Candidate predictors significantly associated with PSQI were subsequently included in multiple linear regression analyses to examine their independent effects on sleep quality. The values of R2 of the reduced model and complete model were compared to determine the contributions of neuroticism trait and economic period on variance in PSQI. Sensitivity analysis with simple linear regression was conducted by resetting the starting date of economic recovery. Therefore, we could observe changes in the regression coefficient during the crisis (before September 2009) to after the recovery at different timepoints. The patients were then divided into two groups according to their neuroticism score (≥7 for the high neuroticism group, <7 for the low neuroticism group, 7 was the median score of neuroticism) for stratified analysis in order to investigate the potential effects of selection bias.
Results
A total of 334 outpatients were enrolled in this study. Their sociodemographic and clinical profiles are outlined in Table 1. The average age of the participants was 38.6 ± 13.1 years, and 54% were female. One-third of the participants were not married. With regard to income, 33.5% had no income, and 24% had a monthly income of <30,000 NTD (around 1000 USD). Only 28% of the patients had an educational attainment lower than junior high school, and 44% had high school degrees. Most participants (63%) were unemployed or worked irregularly. Overall, 29% of the participants were diagnosed with MDD, and the other 71% were diagnosed with BAD. The average PSQI score was 11.0 (±4.0). There was no statistically significant difference in the gender proportion, marital status, educational attainment, and average neuroticism score between participants recruited in different periods.
The correlations between PSQI global score and continuous independent variables (i.e., age and personality trait). PSQI global score was positively correlated with neuroticism (r = 0.33, p < 0.01), while the correlation with extraversion was not significant (r = −0.07, p > 0.05). Age was not significantly associated with PSQI score. Univariate analysis of categorical independent variables showed that gender, marital status, income level, and occupational class were not associated with PSQI scores (Table 2). Only educational attainment (p = 0.001) and diagnostic group were associated with significant between-group differences in sleep quality. The participants with lower educational attainment had higher PSQI scores, and those diagnosed with MDD had worse sleep quality than those with BAD.
Univariate analysis showed that age (p < 0.001), income level (p = 0.01), occupational class (p = 0.003), and trait of extraversion (p = 0.047) of the patients were significantly different in the recession and recovery periods. Considering these findings in univariate analysis, we included variables related to PSQI or economic period into subsequent multivariate linear regression analysis to adjust for sociodemographic and clinical factors. After adjusting for education, occupational class, and diagnosis, the effects of neuroticism and economic period on sleep quality were still significant. The participants with a higher degree of neuroticism [β(se) = 0.49 (0.07), p < 0.001] and recession period (vs. recovery period) [β(se) = 1.72(0.47), p < 0.001] were associated with a higher PSQI score (Table 3). We then compared the R2 values among reduced models and the complete model and found that neuroticism and economic period explained 10.8% and 2.5% variance of the model, respectively.
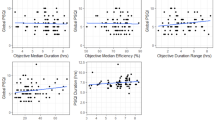
Regression coefficients of economic crisis (vs. recovery period) in a simple linear regression model with different starting timepoints of economic recovery were computed. The results showed that there was a significant difference in PSQI total scores between periods. Figure 1A demonstrates that reported sleep quality was worse during the recession than during the recovery period. Moreover, the differences showed an increasing trend from 1.50 (before September 2009 vs. after September 2009) to 2.79 times (before September 2009 vs. after June 2010). We then performed the analysis again by resetting the starting timepoint of the recovery to after July 2010, and no significant between-period differences were found. This may be due to the small number of participants. Figure 1B illustrates the results of stratified analysis by neuroticism level. Similar trends were observed in the high and low neuroticism groups.

Panel A total participants (N = 334) and B upper line: participants with neuroticism score ≥ 7; lower line: participants with neuroticism score < 7; * indicates p-value < 0.05.
Discussion
Our results suggested that both macroeconomic factors and personality traits had prominent influences on the psychopathology of clinical populations. We investigated the associations between neurotic personality, the 2008 economic crisis, and the self-reported sleep quality of psychiatric outpatients with mood disorders. After adjusting for demographic and clinical covariates, we found that patients who visited outpatient services during the Great Recession had worse sleep quality than those who visited during the economic recovery period. In addition, patients with a high level of neuroticism had worse sleep quality than those with a low level of neuroticism.
Some findings from this study are consistent with previous research, namely, that low educational attainment, manual work (compared to irregular employment), and MDD (relative to BAD) were associated with insomnia (Gellis et al., 2005; Roy et al., 2006; Sun et al., 2015). Furthermore, after adjusting for individual socioeconomic and medical factors, we found that neurotic personality and economic crisis still had marked influences on sleep quality, indicating their independent roles in patients’ mental health.
Neuroticism, but not extraversion, was positively correlated with the PSQI total score in our outpatient sample. Similarly, Tanji et al. reported no association between extraversion and suicide risk in community-dwelling subjects after the 1997–1998 economic crisis in Japan (Tanji et al., 2015). However, they found an increased risk of suicide death among those with the highest neuroticism compared to those with the lowest neuroticism. Supporters of the trait activation theory posit that stressful situations activate relevant personality traits and further magnify differences in behavioral patterns (Caspi and Moffitt, 1993; Tett et al., 2021). For example, Kroencke et al. reported that, during the COVID-19 pandemic, neurotic people paid more attention to relevant information and were more preoccupied with or worried about the pandemic compared to their counterparts (Kroencke et al., 2020). These findings suggest that the mechanism by which neuroticism leads to insomnia involves heightened emotional reactivity and distress, which may contribute to the persistence of sleep disturbances (Calkins et al., 2013).
In the present study, we also found that large-scale economic stress reduced the sleep quality of patients with mood disorders. However, in contrast with Tanji’s findings, we did not discover a significant interaction between the Great Recession and neurotic personality. In other words, the extent to which the economic crisis impacted sleep quality did not change among patients with different levels of personality traits. There are several possible explanations for these findings. First, neuroticism may have been correlated with sleep quality during the economic upturn but not during the recession period. The strong situation hypothesis posits that enormous environmental tension attenuates the influence of personality on human behaviors (Cooper and Withey, 2009). Nevertheless, neuroticism and the PSQI score were both significantly correlated with sleep quality in our two study periods, and the associations remained consistent at the different time periods.
Second, the interaction effect between macro- and individual-level predictors on insomnia symptoms may be less prominent in clinical populations than in the general public. Since mental disorders are the most important contributor to psychopathology, the moderating effect of macro-level adversities can be reduced if the trait activation theory or the strong situation hypothesis are not manifested. However, further studies are needed to clarify this issue. In addition, we recruited patients from psychiatric outpatient departments who volunteered to participate in this study. However, the recruitment process might have been influenced by mental health service utilization and patients’ motivation to participate in research, which partially depended on personality traits and could vary between different time periods.
Third, an interaction effect might not have occurred immediately but could have developed a few months after the recovery period. We found that sleep quality was worse during the economic recession period than during the recovery period. Furthermore, this difference in sleep quality increased when the starting point of the recovery period was set to a later date (from October 2009 to June 2010). This indicated that sleep quality gradually improved after the end of the economic crisis. Participants with high neuroticism showed persistent inter-period differences, whereas participants with low neuroticism did not show significant inter-period differences until five months after the end of the crisis. To examine this explanation, we divided the recovery period into early (1–5 months post-crisis) and late (6–9 months post-crisis) periods and compared both results. Nevertheless, we did not find a significant interaction effect in the early or late recovery periods, and thus a delayed interaction effect was unlikely.
The background of this study should be taken into consideration. The 2008–2009 economic crisis did not last long in Taiwan, so the psychological impact might have been rather transient and mild for most people. For example, the national suicide rate in Taiwan peaked in 2006 and then steadily declined thereafter without fluctuating around 2008 (Liao et al., 2015). Considering this situation, insomnia, a hallmark symptom of most common mental disorders, would be the most sensitive measurement for mental distress caused by economic fluctuations. Brenner proposed that the health effects of business cycles can lag for years or even a decade, but this argument has not been widely accepted yet (Brenner, 2005; Tapia Granados, 2017). Our results showed that sleep quality significantly improved one year after the economic upturn. Because the recession did not last for long in Taiwan, and insomnia responds faster to external stress than other chronic illnesses, we did not expect to observe a lagged health effect in psychiatric outpatients. However, further studies with an adequate follow-up period are warranted.
Furthermore, we recruited outpatients during different time periods in this cross-sectional study. Hence, selection bias was possible as we were uncertain whether psychiatric service utilization and the motivation to participate in the study were totally independent of personality. To clarify the influence of neuroticism on our study results, we divided the participants into two groups according to their level of neuroticism. The trend of regression coefficients of the two groups seemed to be similar within nine months after the end of the economic downturn. Therefore, we believe that selection bias did not distort our main findings.
Directions for future research
The insights gained from our study lay the foundation for several potential directions for future research aimed at enhancing our understanding of the intricate relationship between macroeconomic factors, personality traits, and sleep quality in clinical populations. First, to comprehensively assess the lasting implications of economic downturns on mental health, future studies could adopt a longitudinal approach. Tracking sleep quality and other mental health indicators over an extended duration beyond the immediate post-recession period would contribute to a more nuanced understanding of the prolonged effects. Second, examining the impact of economic fluctuations and personality traits across varying economic contexts would provide a broader perspective on the relationships observed in our study. Comparing findings across different economic scenarios would contribute to a richer understanding. Lastly, exploring the effectiveness of interventions aimed at improving sleep quality among clinical populations during economic fluctuations could be a promising area of research. Investigating whether interventions that target personality traits, coping strategies, or economic stress management can mitigate the negative impact on sleep quality would provide practical insights for mental health professionals (Piepiora and Piepiora, 2021; Piepiora et al., 2022).
Conclusions
This study examined how structural forces shape personal experiences and how personality affects individual responses to external stressors. Our findings increase the understanding of the impact of large-scale crises on sleep quality among clinical populations. Besides educational and occupational disadvantages, neurotic personality and economic recession further worsen sleep quality in patients with mood disorders. Enhancing patients’ understanding of predisposing and precipitating factors of insomnia and offering stress coping strategies may help to improve sleep quality.
Data availability
The datasets generated and analyzed in this study are not publicly accessible due to potential privacy concerns. However, they can be obtained from the corresponding author upon reasonable request.
References
Allen MS, Magee CA, Vella SA (2016) Personality, hedonic balance and the quality and quantity of sleep in adulthood. Psychol Health 31(9):1091–1107. https://doi.org/10.1080/08870446.2016.1178745
Antillón M, Lauderdale DS, Mullahy J (2014) Sleep behavior and unemployment conditions. Econ Hum Biol 14(C):22–32. https://doi.org/10.1016/j.ehb.2014.03.003
Barnes CM, Lefter AM, Bhave DP, Wagner DT (2016) The benefits of bad economies: business cycles and time-based work-life conflict. J Occup Health Psychol 21(2):235–249. https://doi.org/10.1037/a0039896
Bin YS (2016) Is sleep quality more important than sleep duration for public health? Sleep 39(9):1629–1630. https://doi.org/10.5665/sleep.6078
Brenner MH (1973) Mental illness and the economy. Harvard University Press
Brenner MH (1979) Mortality and the national economy. A review, and the experience of England and Wales, 1936–76. Lancet 2(8142):568–573. https://doi.org/10.1016/S0140-6736(79)91626-X
Brenner MH (2005) Commentary: Economic growth is the basis of mortality rate decline in the 20th century—experience of the United States 1901–2000. Int J Epidemiol 34(6):1214–1221. https://doi.org/10.1093/ije/dyi146
Buysse DJ, Reynolds 3rd CF, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28(2):193–213. https://doi.org/10.1016/0165-1781(89)90047-4
Calkins AW, Hearon BA, Capozzoli MC, Otto MW (2013) Psychosocial predictors of sleep dysfunction: the role of anxiety sensitivity, dysfunctional beliefs, and neuroticism. Behav Sleep Med 11(2):133–143. https://doi.org/10.1080/15402002.2011.643968
Cappuccio FP, D’Elia L, Strazzullo P, Miller MA (2010) Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care 33(2):414–420. https://doi.org/10.2337/dc09-1124
Cardon J, Eide E, Phillips K, Showalter M (2018) A model of sleep, leisure and work over the business cycle. https://doi.org/10.1016/j.jedc.2018.08.003
Caspi A, Moffitt TE (1993) When do individual differences matter? A paradoxical theory of personality coherence. Psychol Inq 4(4):247–271. http://www.jstor.org/stable/1449633
Chang S-S, Stuckler D, Yip P, Gunnell D (2013) Impact of 2008 global economic crisis on suicide: time trend study in 54 countries. Br Med J 347. https://doi.org/10.1136/bmj.f5239
Chang SS, Gunnell D, Sterne JA, Lu TH, Cheng AT (2009) Was the economic crisis 1997-1998 responsible for rising suicide rates in east/southeast Asia? A time-trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc Sci Med (1982) 68(7):1322–1331. https://doi.org/10.1016/j.socscimed.2009.01.010
Colodro-Conde L, Couvy-Duchesne B, Zhu G, Coventry WL, Byrne EM, Gordon S, Wright MJ, Montgomery GW, Madden PAF, Major Depressive Disorder Working Group of the Psychiatric Genomics, C, Ripke S, Eaves LJ, Heath AC, Wray NR, Medland SE, Martin NG (2018) A direct test of the diathesis-stress model for depression. Mol Psychiatry 23(7):1590–1596. https://doi.org/10.1038/mp.2017.130
Cooper WH, Withey MJ (2009) The strong situation hypothesis. Pers Soc Psychol Rev 13(1):62–72. https://doi.org/10.1177/1088868308329378
Dørheim SK, Garthus-Niegel S, Bjorvatn B, Eberhard-Gran M (2016) Personality and perinatal maternal insomnia: a study across childbirth. Behav Sleep Med 14(1):34–48. https://doi.org/10.1080/15402002.2014.941063
Dekker K, Blanken TF, Van Someren EJW (2017) Insomnia and personality-a network approach. Brain Sci 7(3):28. https://doi.org/10.3390/brainsci7030028
Directorate General of Budget (2021) Accounting and statistics. Directorate General of Budget, Executive Yuan, Taiwan. https://www.dgbas.gov.tw/point.asp?index=1
Duggan KA, Friedman HS, McDevitt EA, Mednick SC (2014) Personality and healthy sleep: the importance of conscientiousness and neuroticism. PLoS ONE 9(3):e90628. https://doi.org/10.1371/journal.pone.0090628
Eysenck HJ (1963) The biological basis of personality. Nature 199:1031–1034. https://doi.org/10.1038/1991031a0
Gellis LA, Lichstein KL, Scarinci IC, Durrence HH, Taylor DJ, Bush AJ, Riedel BW (2005) Socioeconomic status and insomnia. J Abnorm Psychol. 114(1):111–118. https://doi.org/10.1037/0021-843X.114.1.111
Hamilton M (1960) A rating scale for depression. JNNP 23(1):56–62. https://doi.org/10.1136/jnnp.23.1.56
Ingram RE, Luxton DD (2005) Vulnerability-stress models. In: Hankin BL, Abela JR (eds) Development of psychopathology: a vulnerability-stress perspective vol. 46. Sage Publications
Kroencke L, Geukes K, Utesch T, Kuper N, Back MD (2020) Neuroticism and emotional risk during the COVID-19 pandemic. J Res Pers 89:104038–104038. https://doi.org/10.1016/j.jrp.2020.104038
Lai YC, Lu MK, Yang YK, Lin JJ, Tan HP, Chen WJ, Lu RB, Kuo PH (2010) Clinical features and familial aggregation of social relationships in major depressive and bipolar disorders in southern Taiwan. Taiwan J Public Health 29:169–182. https://doi.org/10.6288/TJPH2010-29-02-10
Liao S-C, Lee M-B, Lung F-W, Wu C-Y, Chang C-M (2015) Suicide prevention in Taiwan: a ten-year review. Taiwan J Public Health 34:227–239. https://doi.org/10.6288/TJPH201534103131
Mai QD, Jacobs AW, Schieman S (2019) Precarious sleep? Nonstandard work, gender, and sleep disturbance in 31 European countries. Soc Sci Med 237:112424. https://doi.org/10.1016/j.socscimed.2019.112424
Ohayon MM, Guilleminault C (2005) Epidemiology of sleep disorders. In: Sleep: a comprehensive handbook. Wiley, pp. 73–82
Perales F, Plage S (2017) Losing ground, losing sleep: local economic conditions, economic vulnerability, and sleep. Soc Sci Res 62:189–203. https://doi.org/10.1016/j.ssresearch.2016.08.006
Piepiora P, Piepiora Z (2021) Personality determinants of success in men’s sports in the light of the big five. IJERPH 18(12):6297, https://www.mdpi.com/1660-4601/18/12/6297
Piepiora P, Piepiora Z, Bagińska J (2022). Personality and sport experience of 20–29-year-old Polish male professional athletes [Original Research]. Front Psychol 13. https://doi.org/10.3389/fpsyg.2022.854804
Roy HP, Brown E, Baker RW, Nierenberg AA (2006) Clinical features of bipolar depression versus major depressive disorder in large multicenter trials. Am J Psychiatry 163(2):225–231. https://doi.org/10.1176/appi.ajp.163.2.225
Ruhm CJ (2000) Are recessions good for your health? Q J Econ 115(2):617–650. https://doi.org/10.1162/003355300554872
Seow LSE, Tan XW, Chong SA, Vaingankar JA, Abdin E, Shafie S, Chua BY, Heng D, Subramaniam M (2020) Independent and combined associations of sleep duration and sleep quality with common physical and mental disorders: results from a multi-ethnic population-based study. PLoS ONE 15(7):e0235816. https://doi.org/10.1371/journal.pone.0235816
Spielman AJ, Caruso LS, Glovinsky PB (1987) A behavioral perspective on insomnia treatment. Psychiatr Clin North Am 10(4):541–553
Su MH, Chen HC, Lu ML, Feng J, Chen IM, Wu CS, Chang SW, Kuo PH (2018) Risk profiles of personality traits for suicidality among mood disorder patients and community controls. Acta Psychiatr Scand 137(1):30–38. https://doi.org/10.1111/acps.12834
Sun W, Yu Y, Yuan J, Li C, Liu T, Lin D, Lau A, Zhong C, Xu T, Shan G (2015) Sleep duration and quality among different occupations—China national study. PLoS ONE 10(3):e0117700–e0117700. https://doi.org/10.1371/journal.pone.0117700
Tanji F, Kakizaki M, Sugawara Y, Watanabe I, Nakaya N, Minami Y, Fukao A, Tsuji I (2015) Personality and suicide risk: the impact of economic crisis in Japan. Psychol Med 45(3):559–573. https://doi.org/10.1017/S0033291714001688
Tapia Granados JA (2005) Increasing mortality during the expansions of the US economy, 1900–1996. Int J Epidemiol 34(6):1194–1202. https://doi.org/10.1093/ije/dyi141
Tapia Granados JA (2008) Macroeconomic fluctuations and mortality in postwar Japan. Demography 45(2):323–343. https://doi.org/10.1353/dem.0.0008
Tapia Granados JA (2017) Macroeconomic effects on mortality: issues, controversies, and directions for research. In: Scott RA, Kosslyn SM, Buchmann MC (eds) Emerging trends in the social and behavioral sciences, John Wiley & Sons, Incorporated, https://doi.org/10.1002/9781118900772.etrds0436
Tapia Granados JA, Ionides EL (2008) The reversal of the relation between economic growth and health progress: Sweden in the 19th and 20th centuries. J Health Econ 27(3):544–563. https://doi.org/10.1016/j.jhealeco.2007.09.006
Tett RP, Toich MJ, Ozkum SB (2021) Trait activation theory: a review of the literature and applications to five lines of personality dynamics research. Annu Rev Organ Psychol Organ Behav 8(1):199–233. https://doi.org/10.1146/annurev-orgpsych-012420-062228
Tsai PS, Wang SY, Wang MY, Su CT, Yang TT, Huang CJ, Fang SC (2005) Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual Life Res 14(8):1943–1952. https://doi.org/10.1007/s11136-005-4346-x
Wu PJ, Chang SM, Lu MK, Chen WJ, Yang YK, Yeh TL, Liao SC, Lu RB, Kuo PH (2012) The profile and familiality of personality traits in mood disorder families. J Affect Disord 138(3):367–374. https://doi.org/10.1016/j.jad.2012.01.015
Yoon J-H, Junger W, Kim B-W, Kim Y-J, Koh S-B (2012) Investigating the time lag effect between economic recession and suicide rates in agriculture, fisheries, and forestry workers in Korea. Saf Health Work 3(4):294–297. https://doi.org/10.5491/SHAW.2012.3.4.294
Acknowledgements
This study was supported by the National Taiwan University Hospital (Grant numbers 109-M4782 and 113-X0030), the National Taiwan University (Career Development grant number 110L7860), and the Ministry of Science and Technology (Grant numbers 108-2314-B-002-136-MY3 and 105-2628-B-002-028-MY3), which had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors acknowledge statistical assistance provided by the Center of Statistical Consultation and Research in the Department of Medical Research, National Taiwan University Hospital. The authors would also like to acknowledge Jennifer Yi-Ying Chen from the Department of Psychiatry, National Taiwan University Hospital, for providing editing and proofreading assistance.
Author information
Authors and Affiliations
Contributions
Conceptualization: I-Ming Chen, Hsi-Chung Chen; data curation: Po-Hsiu Kuo, Ming-Hsien Hsieh, Chih-Ming Liu, Tsung-Yang Wang, Jen-Hui Chan; formal analysis: Shih-Cheng Liao, I-Ming Chen, Hsi-Chung Chen, Po-Hsiu Kuo; writing—original draft preparation: I-Ming Chen, Hsi-Chung Chen, Po-Hsiu Kuo; writing—review and editing: I-Ming Chen, His-Chung Chen, Chih-Ming Liu, Shih-Cheng Liao, Ming-Hsien Hsieh, Tsung-Yang Wang, Jen-Hui Chan, Po-Hsiu Kuo.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study protocol was approved by the Institutional Review Board of the National Taiwan University Hospital (case number 201907138RIND), and all research was performed in accordance with relevant guidelines in the Declaration of Helsinki.
Informed consent
Adult outpatients from two medical centers and a psychiatric hospital were invited to participate in the study. Informed consent was obtained from all individual participants included in the study, who were interviewed by trained research assistants to collect data and complete questionnaires.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, IM., Chen, HC., Liu, CM. et al. The great recession, neurotic personality, and subjective sleep quality among patients with mood disorders. Humanit Soc Sci Commun 11, 969 (2024). https://doi.org/10.1057/s41599-024-03467-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-024-03467-7
